
Abstract
Background
The patient experience of Parkinson's disease (PD) is heterogeneous, with limited prognostic tools to predict individual outcomes, leading to significant uncertainty for people with PD. Under-recognition of both psychosocial and biological drivers of fear and uncertainty in Parkinson's disease (PD) by clinicians may further contribute to patient distress.
Objective
The objective of the present study is to investigate fear and uncertainty in people with PD.
Methods
In-depth interviews were conducted with twenty people with PD (11 semi-structured, 9 guided/prompted). Thematic analysis organized the fears/uncertainties by topic as well as by contextual factors such as the timing of the fear (e.g., active or anticipatory; at the time of diagnosis or developed subsequent to diagnosis) and the lexicon used to describe it.
Results
Participants expressed a wide range of fears and uncertainties about their future and quality of life with PD, which shifted with disease progression. Most fears were anticipatory rather than in response to current concerns. Participants reported substantial psychosocial influence from media personalities or family/friends with PD. Most participants reported that they had not disclosed their fears to their healthcare providers.
Conclusions
Clinicians caring for people with PD should be aware of a range of often-unspoken fears and uncertainties, which may carry a substantial psychosocial burden. Open acknowledgement and normalization by clinicians may help patients feel less isolated in their disease.
Plain language summary
Fears and uncertainties that many people with Parkinson's disease (PD) experience are not always identified or recognized by their healthcare providers. This study interviewed 20 people with PD to explore these emotions in depth. Interview transcripts were analyzed by a team of researchers trained in qualitative, thematic analysis. Study participants reported a wide, diverse range of fears and uncertainties about PD, which often focused on future possibilities more than their present challenges. Many of these fears were influenced by participants’ exposure to media personalities, friends, or family members with PD. Despite their significant emotional impacts, most participants had not discussed their fears with their healthcare providers. These findings suggest that healthcare providers for people with PD should be aware of the breadth of fears and uncertainties that their patients often experience. By addressing these often-unspoken concerns, clinicians can support the emotional well-being of people living with PD.
Introduction
Psychosocial distress is high following the diagnosis of a life-altering, incurable illness like Parkinson's disease (PD). People with PD (PwP) describe a loss of agency, accompanied by “body betrayal” and disconnection from oneself, 1 which may be further exacerbated by clinician emphasis on mechanistic views of disease rather than the biopsychosocial experience of illness, as well as the under-recognition of fear and uncertainty as critical components of well-being. Research in other chronic illnesses, including cancer2,3 and cognitive impairment,4–6 has highlighted the impact of fear and uncertainty on anxiety and other negative health outcomes. 7 Recent research that investigates relationships between stress and mental health concerns with PD symptom severity and disease progression further underscores the importance of understanding fear as a contributing factor to PD morbidity.8–10
One prior study analyzed fear of progression as associated with anxiety and self-efficacy, but not disease duration or severity, 11 implying that fear may affect PwP at any stage. Another survey of fear in a large online symptom database identified a wide variety of specific fears, 12 including fear of future cognitive impairment and fear of becoming a burden on others, as important additional topics of concern for PwP. The objective of the present study is to build on this prior work, developing a richer context for fear and uncertainty in Parkinson's disease by qualitative analysis of PwP's own words.
Methods
This study was designed and implemented by a collaborative team of neurologists at Duke University, the University of Pittsburgh, and the University of Toronto, researchers from The Michael J. Fox Foundation (MJFF), and SSRS, a social science research organization. The study received approval from the WCG Institutional Review Board (Protocol 1366586). Participants were recruited by MJFF through referrals, flyers, and posts in established community engagement research forums. Eligible participants were English-speaking United States residents, age > 18 years with a diagnosis of PD (disease duration of at least one year) and reflected a mix of demographic characteristics including sex, age, race/ethnicity, educational attainment, and geography. Following verbal telephone consent, participants were contacted by a member of the SSRS team to schedule their interview.
Twenty interviews were conducted by authors DS and NL from April to July 2024, each lasting approximately 45 min, in which participants were asked to describe their fears and uncertainties at the time of their PD diagnosis and at the time of the interview, as well as future concerns they may anticipate. After eleven interviews, it was determined that the data had reached thematic saturation. Guided by findings from the first set of interviews (Phase 1) and prior work, 12 a list was developed of possible fears and uncertainties people with Parkinson's disease might be concerned about as they think about their future. For the subsequent nine interviews (Phase 2), participants were presented this list of items and were asked to discuss which fears did or did not resonate with them in the present and future. The focus of this guided discussion was to further interrogate the range of fears and uncertainties as well as refine the lexicon of fear and uncertainty by asking participants to reflect on terminology and classifications of fears.
Analysis of interview transcripts from both phases was performed by authors EDT, DS, NL, and SM, who are trained in qualitative research methods. NVivo 14 was used to develop a codebook of common themes. Themes were refined by iterative discussions between researchers until a single, standardized codebook was developed. Based on the structure of the discussion guides, themes were organized into the major domains discussed next.
Results
Analysis yielded valuable insights about the content of and context in which participants experience fears and uncertainties related to PD. This results section establishes three contextual elements that warranted consideration in interpreting the meaning of fear and uncertainty statements: timing of fear, social environment factors, and language. Then, it will report seven categories of uncertainties that participants reflected on during the interviews: (1) symptoms (2) disease progression (3) healthcare (4) quality of life (5) employment (6) social networks and (7) perception.
Demographics
Demographic details of the twenty participants (phase 1, n = 11; phase 2, n = 9) are shown in Table 1. Most participants were women (n = 12, 60%), White only (n = 13, 65%), and college graduates (n = 19, 95%). Nineteen participants were taking at least one medication for PD; the most common drugs were carbidopa/levodopa (n = 15, 75%) and dopamine agonists (n = 9, 45%).
Participant characteristics.
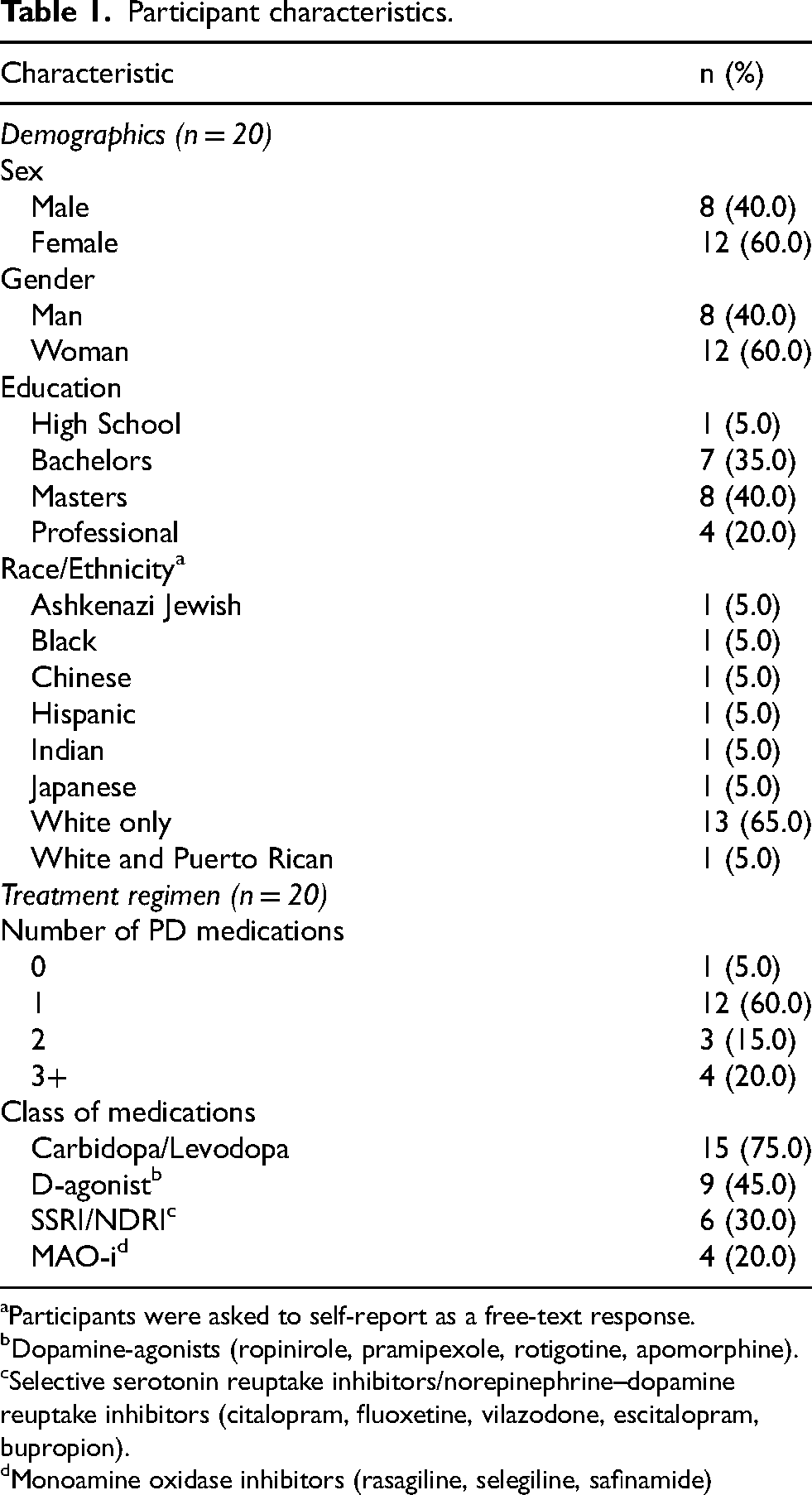
Participants were asked to self-report as a free-text response.
Dopamine-agonists (ropinirole, pramipexole, rotigotine, apomorphine).
Selective serotonin reuptake inhibitors/norepinephrine–dopamine reuptake inhibitors (citalopram, fluoxetine, vilazodone, escitalopram, bupropion).
Monoamine oxidase inhibitors (rasagiline, selegiline, safinamide)
Context
Timing of fears
Analysis of the fear statements expressed by participants revealed two intersecting, distinct contextual factors – timing with respect to disease course (at the time of diagnosis versus subsequent to diagnosis) and timing with respect to the time of the interview (past/resolved, current, and future). These contextual elements were important to consider during analysis in order to recognize potential trends and changes in uncertainties over time for participants. Figure 1 illustrates the four possible timing combinations of fears.
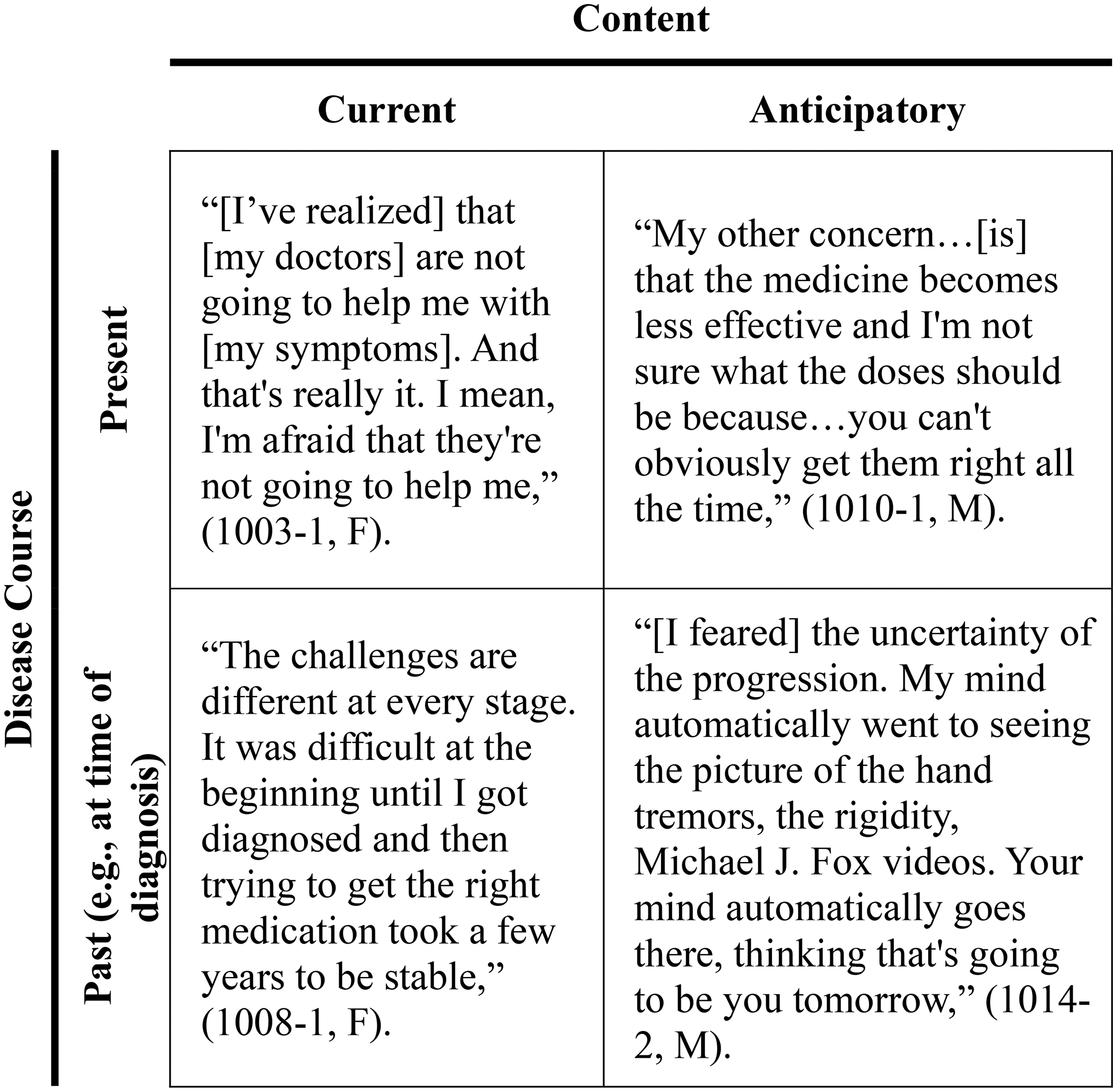
Fear matrix.
Social environment factors
In describing many of their fears, participants referred to a variety of influences that informed their concerns. Some participants referenced depictions of PD in popular media or disclosed by celebrities as a source of fears about their disease progression; e.g., “When you see Michael J. Fox on TV and do his interviews, you think, that's me. Is that going to be me next year?” (1016-2, F) ((Subject identifier-phase, sex); e.g., (1016-2, F) is a female phase 2 participant identified as 1016.). Participants described formative experiences with groups of PwP that provoked fears, like one interviewee who described attending a PD conference: “It was two weeks after my diagnosis and it was a horrible experience for me because I thought, ‘This is what I'm going to look like,’” (1002-1, F). Individuals with first- or second-degree relatives with PD often reported fears directly grounded in the disease courses of their kin. Notably, some individuals contextualized PD-specific fears in the setting of other illnesses they had exposure to; e.g., “My dad died of cancer and my mom died of congestive heart failure. And both of them were extended spirals down and it was hard on me and my sisters, and I don't want to do that,” (1005-1, M).
Language
During phase 1 interviews, which posed predominantly open-ended questions, participants spontaneously volunteered diverse opinions about the terms “fears” and “uncertainties.” In phase 2, participants were specifically asked which word(s) most accurately described their PD experiences: fears, worries, concerns, uncertainties, or anxieties. Multiple participants expressed that “fears” was their preferred term because it carried some emotional salience, while other participants preferred “concerns”, citing that it seemed like the broadest, most general term. Interestingly, one participant implicitly referenced timing as relevant concepts, sharing that, “Currently, I would say concerns. At the time I was diagnosed [I would say], anxieties…it depends upon what stage you’re at,” (1016-2, F). For the sake of consistency, “fears” and “uncertainties” will be used to present analysis results, with further reflections on language in the Discussion.
Content
Symptoms
Participants commonly expressed fears and uncertainties about PD motor and non-motor symptoms. One prevalent fear was anticipating symptoms that may impact mobility, often centered on the need for assistive devices; e.g., “In the beginning I was really, really scared that I would be in a wheelchair very soon, and my mobility I think was the thing that I feared the most,” (1003-1, F). The majority of participants characterized these fears as anticipatory rather than current. Many participants also shared fears about falling, which were frequently related to falls they had already experienced or episodes of imbalance where they nearly fell. Non-motor symptoms of concern included anxiety, bladder/bowel control, sleep difficulties (e.g., insomnia, acting out dreams), and fatigue. Many participants shared both anticipatory and current fears about cognition, such as PD-related dementia or cognitive decline; e.g., “I think most people can deal with the overt symptoms, like tremor and slowness, but I think the cognitive problems, the cognitive decline that often occurs with Parkinson's, is the biggest fear of anyone,” (1011-1, F). Other fears related to cognition included changes in personality, short-term memory loss, and general mental acuity.
Uncertainty about the root causes of symptoms with possible parkinsonian features was also frequently referenced. Participants questioned whether symptoms like muscle spasms, pain, gastrointestinal symptoms, and fatigue may be due to diagnosed or undiagnosed illnesses that were not PD. Participants shared uncertainties about whether cognitive symptoms may be attributable to normal aging or dementia/Alzheimer's disease, rather than PD. One participant disclosed, “I've said since the beginning, ‘Is it age? Is it Parkinson's?’ I mean, we all get a little draggy once in a while…one of my biggest questions is how much can I allocate to Parkinson's?” (1001-1, F).
Disease progression
Participants expressed a myriad of fears related to the progression of PD, mostly in an anticipatory context, with different types of concerns underpinning their worries about disease advancement. While some participants were concerned about how quickly or slowly their PD would progress, uncertainties about the future nature and severity of PD symptoms were reported more frequently. Many participants referenced that exposure to other PwP influenced these fears, ranging from family members to public figures like Michael J. Fox. Day-to-day fluctuation in PD symptoms was also a cause of concern for multiple participants; e.g., “The variability of the disease [throughout the day] and the changes that manifest…[are] what makes it such a terrible disease,” (1010-1, M). The incurable and terminal nature of PD was a prevalent fear, and many participants shared fears about death and dying. When asked if they had any other fears about PD, one participant simply said, “Other fears? It's a terminal disease. We don't get out of life alive,” (1002-1, F). It was more common for participants to share fears about the progression and future severity of their disease than death, specifically.
Healthcare treatments and access
Fears related to PD medical care emerged as a notable source of anxiety. Some participants expressed concern about the side effects of their medications, the potential for waning effectiveness over time, and whether appropriate treatments would be available as new symptoms emerge. One participant commented, “I’m concerned that the medication won’t work after a while…my doctor said that sometimes people take 200 pills a day,” (1010-1, M). Interviewees frequently highlighted fears related to deep brain stimulation (DBS); e.g., “I…am not a candidate [for DBS] yet, and I will worry about it big-time if it becomes a question because I’m terrified. I mean, having my knee replaced was one thing, but putting stuff in my brain… I really hope I can avoid that,” (1001-1, F). Apart from the invasive nature of the procedure, potential adverse effects and mistakes during surgery were cited as causes for concern. A few participants also expressed fears about lacking knowledge about the disease or its treatments or, as one participant described it, “the fear…[that] you don’t know what you don’t know,” (1005-1, M) were voiced by several participants.
Healthcare access and quality were repeatedly mentioned in interviews. Some participants shared that their access to appropriate PD care was limited by insurance coverage, financial limitations, or regional availability. One participant shared, “The availability of healthcare specialists is a huge concern for me…the few that there are, you can't get into, they don't seem to have enough time,” (1018-2, M). Some participants also raised doubts about the quality of healthcare they were receiving, questioning their providers’ level of PD expertise, and a few referenced the presence of systemic health inequities. One woman of color explained that doctors attributed her early motor symptoms and pain to a psychiatric issue, and suggested this was an example of a systemic bias where, “minority women…[are] labeled as…histrionic or exaggerating,” (1008-1, F).
Quality of life
Fear of a decline in quality of life was a common thread through many of the interviews. Participants were worried about functional decline and increasing need for assistance from others. They spoke of concerns of losing aspects of their independence as PD advanced – specifically, participants were concerned about ability to perform activities of daily living and a future need for assisted living. One participant shared, “That's a big fright…moving from independent living to assisted living. I think I'm going to fight that tooth and nail because I am so darn independent. I think…that's going to be my biggest issue,” (1002-1, F). Participants also highlighted the ability to attain personal goals and milestones as an important component of quality of life that they felt may be threatened by PD progression. One participant disclosed, “…you think about, ‘Will I be able to walk my daughters down the aisle? Will I be able to feed myself?’” (1005-1, M).
Employment
Difficulty with employment was a prominent source of fear and uncertainty for several individuals. Some participants commented that PD symptoms had already adversely impacted their ability to perform necessary jobs, while others were fearful of the possibility this may be the case in the future. Some interviewees related this to the threat of termination, with one participant stating, “I want to go on my terms. I don’t want to be forced out,” (1015-2, F). The importance of income was also acknowledged by several participants, who expressed present or future fears about how not working due to PD might affect them and their dependents financially. Finally, the personal and emotional impacts of needing to retire early were apparent during some of the interviews; one participant explained, “I didn’t want the end of my career to be…a situation that I hurt somebody,” (1003-1, F).
Social networks
Another recurring theme in many interviews was the fear of the impacts PD had (or might have) on social roles and relationships. For some participants, their fears centered around the impact PD might have on their ability to engage in group social situations; e.g., “…having the inability to have a good conversation with my friends or my family, that concerns me. I don’t want to be the guy left over in the corner, because no one wants to speak to because he can’t talk appropriately,” (1014-2, M). Other participants were more focused on the impacts on individual relationships, particularly their children and spouses. Ability to perform duties seen as integral to one's familial role came up multiple times; one participant shared it was distressing that, “I always thought that I’d be the person taking care of everyone else and I was slowly realizing that they may be taking care of me,” (1004-1, M). A few participants reported current or anticipatory fears about decreased or lost physical intimacy with their partners.
Several participants voiced fears related to care partners (CP). Many focused on the burden they believed they may pose, currently or in the future, to their CPs. For example, one participant explained of his family, “I’ve told them repeatedly, I do not want them to be the ones caring for me…I have no problem being put into a memory care unit. Because I absolutely don’t want them to be burdened by this,” (1003-1, F). Another source of uncertainty was the availability of CPs; one participant questioned, “I guess the other issue is if my husband dies before I do, who's going to take care of me?” (1001-1, F).
Perception
Multiple participants highlighted the issue of the stigma of having PD; often, this centered around fears that their PD symptoms would be apparent to other people. One participant noted, “I do not like when I have off-times at work. It just makes me feel kind of inferior and embarrassed, which I know I shouldn’t, but it does,” (1004-1, M). In particular, participants were worried about the assumptions other people might make if they were aware of the participants’ diagnoses; for example, “I don’t want them to feel sorry for me…I don’t want it to define me,” (1002-1, F).
Discussion
This qualitative study of PwP provides deep characterization of a wide range of fears and uncertainties, which shift as the disease progresses. Often, in the initial months after diagnosis, PwP tend to spotlight fears around losses, including loss of mobility, employment, and/or independence. These existential fears mirror those reported in studies of individuals with other life-limiting conditions, such as cancer or asthma.2,13 However, as the disease progresses and the PwP becomes more familiar with PD's impact on daily life, fears and uncertainties become more concrete, focusing on variability in medication response, fear of falling, or the inherent uncertainty in disease progression.
This interplay between disease course (present vs past fears) and content (current vs anticipatory fears) provides important context for the clinician providing guidance to the PwP. By taking the time to understand in which quadrant the PwP's fears lie, the clinician can provide better support, such as empathetic listening, referral to grief counseling services, and/or recognition of mental health concerns such as anxiety or depression. For instance, some PwP may benefit from support groups, but for many others, particularly at the earlier stages of the disease, seeing more advanced people at support groups, in the media, or even in the clinical waiting room can further amplify their fears about loss and disability. Several participants specifically referenced Michael J. Fox, reflecting in part the study recruitment strategy through MJFF-sponsored activities, but also the impact that a celebrity can have in shaping public perception of illness, both positive (raising awareness) and negative (implying that a single person's story is representativeness of all PwP stories). Therefore, it would be appropriate for a clinician's professional advice about whether to access support groups or media about PD to be informed by their assessment and characterization of a patient's personal combination of fears and uncertainties at a given time. Furthermore, anticipatory guidance about specific complications, such as cognitive impairment, psychosis, or loss of mobility, may reassure the PwP about treatment options and improve the clinician-patient relationship. Similar to depression screening 14 and proactive referral to rehabilitation therapy, 15 early and non-judgmental discussion of fear and uncertainty has the potential to improve quality of life among PwP.
The clinician should also be aware of the impact of the language used when addressing fears and uncertainties. During Phase 1 of our study, which was unprompted with predominantly open-ended questions, participants often used the words “fear” and “uncertainty” interchangeably or volunteered alternate terms such as “concerns” or “anxieties.” However, during the prompted portion of our study, when asked specifically which terms were accurate, participants made important distinctions between the emotional valence of “fear,” the specificity of “uncertainty,” the broad appeal of “concern,” and the clinical bent of “anxiety.” Some participants felt strongly that “fear” was the best term for their experience, while others said they specifically did not like that term due to its negative connotations. This has important implications for clinical communication, particularly given the impact of PD-mediated dysfunction of the frontostriatal fluency network.16,17 It would be of benefit for providers to take the time to clarify their patients’ preferred terms and the distinctions they draw between different words. For example, understanding why a particular patient considers falling to be an “anxiety” but cognitive decline to be a “fear” may yield clinically-relevant insights. The terminology used by patients and providers is both individualized and nuanced, highlighting the complexity of care for this patient population.
Most prior studies of fear and uncertainty in PD have focused on specific fears (e.g., fear of falling) 18 or quantified domains of fear 12 without added nuance. To this growing body of literature, the present study adds important contextual features, including attention to the lexicon used by participants themselves as well as the influence of disease course, current/anticipatory concerns, and social relationships. In so doing, the study provides guidance to improve clinician-PwP communication in this area. In particular, the time of diagnosis was associated with highly salient—and for some participants, all-consuming—fear and uncertainty. This work further emphasizes the need for clinicians to be attentive to the method of diagnostic disclosure and to proactively offer opportunities for PwP to express sometimes intense and vulnerable emotions.
Clinicians are positioned to recommend specific actions for their patients to address their individual fears and uncertainties. Recommendations for non-pharmacologic support should be informed by a patient's unique concerns at a given point in time and based on shared decision making. For example, an individual considering attending a support group should be offered information about what aspects may be beneficial or detrimental to them, given their clinician's understanding of their current and anticipatory concerns. Providers should plan to revisit these conversations regularly as their patients’ fears and uncertainties change. Addressing treatment-related fears through a combination of active listening and patient education may also lessen potential for nocebo effects, which early research suggests may affect DBS and other PD treatment responses.19,20 Discussions about advanced/interventional treatments for PD, such as DBS, in this study suggest they will likely be central to fears and uncertainties in many PwP in the years to come. Physicians can also support PwP in communicating their concerns to other healthcare providers such as social workers and other mental health professionals, thus facilitating direct conversations about these concerns. The significance of word choice and phrasing when discussing fears and uncertainties to this study's participants suggest that PwP will benefit from invitations by providers for patients to give constructive feedback on communication style.
The fear clusters identified by participants are consistent with prior qualitative analysis of meaningfulness and symptom impact, even at early stages of the disease.21,22 In this study, more than a third of participants self-identified with minoritized racial/ethnic identities, which is particularly important given the impact of culture and language on the lived experience of illness. Nevertheless, some caveats should be noted. Participants in this study were highly educated (95% with post-secondary education) and able to articulate nuanced perspectives on both current and past/future fears. PwP with lower cognitive reserve may have more difficulty expressing their concerns. Further, we did not capture additional demographic features such as years since diagnosis or presence of mood symptoms, both of which may influence the types and severity of fear or uncertainty experienced by the participant. It should be noted that participant medications may provide an approximation of disease severity and an indicator of comorbid mood disorder, particularly since reported frequencies are broadly representative of research on prescribing patterns for PwP.23,24 A follow-up survey of a larger and deeply-phenotyped cohort is underway to help address these limitations. Future research should focus on understanding fears and uncertainties at different disease stages in larger study populations, to allow for quantitative analysis and, ultimately, a statistically-driven hierarchy of fears and uncertainties among PwP. Moreover, nonprofits, advocacy groups, and specialty societies play a crucial role in raising visibility of new insights regarding fears and uncertainties and disseminating key findings to a range of stakeholders, 25 including people with PD, clinicians caring for them, and regulatory agencies tasked with evaluating novel therapeutics.
In conclusion, PwP experience a wide range of worries, fears, and uncertainties, which may shift over time. Better clinician awareness, direct questioning with both closed- and open-ended questions, and anticipatory guidance may be able to help allay these distressing thoughts, both at the time of diagnosis and at clinically-relevant milestones throughout the disease course.
Footnotes
Acknowledgments
The authors wish to thank the people with Parkinson's disease who contributed to this research.
ORCID iDs
Ethical considerations
This study was approved by the WCG Institutional Review Board (Protocol 1366586).
Consent to participate
Verbal informed consent was obtained from each participant immediately prior to the start of the interview.
Consent for publication
Not applicable
Funding statement
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was wholly funded by a grant from The Michael J. Fox Foundation for Parkinson's Research (MJFF, grant 024438).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Caitlin Kelliher, Stephanie Benvengo, and Catherine Kopil are employees of MJFF. Lana Chahine receives research support from MJFF, National Institutes of Health, and University of Pittsburgh, is study site investigator for a study sponsored by Biogen, receives consulting fees from MJFF, receives royalties from Elsevier (for authorship) and from Wolters Kluwel (for authorship). Connie Marras receives consulting fees from modality.ai, financial compensation as a steering committee member from MJFF and the Parkinson's Foundation (PF), research support from MJFF, Canadian Institutes of Health Research, International Parkinson and Movement Disorders Society, the Weston Brain Institute and PF. Sneha Mantri receives consulting fees from International Consulting Associates and AbbVie, honoraria and travel reimbursement from PF and MJFF, and research support from the Duke Endowment, PF, MJFF, and the Josiah Macy Jr Foundation. Other authors (EDT, DS, NL, and RR) have no financial conflicts to report.
Data availability
The audiovisual interviews obtained and analyzed in this study are not publicly available due to privacy concerns. The interview transcripts are available upon signing a data use agreement with MJFF and Duke University.