
Abstract
Purpose
Lower extremity spasticity can cause pain and limit function. This study examined the safety and efficacy of hyperselective neurectomy (HSN) of the gastrocnemius-soleus complex (GSC) in addressing spastic equinus deformities in pediatric patients.
Methods
Pediatric patients that underwent HSN of the GSC by a single surgeon were retrospectively reviewed. Preoperative and postoperative Modified Ashworth Score and passive ankle dorsiflexion (°) were compared using Wilcoxon signed-rank test and Student's paired two-tailed t-test, respectively.
Results
Ten lower extremities in seven patients with a mean age of 10 years were reviewed. Mean follow-up was 15 months. All extremities demonstrated improvement in spasticity. All exhibited improved passive ankle dorsiflexion range of motion with the knee in extension (mean change +17°, SD = 8°, p = 0.000). Five patients demonstrated improved passive dorsiflexion with the knee in flexion while two remained unchanged from preoperative assessment (mean change +13°, SD = 9°, p = 0.002). One complication, wound dehiscence, was noted and managed conservatively. No patients reported loss of strength or sensation. Four patients underwent subsequent staged surgery on the ipsilateral extremity for concomitant contractures.
Conclusion
HSN of the GSC is safe in pediatric patients and effectively reduces spastic equinus deformity and improves ankle passive dorsiflexion in short-term follow-up.
Introduction
Spasticity is a velocity-dependent resistance to stretch applied to a muscle group across a joint. 1 Spasticity is commonly observed in individuals with congenital or acquired upper motor neuron (UMN) injuries including cerebral palsy, traumatic brain injury, stroke, and spinal cord injury. The disruption of normal inhibitory UMN pathways interrupts inhibitory influences and causes heightened excitability of spinal reflexes. 2 This leads to reduced motor control and discoordination between agonistic and antagonistic muscle groups. If not addressed, spasticity can lead to progressive muscle and joint contractures, markedly affecting gait, posture, function, and self-care.
Specifically, individuals with spastic hemiplegia commonly exhibit equinus foot deformities and abnormal gait patterns. 3 Spasticity within the gastrocnemius and soleus muscles, otherwise known as the gastrocnemius-soleus complex (GSC), drives equinus deformity while concomitant posterior tibialis (PT) muscle spasticity results in an equinovarus deformity.4,5 Addressing spastic posturing of the foot and ankle optimizes initiation and termination of gait, improves balance, and mitigates the development of fixed equinus or equinovarus deformities. Furthermore, in children, these deformities can occur rapidly during growth due to the imbalance in agonist and antagonist muscles and underlying spasticity. 6
Non-operative management of lower extremity (LE) spasticity typically involves a combination of physical therapy, orthoses, anti-spasmodic medications, and chemical denervation.6,7 When positioning, function, or deformity worsen, surgery may provide lasting relief by targeting spasticity at the level of the muscle, tendon, or peripheral nerve. 8 Surgical treatment may include muscle release/recession, tendon lengthening/tenotomy, and nerve-based procedures such as selective dorsal rhizotomy (SDR) and partial or selective motor nerve neurectomy.9–11 Spasticity without muscle or joint contracture can be effectively treated by nerve-based procedures alone, while spasticity with muscle contracture may be best addressed with nerve-based procedures in conjunction with muscle-tendon lengthening procedures. Of note, muscle-tendon lengthening procedures have variable long-term efficacy in children, likely due to ongoing longitudinal skeletal growth with ongoing spasticity. 12
Nerve-based procedures to address spasticity may involve several targets within the peripheral nerve. SDR involves sectioning portions of the dorsal nerve root, permanently reducing spasticity, yet can have unintended weakening of non-spastic muscles. 6 Total, partial, and selective neurectomies target peripheral nerves downstream of this location (Table 1). Neurectomy consists of excising a segment of nerve to prevent unwanted axonal regeneration and motor reinnervation. Partial motor neurectomy and selective motor neurectomy were first described in the LE by Adolf Stoffel in 1913 to disrupt the neural reflex arc that facilitates spasticity. 13 These procedures target either the main motor branch or the primary branch of the main motor nerve. In 1983, Brunelli et al. improved the technique for selective neurectomy in the upper extremity with more extensive nerve resection, though over half required a second surgery due to recurrence of spasticity. 9 Subsequently, Sindou and Mertens furthered the technique by introducing fascicular dissections via a microscope.11,14
Nomenclature of neurectomy based on location within the peripheral nerve.
Neurectomy – resection of a nerve segment, Total – complete nerve, Partial – portion of nerve.
Leclercq et al. further refined this technique as hyperselective neurectomy (HSN). Although initially reported in the LE, recent literature has pertained to surgery of the upper extremity. 10 Compared with other nerve-based procedures, such as SDR, HSN offers the advantage of specifically targeting the motor rami as it interfaces with the target muscle at the motor endplate, thus minimizing collateral neuromotor dysfunction or injury (Table 1).
The safety and efficacy of HSN of the upper extremity and selective partial motor neurectomy of the LE in children and adults with hypertonia is well-described; however, HSN of the GSC has not been evaluated.9–11,15 As HSN can offer permanent spasticity reduction critical for reducing deformity, especially in children for whom muscle and tendon based procedures can recur with skeletal growth, the purpose of this study was to determine the efficacy and safety of HSN in addressing primary spastic equinus deformity within a pediatric population.
Methods
Clinical patient cohort
A retrospective chart review was performed for pediatric patients (<18 years old) who underwent HSN of the GSC by a single surgeon (P.C.R.) at a tertiary referral institution from 2020 to 2023. Institutional ethics approval was obtained prior to the study.
Outcome measures
Patient charts were reviewed for demographic information, underlying diagnoses, and Gross Motor Functional Classification Score (GMFCS) for those with cerebral palsy. Outcome measures included pre- and postoperative Modified Ashworth Scale (MAS), motor strength (Medical Research Council scale), sensory disturbance, passive ankle dorsiflexion (°) with the knee in flexion and extension, and use of gait aids/ankle-foot orthoses. 16 Passive dorsiflexion was assessed with a handheld goniometer with the patient in supine position. The presence of a gastrocnemius contracture was determined based on physical examination, specifically by comparing passive ankle dorsiflexion with the knee in flexion versus extension. Major complications were defined as those requiring return to the operating room and minor complications as those managed non-operatively.
Multidisciplinary approach
Patients were initially evaluated by a multidisciplinary team and non-operative spasticity management was guided by a physical medicine and rehabilitation (PMR) physician. Treatments included chemical denervation with botulinum toxin, phenol, and/or oral antispasmodics. For ambulatory patients considering surgical spasticity management, dynamic electromyography (EMG) and gait/motion analyses with a comprehensive assessment facilitated the development of an individualized surgical treatment plan for HSN. The assessment team included pediatric orthopedic, foot/ankle and peripheral nerve surgeons. HSN was followed by a period of physical therapy, including gait retraining. Follow-up evaluation determined if additional muscle, tendon, or joint procedures were necessary to address residual deformity.
Surgical technique
HSN was performed under tourniquet control through a longitudinal incision in the midline of the posterior aspect of the leg, extending from the popliteal crease to the middle third of the calf. The sural nerve and lesser saphenous vein were identified coursing between the medial and lateral heads of the gastrocnemius. Retrograde dissection of the sural nerve facilitated identification of the tibial nerve deep within the popliteal fossa. Antegrade dissection along the tibial nerve revealed the origin of the motor branches to the medial and lateral heads of the gastrocnemius muscles and the motor branches to the soleus muscle Figure 1. There are usually one to two motor branches to the medial gastrocnemius, lateral gastrocnemius, and soleus Figure 2.17,18
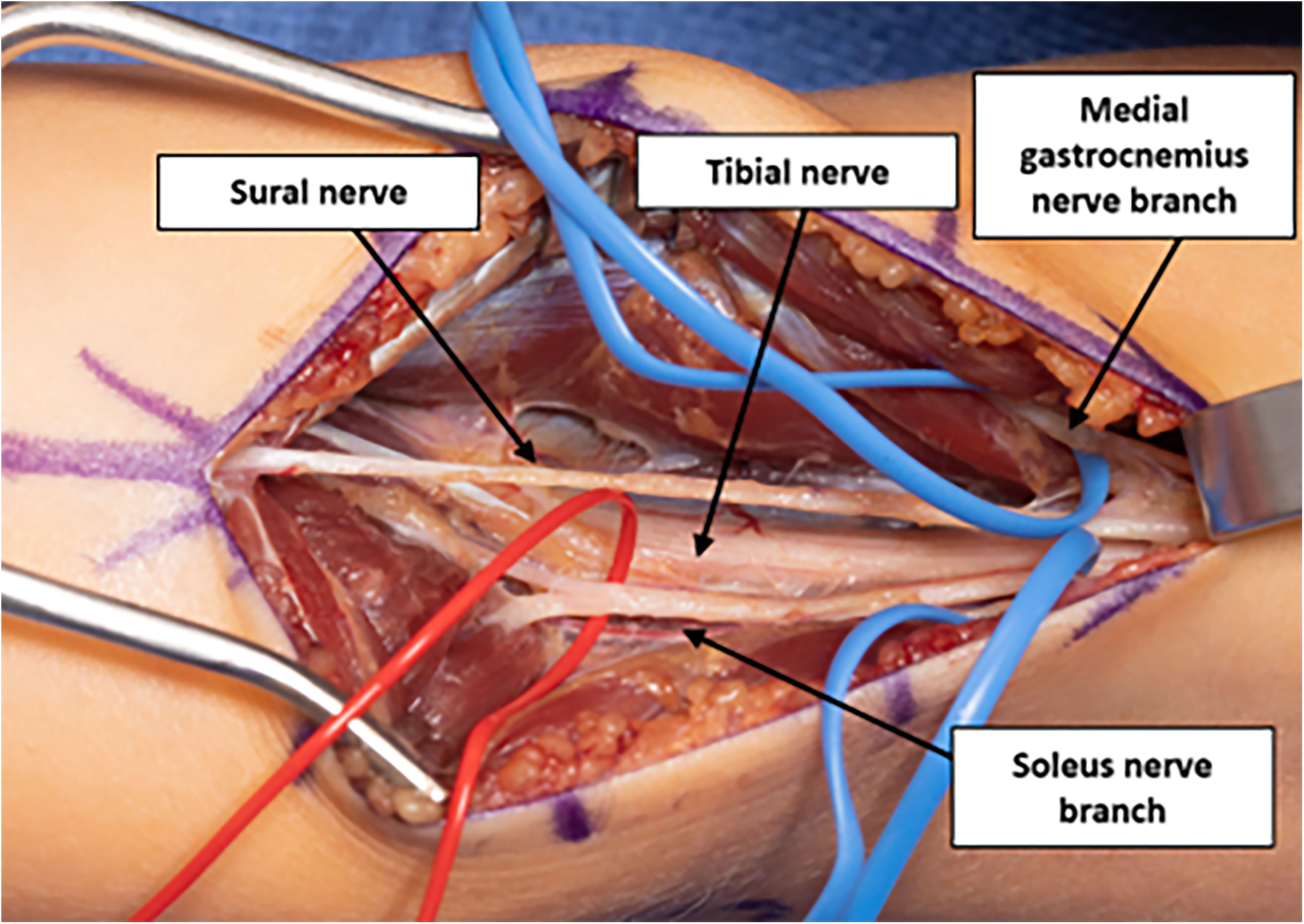
Tibial and sural nerves and motor nerve branches to the medial head of the gastrocnemius and soleus in a right lower extremity.
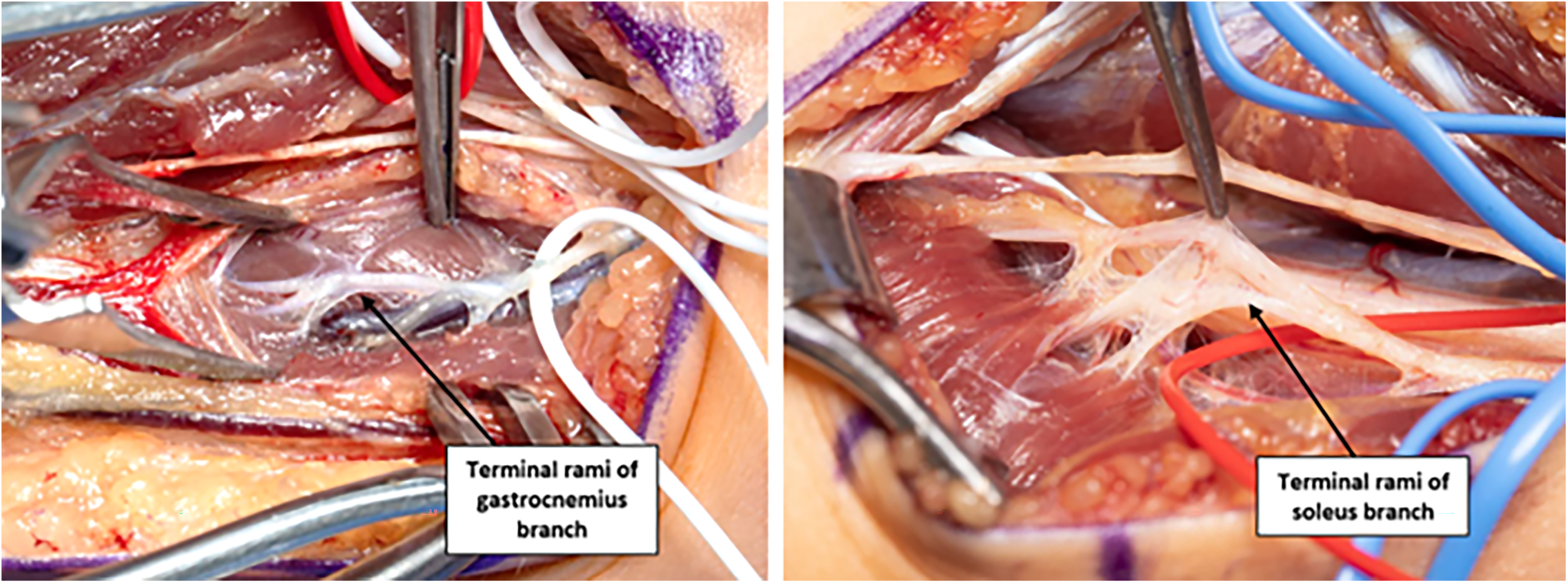
Terminal rami of the gastrocnemius and soleus motor nerve branches.
The motor branches to the gastrocnemius and soleus muscles were dissected intra-muscularly to expose, identify, and mobilize the terminal motor rami of each motor branch prior to their integration with the motor endplates Figure 2. The identity of the terminal motor rami was confirmed with the use of a handheld, intra-operative nerve stimulator. The tourniquet was deflated for up to 20 min to permit neuromotor reperfusion prior to electrical stimulation, and patients had reversal of any paralytic agents. A 1–2-centimeter segment of approximately 60–70% of the terminal motor rami of each motor branch to the gastrocnemius and soleus was excised.
Additionally, partial motor neurectomy was performed by excising approximately 60–70% of the terminal motor rami, under loupe magnification based on intra-operative identification with a nerve stimulator, within the primary motor branch to the PT if substantial varus or inversion posture was noted during gait or at rest on physical examination Figure 3. A handheld nerve stimulator was utilized to confirm the motor fascicles to the PT prior to neurectomy. If stimulation resulted in activation of non-target muscles, those fascicles were preserved, and only those eliciting isolated PT contraction were selected for neurectomy.
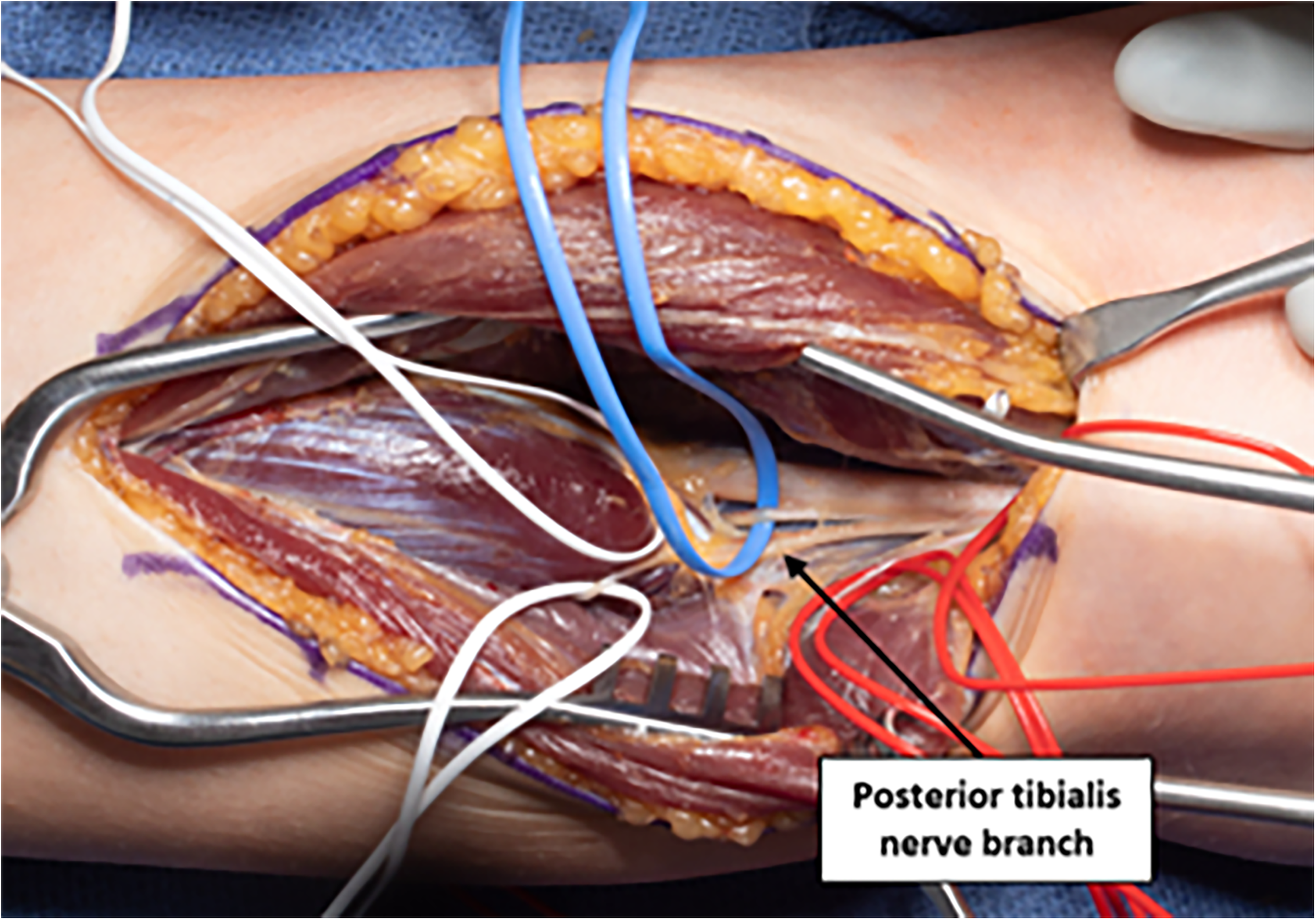
Motor nerve branch to the posterior tibialis.
The skin incision was closed with absorbable sutures. Postoperatively, patients were permitted to ambulate as tolerated while refraining from passive knee stretching exercises to decrease tension on the wound. A compressive dressing was applied across the knee joint to minimize edema and prevent soft tissue irritation for patients who required continued use of an ankle-foot orthosis.
Statistical analysis
Pre- and postoperative degrees of passive ankle dorsiflexion were compared using Student's two-tailed paired t-test and descriptive statistics. The normality of the distribution of differences between preoperative and postoperative degrees of dorsiflexion was assessed using the Shapiro-Wilk test. The data did not significantly deviate from normality (p = 0.057), supporting the use of the paired t-test. MAS scores were compared using non-parametric statistics. MAS grades for each extremity were compared pre- and postoperatively. A MAS of 1 and 1 + were counted as distinct grades.
Results
Patient demographics
Ten lower extremities in seven patients (five female) underwent HSN of the GSC for spastic equinus deformity at a mean age of 10 (range: 6 to 17) years. Demographic data and surgical details are included in Table 2. Surgical outcomes are detailed in Tables 3–6. Single-stage bilateral HSN procedures were performed on three patients. In addition to HSN, four lower extremities in three patients had concurrent partial motor neurectomies of the PT to address spastic equinovarus deformity (Table 2).
Patient demographics, surgical details.
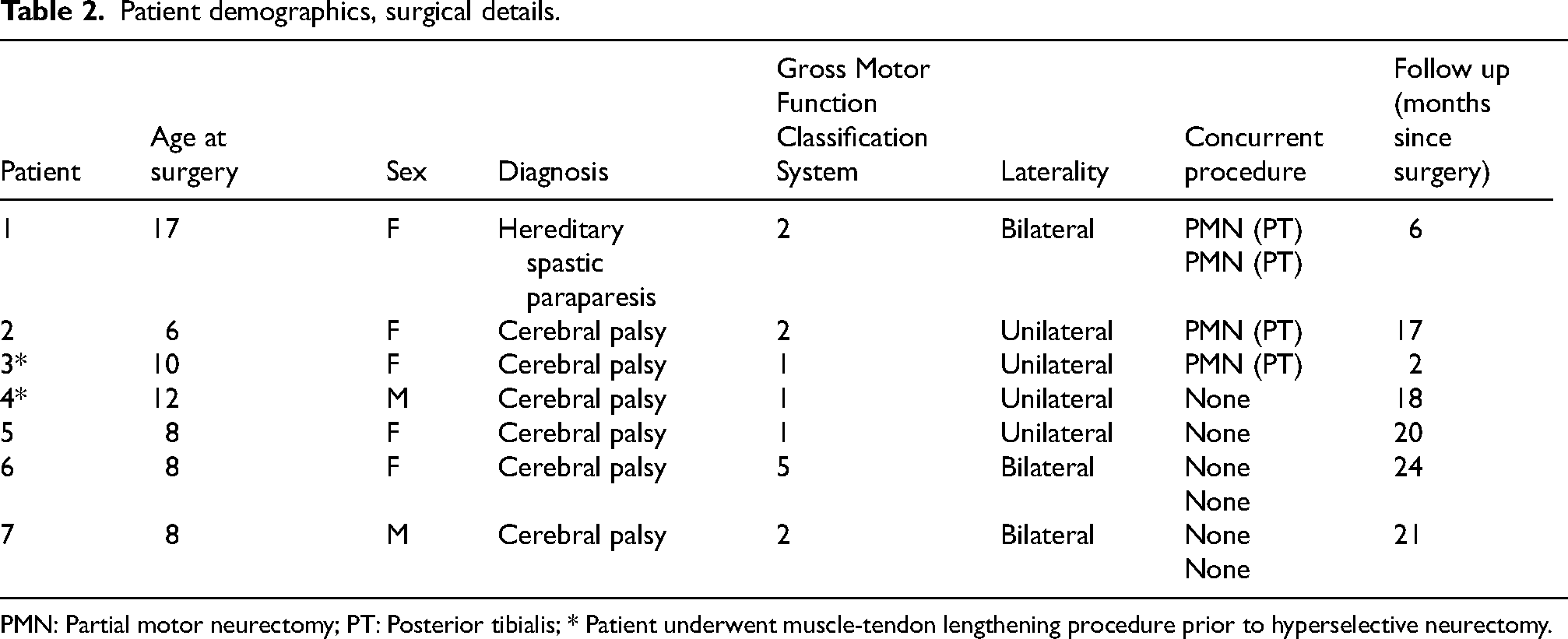
PMN: Partial motor neurectomy; PT: Posterior tibialis; * Patient underwent muscle-tendon lengthening procedure prior to hyperselective neurectomy.
Range of motion, spasticity scores.
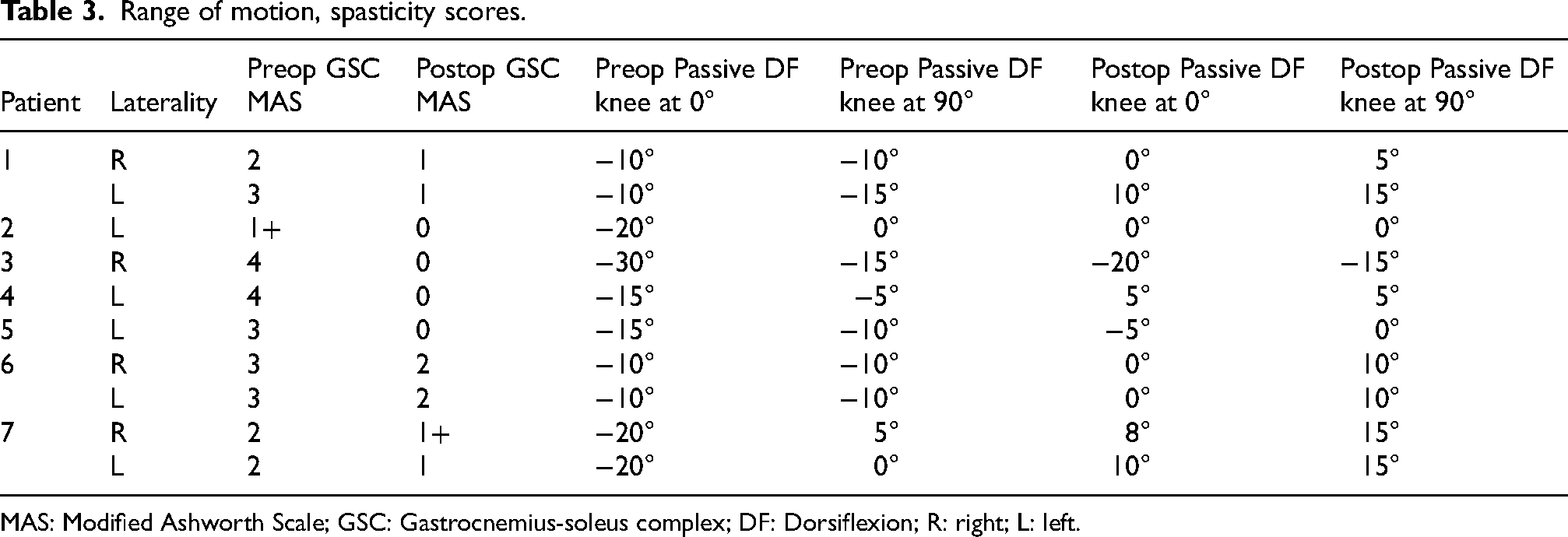
MAS: Modified Ashworth Scale; GSC: Gastrocnemius-soleus complex; DF: Dorsiflexion; R: right; L: left.
Summary counts of spasticity scores before and after surgery.
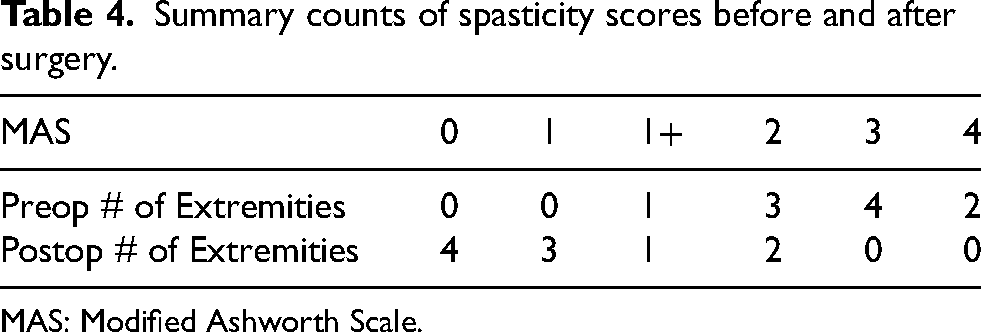
MAS: Modified Ashworth Scale.
Summary counts of extremities with various MAS grade improvements.
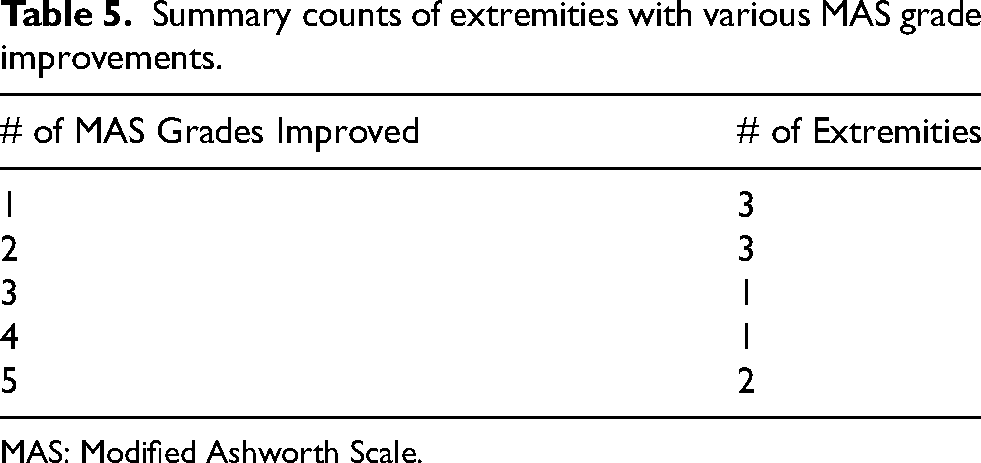
MAS: Modified Ashworth Scale.
Strength before and after surgery.
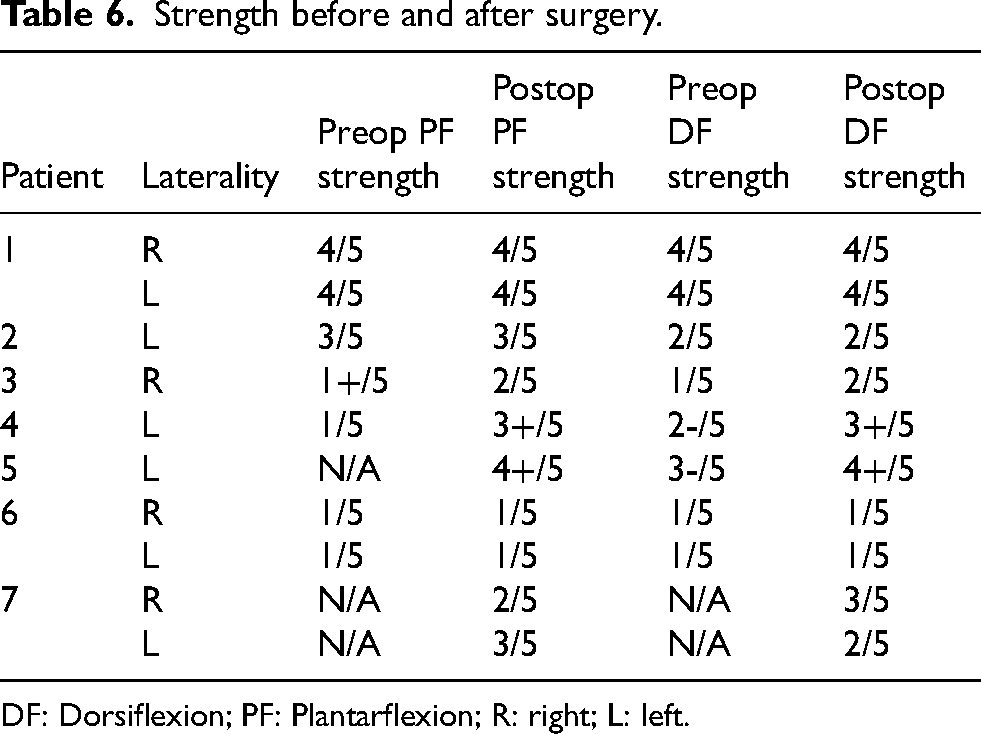
DF: Dorsiflexion; PF: Plantarflexion; R: right; L: left.
Status prior to intervention
All patients attempted treatment with botulinum toxin injections more than three months prior to HSN. Five patients noted substantial reduction in spasticity after botulinum toxin injections, while two patients reported no improvement of their spastic equinus deformity (patients 3 and 6). Two patients underwent prior surgery on the operative extremity, consisting of gastrocnemius fractional lengthening with percutaneous tendo-Achilles lengthening in one (patient 3) and gastrocnemius recession alone in another (patient 4, Table 2).
Six out of seven patients were ambulatory before and after surgery. One patient (patient 6) was non-ambulatory before and after surgery. GMFCS scores, noted in Table 2, remained unchanged for all patients after surgery.
MAS scores
At a mean follow up of 15 months (range: six to 24 months), all patients had a decrease in GSC MAS compared to their preoperative values. Preoperatively, 10% of extremities had a MAS of 1+, 30% had a MAS of 2, 40% had a MAS of 3, and 20% had a MAS of 4. Postoperatively, 40% of extremities had no residual spasticity, 30% had a MAS of 1, 10% had a MAS of 1+, and 20% had a MAS of 2 (Tables 3–5).
Range of motion (ROM)
All patients exhibited improved passive dorsiflexion ROM with the knee in extension with mean improvement of 17° (SD = 8°, p = 0.00009). Passive dorsiflexion with the knee in flexion had a mean 13° of improvement (SD = 9°, p = 0.002) (Table 3).
Strength
No patients exhibited a reduction in dorsiflexion or plantarflexion strength (Table 6). Three patients had stable strength as compared to their preoperative exams. Two patients displayed improved strength with both plantarflexion and dorsiflexion.
Complications
There were no major complications. One minor complication of wound dehiscence was successfully managed with local wound care and gentle compression; there was no clinical evidence of infection and antibiotics were not required. Loss of sensation and associated hyperalgesia was noted at an early postoperative appointment for one patient, with subsequent resolution without intervention.
Need for subsequent surgery
Four patients underwent staged subsequent muscle-tendon based surgery on the ipsilateral extremity (Table 7) which included gastrocnemius recession (patient 2), Achilles tendon, PT and flexor hallucis longus lengthening (patient 4), GSC lengthening and Achilles tendon lengthening (patient 5), and gastrocnemius recession on one leg and Achilles tendon lengthening on the other (patient 7, who had bilateral HSN).
Subsequent surgery of the ipsilateral lower extremity.
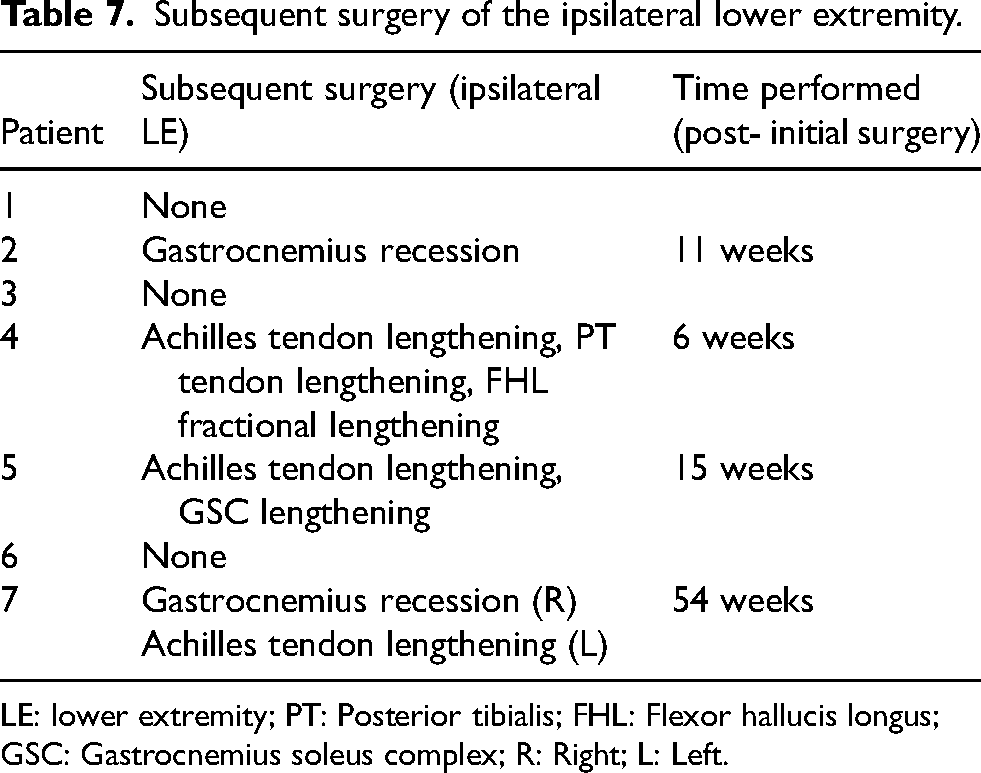
LE: lower extremity; PT: Posterior tibialis; FHL: Flexor hallucis longus; GSC: Gastrocnemius soleus complex; R: Right; L: Left.
Discussion
Previous studies have also explored selective motor neurectomy in the pediatric LE, though no specific outcome measures were reported.15,19,20 The current study found that HSN 1) effectively reduces spasticity in the GSC, 2) improves passive ankle dorsiflexion, 3) preserves strength and sensation and 4) is safe for pediatric patients in early-term follow-up.
Previous studies have demonstrated the safety and efficacy of HSN in the pediatric upper extremity. 10 Leclercq et al. prospectively examined pediatric patients who underwent HSN of the upper extremity. All patients had reduced spasticity and improved spontaneous posturing and self-reported functionality at a mean follow-up of 15 months. There were no immediate postoperative complications and long-term patient satisfaction was high.3,11,19–21
Several studies have examined partial motor neurotomy and selective motor neurectomy in the adult LE.3,11,21–23 Decq et al. prospectively examined adult patients who underwent partial motor neurotomy of the tibial nerve to the soleus and partial motor neurotomy of the PT and/or toe flexors if indicated. Spasticity was eliminated in 44 of 46 patients, and ankle ROM during gait was significantly increased. 22 Buffenoir et al. examined 55 patients with spastic equinus deformities who were treated with selective motor neurectomy of the tibial nerve to the soleus. Passive ankle dorsiflexion significantly increased from −0.56 degrees to +6.85 degrees, and gait speed significantly increased. Early complications were noted in five patients including wound dehiscence, reflex sympathetic dystrophy and transient deafferentation pain. No late complications were observed. 23 Sindou et al. reported on 53 patients who underwent selective motor neurectomy of the tibial nerve with 51 of 62 spastic feet having resolution of spasticity, associated total pain relief and improvement in voluntary movements for up to 10 years. 22
The primary aim of neurectomy/neurotomy is to reduce spasticity without excessively weakening the muscle. Anti-gravity motor strength, at the least, is expected to be preserved even after substantial axonotmesis when at least 20–30% of the motor pathway is left intact due to collateral sprouting of motor units. 24 HSN, targeting the terminal motor rami prior to inserting into the motor endplate, thus has a theoretical advantage of targeting the most distal portion of the nerve, allowing a high degree of selectivity and avoiding any unintentional denervation of non-target motor or sensory nerves. Of note, alpha motor neurons attempt to compensate for partial axonal loss by collateral sprouting of new axons, in which the size and duration of motor units action potentials increase on EMG proportionally with the amount of axons divided, thus indicating the reinnervation of denervated motor endplates.11,25 This may account for recurrence of spasticity after HSN while illustrating the need to resect a substantial proportion of motor axons at the index surgery.
In evaluating the utility of HSN for LE spasticity, it is necessary to compare it to well-established treatment modalities. SDR has been shown to effectively reduce spasticity and improve gross motor function in pediatric patients.26–28 The most common complication for this procedure is paresthesia, leading to dysesthesia or neuropathic pain in 6% of patients. 29 SDR may also increase the risk of developing progressive spinal deformity, particularly in non-ambulatory children. Other complications include bladder dysfunction, gastrointestinal dysfunction, and loss of motor function. 30 Furthermore, SDR is not selective for specific muscle groups, but rather performed for global spasticity of the LEs. While “focal” SDR techniques have been explored to limit dorsal rootlet sectioning to specific myotomes, the approach still affects multiple muscles due to overlapping innervation and lacks the fascicular-level precision afforded by HSN. Intrathecal baclofen reduces spasticity but is associated with infection, cerebrospinal fluid leakage and other serious complications.31–37 Additionally, patients require ongoing appointments for dosage adjustments, pump refilling and replacement. Chemodenervation including botulinum toxins, phenol, and alcohol injections, is effective but yields only temporary effects. Consequently, there is often repetitive administration under anesthesia to maintain efficacy, yet another disadvantage as it may be associated with adverse neurocognitive effects when administered to young children. 38 Given the risks of these treatments, HSN is emerging as an effective and long-term focal spasticity treatment option.
When evaluating patients with GSC spasticity, it is important to consider the presence or absence of contractures, as these conditions may necessitate further muscle-based surgical procedures. Patients that present with pure spasticity are ideal candidates for nerve-based surgeries such as HSN or SDR. Patients with spasticity and concomitant muscle contractures are best addressed with a staged approach involving HSN followed by muscle-tendon lengthening or transfers and joint releasing procedures. The patient cohort in the current study included a mix of these two distinct profiles, and as such, outcome should be interpreted with an awareness of this nuance.
HSN predominantly addresses spasticity but not contractures. 39 Patients that present with fixed deformities from predominant muscle and/or joint contractures require muscle lengthening and periarticular soft tissue release procedures. More restricted ankle dorsiflexion with the knee extended versus flexed indicates a gastrocnemius contracture. Patients with this finding may require additional interventions, such as muscle-tendon lengthening procedures, as was done in the patients who underwent subsequent procedures (Table 7). A critical concept is that nerve-based procedures, such as HSN, can effectively treat spasticity, a neurologically mediated process, and can optimize the outcome of muscle-based procedures by decreasing the underlying spastic tone.
Despite significant postoperative reductions in spasticity, no changes were observed in GMFCS levels. While spasticity reduction may improve joint mobility, comfort and ease of care, it does not necessarily translate to changes in GMFCS. The GMFCS is a broad functional measure that reflects a child's typical performance in everyday settings, which can be influenced by factors beyond spasticity—such as motor control, strength and coordination, and preexisting deformities. The GMFCS is known to be relatively stable over time, particularly in older children, and may not be sensitive enough to detect subtle improvements in mobility following isolated interventions. 40 As such, although spasticity reduction was achieved, its isolated effect may be insufficient to meaningfully alter a patient's functional classification within the GMFCS framework.
A multidisciplinary approach involving pediatric orthopedic, peripheral nerve, and foot and ankle surgeons, PMR physicians, and physical therapists is paramount in addressing spastic equinus deformity. In this cohort, patients initially consulted with PMR physicians and underwent non-operative treatments including botulinum toxin injections and oral muscle relaxants. Following a comprehensive assessment (including dynamic EMG and gait/motion analysis), a team of physiatrists and surgeons developed an individualized surgical treatment plan. HSN was followed by a six-month observation period and re-evaluation by pediatric orthopedic specialists to consider further optimization of functional outcomes through operative and non-operative modalities. Thorough evaluation by the appropriate disciplines ensures that all non-operative measures have been exhausted and allows for comprehensive surgical planning and follow-up care.
Limitations of this study include a small patient cohort with short-term follow-up. The latter is attributed to the destination medical practice that many ambulatory patients seek out. Additionally, post-operative dynamic EMG and gait analysis were not obtained but could have revealed changes in the muscle activation pattern and gait mechanics after HSN. The retrospective design and lack of a control group limit causal inference. Additionally, outcome assessments were performed by the treating surgeon in a non-blinded fashion, introducing potential assessor bias. The use of the MAS as originally described by Bohannon and Smith also presents limitations. 41 While widely used, the MAS is a subjective measure with variable inter-rater reliability.41,42 Future studies would benefit from prospective controlled designs, blinded assessment, objective functional testing, and more robust and reliable measures of spasticity and motor function.
There are a variety of surgical procedures that can improve GSC spasticity, ankle ROM, and gait in the pediatric population. Nerve-based procedures are ideal for spastic deformities; however, upstream targets for neurectomy, such as SDR, can result in sensory disturbances or weaken unintended muscles. HSN is performed at the distal terminal motor rami to mitigate occurrence of these complications. HSN for spastic equinus deformity is safe and effective in the short term for pediatric patients. However, this procedure should be examined in a larger population with long term follow-up to more definitively determine risks, benefits, and development of secondary deformities attributed to this procedure.
Footnotes
Acknowledgments
The authors have no acknowledgments
Ethical considerations
This study received ethical approval from the Mayo Clinic IRB (approval #22-009869) on 10/18/22. This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Author contributions
Lainey G Bukowiec: Primary author, writing and editing manuscript, data collection Kitty Y Wu: Writing portions of the manuscript and editing the manuscript Joline E Brandenburg: Writing portions of the manuscript and editing the manuscript Peter C Rhee: Conception of idea, writing portions of the manuscript and editing the manuscript
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.