
Abstract
Background
Best practice guidelines in Parkinson's disease (PD) calls for the immediate initiation of rehabilitation therapies (inclusive of physical (PT) and occupational therapy (OT)) to prevent or ameliorate the loss of function and quality of life associated with disease progression.
Objective
The purpose of this study was to determine the utilization of PT and OT services within the first 2 years following PD diagnosis and to observe longitudinal trends in PT and OT utilization early following PD diagnosis.
Methods
This retrospective cohort study accessed 12 years (2011 to 2023) of data from electronic health records at a midwestern US healthy system. Patients with new PD diagnoses and two-years of visit history were included. The primary outcome was utilization of PT or OT services within two-years of PD diagnosis. Data extracted included demographics and PD therapies. Records of 9720 patients were included in the analyses.
Results
Overall, 36.9% of the cohort (n = 3586) received either physical or occupational therapy within two years of receipt of PD diagnosis. Increasing age, higher comorbidity index, female gender, use of dopamine replacement therapies, and African American race were all positively associated with receipt of PT or OT services (ps < 0.007). The longitudinal trend revealed an average year over year increase in PT/OT utilization of 1.4% between 2013 and 2021 (p < 0.001).
Conclusions
This study shows a promising increase in utilization of PT and OT services over previous reports and longitudinally, however it continues to convey how far clinical practice continues to lag behind best practice and scientific recommendation.
Plain language summary
This study looked at how often people with Parkinson's disease (PD) use physical therapy (PT) and occupational therapy (OT) in the first two years after being diagnosed. These therapies are important because they can help maintain a person's ability to function and improve their quality of life as the disease progresses. The researchers analyzed data from 9720 patients diagnosed with PD between 2011 and 2023. They wanted to see how many of these patients received PT or OT within two years of their diagnosis and to track how the use of these therapies changed over time. The study found that only about 37% of patients received PT or OT within the first two years of their PD diagnosis. Certain groups of people were more likely to use these therapies, including older adults, women, African Americans, those with other health conditions, and those taking medication to manage PD symptoms. Over time, the use of PT and OT increased slightly each year by about 1.4% between 2013 and 2021. The findings suggest that while more people are using PT and OT after a PD diagnosis than in the past, many still aren’t receiving these important therapies as recommended. This highlights a gap between what is considered best practice and what is actually happening in clinical care. More efforts may be needed to ensure that all people with PD have access to the therapies that can help them live better with the disease.
Keywords
Introduction
In the management of Parkinson's disease (PD) physical (PT) and occupational therapists (OT) play a critical role in addressing a wide constellation of symptoms experienced by those with PD. 1 PT and OT services have demonstrated the ability to improve function, increase independence with activities of daily living, and elevate quality of life for those living with PD.2–5 This has resulted in recommendations of annual review of rehabilitation needs among individuals with PD by both the American Academy of Neurology (AAN), National Institutes for Health and Care Excellence (NICE), and a recent Parkinson's Foundation internation task force consensus statement.6–8 Despite these recommendations, previous studies have shown low utilization of and referral rates to rehabilitation services among individuals with PD,9–11 those these studies have been limited geographically to the United States, Korea, and Parkinson's Foundation Centers of Excellence. This incongruence between the preponderance of evidence for and the actual utilization of rehabilitation services is troubling 12 and further evidence is needed to better understand the factors that contribute to lack of provider referral and patient utilization of these valuable services.
While much of the above evidence for the benefit of PT and OT services is focused on those with moderate to advanced disease, there is strong evidence to support the early utilization of rehabilitation services among individuals with PD. 13 Traditionally, the need for rehab services have been assumed to be negligible prior to the onset of disability (falls, freezing of gait, ADL difficulty, etc.) among those with PD which typically occurs in the moderate to late stages of disease, many years following diagnosis.12–14 However, recent evidence shows changes in function and slow accumulation of disability occurring early in the disease process, preceding diagnosis.13–17 Given the evidence for benefits of rehabilitation interventions among those in the early stages of PD, the NICE guidelines and Parkinson's Foundation consensus statement go as far as to recommend referral to PT and OT services for those in the early stages of PD.7,8,13 Ultimately, intervening in early PD provides a more robust opportunity to mitigate disability and lead to better long term outcomes over the course of PD. 13
With the increase in proliferation of evidence supporting early and regular rehabilitation services for individuals with PD and the recommendations of the AAN, NICE, and The Parkinson's Foundation task force it is hoped that the trends regarding utilization of rehabilitation services, particularly among those in the early stages of PD, have increase, however this has not been investigated. As such, the purpose of this study was to describe the utilization of PT and OT services among individuals recently diagnosed with PD (within the first 2 years of PD diagnosis), in a large midwestern health system in the United States. Additionally, this study aimed to determine factors associated with utilization of PT and OT services among individuals with PD. It was anticipated that increased age and a greater number of comorbid conditions would be related to increased utilization of PT and OT services. Lastly, the current study analyzed the longitudinal trends in utilization of PT and OT services among recently diagnosed individuals with PD.
Methods
Data were obtained from Saint Louis University-SSM (SLU-SSM) health care System's Virtual Data Warehouse (VDW). SLU-SSM is a member site of the Health Care Systems Research Network (HCSRN) (http://www.hcsrn.org) and the VDW was created and is maintained per HCSRN specifications. The SSM healthcare system includes locations in Missouri, Illinois, Oklahoma, and Wisconsin. The VDW contains deidentified clinical data for over 5 million patients dating back to 2008. This includes ICD-9 and ICD-10 codes, procedure codes, pharmacy orders, and demographics. Multiple studies have been published using this data source.18–22 As patients do not actively participate and all data is de-identified, all studies utilizing VDW data are approved as non-human subjects research by the Saint Louis University Institutional Review Board.
Cohort definition
For this retrospective cohort study, we selected patients ages 18 or older with a new ICD-9 or ICD-10 diagnosis of PD between 1/1/2011-1/31/2021. These dates were chosen to allow a 2-year wash out period prior to PD diagnosis and a 2-year follow-up period to define the outcome, utilization of PT or OT services. Additionally, to ensure patients were regular users of the SSM system, patients were required to have activity in the 2 years prior and the 30 days after PD diagnosis. This provides confidence that when the PD diagnosis is received, it is in fact the patient's first PD diagnosis. Specifically, data was available going back to 2008, and at the time of analysis, as far forward as January 31, 2023. The analytic cohort was limited to patients whose first PD diagnosis was between January 1, 2011 and January 31, 2021. This provides patients diagnosed in 2021 and earlier at least 2-years of follow up data. Also, for patients receiving a PD diagnosis in 2011, there was at least 2-years washout period Further operational details of the cohort definition are provided in Figure 1. These criteria resulted in a cohort of 9720 patients with a new diagnosis of PD.
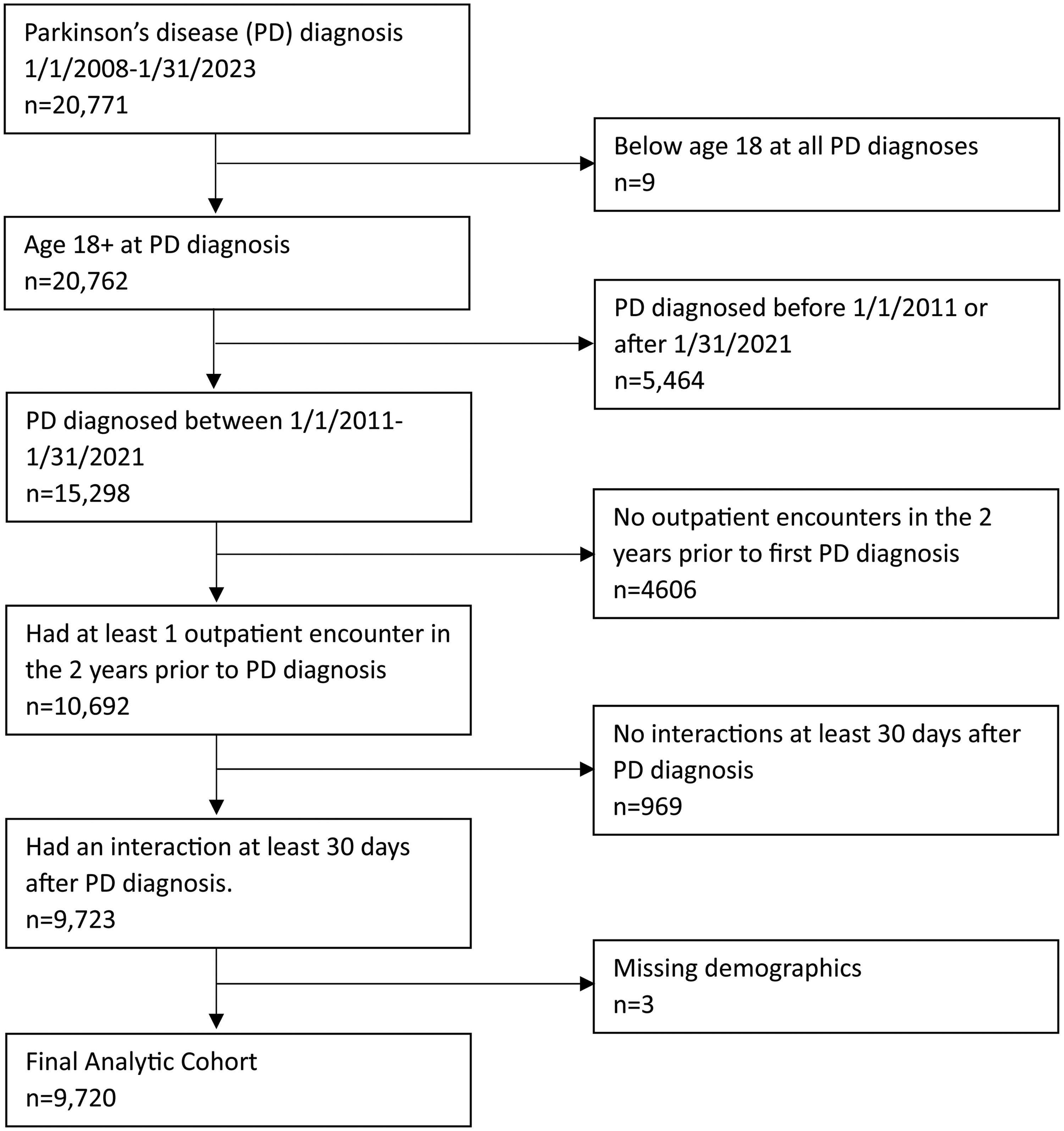
Cohort inclusion flow diagram.
Variable definitions
The outcome of interest was the receipt of a physical therapy or occupational therapy CPT code within 2 years of PD diagnosis. For this exploratory analysis, multiple independent variables were defined and examined. Demographics included age at PD diagnosis, sex, and self-identified race. Charlson Comorbidity Index was defined at time of PD diagnosis. Medications of interest were antiparkinsonian medications and were categorized into the following classes: dopamine replacements, dopamine agonists, and MAOB inhibitors. Placement of deep brain stimulator was defined using CPT, ICD-9 procedure, and ICD-10 procedure codes. Detailed definitions for all variables are included in Supplemental Material 1.
Analysis
Bivariate associations were tested for using Student's t-tests for continuous variables and Chi-square and Fisher's exact tests for categorical variables. Unadjusted and adjusted logistic regression models were computed to estimate the association between therapy receipt and each covariate. Measures of association were expressed as odds ratios and 95% confidence intervals. Sensitivity analyses were conducted for receipt of PT and OT individually to determine if factors differentially associated with PT compared to OT utilization. These results are presented in Supplemental Material 2. However, these PT and OT specific models were not substantively different from each other or the combined PT and OT model, as such the combined approach is presented and utilized for the subsequent analyses. Longitudinal trend in PT/OT utilization was first analyzed using Joinpoint Regression, 23 which identifies statistically significant changes in a linear trend. However, no significant join points were found, so linear regression was utilized for the analysis of therapy receipt by year. Alpha of 0.05 was used for all tests and SAS v9.4 (Cary, NC) was used for all analyses.
Results
The average age for this cohort of newly diagnosed PD patients was 72.4 (SD 11.3) years and the average Charlson Comorbidity Index was 2.2 (SD 2.5) (see Table 1). Patients were more commonly male gender (53.8%) and White race (88.4%). Almost half of our cohort received dopamine replacement therapy prior to the end of the 2-year follow-up period (44.5%). Dopamine agonists (7.1%), MAOB inhibitors (3.5%) and deep brain stimulators (0.2%) were much less common. Overall, 36.9% of the cohort (n = 3586) received either physical or occupational therapy within two years of receipt of PD diagnosis.
Summary of cohort characteristics overall, and by physical therapy or occupational therapy receipt within two years.
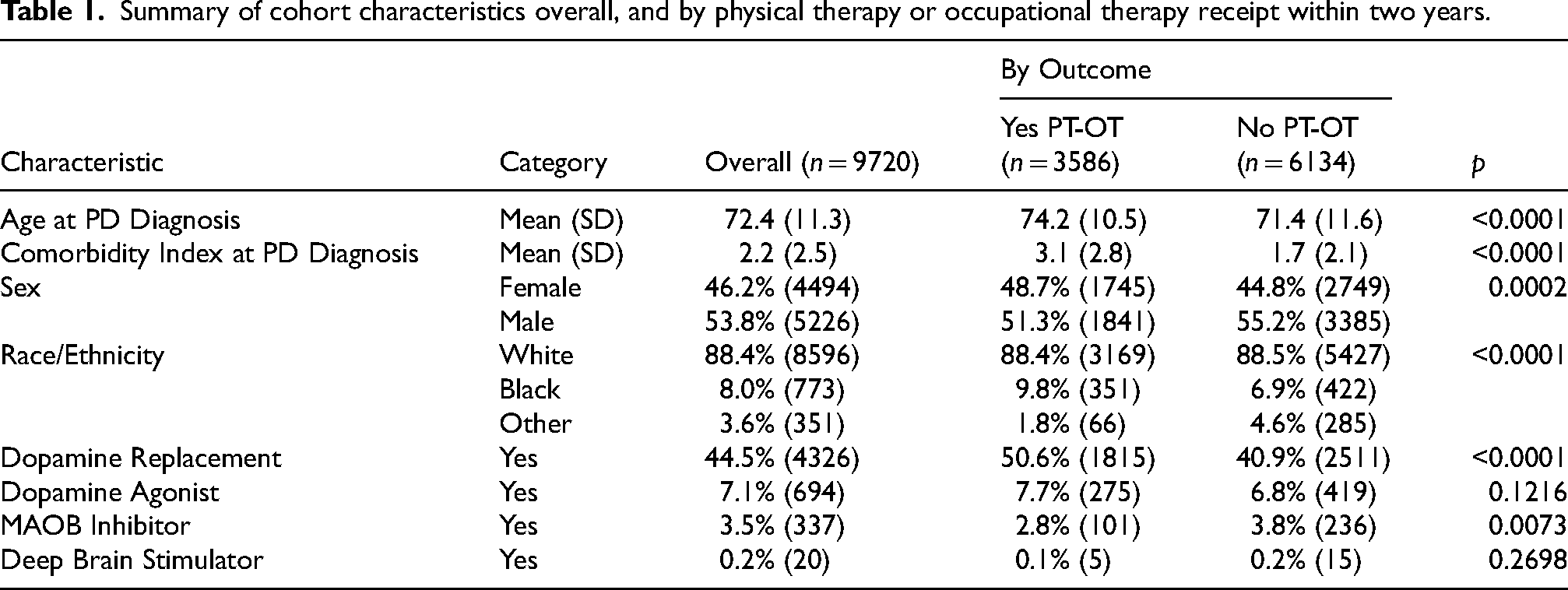
Of these factors described above, only dopamine agonist medication and deep brain stimulator placement were not significantly associated with receipt of therapy within 2 years of PD diagnosis (p = 0.1216 and p = 0.2698, respectively). Those receiving therapy were older (74.2 vs. 71.4, p < 0.0001) and had more comorbidities (Charlson Comorbidity Index of 3.1 vs. 1.7 (p < 0.0001). Female gender (p = 0.0002) and African American race (p < 0.0001) were disproportionately represented in those receiving therapy. A higher proportion of those receiving therapy also received dopamine replacement therapies (50.6% vs 40.9%, p < 0.0001) while a lower proportion of those receiving therapy also received MAOB inhibitors (2.8% vs 3.8%, p = 0.0073).
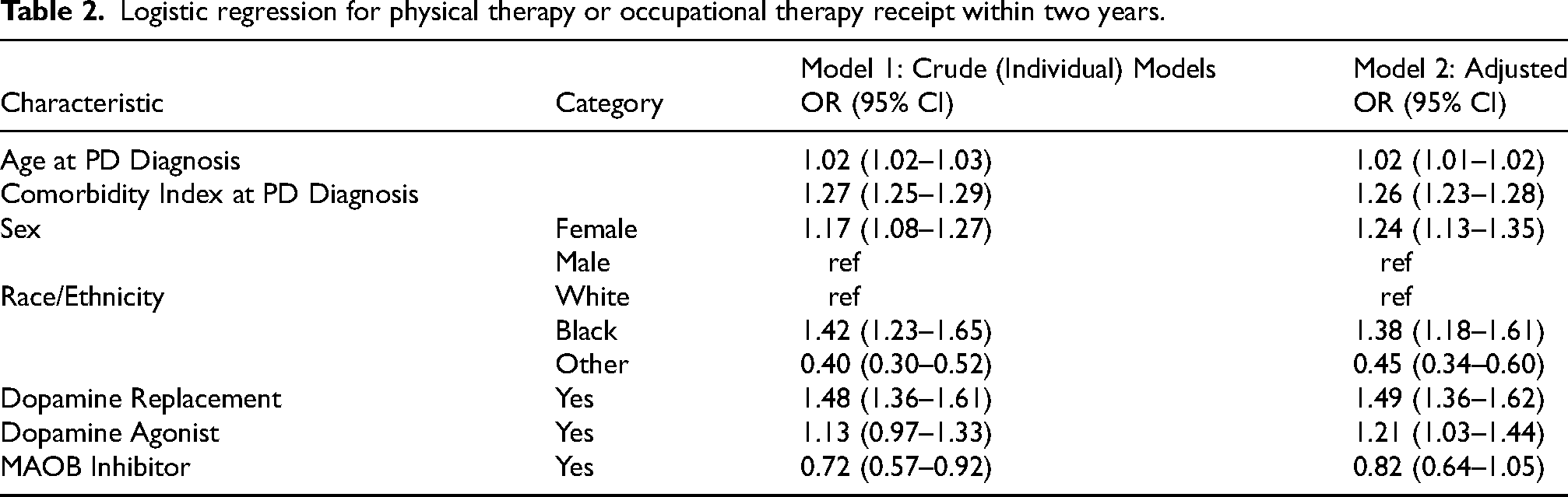
Logistic regression was used to quantify the association between therapy receipt and patient characteristics. Because the crude and adjusted models provided similar point estimates (see Table 2), the adjusted results will be discussed here. The strongest association with therapy receipt was seen for dopamine replacement therapy, with 49% higher odds of dopamine replacement therapy among those receiving PT or OT (OR 1.49; 95% CI: 1.36–1.62). Compared to white race, African American race displayed a similarly strong association with therapy receipt (OR 1.38; 95% CI: 1.18–1.61) while any other race showed significantly lower odds (OR 0.45; 95% CI: 0.34–0.60). Increasing age, higher comorbidity index, and female gender were all positively associated with PT or OT receipt (see Figure 2).
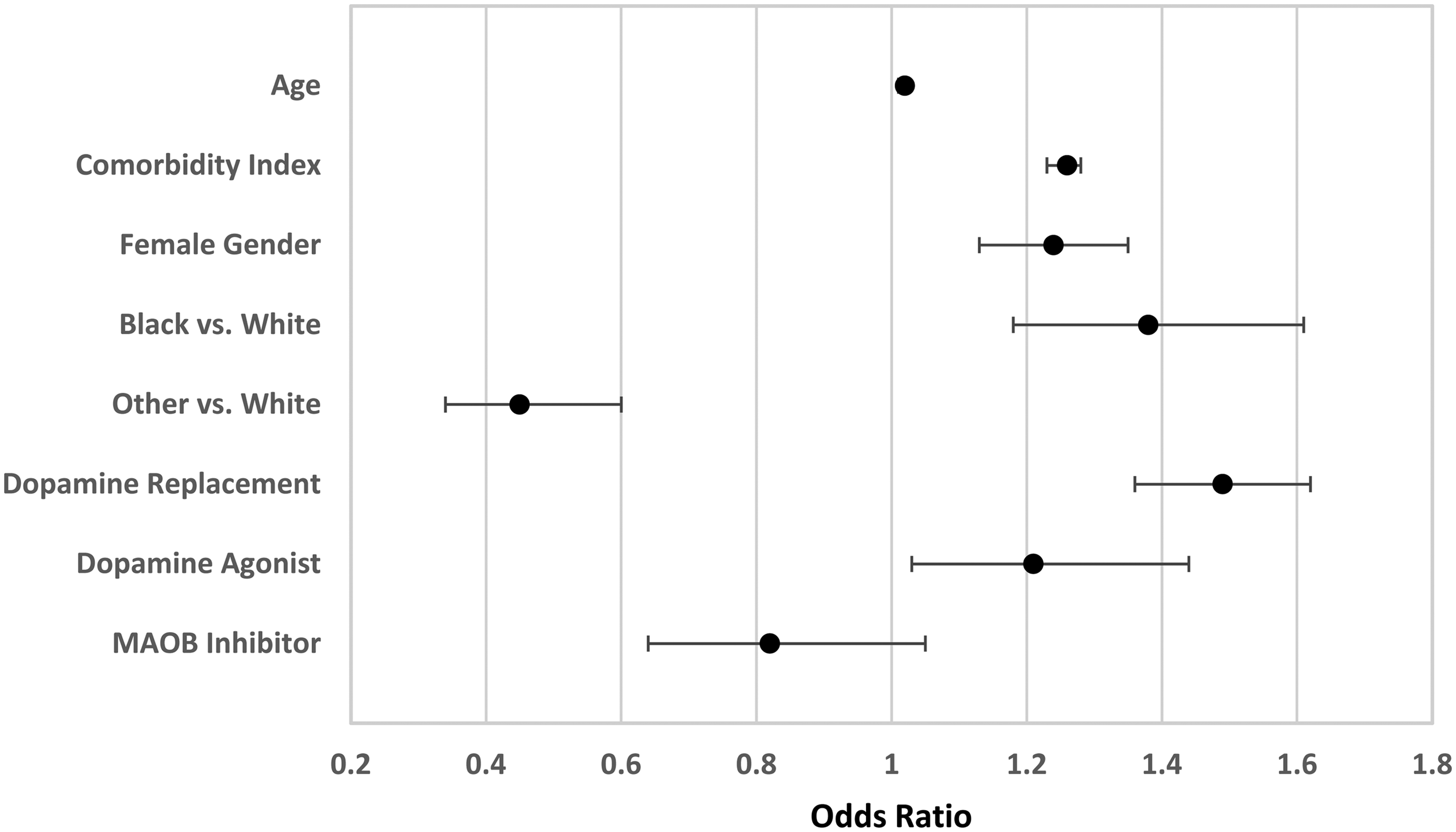
Forrest plot of adjusted odds ratios for PT or OT receipt presented as mean and 95% confidence interval.
Logistic regression for physical therapy or occupational therapy receipt within two years.
Notably, in 2011 and 2012, the number of new PD diagnoses and the rate of therapy receipt was substantially lower than the remaining years (see Table 3). This coincides with the electronic health record becoming fully integrated into the healthcare system. Because of this, the analysis of the trend in therapy receipt excluded 2011 and 2012 because these two years were systematically different than the remaining observation period. Additionally, because of this concern over the first 2 years of data, a sensitivity analysis was conducted in which the first two years (2011 and 2012) of the cohort were removed. No changes in statistical significance were observed, and changes in point estimates and confidence intervals were minimal. Results of this sensitivity analysis are included in Supplemental Material 3.
Receipt of physical therapy (PT) or occupational therapy (OT) receipt by year of PD diagnosis.
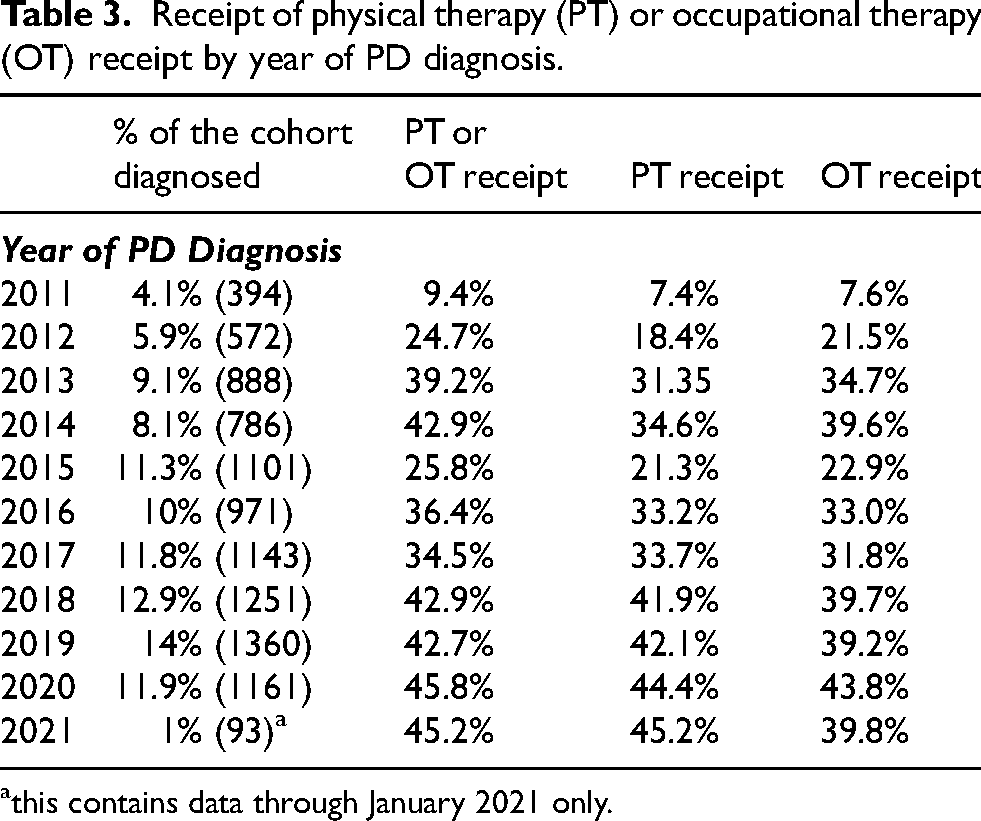
this contains data through January 2021 only.
In the analysis of longitudinal trend, the regressed results showed a statistically significant (p < 0.001) average increase of 1.4% between 2013 and 2021. Starting in 2013, the observed rate of therapy receipt was 39.2% and ended at 45.2% in 2021. By contrast, the regressed rate was 32.2% in 2013 and 43.3% in 2021. Figure 3 displays the observed and regression estimated rates of therapy receipt by year. Despite the observable reduction in rehabilitation utilization in 2015, no statistically significant changes in trend (join points) observed.
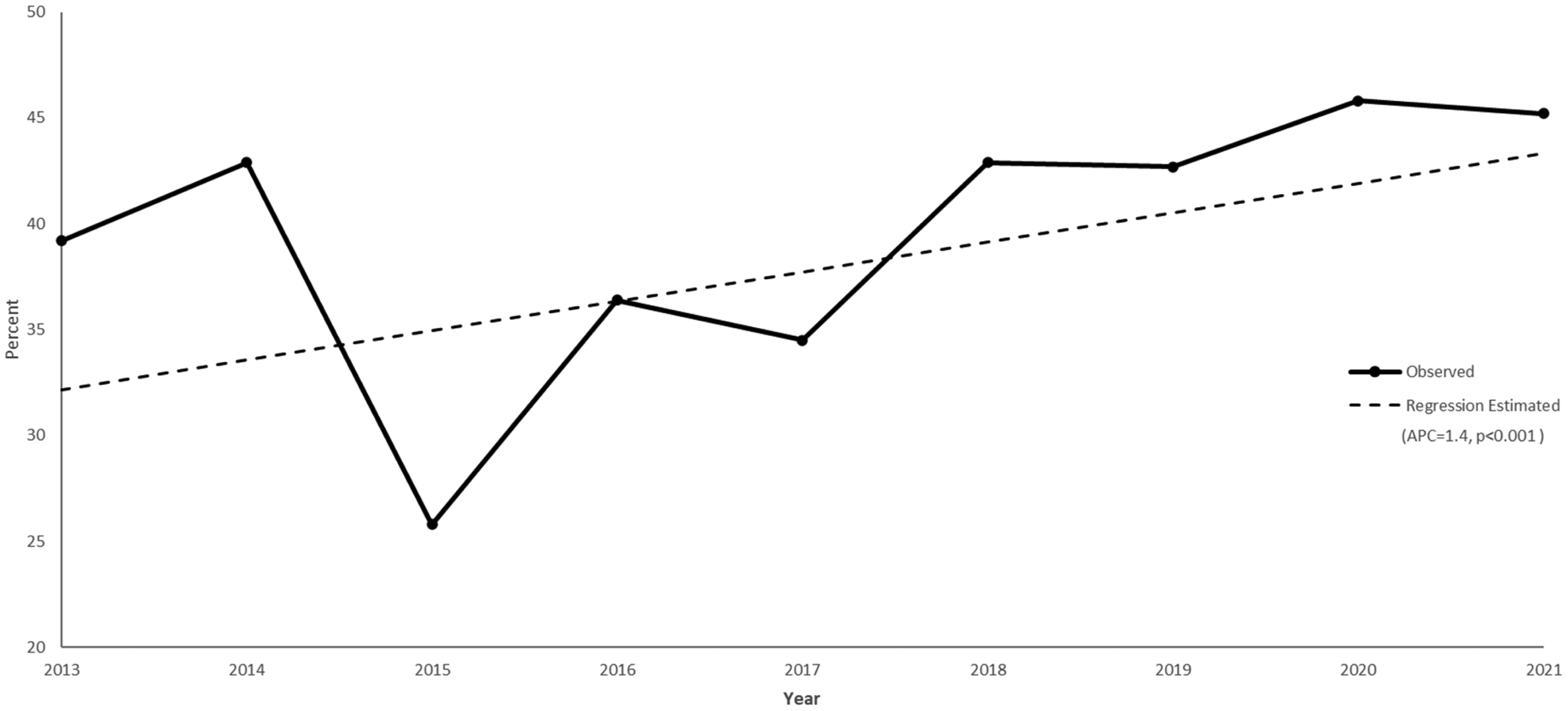
Plot of linear trend in physical and occupational therapy utilization from 2013 to 2021.
Discussion
The findings of this study indicate that nearly 37% of individuals utilized PT or OT services within two years of receiving a PD diagnosis at a large midwestern health system in the United States. This differs from the findings of previous studies. Most notably, Fullard and colleagues conducted a study of Medicare beneficiaries with PD between 2007 and 2009 which found that only 14.2% of the 174,643 patients with PD included utilized outpatient rehabilitation services. 10 More recently, Roberts and colleagues investigated referral patterns at 29 Parkinson's Foundation Centers of Excellence between 2016 and 2018. They found that among 5020 patient records only 25.1% had been referred to rehabilitation service providers. 9 While both studies used similar statistical methods to the current study, it should be noted that Roberts et al. investigated referral to rehabilitation services over 2-year period, and that Fullard et al. investigated utilization of rehabilitation services over a 3-year period. Additionally, these studies also included individuals with more advanced PD than those in the current study. Given current best practice recommendations, supported by scientific evidence, that all patients with PD be provided rehabilitation care,6–8 the findings of this study provide encouraging evidence showing of a meaningful step forward in the utilization of rehabilitation services among patients with PD. Additionally, this study differed from previous in investigating exclusively rehabilitation utilization in early PD, within two years of receiving a diagnosis of PD. The findings of this study in considering this aspect of the study cohort provide evidence that utilization of rehabilitation services may be higher early in the disease progression, in contrast to findings of Roberts et al., 9 when symptoms are milder, disability and carer burden is less pronounced, and individuals may have more potential for maintaining functional and neuroplastic changes incurred during rehabilitation.5,12,13,24,25 While promising, given that this study utilized a sample limited to individuals within two years of receiving a PD diagnosis, it may underestimate the utilization at later stages of the disease when disability and rehabilitation needs become more prominent. However, this requires further investigation.
Unique from prior studies, this study included an analysis of the longitudinal trends of utilization of PT and OT services. This analysis found a 1.4% year over year increase in utilization of PT and OT services between 2013 and 2021 for the cohort. While specific to this cohort, this study offers the first evidence of a longitudinal increase in utilization of rehabilitation services among patients with PD. The timing of the observed increases in utilization coincides with the publication of several updated care guidelines for patients with PD that included strong recommendation regarding rehabilitation services, as noted previously,6,7 though the analyses did not identify any particular increase that appear to specifically relate to practice change at the time of publication of these recommendations. These findings, when paired with the increase in overall utilization/referral rates for rehabilitation services over time observed when comparing the results of Fullard et al. in 2009 (14.2%), Roberts et al. in 2018 (25.1%), and this study in 2021 (as much as 45%), provides strong evidence for increasing utilization of rehabilitation services.9,10 Despite these encouraging findings, their remains a large gap between recommendations and clinical practice that represents opportunity lost. 12
As a secondary aim, this study investigated factors that were associated with utilization of PT and OT services. This study found that comorbidity burden, PD medication type, sex, race, and age were all related to utilization of PT and OT services for individuals within two year of receiving a PD and received care at SSM health system. Notably, the findings indicated no difference in factors associated with receipt of PT compared to OT services. Regarding racial differences, patients that were African Americans were most likely to receive PT and OT services (adjusted odds ratio (AOR) = 1.38), followed by white (reference), and lastly other racial groups (AOR = 0.45). These findings differ widely from those of Fullard et al. which showed lower utilization of PT and OT services by those of African American races (AOR = 0.63). 10 Conversely, utilization among those of “other” racial groups was lower than the findings of Fullard et al. (AOR = 0.97). 10 Notably, the sample of the current study included a larger proportion of patients of African American race (8.0%) compared to Fullard et al. (4.1%). Additionally, the current study utilized data from 2011 to 2021 whereas Fullard et al. utilized data from 2007 to 2009. Considering these differences in proportion and timing together, it is possible that increases in societal awareness of race-related health disparities in combination with the larger portion of African American patients in this study may have influenced provider attitudes toward recommendation of rehabilitation services. Regardless, there was large difference in rehabilitation utilization among African Americans in the study (45.4%) compared to Fullard et al. (7.8%). 10 This finding is quite striking and requires further investigation. The findings of this study indicate that female patients had increased odds of utilization of PT and OT services by 24% (AOR = 1.24), different from Roberts et al. which found roughly no difference in referral pattern for males versus females (AOR = 0.97), but similar to Fullard et al. which observed slightly higher utilization in females (AOR = 1.06).9,10 This study observed similar to the findings of Roberts et al. that comorbidities increased utilization of rehabilitation services. Roberts et al. found a 19% increase in utilization for patients with greater than two comorbidities, whereas this study observed a 26% increase in utilization of rehabilitation services per comorbid condition. 9 Unique from prior studies, this study also investigated the relationship between class of antiparkinsonian medication and rehabilitation utilization, finding that those on dopamine replacements (AOR = 1.49), and dopamine agonists (AOR = 1.21) were more likely to utilize PT and OT services. However, those on MAO-B inhibitors were 18% less likely to utilize PT and OT services. Best practice guidelines and evidence suggests that optimal care include both pharmacologic therapies as well as rehabilitative care.6–8 This study indicates that individuals who did not receive PT and OT may not have benefited from aggressive pharmacologic intervention. Alternatively, when considering this finding with the finding that the presence of more comorbidities and older age increased the odds of utilization of rehabilitation services and that MAO-B inhibitors are often utilized early in the course of disease when PD symptoms are minimal, it is possible that rehabilitation utilization was dominantly following a tertiary prevention model, care for those with overt disability, rather than a secondary prevention model, where individuals with subclinical or mild evidence disease may benefit from PT/OT. This may indicate that despite evidence-based recommendations for earlier rehabilitation care, following a secondary preventive model, that the focus of referral and utilization of rehabilitation services has not shifted to those with minimal to no disability. Taken together, these findings provide insight into factors that influence PT and OT service utilization among individuals with PD.
While the findings of this study are encouraging, they should be viewed in the context of its limitations. Notably, this study utilized data from a single health system in the midwestern United States, which may not represent other health systems within the United States or in other regions of the world. Additionally, this study reports data from electronic health records, which may be incomplete. The health system completed a mandatory transition to electronic health records across their system by 2013 with outpatient services being the last services to complete the transition. Thus, data before 2013 may under report utilization of PT and OT services. A sensitivity analysis was conducted by removing years 2011 and 2012 from the logistic regression analyses and no significant differences from the substantive analysis were observed (Supplemental Materail 3). Additionally, data from 2011 and 2012 were excluded from the longitudinal trend analysis. Data for reported for the year 2021 include only data through January 31 as data was extracted in February 2023 and required two prior years of existing data. Data from 2021 should be interpreted cautiously as it represents a much smaller sample than prior years (i.e., 2021: n = 93 compared to 2020: n = 1161). Further, the findings should be interpreted with caution as the current study included the smallest geographical region (five midwestern states) compared to the Fullard et al. study that was inclusive of all 50 states, and the Roberts study which included 23 PD expert care centers from 4 countries.9,10 Lastly, while prior studies investigated utilization or referral across all rehabilitation services (PT, OT, and speech therapy),9,10 this study investigated only PT and OT services. This places this study at risk of again underreporting rehabilitation service utilization compared to prior studies that investigate utilization across any of the three rehabilitation services.
Conclusions
It is well established that early physical rehabilitation decreases PD symptomology, improves motor and functional outcomes, and can improve quality of life among individuals with PD. Given this, previous studies show a disturbing lack of utilization of PT and OT services. This study shows an increase in utilization of PT and OT services over previous reports and longitudinally, however it continues to convey how far clinical practice continues to lag behind best practice and scientific recommendation.
Supplemental Material
sj-docx-1-pkn-10.1177_1877718X241291991 - Supplemental material for Increasing trends in utilization of physical and occupational therapy services in early Parkinson's disease
Supplemental material, sj-docx-1-pkn-10.1177_1877718X241291991 for Increasing trends in utilization of physical and occupational therapy services in early Parkinson's disease by Jason K Longhurst, Timothy Chrusciel and Syed O Ahmad in Journal of Parkinson's Disease
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by the Institute of Clinical and Translational Science (ICTS) at Washington University, award designation JIT948. Research reported in this publication was supported by the Washington University ICTS grant UL1TR002345 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official view of the NIH.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The authors do not have permission to share these data per data use agreements.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.