
Abstract
Purpose
This study aimed to understand and describe the rehabilitation and care complexity needs of adults with cerebral palsy (CP) receiving care in a pediatric healthcare setting.
Methods
This was an exploratory sequential mixed-methods study. Qualitative data included 20 semi-structured interviews with adults with CP and caregivers. Quantitative data included electronic health record data from adults with CP who were active pediatric rehabilitation medicine (PRM) patients over a two-year period at a pediatric health system (N = 280). Results from analyses were mixed and merged through narrative and joint display approaches.
Results
Three qualitative themes were identified: 1) Wide range of equipment and orthotic needs that change over time; 2) Various roles of therapies in adulthood; and 3) High levels of rehabilitation and subspecialty care utilization. Quantitatively, n = 150 (53.8%) had equipment prescription(s), n = 79 (28.2%) had orthotic prescription(s), and n = 162 (57.9%) were actively engaged in at least one type of therapy. Participants cumulatively saw over 30 types of specialists. Only n = 21 (7.7%) had documented transition efforts during their PRM visits.
Conclusion
While the rehabilitation needs of individuals with CP evolve over time, adults with CP have high rehabilitation and overall healthcare utilization needs. This can complicate the transition to adult-based care and underscores the importance of comprehensive and longitudinal transition processes.
Introduction
Cerebral palsy (CP) is the most common physical disability of childhood, with a prevalence of approximately 3 in 1000 births. 1 The life expectancy of individuals with CP is increasing, with more and more children with CP now reaching, and thriving in, adulthood. 2 Adults with CP have unique healthcare needs and risks, including a high prevalence of cardiac, metabolic, musculoskeletal, endocrine, respiratory, and psychological chronic conditions.3–8 Consequently, adults with CP require comprehensive adult-based care in addition to coordination of interdisciplinary care between multiple medical specialists. Additionally, rehabilitation specialists play an important role in supporting the function of adults with CP as they age. 9 This need for comprehensive care across the lifespan necessitates a transition from pediatric- to adult-based care. However, there are numerous barriers to transition for young adults with CP.10,11 Many pediatric CP programs do not have structured transition programs, and those that do have varying frameworks and practices. 12 Additionally, young adults with more complex medical needs often struggle to find appropriate providers in the adult care setting.13–15 As a result of these multifaceted challenges, the transition period is frequently stressful for both youth and caregivers.16–18 Poor transitions can also result in more frequent hospitalizations and poorer overall health outcomes. 19
Although there is currently no standardization of transition programs, including CP programs, there is specific guidance regarding the phases of transition: transition preparation, transfer of care, and integration into adult care.19,20 However, given the ongoing barriers to transition and the care complexity of many young adults with CP, more research is needed to define rehabilitation needs and care utilization to appropriately support and guide the healthcare transition. To develop a comprehensive, patient- and family-centered transition program for youth with CP, this mixed-methods study sought to understand and describe the rehabilitation and overall care complexity needs of adults with CP who continue to receive care in a pediatric healthcare setting. Qualitative data also provided rich themes related to barriers and facilitators to healthcare transition, 11 and the complex and varied roles that caregivers play during the transition to adulthood for young adults with CP. 18 Here, the focus was on the qualitative data related to complexity of rehabilitation-related and other healthcare needs to align with the quantitative data collected.
Methods
This was an exploratory sequential mixed-methods study. The qualitative phase of the study consisted of semi-structured interviews and took place first, thereby informing the subsequent quantitative phase, which included retrospective electronic health record (EHR) data extraction and descriptive analysis. This study, given its minimal risk, was deemed exempt by the Colorado Multiple Institutional Review Board (Protocol #22-0821).
Qualitative methods
Participants
Eligibility criteria were: 1) adult with CP aged 18 years or older and/or their caregivers; 2) English speaking; and 3) active pediatric rehabilitation medicine (PRM) patients (seen in the PRM clinic at least once between July 2020 – June 2022 and not yet transitioned to adult rehabilitation care). Using maximum variation purposeful sampling,21–23 participants were recruited for diversity of demographic background and level of function based on the Gross Motor Function Classification System (GMFCS). 24 In maximum variation sampling, key variables are selected by the research team and then cases that vary from each other as much as possible are identified, allowing meaningful patterns from a diverse sample to emerge. 23 Both patient and caregiver(s) were invited to be interviewed unless significant cognitive, communication, and/or behavioral impairments precluded patient participation. Options for patients and caregivers to interview separately or in dyads were offered.
Procedures
Semi-structured interviews were conducted using an interview guide (Supplemental Content 1) developed based on prior research, the study objectives, input from the study team's institutional Patient and Family Research Advisory Panel, and three pilot interviews (conducted by CG). Interviews took place from September 2022 – February 2023 over Zoom video conferencing or phone (depending on participant preference). Study team members who conducted interviews either had extensive qualitative research experience or participated in interview training (CG, CS, and JW). Participants who directly received care from one of the study team's clinicians (CS, JW) were interviewed by the qualitative analyst (CG) instead to avoid potential bias or influence. Verbal consent was obtained at the start of each interview, and participants self-reported demographic data that were entered into a secure REDCap electronic database. 25 Interviewers then guided conversation regarding the participant's priorities related to health and healthcare, experiences with pediatric rehabilitation care, changes in rehabilitation needs over time, and goals related to adult care. Interviews lasted 60–90 min, were audio-recorded with permission from participants, and were professionally transcribed (Landmark Associates; Phoenix, AZ). Transcripts were de-identified and entered into a qualitative software program for coding and analysis (ATLAS.ti version 23; Berlin, Germany). Interviews were conducted until thematic saturation was reached based on team consensus that no new information was being received. 26
Data analysis
Data were analyzed using a qualitative descriptive approach informed by phenomenological principles to explore the lived experience and values of young adults with CP and their caregivers. A qualitative descriptive approach allows researchers to explore, understand, and describe participant perspectives. Phenomenological principles focus on the lived experience of young adults with CP and their caregivers.27–30 The study team (CS, CG, JW) coded interview transcripts inductively by creating codes based on emergent data, 31 and met regularly to reconcile and calibrate coded transcripts until the codebook was finalized. 32 The remaining transcripts were coded separately, with 20% being double coded by two of the three coding team members. Once coding was complete, queries – or code reports – were generated, listing all associated quotations verbatim. Using traditional thematic analysis, quotations within each report were reviewed and summarized to identify salient themes.32,33
Quantitative methods
Participants
The quantitative phase of this project consisted of EHR data extraction and analysis of all patients that had a diagnosis of CP, were aged 18 years or older at their most recent PRM visit, and were active PRM patients as defined above.
Procedures
EHR data elements were retrospectively collected to quantitatively describe the characteristics and complexity of care of this population, as informed by patient- and caregiver-identified priorities, barriers, and facilitators from the qualitative data. Using a population sampling strategy, data were extracted from the EHR of all eligible participants through a combination of automated and manual means and entered into a secure REDCap electronic database. 25 Extracted data included patient demographics; medical history (based on diagnoses listed in the patient's medical history section of the EHR); encounters with the PRM clinic; durable medical equipment (DME), orthotics, and therapies (extracted through manual review of PRM clinic notes); rehabilitation-related procedures (e.g., focal tone management injections); documentation of healthcare transition efforts; and other subspecialist care within this health system. Data on office visit and procedural billing codes were extracted directly from the EHR as well. Because all of a patient's current equipment needs were not always documented, the number of equipment and orthotic prescriptions for either new or replacement DME during the two-year study period was extracted instead. Documentation of healthcare transition efforts included any of the following during manual EHR review: documentation of transition discussion/plan in most recent PRM clinic note, use of transition-related International Classification of Diseases-10 code during most recent PRM clinic encounter, or use of EHR-integrated transition planning tool.
Data analysis
Descriptive statistics for demographic, clinical, and care utilization data were calculated for all participants. Counts (percentages) were used to summarize categorical variables, while measures of central tendency were used to summarize continuous variables. Demographic and clinical characteristics between those adults with CP who were ambulatory (GMFCS levels I-III) and non-ambulatory (GMFCS levels IV-V) were compared, as well as those <22 years old (pre-typical transition age) and ≥22 years old (post-typical transition age). Fisher's exact tests were used to compare categorical variables between groups, while Student's t-tests were used to compare continuous variables between groups. Statistical significance was considered as alpha <0.05. All analyses were performed using SAS, version 9.4 (Cary, NC).
Mixed methods and data integration
This exploratory sequential mixed methods design used an independent analysis process whereby the qualitative and quantitative data were analyzed separately prior to merging results. 34 The qualitative findings guided the selection of EHR data items to extract so that qualitative trends could be explored quantitatively and generalized to a larger sample in an integration procedure known as building.34,35 The overall integration of qualitative and quantitative results provides both an in-depth understanding of patient and caregiver experiences and perspectives in the rehabilitation transition process, as well as a general understanding of this patient population in terms of demographic characteristics, complexity of care, and care utilization.
During data analysis, the data integration strategies of corroborating, enhancing, and transferring were used. 34 Corroborating allows for one type of data (descriptive quantitative data) to verify the findings of the other data (qualitative interview findings). Enhancing allows for both the qualitative and quantitative data to increase the meaningfulness of findings. Transferring helps to consider the relevance of qualitative interview findings in the larger quantitative sample. Results from both the qualitative and quantitative analyses were mixed and merged through both narrative and joint display approaches.35,36
Results
Twenty interviews were completed (13 caregiver, seven patient/caregiver dyads; 27 participants total). No adult with CP chose or was able to participate in an interview alone. All caregivers were parents, except for one who was a court-appointed legal guardian. Demographics of interview participants are presented in Table 1. The mean age of adults with CP who participated or were represented in interviews was 24.3 years. The quantitative retrospective chart review included N = 280 adults with CP. Demographic data are presented in Table 2. The mean age of adults with CP who continued to be seen in PRM was similar to those who participated in interviews (24.9 vs. 24.3 years, respectively), and ranged from 18 to 44 years old. Most adults with CP were between 18–25 years old (Figure 1). These patients were mostly female (57.1%), while interview participants with CP were mostly male (60%). The majority of patients included in quantitative analyses were non-ambulatory (GMFCS levels IV-V, 68.5%), which was also true of interview participants (70%). Almost 30% of this population identified as Hispanic or Latino/a, which is greater than the proportion of interview participants identifying as Hispanic or Latino/a (20%). The majority of adults with CP in both qualitative interviews and qualitative analyses had public insurance (Medicare or Medicaid). A similar proportion of both groups also resided in rural areas. Of these 280 adults with CP actively seen in the PRM clinic, only 21 (7.7%) had any documented transition efforts during their PRM visits. Most commonly, this was documented in the clinical note (n = 18) by the PRM provider. These patients also had high levels of medical complexity, with an average of 14.0 items in their medical history and seeing an average of 2.7 unique non-PRM specialists during the study period.
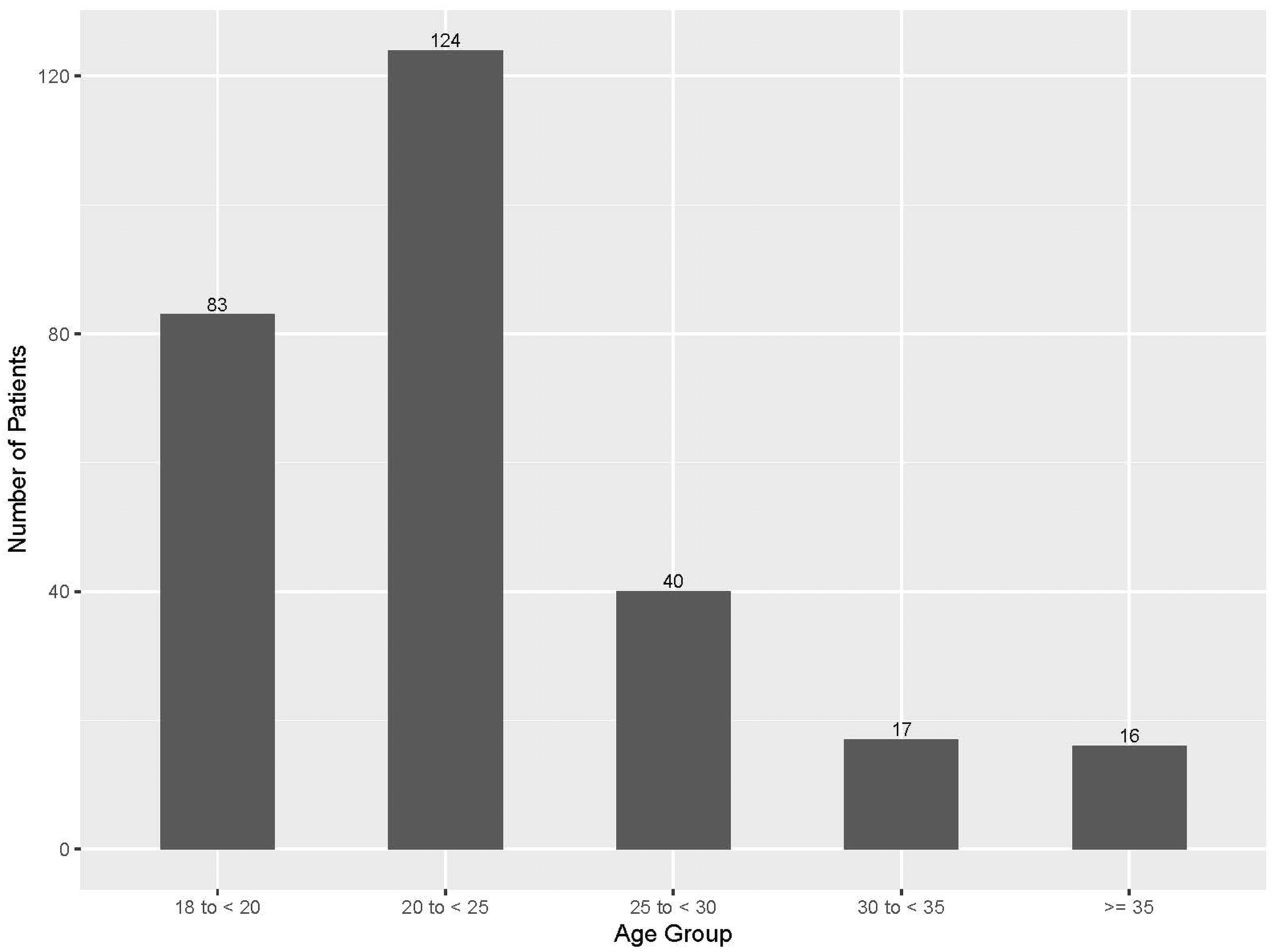
Ages of adults with cerebral palsy who had not yet transitioned to adult-based rehabilitation medicine care (N = 280).
Self-reported demographic data of qualitative interview participants (for caregiver-only interviews, demographic data about the adult with cerebral palsy for whom they provide care are included). One caregiver participant was a court-appointed legal guardian; their demographic data are excluded. Presented as n (%) unless otherwise stated.
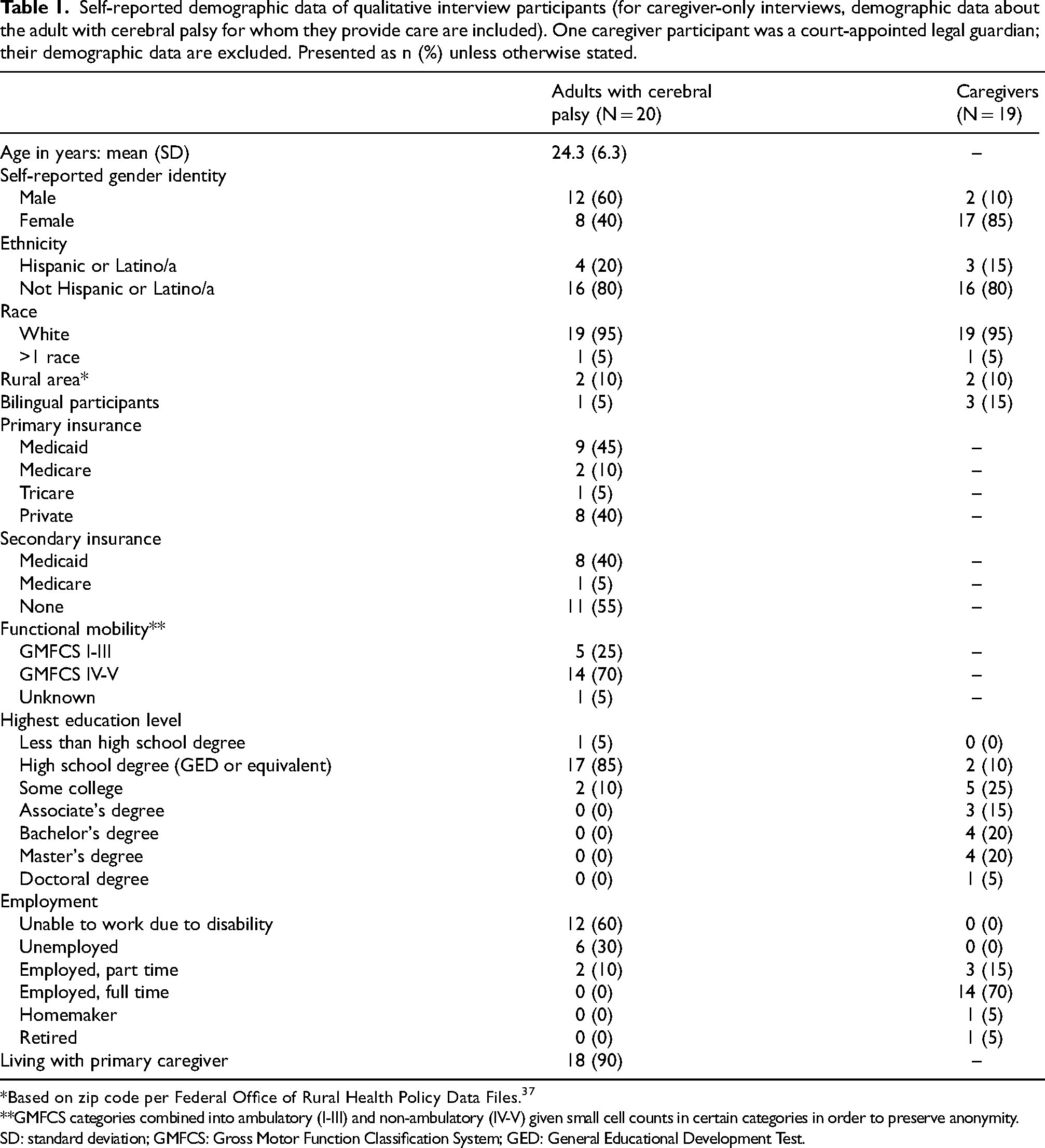
*Based on zip code per Federal Office of Rural Health Policy Data Files. 37
**GMFCS categories combined into ambulatory (I-III) and non-ambulatory (IV-V) given small cell counts in certain categories in order to preserve anonymity.
SD: standard deviation; GMFCS: Gross Motor Function Classification System; GED: General Educational Development Test.
Demographic and clinical characteristics of adults with cerebral palsy who have not yet transitioned to adult-based rehabilitation medicine care (N = 280). Presented as n (%) unless otherwise stated.
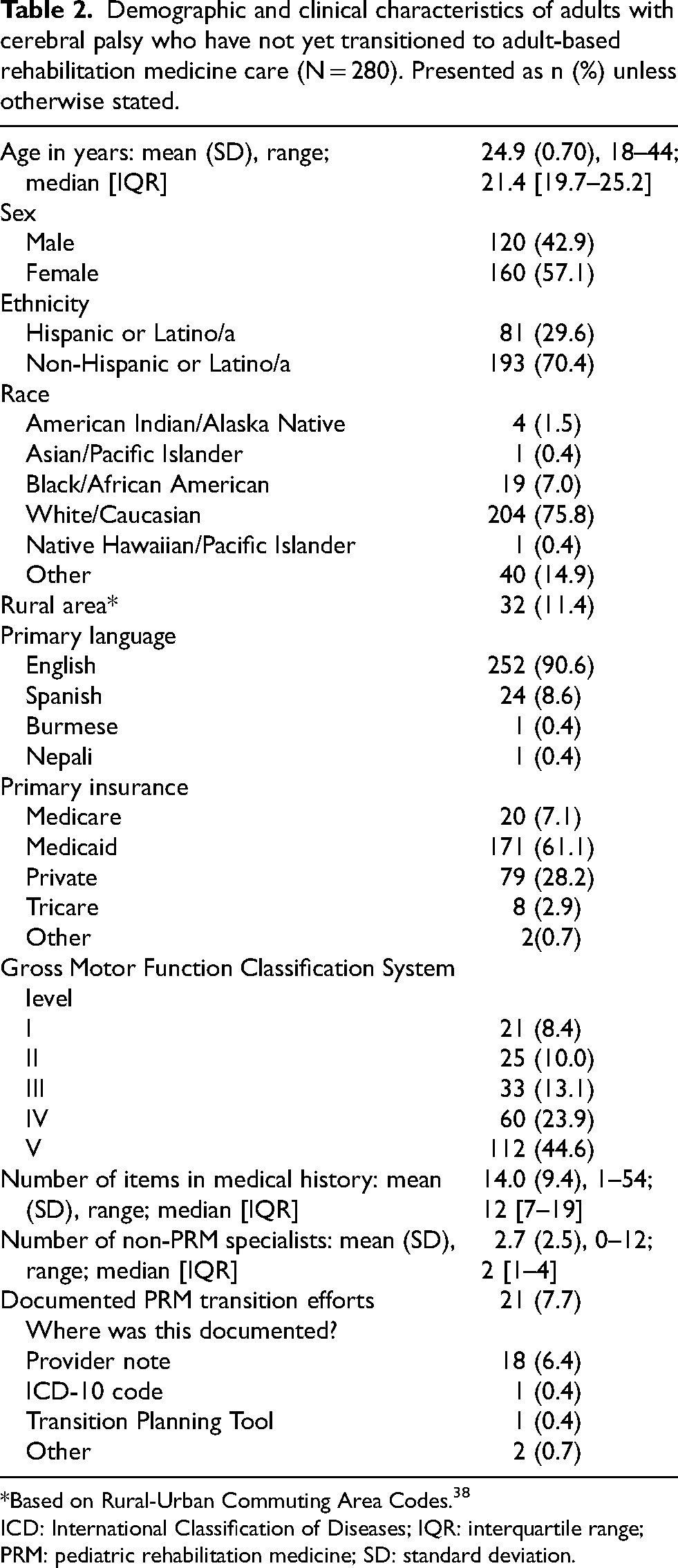
*Based on Rural-Urban Commuting Area Codes. 38
ICD: International Classification of Diseases; IQR: interquartile range; PRM: pediatric rehabilitation medicine; SD: standard deviation.
This study identified three qualitative themes, which guided the quantitative descriptive analysis: 1) Wide range of equipment and orthotic needs that change over time, 2) Various roles of therapies in adulthood, and 3) High levels of rehabilitation and subspecialty care utilization. Integrated qualitative and quantitative findings related to rehabilitation and overall healthcare needs follow.
Wide range of equipment and orthotic needs that change over time
Interviewed participants reported using a wide variety of DME – including various types of mobility devices, standers, custom seating systems, bath and shower equipment, hospital and safety beds and specialty mattresses, communication devices, and various orthoses. Interestingly, many caregiver participants shared that they currently had less equipment for their adult children than they did when they were younger. One caregiver shared how it was a gradual process of figuring out what equipment worked best for them, and what was unnecessary: We were always looking for the magic combination when he was smaller, right? I think a lot of people do that. Well, if we just have the right wheelchair, it’ll be easier for us, or if we just have the right whatever….We, at one point, had equipment everywhere, and none of it, actually, made life that much better….We’d go home with all of these things, and then we’d store them for years and never use them. - Participant 12
Functional goals drove DME selection and usage. A few participants noted that their adult child became “…less interested in using [certain equipment]” (participant 4) and only would use DME if they noticed a functional benefit. For example, one caregiver shared that her adult child would only wear her ankle foot orthoses (AFOs) when she noticed it helped her work as a camp counselor. Some participants noted that types of DME needed to be changed over time whereas others noted that the types of DME remained relatively the same.
Several caregivers described that functional goals for their children had shifted over time to be focused on comfort and quality of life. Sometimes, this necessitated new DME that would help caregivers continue to care for their growing children, such as lifts to aid in transfers. At other times, this meant less equipment and bracing to prioritize comfort and quality of life.
From the retrospective data analysis, adults with CP who continued to receive care in the PRM setting had a wide range of equipment and orthotic needs (Table 3 joint display), confirming what was captured during interviews. Slightly more than half of patients (n = 150, 53.8%) had at least one new DME prescription during this timeframe, though only 28.2% (n = 79) had a need for a new orthotic prescription. The most common type of equipment prescribed was mobility equipment (e.g., wheelchairs and walkers), and the most common type of orthotic prescribed was AFOs. When comparing ambulatory and non-ambulatory adults with CP (Table 4), there was a statistically significant difference in both the number of orthotic and DME prescriptions (0 vs. 1 vs. 2+) based on mobility status with ambulatory adults with CP more commonly having orthotic prescriptions but non-ambulatory participants more commonly having DME prescriptions. When comparing adults with CP <22 years old and those ≥22 years old (Table 4), there was also a statistically significant difference in number of orthotic and DME prescriptions with younger participants more commonly having orthotic prescriptions, but older participants more commonly having DME prescriptions.
Joint display of qualitative perspectives on durable medical equipment, orthotic, and therapy needs (N = 20) and quantitative data of these needs of adults with cerebral palsy who have not yet transitioned to adult-based rehabilitation medicine care, over the two-year study period (N = 280).
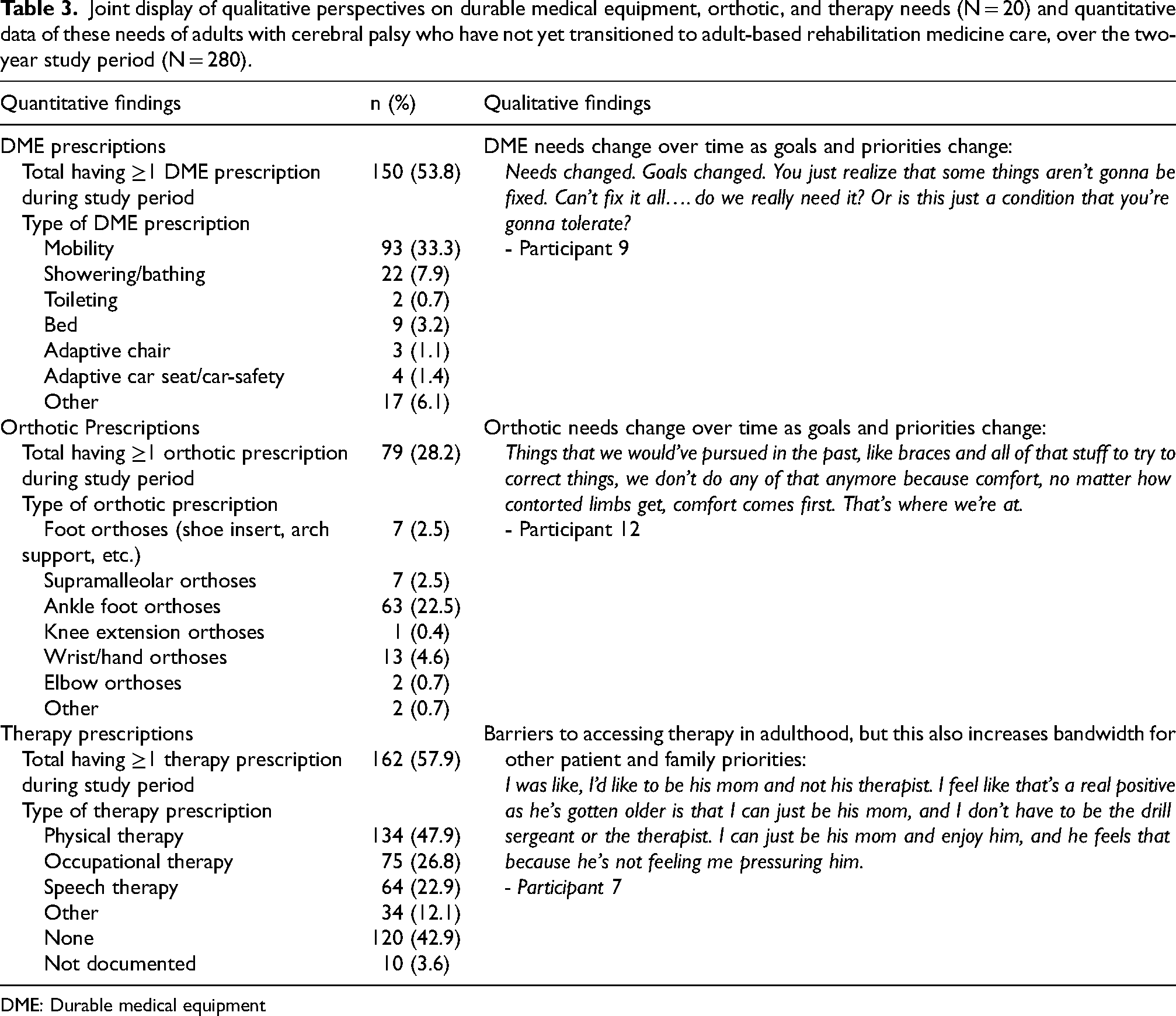
DME: Durable medical equipment
Comparison of rehabilitation needs between adults with cerebral palsy who are ambulatory (GMFCS levels I-III) and non-ambulatory (GMFCS levels IV-V), and those who are <22 years old (pre-typical transition age) and ≥22 years old (post-typical transition age). Presented as n (%) unless otherwise stated.
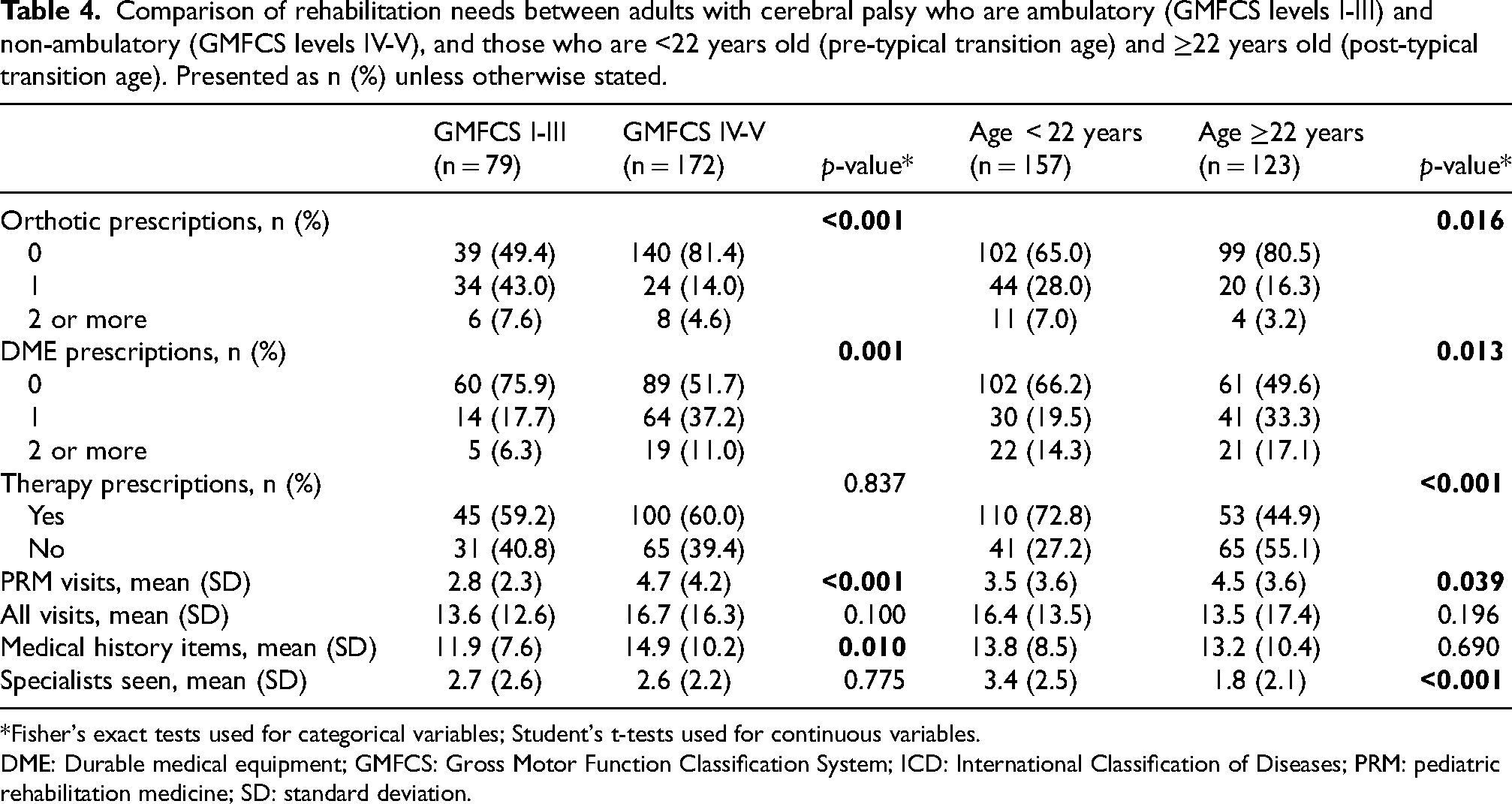
*Fisher's exact tests used for categorical variables; Student's t-tests used for continuous variables.
DME: Durable medical equipment; GMFCS: Gross Motor Function Classification System; ICD: International Classification of Diseases; PRM: pediatric rehabilitation medicine; SD: standard deviation.
Various roles of therapies in adulthood
While some interview participants reported that they or their child was not participating in formal therapies at the time of their interview, others reported engaging in a variety of therapies – physical therapy, occupational therapy, speech therapy, applied behavior analysis therapy, hippotherapy, vision therapy, social skills programs, music therapy, and feeding therapy. Beyond formal therapies, participants emphasized the benefits of other recreational activities, such as regular exercise, swim lessons, martial arts, and yoga.
However, participants also cited many challenges to participating in therapies. These included logistical barriers like scheduling appointments, transportation, and competing demands with limited time. While a few participants noted that their therapies were consistent over time, most noted a gradual decrease in the frequency and intensity of therapies as they or their child aged. Many felt that therapy would still be beneficial to maintain abilities, avoid contractures, and reduce pain, but, due to the above barriers, this was not possible. One parent shared that her adult child had less motivation to do formal therapies as an adult since she had participated in them for so long: <NAME>'s definitely experienced burnout and has gotten tired of spending her life in therapy which is understandable. - Participant 19
Many participants cited lack of insurance coverage as a critical barrier to therapies as an adult. They shared that “maintenance” therapy was not covered; it was difficult to find adult therapy facilities comfortable with CP; and it was difficult to continue getting therapy in pediatric facilities due to lack of appropriately sized equipment. As one caregiver expressed: …it was frustrating when he turned 18. It seemed like they didn't want to treat him in a sense. I'm like, nothing has changed. He still has CP. He's still a blind man, and he's having more problems, or he's getting stiff on this side from doing different activities. From high school to adulthood, things have changed. It just seems like the insurance, more so, didn't want to—I don't know, they needed more reasoning to get it approved. - Participant 6
Some participants felt like the decrease in formal therapies in adulthood was appropriate. A few caregivers reflected on their child's younger years when they were in frequent, intense therapy to try to optimize development and function. One caregiver felt that now she was “more relaxed toward his care” and “not feeling this pressure to do stuff” (participant 7). She shared how this shift let their family enjoy time together more and focus on what was important to them as a family.
Given the in-depth discussion of the role of therapies in qualitative interviews, quantitative data on active therapies were collected in the retrospective EHR review (Table 3 joint display). The majority of patients had some type of active therapy (n = 162, 57.9%). The most common therapy was physical therapy (n = 134, 47.9%), though occupational and speech therapy were also common (n = 75, 26.8% and n = 64, 22.9%, respectively). These quantitative results similarly confirm the qualitative findings – adults with CP receive varying amounts and types of formal therapies. When comparing ambulatory and non-ambulatory adults with CP (Table 4), there was no statistically significant difference in the presence of active therapies between ambulatory and non-ambulatory participants. When comparing adults with CP <22 years old and those ≥22 years old (Table 4), there was a statistically significant difference with younger participants more commonly having active therapies than older participants.
High levels of rehabilitation and subspecialty care utilization
Interviewed participants recalled largely positive interactions with their pediatric-based rehabilitation team, likening it to “seeing family or friends” (participant 8). Many shared that they will miss their PRM team once they transition to adult-based care, which was an often-cited barrier to transition. Participants felt comfortable with providers they had seen for years or even decades and valued their experiences with comprehensive care and excellent communication. As one caregiver shared: They actually take the time to listen to <NAME>, know <NAME>. They're not rushing us out the door. They take interest in her after 20 years like she's part of their family. They're gonna make sure she's okay. You just felt good about it. - Participant 9
Most interview participants largely felt that they were seeing their PRM provider at an appropriate frequency and expressed confidence that they would be able to be seen sooner, if needed. However, some recalled having to wait longer than expected to schedule appointments due to provider availability, and this was particularly challenging for families that had to travel greater distances to be seen.
While some interview participants did not receive any regular procedures with their PRM providers, others received botulinum toxin injections, phenol neurolysis, and/or intrathecal baclofen pump management. Several shared that the number of such procedures, particularly focal tone management procedures, decreased over time due to waning effects. Those that still received such procedures often cited pain management and comfort as the reasons they still pursued them. Participants also reported feeling confident in their providers’ procedural expertise, partially because they had consistently received these same procedures for years with the same providers. This comfort with their pediatric provider's procedural skills was sometimes cited as a barrier to transitioning to adult care. For example, one participant who had unsuccessfully attempted to transition noted that their adult-based provider appeared to have different opinions and/or thoughts about treatment indications regarding botulinum toxin injections than their pediatric-based provider.
Beyond rehabilitation medicine, qualitative interview participants highly valued well-coordinated, “one-stop-shop” care among their pediatric care teams at-large. Participants appreciated providers sharing their thinking processes and communicating with team members, and worried that this same level of care coordination may not be present in adult care. Additionally, they appreciated providers who saw the “whole person” rather than operating solely within their siloed disciplines. As one caregiver expressed: …the [pediatric] physicians … seem more able to look big picture than my experience with adult doctors, just from my own experience. …oh, this is one person seeing all these specialists, and all these things interact and impact each other, and you have to keep your mind aware of that, not just open to it, but aware of it so you see how things might ripple. … It's all the things stacking up that makes life so hard. Each individual thing might not be as horrible. The doctor there was able to see that. He sees everything. He sees how it all connects, and that's huge. - Participant 2
The 280 adults with CP included in quantitative analyses had a total of 1115 outpatient PRM visits during the two-year study period (Table 5 and Figure 2(a)). Beyond outpatient visits, there were 509 patient messages and 441 telephone calls with the PRM clinic during the study period. The median number of PRM visits during the study period was two per person, though this number ranged from 1 to 25 visits per person (interquartile range 1–5). The most common diagnosis code at PRM visits was for spastic quadriplegic CP (Table 6; n = 127), and visits were often billed at high levels based on time (Table 6). Procedures were also common at PRM visits, with n = 104 billing codes related to intrathecal baclofen pump management and n = 207 billing codes related to focal tone management procedures (Table 6). The value placed on team-based care and interdisciplinary communication and coordination was supported by the complexity of overall care seen during quantitative analyses. Adults with CP seen in the pediatric rehabilitation clinic cumulatively saw over 30 different types of specialists outside of the PRM clinic (Table 5). There were 2037 non-PRM specialist visits among this population during the study period, with a mean of nearly 10 non-PRM specialist visits per patient, though this number ranged from 0 to 64 (Table 5 and Figure 2(b)). The most commonly seen specialists were radiology (n = 141 patients saw radiology at least once during the two-year study period, 50.4%), neurology (n = 84, 30.0%), orthopedics (n = 78, 27.9%), and pulmonary (n = 61, 21.8%).
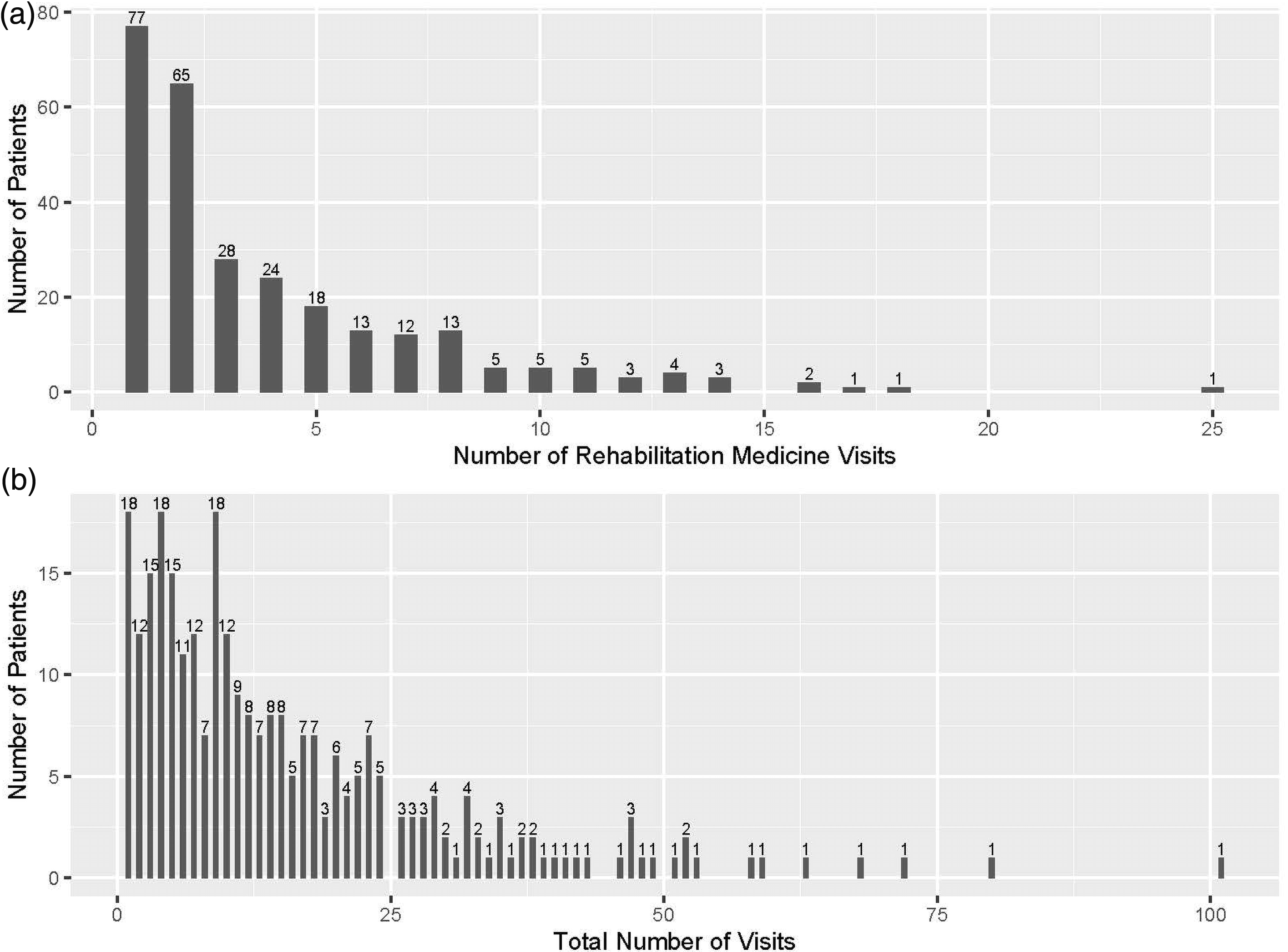
Number of pediatric rehabilitation medicine visits (2a) and all-specialty outpatient visits (2b) within the pediatric healthcare system of adults with cerebral palsy who had not yet transitioned to adult-based rehabilitation medicine care (N = 280), over the two-year study period.
Outpatient encounters of adults with cerebral palsy who had not yet transitioned to adult-based rehabilitation medicine care, over the two-year study period (N = 280).
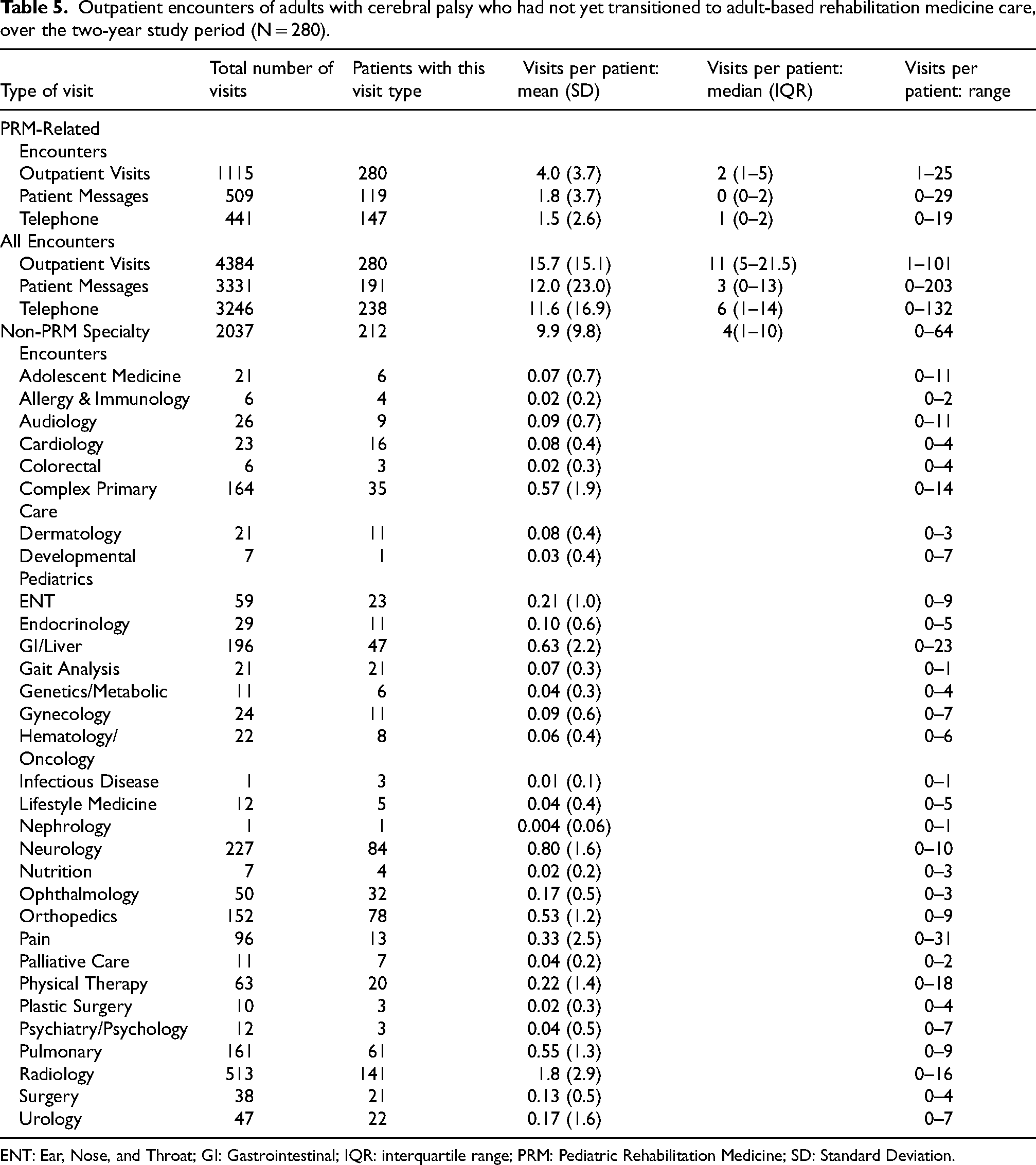
ENT: Ear, Nose, and Throat; GI: Gastrointestinal; IQR: interquartile range; PRM: Pediatric Rehabilitation Medicine; SD: Standard Deviation.
Diagnosis and billing codes at most recent pediatric rehabilitation medicine visit during two-year study period of adults with cerebral palsy who had not yet transitioned to adult-based rehabilitation medicine care (N = 280). Presented as n (%).
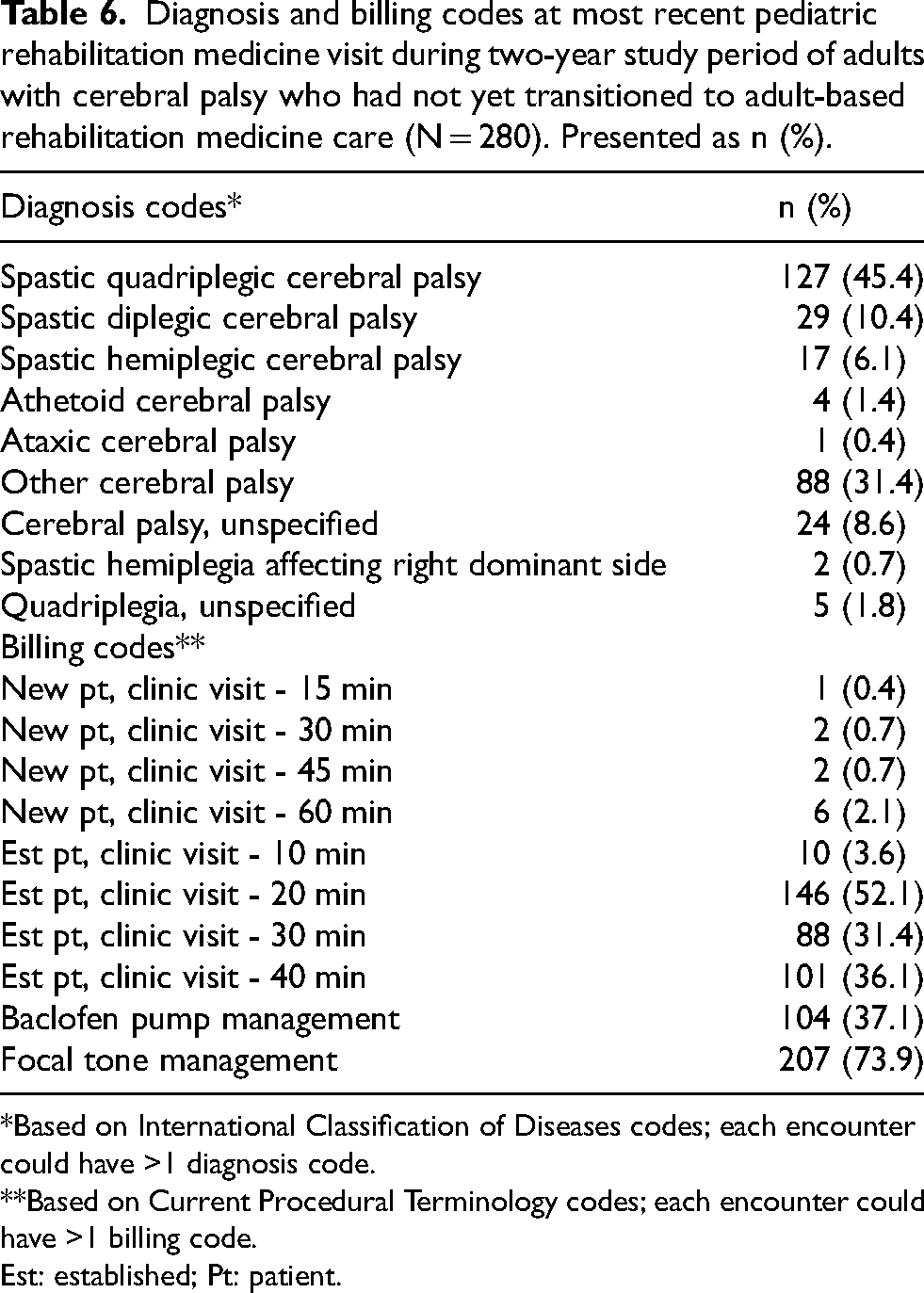
*Based on International Classification of Diseases codes; each encounter could have >1 diagnosis code.
**Based on Current Procedural Terminology codes; each encounter could have >1 billing code.
Est: established; Pt: patient.
The medical complexity and degree of interdisciplinary care demonstrated by these quantitative data helped to confirm qualitative results demonstrating that interview participants, particularly caregivers, placed such high value on coordinated, team-based care.
Discussion
This study used an exploratory sequential mixed-methods approach with qualitative semi-structured interviews and quantitative analyses of retrospective EHR data. These methods helped increase understanding of the rehabilitation and overall care complexity needs of adults with CP who continued to receive care in a pediatric healthcare setting. Qualitatively, participants described a wide range of equipment and orthotics needs that changed over time, various roles of therapies in adulthood, and high levels of rehabilitation and subspecialty care utilization. Quantitative findings confirmed the qualitative themes. Equipment and orthotic needs varied based on functional mobility status and age; engagement with therapies also varied based on age. And finally, participants had extremely high levels of healthcare utilization and care complexity.
Individuals aging with CP have high rates of chronic conditions that require comprehensive rehabilitation care. This includes chronic pain in at least 70% of adults with CP, chronic fatigue in 65%, and a higher prevalence of many neurological and musculoskeletal chronic conditions compared to adults without CP.6,739–42 Not surprisingly given these comorbidities, functional decline has been frequently noted among adults with CP, with some studies finding 60% experienced a decline in gross motor function since childhood.40,43
Rehabilitation specialists, including physiatrists, can play a key role in identifying and managing many of these conditions to optimize function and quality of life. Physiatrists specialize in serving patients with disabilities that affect multiple domains, such as those with CP. 9 A prior study among Canadian physiatrists found that more than 80% felt that physiatry was the most appropriate specialty to provide this care to adults with CP; however, in practice most physiatrists saw very few adults with CP (10 or fewer). 9 Adults with CP also lack access to other associated rehabilitation services, including difficulty accessing assistive equipment and orthoses, lack of useable mobility aids, and inappropriately fitting/unsupportive mobility devices.44,45 By virtue of its design, this study only included adults with CP with access to PRM specialty care. Among these patients, many adults with CP had equipment and orthotic needs that required ongoing rehabilitation management.
Similarly, therapies can play a critical role in optimizing, maintaining, or restoring function for adults with CP. 46 While more than half of the 280 adults with CP included in the quantitative analyses had a new therapy prescription during the study period, this differed significantly between those who were pre-transition age (less than 22 years) or post-transition age (22 years or greater). Almost 73% of those <22 years old had a new therapy prescription, while only 45% of those ≥22 years old did. This decrease in therapies for adults with CP in their early 20 s is consistent with a prior study. This prior study found that youth with CP had dramatically decreased participation in physical therapy after leaving secondary school, where many youth with CP have access to therapies. 46 The reasons for this difference are unclear from the quantitative data. However, qualitatively, participants described barriers to accessing therapies in adulthood including lack of appropriate facilities/therapists and insurance barriers to ongoing therapy. However, some also perceived a decreased need for skilled therapies in adulthood, which also allowed for more time and energy to pursue other activities. A prior study of physical therapists found that the top perceived barriers to providing therapy to adults with childhood-onset neuromotor disabilities (e.g., CP) included the extra time required for complex patients, lack of insurance coverage, and lack of experience. 47 While the reasons for decreased therapy participation in adulthood for patients with CP are likely multifactorial, lack of access to appropriately trained providers and insurance barriers were commonly cited in the current study and the existing literature and thus warrant future study and advocacy to adequately address.
Beyond the comorbidities described above (e.g., pain, fatigue, musculoskeletal issues), adults with CP also experience higher rates of many other chronic conditions and at earlier ages than the general population. This includes a higher prevalence of diabetes, asthma, hypertension, stroke, emphysema, and mental health diagnoses as well as a higher prevalence of multimorbidity.5–8,40–42 In accordance with this medical complexity (i.e., high prevalence of chronic diseases and multimorbidity) described in the literature, there was a high level of overall care complexity and utilization described by interview participants and seen during quantitative analyses. Patients had complex medical histories and had care teams involving many specialists. Those who were non-ambulatory (GMFCS levels IV-V) had significantly longer medical histories than those who were ambulatory (GMFCS levels I-III), likely reflecting more medical comorbidities among those with more severe functional mobility impairments. Those who were post-transition age saw significantly fewer specialists than those who were pre-transition age, which may reflect the transition to adult-based care within some of these other specialties, or the loss of specialist care upon entering adulthood. Approximately 750,000 youth with special health care needs in the United States transition to adulthood each year, yet fewer than half receive adequate transition care. 13 A prior study of pediatric CP clinics in the United States found that only 55% had a structured transition program. Only one transitioned all patients to adult providers by 22 years of age, and none were completely satisfied with their transition process. 12 Similarly, less than 8% of the 280 adults with CP actively seen by PRM in this study had any documented transition effort at their most recent PRM visit, despite being of appropriate transition age. While the barriers to transition are complex and multifactorial for youth with CP, as were explored in depth with qualitative participants and described fully elsewhere, 11 there are significant difficulties accessing healthcare professionals who are comfortable and experienced caring for adults with CP and other childhood-onset disabilities. 48 This perpetuates the lack of coordinated services available to adults with CP, the abrupt discontinuity of care upon leaving the pediatric system, and the difficulties of ensuring lifespan care for persons with CP. 49
Limitations
This study had several limitations that should be considered. First, it was conducted at a single academic pediatric health system located in the United States, which may affect the transferability of the qualitative findings 50 and generalizability of the quantitative results. Second, among qualitative interview participants, interviewees were mostly White, caregivers mostly female and employed, and adults with CP were mostly non-ambulatory. Additionally, qualitative interviews included only English-speaking participants. This may limit transferability to individuals of different backgrounds. In qualitative research, transferability refers to the ability to “apply information drawn from specific persons, settings, and eras to others that have not been directly studied.” 51 As such, the findings may not represent the experiences of individuals who are non-White, male caregivers, ambulatory adults with CP, or non-English speaking individuals. Finally, participants in both qualitative and quantitative portions of this study all received pediatric CP specialty care by virtue of the study design and recruitment. As such they had experience accessing rehabilitation services focused on providing care for complex needs. Those who do not receive such specialized care may have lower rates of rehabilitation and other healthcare utilization. However, this likely reflects unmet need in lower-resource settings rather than lesser need.
Conclusions
While the rehabilitation needs of individuals with CP may change and evolve over time, adults with CP continue to have high rehabilitation and overall healthcare utilization needs. This can complicate the transition to adult-based care and underscores the importance of comprehensive and longitudinal transition processes. The shifting view of CP from a pediatric disability to a lifespan disability also emphasizes the need for age- and developmentally appropriate care.
Supplemental Material
sj-docx-1-prm-10.1177_18758894251391901 - Supplemental material for Rehabilitation needs and healthcare utilization of adults with cerebral palsy: A mixed methods study
Supplemental material, sj-docx-1-prm-10.1177_18758894251391901 for Rehabilitation needs and healthcare utilization of adults with cerebral palsy: A mixed methods study by Cristina A Sarmiento, Chloe Glaros, Jordan M Wyrwa, Emily Gianetti, McKenzie Bremel, Lori Silveira, Donald Borchert, Lisa A Brenner and Brooke Dorsey Holliman in Journal of Pediatric Rehabilitation Medicine
Footnotes
Acknowledgments
We would like to thank the young adults and caregivers who participated in our study, sharing their experiences to increase our understanding with the hopes of improving care for individuals with cerebral palsy across the lifespan.
Ethical considerations
This study, given its minimal risk, was deemed exempt by the Colorado Multiple Institutional Review Board (Protocol #22-0821).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Foundation for Physical Medicine and Rehabilitation and the Tai Foundation. They did not participate in the study design, data collection or analysis, or manuscript preparation. Through our use of the University of Colorado’s REDCap database, this work was supported by NIH/NCATS Colorado CTSA Grant Number UL1 TR002535. Dr. Sarmiento is also supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under award number K23HD117945. This content is the authors’ sole responsibility and does not necessarily represent official NIH views.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Sarmiento reports funding from the Foundation for Physical Medicine and Rehabilitation, the Cerebral Palsy Alliance Research Foundation, the Tai Foundation, and the National Institute on Disability, Independent Living, and Rehabilitation Research. The remaining authors have no conflict of interest to report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.