
Abstract
Aim
With medical advances, children with spinal muscular atrophy (SMA) now survive. Literature reporting on SMA rehabilitation approaches before and after disease-modifying treatments has not been reviewed.
Method
Five databases and grey literature were systematically searched for pediatric reports with a SMA rehabilitation focus, published between 2000–2024. Two independent reviewers screened titles and abstracts; a third reviewer resolved disagreements. Rehabilitation interventions and outcomes were extracted and coded using the International Classification of Function (ICF) Category Tool and analysed using the ‘F-words for Childhood Disability’ as an interpretive framework.
Results
With duplicates removed, 2621 reports were screened, 268 reviewed and 71 retained for detailed extraction. Authors described interventions directed at impairment (50%), functioning (15%), participation (8%), and environmental (27%) domains. Rehabilitation outcomes focused on impairment (42%), functioning (43%), participation (9%), and quality of life (6%) outcomes.
Interpretation
There is a trend in SMA rehabilitation to address impairments with hopes of translation to functional gains. Recommendations include applying the F-words framework, using individual goal-directed multi-disciplinary approaches, and considering the voices of children and families to broaden and re-imagine SMA rehabilitation.
Protocol Registry
Open Science Framework (https://osf.io/w47m8/)
This is a visual representation of the abstract.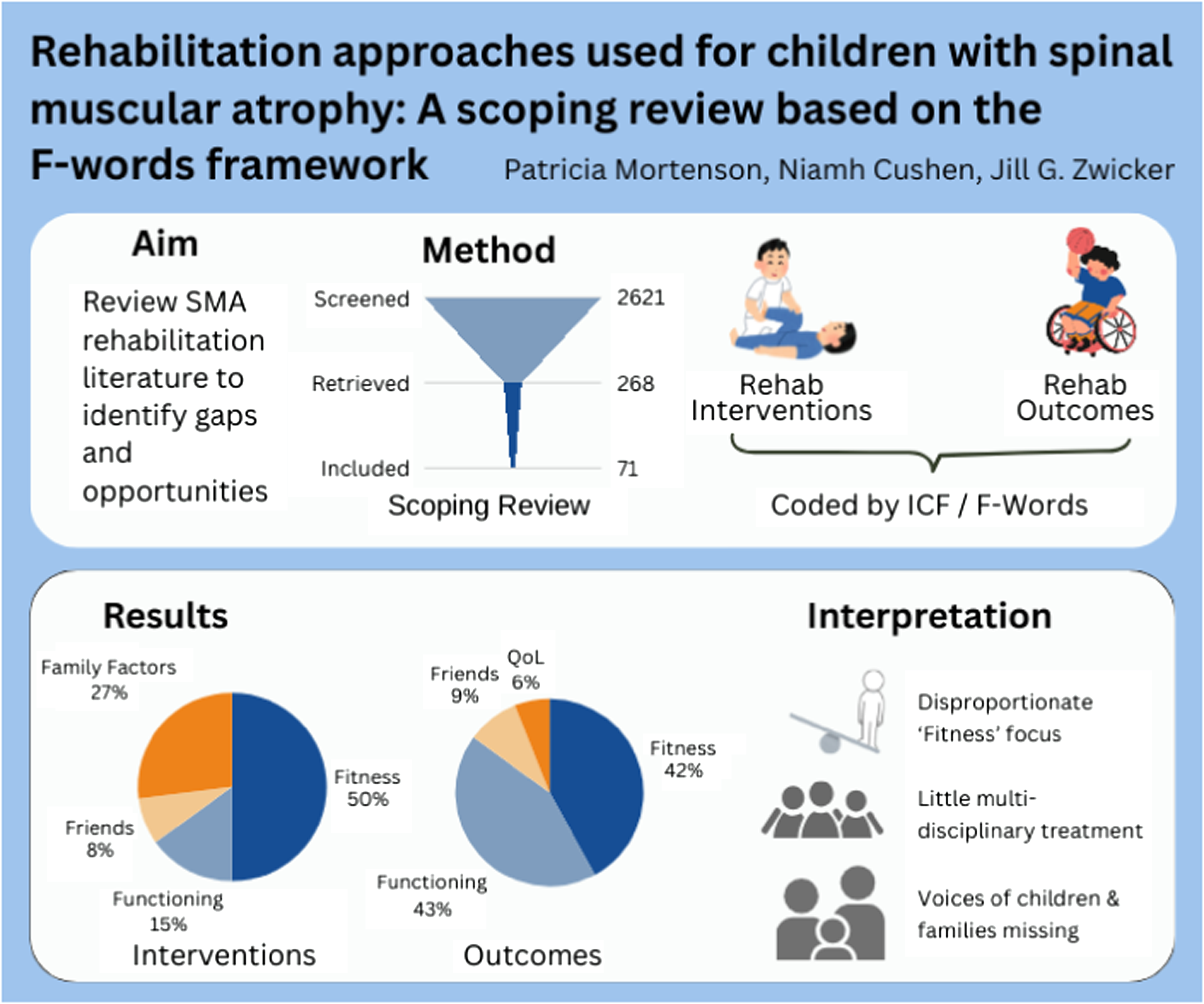
What this paper adds
SMA rehabilitation disproportionately focuses on impairment over functioning and participation
The ‘F-words for Childhood Disability’ framework can be applied to new understandings of SMA rehabilitation
Child and family voices are not well-represented in SMA rehabilitation
There is potential for broader multi-disciplinary approaches in SMA rehabilitation
Spinal muscular atrophy (SMA) is a rare neuromuscular condition, with reported incidence ranging from 1 in 8000 to 1 in 20,000 births depending on ethnic population. 1 SMA was once one of the most common genetic causes of infant death, 2 but with recent medical advances, families have hope for a brighter future. 3 SMA causes progressive muscle weakness and associated disability following previously predictable trajectories. 4 Disease modifying treatments (DMTs) (pharmacologics nusinersen and risdiplam, and gene replacement therapy onasemnogene abeparvovec-xioi), newborn screening (NBS), and early and dual treatments are rapidly changing the course of SMA.5–8 Children are not only surviving, but maintaining and gaining motor skills, such as sitting and, for some, standing and walking.8–10 However, children continue to live with varying levels of disability, depending on genetic expression, timing of diagnosis, availability of therapeutics, and discomforts of ongoing treatment.11,12
To date, SMA research has primarily focused on medical therapeutics, ‘burden’ of care, and impact on quality of life (QoL). Despite rehabilitation being a part of the 2007 and 2018 SMA standards of care (SOC),13,14 there is a paucity of substantive rehabilitation research.15,16 Traditionally, SMA rehabilitation consisted of an ‘accommodation’ approach, supporting daily living by addressing barriers and providing adaptive equipment and positioning. 13 This is now shifting towards active ‘remediation,’ with expectations for improvements in skill and function.16,17 With no consolidation of evidence, however, rehabilitation professionals and families have little to guide their clinical decisions. 15 A scoping review would provide consolidated information of past and current rehabilitation approaches to guide the future. The objectives of the review, therefore, were to (1) assemble, classify, and interpret the available literature regarding rehabilitation strategies and approaches used with children and youth with SMA, both pre and post new DMT using a holistic, child-centred framework; and (2) identify gaps in knowledge and practice.
Method
The protocol for this scoping review followed the methods outlined by Levac et al. 18 and the JBI Manual for Evidence Synthesis. 19 This included the following steps: (1) defining the question; (2) identifying relevant evidence; (3) selecting the evidence; (4) extracting and charting the data; and (5) collating, summarizing and reporting the results. The review protocol was registered on Open Science Framework on October 9, 2022 (https://osf.io/w47m8/).
Step 1: define the question
The guiding population, concept, context (PCC) question was: What rehabilitation approaches are used for children and youth with SMA, both before and after new DMTs?
Population
The population of focus was children and youth aged 0–18 years of age living with SMA types I, II, or III (non-sitters, sitters, walkers).
Concept
Rehabilitation is complex, occurring in multiple settings, conducted by different professionals, using a variety of processes and modalities to achieve a divergency of aims. 20 For research purposes, Meyer et al. proposed defining ‘rehabilitation’ as the processes and methods used to develop goal-focused strategies to optimize function, social participation, and self-determination. 20 By integrating the biomedical, social, and environmental determinants of disability, the International Classification of Functioning, Disability and Health (ICF) 21 fits well with this holistic and complex definition of rehabilitation. The ICF framework has demonstrated applicability for children with SMA 22 and is particularly relevant to the objectives of this review. The ‘F-words Framework’ 23 re-imagines the ICF domains to focus on six childhood disability factors: ‘Fitness,’ ‘Functioning,’ ‘Friends,’ Family,’ ‘Fun,’ and ‘Future.’ For the purpose of this scoping review, rehabilitation was operationalized within the Meyer et al. definition and ICF/F-words framework to include approaches and interventions conducted or supervised by rehabilitation professionals (e.g., physical therapists, occupational therapists, speech-language pathologists) to support or maintain ‘Impairments’ (in ‘Body Structures and Function’/‘Fitness’); address ‘Limitations’ in mobility, self-care, learning, and development activities (‘Activities’/‘Functioning’); mitigate ‘Restrictions’ in play, recreation, and social participation (‘Participation’/‘Friends’); and assist with transition to future growth and adult lives (‘Future’), while considering ‘Personal’ (‘Fun’) and home and community ‘Environmental Factors’ (‘Family’). An ‘approach’ was defined as an overall framework that informs the specifics of what and how rehabilitation is delivered and measured (‘motor learning,’ ‘child-directed,’ ‘multi-disciplinary,’ etc.), while an ‘intervention’ was defined as the specific technique or modality applied with a patient. 24
Context
The context of this review was the changing prognostic course for children with SMA. This review bridged rehabilitation evidence both before and after the availability of DMTs.
Step 2: identify relevant evidence
An iterative, three-step search strategy was used to search the peer-reviewed literature, as described in the JBI Manual and in consultation with an experienced medical librarian. First, initial searches were conducted in Ovid MEDLINE and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases to identify text words in titles, abstracts, and indexes. Second, a detailed search of all planned databases (Ovid MEDLINE and Epub Ahead of Print, CINAHL [via EBSCOhost], Embase [Ovid], PsycInfo [via EBSCOhost] and the Cochrane Library of databases through Ovid Evidence-Based Medicine Reviews [EBMR]) was conducted using all identified keyword and controlled vocabulary terms (see Supplemental Table S1 for search strategies and dates). Third, the reference lists of eligible papers were examined. Finally, three sources of grey literature (conference abstracts, graduate theses and dissertations, and clinical documents) were searched in Embase and MEDLINE (MeSH headings “congresses"[Publication Type] OR “congresses as topic"[MeSH Terms]), ProQuest Dissertations and Theses Global, and the Trip database, as well as on SMA neuromuscular organization websites. 25
Step 3: select the evidence
The following inclusion criteria were applied: (1) paediatric SMA as a distinct part or sole composition of the population focus (aged 0–18 years); (2) a focus on rehabilitation practices, interventions, or approaches (as defined above); and (3) published or produced between January 01, 2000 – January 06, 2025. Original records were described in accordance to the definition given by Page et al., 26 with the term report being used to refer to any document type providing relevant information.
Published works of quantitative, qualitative, and mixed-methods studies, as well as case studies, practice statement and practice guideline papers, editorials, conference proceedings, and graduate theses were included. Exclusion criteria included reports with a focus on (1) QoL as the prime construct; (2) measurement use and development; (3) economic discussions of care or ‘burden’; (4) medical and pharmaceutical interventions and treatments; and (5) narrative review and summary (with those reference lists scanned to ensure inclusion of original cited works in the review).
All citation records were exported to Zotero open-source citation management software 27 and to the Covidence platform. 28 Two reviewers (PM, NC) independently screened the titles and abstracts for eligibility, with disagreements resolved by a third reviewer (JZ). As described by Peters et al., 19 a pilot test of the selection process was conducted by PM and NC over a random sample of 25 articles. A title and abstract screening agreement goal of 75% was achieved (initial agreement = 92%). Discrepancies were discussed and modifications made to the criteria; a decision was made to exclude respiratory physiotherapy articles (adjusted screen agreement = 93%, final review agreement = 94%). Full article screening occurred in the same manner (screen agreement = 84%, final agreement = 86%). Authors were contacted for further details as needed, and an online translation app was used for non-English reports.
Step 4: extract and chart the data
One reviewer (PM) extracted the data, which was captured on a shared Microsoft Excel® for Microsoft 365 (version 2407) spreadsheet and verified by a second reviewer (NC). Extraction data included use of DMTs, overarching rehabilitation approaches if and as explicitly reported, interventions, measured or desired outcomes, and rehabilitation service(s) involved. Related records (for example, a protocol paper for a subsequently published study, an editorial commentary of a paper, a conference presentation of a published work, and an update of a previous standard or report) were merged and the more recent or higher evidence level was chosen as the primary report.
Step 5: data analysis and presentation of results
The Modernized ICF Online Browser was used to code the type or focus of intervention and the goal or outcome measured for reported rehabilitation practices. 29 Interventions and outcomes crossing domains were coded to each relevant domain. As QoL as a construct does not fit neatly into the ICF, when listed as a measured outcome, QoL was extracted separately. 30 One reviewer (PM) completed this detailed content analysis and ICF coding, confirmed by a second reviewer (NC). Visual presentation of the ICF/F-words framework coded frequencies enabled identification of patterns, and the strengths and gaps in current SMA rehabilitation practice. Four patient-partners (three young adults with SMA and a parent of an adolescent with SMA involved as co-investigators in a related qualitative research project) provided experiential insights and feedback on the analysis and recommendations during virtual group project meeting calls.
Results
Selection of articles and abstracts
Results of the database searches and selections are outlined in the PRISMA flowchart (Figure 1). Thirteen authors and one study protocol e-mail were contacted for further details; eight responded and those reports are included with the additional information from authors.31–38 Overall, 71 citations met the inclusion/exclusion criteria, consisting of journal articles (n = 52), conference abstracts (n = 17), and letters to the editor (n = 2), with three works translated from other languages (Supplemental Table S2 for details).
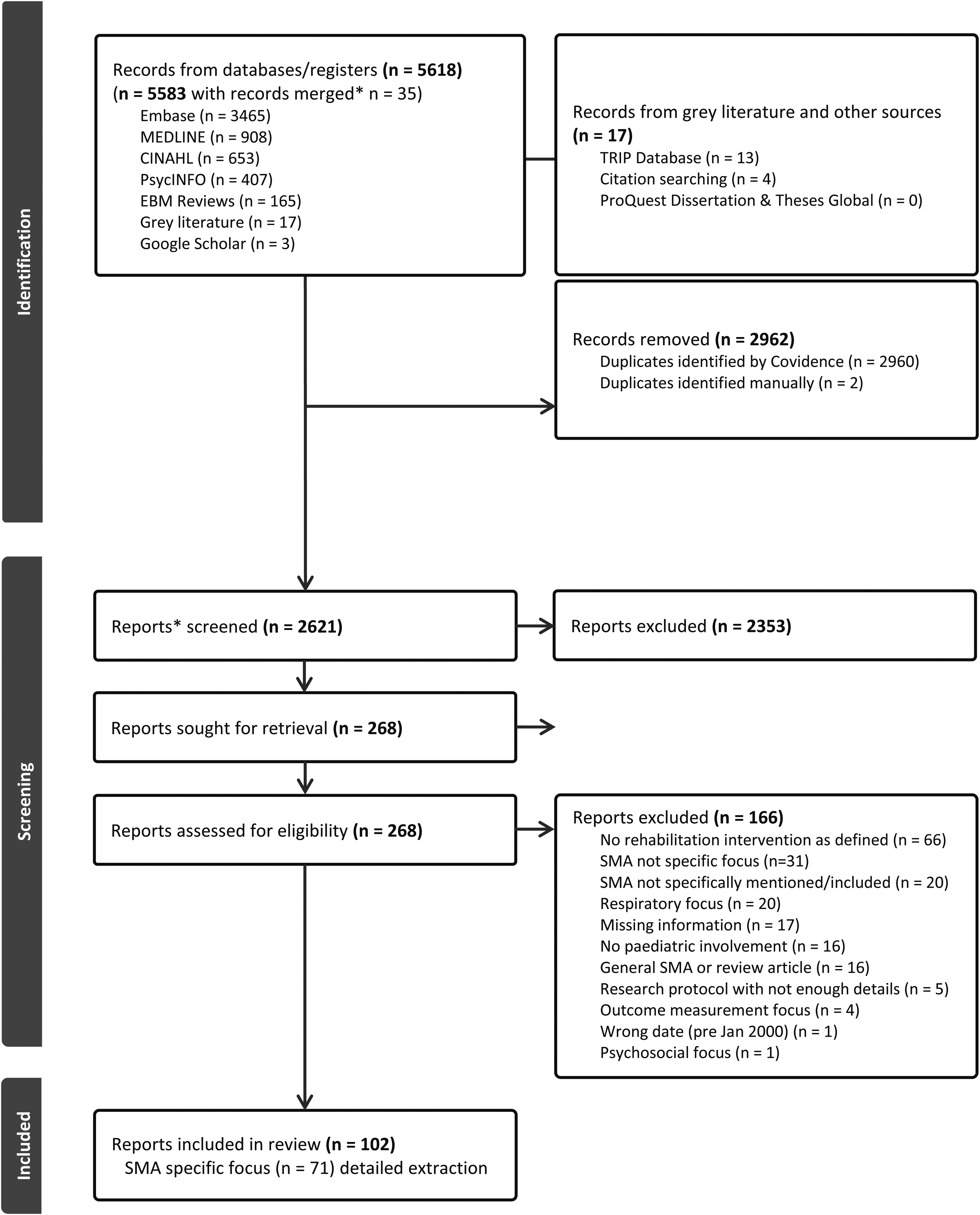
Preferred reporting items for systematic reviews and meta-analyses flowchart showing reference selection process.
Characteristics of articles and abstracts
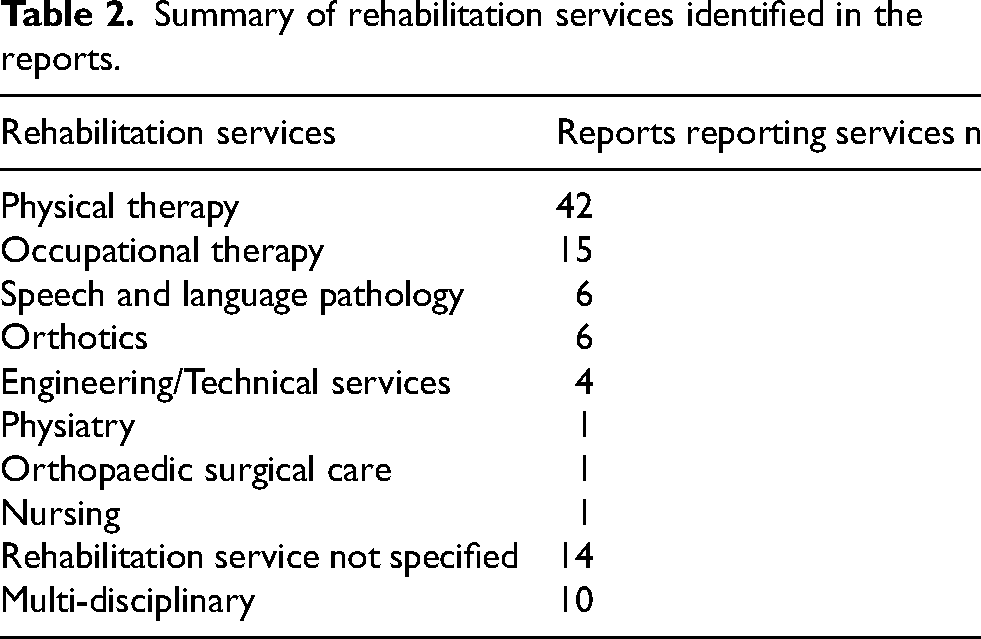
Year, type, and country of reports are described in Table 1 and Supplemental Table S2, including categorization by years when DMTs and gene therapy became available. Twenty-seven authors received funding from not-for-profit, educational, or government organizations/institutions, nine were unfunded, and 34 omitted a funding statement. Pharmaceutical companies of SMA DMTs funded one study, 33 employed authors of another study, 39 and had previously reimbursed the salary of one author who served as a primary investigator for a different study trial. 35 Other potential conflicts of interest included paid employment by or funding from manufacturers/companies of the devices trialed,32,36,40–42 no cost provision of the trial device, 43 and product licensing and founding of a company to sell a trial device. 38 Sample sizes in research studies ranged from one to 361, with most studies having small numbers (n≤5 in 36 studies). When sex was reported, the total of male participants (n = 750) out-numbered female (n = 658). Rehabilitation services reported are summarized in Table 2; a ‘multi-disciplinary’ approach involving two or more services was reported by 10 authors. Of the few authors who specified a rehabilitation approach to support the choice and delivery of interventions, three used goal-directed motor learning approaches,42,44,45 two applied the ICF or F-words,22,38 and one reported neurodevelopmental theory (detail obtained from author contact). 31
General summary of reports, n = 71.
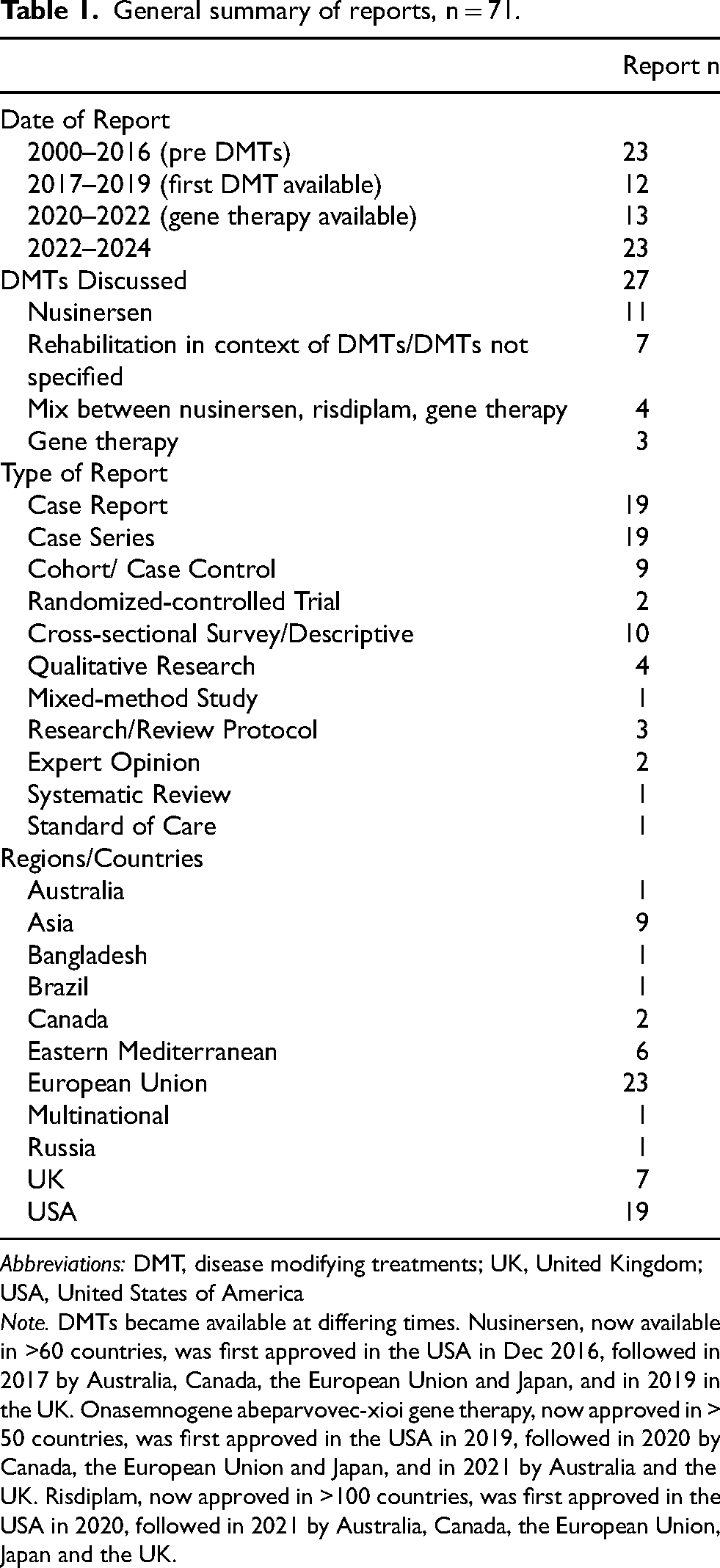
Abbreviations: DMT, disease modifying treatments; UK, United Kingdom; USA, United States of America
Note. DMTs became available at differing times. Nusinersen, now available in >60 countries, was first approved in the USA in Dec 2016, followed in 2017 by Australia, Canada, the European Union and Japan, and in 2019 in the UK. Onasemnogene abeparvovec-xioi gene therapy, now approved in > 50 countries, was first approved in the USA in 2019, followed in 2020 by Canada, the European Union and Japan, and in 2021 by Australia and the UK. Risdiplam, now approved in >100 countries, was first approved in the USA in 2020, followed in 2021 by Australia, Canada, the European Union, Japan and the UK.
Summary of rehabilitation services identified in the reports.
Rehabilitation interventions
The extracted rehabilitation interventions, frequencies of ‘use,’ and the categorized ICF/F-words domains are summarized in Figure 2 (Supplemental Tables S2 and S3 for extraction and coding details). Interventions ranged from simple, single-focused interventions (e.g., provision of orthotic trunk braces) to complex combinations of exercises (e.g., strengthening and balance exercises) or mixed exercises and functional activities (e.g., exercise and mobility programs).
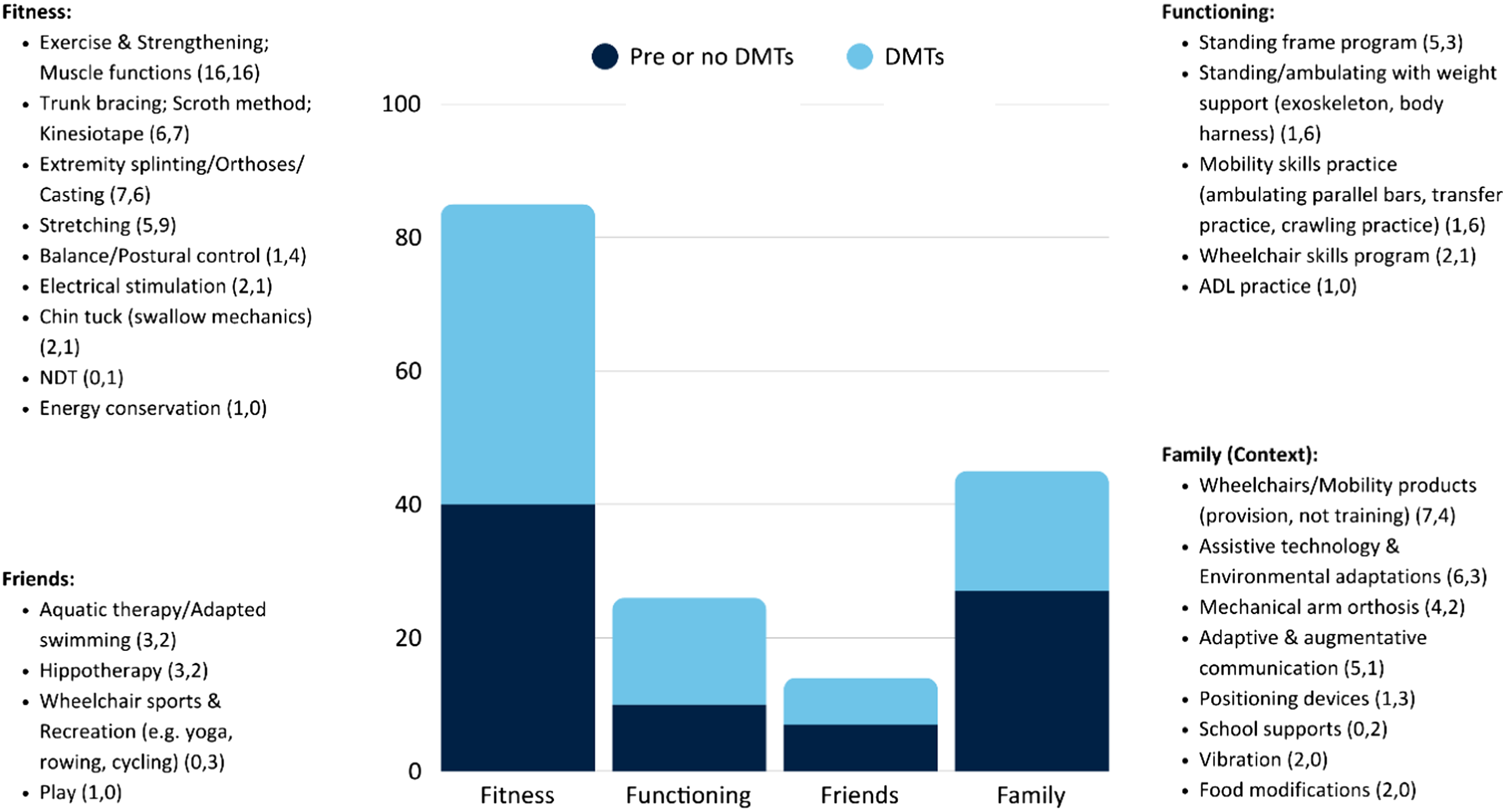
Rehabilitation interventions categorized by F-word domains (with frequency of citations before or with no DMTs mentioned, and with DMTs mentioned).
Interventions with a focus on remediation of ‘Fitness’ domain impairments of body structures and functions were the most frequently used or recommended for children with SMA (50% of total counted interventions). Of these, exercise and strengthening programs, such as cycle ergometer use and resistance training, were the most cited of any interventions (32/170 interventions; 19% of all interventions) with 31 of the 71 reports (44%) including an exercise intervention.13,16,22,31,34,38,39,42,44,46–67 “Aquatic therapy” when described as therapist-led exercises in water was classified as an exercise ‘Fitness’ level intervention and not as a social or an activity-focused intervention.44,51,61,62
With tallies combined, interventions directed at all other F-Word domains reached 50%. The use of environmental accommodations, classified under ‘Family’ (environment context), were the next most frequently reported type of counted intervention (27% total); this included the provision of mobility and assistive technology equipment and other home and school supports. Interventions using ‘Functioning’ domain level (activity-based) approaches (15% total) almost exclusively consisted of mobility programs (standing and mobility practice programs and wheelchair skills practice).13,16,22,41,42,45,46,49,52,55,58,59,63,64,68–76 One report mentioned activity practice in the self-care activity domain. 49 Finally, interventions supporting ‘Friends’ (participation in recreational and other community level activities) were limited to adapted swimming, hippotherapy, and adapted sports (8% total).13,22,42,46,48,49,77 None of these reports were intervention studies; they included surveys of use, case reports, and practice recommendation papers.
Four reports focused on ‘Fun’ (personal) factors. Flodin discussed the importance of personal preference in determining her daughter's standing position and mobility,78,79 Lemke at el. discussed personal meaning with hippotherapy, 77 Sugie and Sugie described a child's pleasure with adapted access to art, 80 and Iraqi et al. developed a video game specifically to support exercise therapy through gaming. 39 Supporting youth transition to ‘Future’ was indirectly discussed by Flodin, 78 but no reports specifically addressed supporting transition to future life roles and aspirations.
Rehabilitation outcomes
Identified outcomes for rehabilitation and the frequencies of ‘use’ are presented in Figure 3 (Supplemental Tables S2 and S3 for extraction and code details). Of the 71 total reports, four practice surveys addressed interventions only and did not mention specific outcomes.16,49,58,69 For the four qualitative studies, themes related to child experiences were extracted as the outcomes of interest. For example, Flodin reported three themes consistent with rehabilitation outcomes (comfort; accessibility in the world; social interactions). 78 Only two reports used a formal approach (ICF and F-words) to structure their outcomes.22,38 Three author groups reported individualized patient-identified outcomes.37,74,81 Twenty-seven reports used standardized assessments to quantify outcomes or self-report (Supplemental Table S3 for details).14,22,31,37,38,41–44,46,47,50,51,55–57,59,61,67,71,72,74,82–85 Three studies used individualized outcome measures, the Canadian Occupational Performance Measure 37 or the Goal Attainment Scale,74,86 and only one study protocol used a formalized measure of participation (‘Friends’), the Young Children's Participation and Environment Measure. 74 The remaining studies used a variety of observational or clinical outcomes, ranging from measured specifics of hip range of motion 75 to non-specified ‘motor function.’ 34
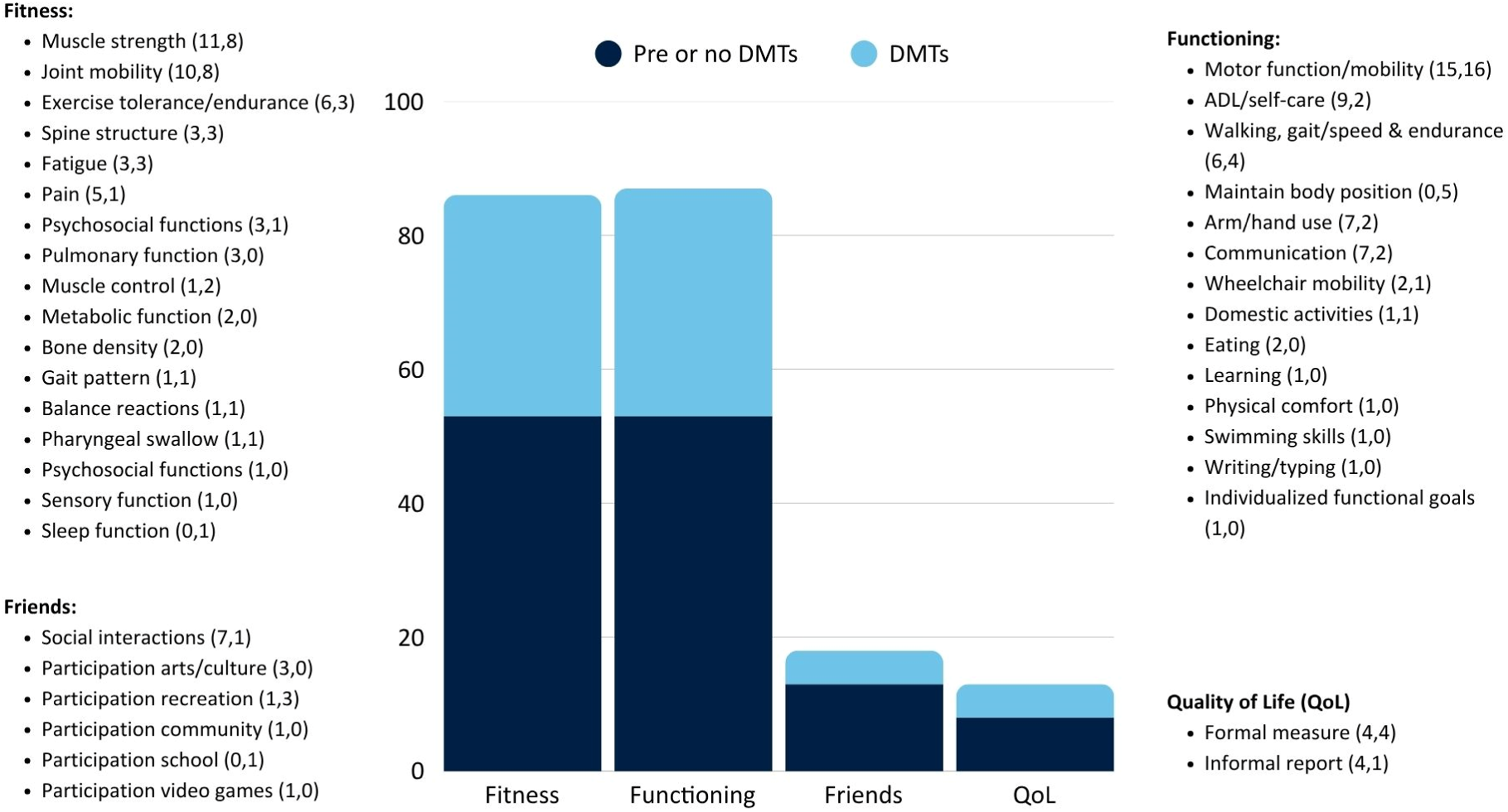
Desired outcomes of rehabilitation interventions categorized by F-word domains (with frequency of citations before or with no DMTs mentioned, and with DMTs mentioned).
In categorizing outcome domains by the F-words, there is a noticeable difference between the coding of ‘Fitness’ and ‘Functioning’ domains for interventions versus outcomes, with near equal representation between the two domains in outcomes (‘Fitness’ at 42% of total outcomes and ‘Functioning’ at 43%) (Figure 3, Table 3). However, 28 reports cited the use of ‘Fitness’-based interventions with hopes of translation to cross-domain improvements for ‘Functioning’ (Supplemental Table S2), for example, the use of strengthening and exercise programs to improve motor function/mobility.13,22,31,34,35,42,44,46,48,50,51,54,56,57,59,61,62,64–67,82,85,87–91 Three reports in this subgroup only used ‘Fitness’-based interventions and only reported ‘Functioning’ outcomes (e.g., they used exercises or braces and did not measure the corresponding muscle strength or limb structure or position)34,62,89 Twelve had a mismatch between the ‘Fitness’-based intervention used/recommended and the ‘Fitness’-based component(s) that were considered.13,31,44,46,51,56,59,61,64,65,67,85 Motor function/mobility was the most frequently measured or cited outcome of interest (Figure 3), with other ‘Functioning’ category outcomes, such as self-care, communication, and learning functions having a less frequent focus. A small number of reports considered the ‘Friend’ domain (participation) as an outcome for rehabilitation (8% of all counted outcomes), primarily for social and recreation participation, with only one report listing school participation. 22 ‘Quality of life’ was mentioned as a non-specified outcome in five reports55,62,83,90,92 and was specifically measured using the Pediatric Quality of Life Inventory (PedsQLTM) by an additional eight studies,45,47,51,57,67,72,74,91 for a total of 6% of total outcomes, but the specific aspects of QoL measured or reported were not well-identified or discussed. Finally, there were no outcomes that could be coded under ‘Future.’
Frequency of interventions and outcomes pre- and post-DMTs by F-word domains.
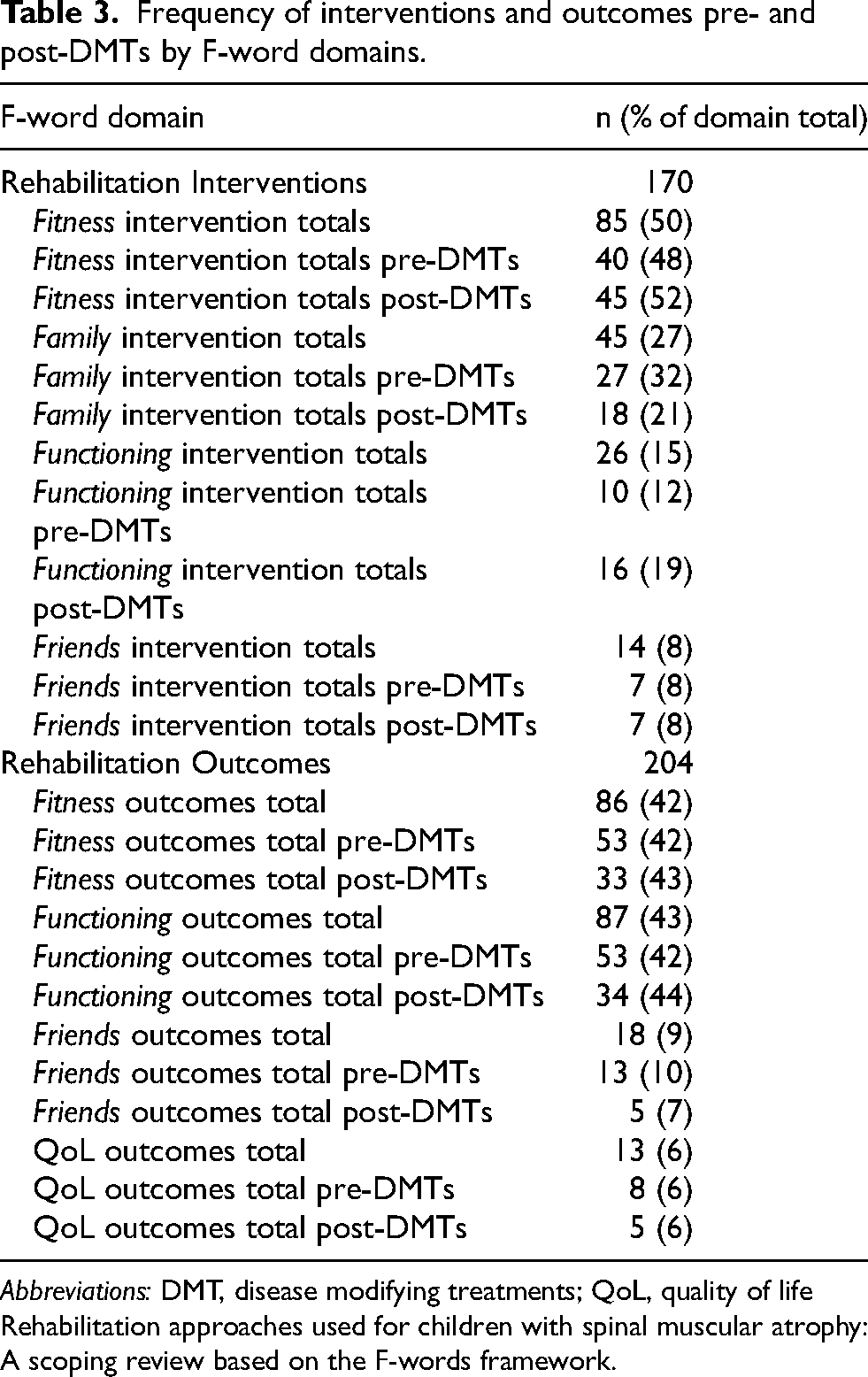
Abbreviations: DMT, disease modifying treatments; QoL, quality of life
Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework.
Pre- and post-DMT comparisons
The introduction of DMTs had little impact on the F-word domain foci for rehabilitation interventions and outcomes (Table 1 and Supplemental Table S2 for DMTs reported; Table 3 for summary by F-words domain; Supplemental Table S2 for detailed coding). The proportion of ‘Fitness’ and ‘Friends’ interventions remained the same. ‘Functioning’ interventions saw a modest increase in frequency usage (from 12% pre-DMTs to 19% post-DMTs). ‘Family’ based interventions showed the biggest change (a drop from 32% pre-DMTs to 21% post-DMTs). The detailed coding shows similar interventions used post-DMTs, apart from increased use of exoskeletons and harnesses for ambulation support and mobility practice, and decreased use of communication and assistive devices (Figure 2, Supplemental Table S2). Authors specified DMT related intervention changes in terms of earlier timing of physical therapy 31 and intensive bursts of rehabilitation,34,56,64 including rehabilitation-purposed inpatient stays22,35 (Supplemental Table S2). There was no substantial change in the focus of F-words outcome domains post-DMTs (Table 3, Figure 3). Within the ‘Functioning’ domain, there was proportionally greater reporting of motor and mobility outcomes post-DMTs, with decreased outcomes for self-care, arm and hand skills, communication and social participation (Figure 3, Supplemental Table S2).
Discussion
Summarize the results
The results of this scoping review indicate patterns in past and current SMA rehabilitation practices. While overarching approaches and frameworks are important to guide practice, few authors referenced one explicitly in their work. Others, however, have called for an increased focus on and re-imagining of rehabilitation post-DMTs and NBS. In applying the ICF/F-words framework, the data coding results show similar patterns, both pre- and post-DMTs, in the types of rehabilitation interventions being used and the outcomes of interest.
Rehabilitation interventions
From the coded results, summary statements can be made about the interventions in use. First, there was a predominant focus on ‘Fitness’ domain impairment-based interventions. In many cases, these were used in a ‘bottom-up’ approach, with the desired outcome of the ‘Fitness’-based interventions being an improvement in ‘Functioning.’ Second, ‘Functioning’ interventions primarily supported mobility, with little focus on other types of functions; this difference increased post-DMTs. Third, a decrease was seen in the ‘Family’ domain, in environmental and equipment adaptations used post-DMTs. Fourth, ‘Friends’ and ‘Fun’ domain interventions and considerations were under-represented, and ‘Future’ focused interventions to prepare youth for transitions to adult roles were missing from SMA rehabilitation. Finally, there were few individualized, goal-directed intervention approaches in use.
Rehabilitation outcomes
From the outcomes coding, the trends in outcomes mirrored those of interventions. First, the most frequently reported or measured outcomes in this review were ‘Fitness’ focused, followed by mobility ‘Functioning.’ Second, in keeping with the ‘bottom-up’ approach seen in interventions, at times the outcome domain of interest did not match the intervention domain. Third, daily living, communication and psychological ‘Functioning’, and social participation (‘Friends’) outcomes were infrequently mentioned. Fourth, there were exceptions in the extracted outcomes that might point to new ways of investigating and reporting treatment impacts, such as the use of patient reported and individualized outcomes.
Limitations
There are several limitations with this scoping review. First, ‘rehabilitation’ is a broad topic and challenging to define. The reviewers conducting this work attempted to use a broad range of search terms and implement clear definitions. High reliability was achieved in the article inclusion process and coding, but bias could be implicit throughout. Second, while a variety of databases and grey literature sources were searched, it is difficult to locate all literature; this overview of SMA rehabilitation practices is limited to what could be found in the literature and may not reflect ‘real world practice.’ Third, SMA is a rare condition and studies specific to SMA are difficult to produce. Most studies consisted of small case studies or case series, and similar to some SMA databases, there was a pattern of unequal sex representation, with more males represented. 93 Larger studies of disabled children more broadly may only include one to two children with SMA in their samples. By analyzing the literature with a clear focus on SMA, rehabilitation conceptualization specifically within the community of SMA care was analyzed, but not in reference to paediatric rehabilitation in general. Fourth, the goal was to identify patterns and gaps, and not to measure or weigh interventions and outcomes. The approach used to code and count interventions provided the wide scope needed to look at practice trends, but others may conceptualize this differently. Fifth, while this review found global representation in the literature, it is important to note that DMTs and NBS are not equally available around the world, and not all authors in the last four years report use of DMTs. Finally, this was not a review of the quality of evidence, although based on the types of reports and study designs coded, it is reasonable to conclude that limited, low-level evidence exists for much of rehabilitation targeted specifically for SMA. This review, however, is the first to present a wide, rigorous look at SMA rehabilitation practice trends to form recommendations for the future.
Implications
F-words practice gaps
The disproportionate representation of ‘Fitness’ interventions and limited focus on other F-word domains is a significant gap in SMA practice. In many cases, the desired outcome of these interventions is not only for improved ‘Fitness,’ but for improved ‘Functioning’. A cited premise for this ‘bottom-up’ intervention approach in SMA rehabilitation is that improvements in impairments transfer ‘up’ to improved ‘Functioning,’13,16 but this assumption has yet to be demonstrated. Reports describing this approach in SMA have low levels of evidence and/or significant methodological issues and biases,35,46,48,54,56,61,64 while others report limited and uncertain benefits.47,57,94,95 Research in other paediatric populations supports a move away from impairment-focused interventions in favour of greater functional outcomes with ‘Functioning’-focused interventions. Evidence-supported, activity-based motor learning and behavioural change methods were missing from the SMA rehabilitation literature, including (1) a focus on child-chosen goals; (2) meaningful and enjoyable activities; (3) whole task (task-specific) practice; (4) cognitive approaches with child-supported problem solving; (5) dosages to meet effective thresholds, including blocked practice; (6) practice in environmental context; and (7) supported home practice.96,97
A second practice gap is the use of ‘Fitness’ goals to remediate impairments only, without consideration of also addressing health. Children with disabilities experience barriers accessing physical fitness and are at elevated risk of sedentary-related health issues. 98 In this scoping review, no instances were found that included child- and family-focused exercise fitness goals using activities suited to individual interests and motivations. Evidence from other childhood disability populations supports this approach when supplemented with applied behaviour change strategies. This includes the described use of rigorous goal setting, reporting of complex interventions, and the use of sensitive measures for future clinical practice and research. 96
A limited exploration of the ‘Functioning’ domain is a third gap in SMA rehabilitation practice. Gross motor skill development and mobility were the predominant ‘Functioning’ foci of articles and abstracts. Other than one mention of therapists providing “developmental/ADL [activities of daily living] activity” interventions 49 and the use of an upper extremity exoskeleton to support ADL practice, 37 no other mentions of ADL practice as an intervention focus in SMA rehabilitation were found. Yet for many families, a child's ‘Functioning’ of ADL is of significant concern. 99 Communication and psychological functioning are also impacted by SMA, 22 but following the availability of DMTs, few reports specifically targeted speech and language skill development.
A fourth practice gap identified through the coding is the under-representation of the ‘Friends’ domain. What social inclusion and participation mean to children with disabilities is not well known.
100
The ‘Friends’ interventions seen in this review, adapted special programs (e.g., wheelchair sports and hippotherapy), can enable play and participation and positively impact mental health,
101
but can also be spaces of segregation.
102
In another intervention, Iraqi et al. developed a video game specifically to incorporate exercise for children with SMA through a gaming medium.
39
It is unclear, however, if children had a voice in the development to ensure the game does not become another segregated activity. ‘Family’ interventions primarily consisted of mobility equipment and assistive devices for mobility outcomes at home and school; the decreased usage of these post-DMTs might represent reduced need for these purposes. However, the lack of interventions addressing environmental ‘Family’ factors to promote ‘Friends’ (social participation) presents another practice gap. For example, there were no instances of adapted controllers for exergaming purposes being used to allow participation in popular games with peers, while still meeting ‘Fitness’ goals. Likewise, no programs were found that were directed at increasing participation for children with SMA, such as the “Pathways and Resources for Engagement and Participation (PREP)” program, which has measured success using an individualized approach to address ‘Family’ (environmental) factors to support ‘Friends’ goals.
103
Finally, now that DMTs have given children with SMA the possibility for longer and full lives, their ‘Future’ and transitions to post-secondary, work, and adult social roles need consideration and barriers addressed.104,105 This review found a lack of rehabilitation strategies addressing this new ‘Future.’ This might represent the sudden shift in possibilities for children and families living with SMA but is a distinct gap in knowledge and practice.
Standards of care
Implications of this work include rethinking how standards of care for SMA rehabilitation are informed. Due to the paucity of research evidence, the current 2018 SOC were developed by expert consensus, 13 without reference to guiding approaches or frameworks. The result is a primary focus on impairment domain interventions, with less detailing of the possible equipment and environmental supports listed, and a mention of adapted sports without a fulsome consideration of meaningful participation. In turn, the outcome focus is similarly predominately weighted on the impact on impairments, mobility, and undefined ‘function.’ 13 This limited breadth bears little resemblance to the individualized and goal-directed broad definitional possibilities of rehabilitation, as defined by Meyer et al. 20 Although, in practice, therapist recommendations and service provisions often do not fully meet the outlined standards,16,49,58 they have had a prevailing influence, as seen throughout this review. The SOC predate DMTs and NBS and are due for an update; this presents an opportunity to explicitly use holistic, child- and family-centered, and evidence-based rehabilitation approaches in the next iteration. As SMA is a rare disease, it may be fruitful to learn from other childhood disability populations to advance rehabilitation research and practice.
Multi-disciplinary practice gaps
Few authors describe a truly multi-disciplinary approach to rehabilitation, with the exception of Trabacca et al., 22 who applied the ICF. Physical therapy is the service most often reported, but often in isolation, and sometimes referenced as ‘physical therapy’ as an intervention unto itself, with no specifics as to the type of intervention actually provided, and with limited articulation of specific goals. While occupational therapy and speech-language pathology services are mentioned in the SOC, the full scopes of these professions are not well-represented in the reports found. The F-words framework may better facilitate collaboration and reporting of integrated, multi-disciplinary services to meet the complexities for SMA care.
Family and child voices
Most importantly, the voices of children with SMA and their families are largely missing from the SMA rehabilitation literature. This review found little use of individualized interventions or outcomes. In considering new possibilities for SMA rehabilitation, the F-words framework allows for a child-centred and broader conceptualization of disability, functioning, participation, and therapy goals.104,106 Both Trabacca et al. 22 and Giannotta et al. 107 reported the feasibility of applying the related ICF for multi-disciplinary SMA care planning.22,38 Beyond the ICF, the F-words provide family- and child-friendly language and the additional consideration of a child's changing development and ultimate transition to adulthood. 108
Next steps
Based upon the identified gaps and opportunities discussed in this paper (objective #2), the next steps for SMA rehabilitation include the following:
Use of holistic frameworks, such as the F-words, to reconsider the past and current priority on ‘Fitness’ over ‘Functioning’, ‘Friends’, ‘Fun’ and ‘Future’; Use ‘Fitness’-based interventions mindfully, with less emphasis on correction, and more on health; Expand consideration of the ‘Functioning’ domain to better balance mobility function with the self-care, communication, and the psychological functions also impacted by SMA; Include child-directed and activity-based goal-focused therapy, motor learning, and behavioural change approaches; Ensure children with SMA are not directed solely to adapted programs, but that their interests are discovered and supported (‘Friends’ and ‘Fun’); Support the transition to adult lives through ‘Future’ focused interventions; Ensure outcome domains match intervention domains; Broaden domains and types of outcomes of interest; include individualized patient-reported outcome measures; Expand multi-disciplinary approaches; Involve child and parental voices in individual practices and research, and in the broader development of SMA specific rehabilitation frameworks; and Grow collaborations for multi-site research to increase study sample sizes and practice knowledge.
In this era of new possibilities, it is time to actively engage with children and families and to broaden the understanding and scope of rehabilitation services and research, to rehabilitate SMA rehabilitation.
Supplemental Material
sj-docx-1-prm-10.1177_18758894261443738 - Supplemental material for Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework
Supplemental material, sj-docx-1-prm-10.1177_18758894261443738 for Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework by Patricia Mortenson, Niamh Cushen and Jill G Zwicker in Journal of Pediatric Rehabilitation Medicine
Supplemental Material
sj-docx-2-prm-10.1177_18758894261443738 - Supplemental material for Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework
Supplemental material, sj-docx-2-prm-10.1177_18758894261443738 for Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework by Patricia Mortenson, Niamh Cushen and Jill G Zwicker in Journal of Pediatric Rehabilitation Medicine
Supplemental Material
sj-docx-3-prm-10.1177_18758894261443738 - Supplemental material for Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework
Supplemental material, sj-docx-3-prm-10.1177_18758894261443738 for Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework by Patricia Mortenson, Niamh Cushen and Jill G Zwicker in Journal of Pediatric Rehabilitation Medicine
Supplemental Material
sj-docx-4-prm-10.1177_18758894261443738 - Supplemental material for Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework
Supplemental material, sj-docx-4-prm-10.1177_18758894261443738 for Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework by Patricia Mortenson, Niamh Cushen and Jill G Zwicker in Journal of Pediatric Rehabilitation Medicine
Supplemental Material
sj-docx-5-prm-10.1177_18758894261443738 - Supplemental material for Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework
Supplemental material, sj-docx-5-prm-10.1177_18758894261443738 for Rehabilitation approaches used for children with spinal muscular atrophy: A scoping review based on the F-words framework by Patricia Mortenson, Niamh Cushen and Jill G Zwicker in Journal of Pediatric Rehabilitation Medicine
Footnotes
Acknowledgements
The authors would like to thank Charlotte Beck, medical and rehabilitation sciences reference librarian at the University of British Columbia, for her expertise and guidance in developing the search strategy for this project. We also thank patient-partners Renelle Belliveau, Julie Clegg, Amneet Goraya, and Serenity Tremblay whose experiences and insights provided meaning to the analyses and recommendations. Patricia Mortenson acknowledges doctoral student support from the University of British Columbia (Four Year Doctoral Fellowship) and the BC Children's Hospital Research Institute (Trainee Boost Award).
Ethical approval and informed consent statements
Not applicable for this scoping review.
Author contributions
PM led the project administration, study conception, study design, extraction, analysis and interpretation of data, drafted the manuscript, and revised content based on feedback. NC contributed to the article screening, extraction, analysis, and interpretation process. JZ supervised the project, assisted with study conception and design, contributed to the article screening, interpretation of data, and provided critical revision of drafts. All authors reviewed and approved the final version of the manuscript. PM is responsible for the integrity of the work as a whole.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: Jill Zwicker is funded by the Canada Research Chairs Program (950–233161), BC Children's Hospital Research Institute & Foundation, and Canadian Institutes of Health Research (PJV-179798; AWD-025383). This work was supported by a grant from Muscular Dystrophy Canada (1045817-Zwicker).
BC Children's Hospital, Canada Research Chairs, Canadian Institutes of Health Research, Muscular Dystrophy Canada, (grant number PJV-179798, 950-233161, AWD-025383, 1045817-Zwicker).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All supporting data are available in the supplemental tables.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.