
Abstract
Purpose
Following the Global Health Symposium at the Spina Bifida World Congress in 2023, the purpose of this work is to provide a historical overview and a state-of-the-art update on the current global practice of myelomeningocele (MMC) closure and to highlight the importance of care coordination and outcomes reporting to mitigate care fragmentation through a multidisciplinary approach.
Methods
Panelists from the Spina Bifida World Congress Global Health Symposium reviewed their institutions’ history and experience with risk for fragmentation of care following prenatal repair and proposed solutions to address fragmentation of care.
Results
New and rapidly evolving in-utero approaches to MMC repair are increasingly accessible for patients worldwide but bring more complexity to follow-up care. There is a consensus that unifying multidisciplinary practices and evaluations across institutions and countries will help make care coordination more comprehensive and longitudinal, and that meeting these standards may decrease care fragmentation.
Conclusion
Regardless of the open spina bifida repair technique, longitudinal follow-up must be established after fetal surgery, not only for the optimal care of individual patients but also to mitigate care fragmentation, transparently evaluate and compare techniques (for example, through the North American Fetal Therapy Network, the National Spina Bifida Patient Registry, etc.), engage health care professionals, and provide evidence-based multidisciplinary care.
Introduction
Myelomeningocele (MMC) is a severe form of open spina bifida, characterized by a failure of neural tube closure during the third week of gestation. The incidence of MMC is nearly 3.63 per 10,000 live births in the United States (US) and as high as 18.6 in 10,000 live births in some areas of the world. 1 This congenital malformation results in the herniation of the spinal cord and meninges through a defect in the posterior vertebral arches, and a leak of cerebrospinal fluid, forming an exposed sac. 1 Neurological deficits in MMC are explained through a “two-hit hypothesis.” 2 The first “hit” involves abnormal neurulation leading to incomplete closure of the neural tube. The second “hit” occurs later during the pregnancy, as the exposed spinal cord can be damaged by contact with amniotic fluid and the surrounding intrauterine environment. This prolonged exposure contributes to further spinal cord deterioration, exacerbating neurological impairment.3,4 MMC is also associated with a downwardly displaced cerebellum, part of the Chiari II malformation, which can obstruct and alter cerebrospinal fluid circulation, potentially leading to hydrocephalus and further worsening of the neurological prognosis. 5 Thus, MMC is associated with severe neurological damages, affecting a myriad of systems including bowel, bladder, and lower extremity function, that require lifelong care involving multiple subspecialties.
To minimize effects of the second “hit” and limit further neurological damage, prenatal MMC closure surgery during the second trimester of pregnancy has been developed.3,6,7 Prenatal MMC closure has been shown to improve motor function and reduce the need for hydrocephalus treatment after birth compared to postnatal MMC closure. Moreover, given the compounded challenges that individuals with MMC face when they belong to historically underserved populations, a “three-hit model” has been proposed, conceptualizing the third “hit” as adverse social determinants of health. 8 Social determinants of health, which are modifiable contributors to outcomes, include health-related behaviors, socioeconomic aspects, and economic factors.9–12 To explore differences in social determinants and practice experience, panelists from the Global Health Symposium (representing five continents) at the Spina Bifida World Congress in 2023 reviewed their institutions’ history. They also reviewed their experience with risk for fragmentation of care following prenatal repair and proposed solutions to address fragmentation of care. As an extension of this symposium, the purpose of this work is to provide a historical overview and state-of-the-art update on the current global practice of MMC closure and follow-up, as well as to highlight the importance of care coordination and outcomes reporting to mitigate care fragmentation through a multidisciplinary approach.
Development of neonate and the postnatal closure approach
Over the last century, the treatment of MMC has included surgical closure of the defect shortly after birth, along with supportive care. Postnatal repair remains the standard of care globally, as prenatal repair is a relatively new technique available primarily in specialized centers. Typically, to reduce the risk of infection and minimize the time the spinal cord is exposed, neonates undergo neurosurgical closure within the first 24–48 h of life. 13 Through postnatal repair, pediatric neurosurgeons aim to protect the exposed neural elements and prevent additional cerebral spinal fluid leakage and risk of infection.14,15 Postnatal closure has not been shown to restore neurologic function. The long-term prognosis of neonates who undergo postnatal repair depends on a variety of factors, including the level of the lesion, severity of Chiari II malformation, and presence of hydrocephalus. 16 People living with MMC experience a variety of neurologic and developmental sequela, such as hydrocephalus, ventriculoperitoneal shunt-related complications, developmental delay, lower urinary tract infections, pyelonephritis, renal dysfunction, bowel incontinence, paraplegia, tethered cord syndrome, orthopedic malformations, and seizures, as well as endocrinologic, sexual, sleep, and psychosocial issues.4,17–20 Among neonates who undergo postnatal repair, approximately 66–75% survive to early adulthood.21,22 Causes of death, most of which occur during infancy and the preschool years, 18 are associated with hindbrain dysfunction, shunt-related complications, and cardiorespiratory or urologic reasons.18,23 While immediate postnatal neurosurgical intervention is paramount, longitudinal care at a local medical center and follow-up by trained multidisciplinary teams throughout the lifespan have become essential components of evidence-based care.
Development of the open-hysterotomy prenatal closure approach
Building on the work by Meuli-Simmen et al., the Management of Myelomeningocele Study (MOMS) was conducted at the Children's Hospital of Philadelphia, Vanderbilt University, and the University of California, San Francisco. In 2011, the study demonstrated that prenatal repair of MMC via open-hysterotomy, as compared with postnatal repair, provided a variety of benefits.13,24 In particular, data from MOMS showed that prenatal repair conferred a 50% reduction in the need for postnatal shunt placement (82% in the postnatal surgery group vs. 40% in the prenatal surgery group, p < 0.001) and a significant improvement in motor function at 30 months of age demonstrated by a higher rate of independent ambulation (42% vs. 21%, p = 0.01). 13 Additionally, the proportion of infants with evidence of complete hindbrain herniation reversal at 12 months of age was greater in the prenatal surgery group than in the postnatal surgery group (36% vs. 4%, p < 0.001). 13
A follow-up study, MOMS-II, assessed the original MOMS cohort at school age (5.9–10.3 years). Regarding neuromotor outcomes, the benefit of prenatal repair persisted, but differences in independent ambulation became less pronounced (29% vs 11%, p = 0.06). Furthermore, among children who needed shunt placement, those in the prenatal group had fewer shunt revisions (47% vs. 70%, p = 0.02). Neurocognitive outcomes, such as adaptive behavior and cognitive functioning, were not different between the two groups. Importantly, parents of children who underwent prenatal repair reported relatively improved child quality of life. 25
While prenatal repair of MMC via open hysterotomy has been documented to provide the aforementioned benefits, this approach is also associated with maternal morbidity. Open hysterotomy is a more invasive procedure leading to an increased risk of bleeding, infection, and postoperative complications for the mother. Moreover, this technique involves the incision of the uterus, creating a significant scar, which can increase the risk of uterine rupture in future pregnancy and requires scheduled cesarean section for subsequent deliveries.13,26–29 Indeed, 35% of mothers who underwent open hysterotomy were found to have uterine dehiscence at the surgical site at the time of cesarean delivery. 13 A study by Goodnight et al. reported a 10% risk of uterine rupture in the subsequent pregnancy, which occurred between 26- and 32-weeks’ gestation, resulting in fetal demise in 2 of 5 cases. 27 Additional pregnancy complications such as chorioamniotic membrane separation, oligohydramnios, placental abruption, and prelabor premature rupture of membranes (PPROM) are increased after open hysterotomy procedures. 16 Lastly, along with occasional fetal loss, when compared to postnatal repair, patients in the prenatal repair group delivered earlier (34.1 weeks vs. 37.3 weeks), with an increased risk of severe prematurity, defined as birth before 30 weeks of gestation (13% vs. 0%). 13
Development of the prenatal fetoscopic laparotomy-assisted closure approach
To reduce maternal morbidity related to open hysterotomy repair, alternative minimally invasive approaches have been developed. Texas Children's Fetal Center/Baylor College of Medicine contributed to the development of a two/three port, multi-layer fetoscopic MMC repair technique through a laparotomy-assisted approach. 30 Under maternal general anesthesia, this technique consists of making an abdominal incision to expose the uterus, which is then exteriorized. The amniotic fluid is subsequently removed and replaced with carbon dioxide gas. The ports are placed into the uterus and the scope and instruments are inserted through them. The membrane attached to the exposed spinal cord is dissected and a patch is placed over the defect. Muscles and skin are then sutured over the patch to protect it further. Compared to the open hysterotomy technique, this fetoscopic approach has demonstrated improved maternal outcomes, including a lower risk of uterine rupture, the possibility of vaginal deliveries, and a decreased rate of preterm birth. 16
Development of an outcomes reporting consortium
This new hybrid approach, which combines open and fetoscopic techniques by exteriorizing the uterus but using fetoscopy to close the MMC, exemplifies the variability of prenatal repair options for MMC around the globe (Table 1). Furthermore, a variety of minimally invasive fetoscopic techniques have been developed, including total percutaneous fetoscopic repair and percutaneous-minilaparotomy fetoscopic repair.31–33 Although these approaches differ, the overall aspects of fetal repair are relatively consistent and produce similar outcomes as closure by open hysterotomy. Thus, innovation in minimally invasive procedures has increased the global variability of prenatal repair options for MMC, making the evaluation, interpretation, comparison, and specific neonatal management between different techniques more complex.
Comparison of myelomeningocele (MMC) repair techniques.
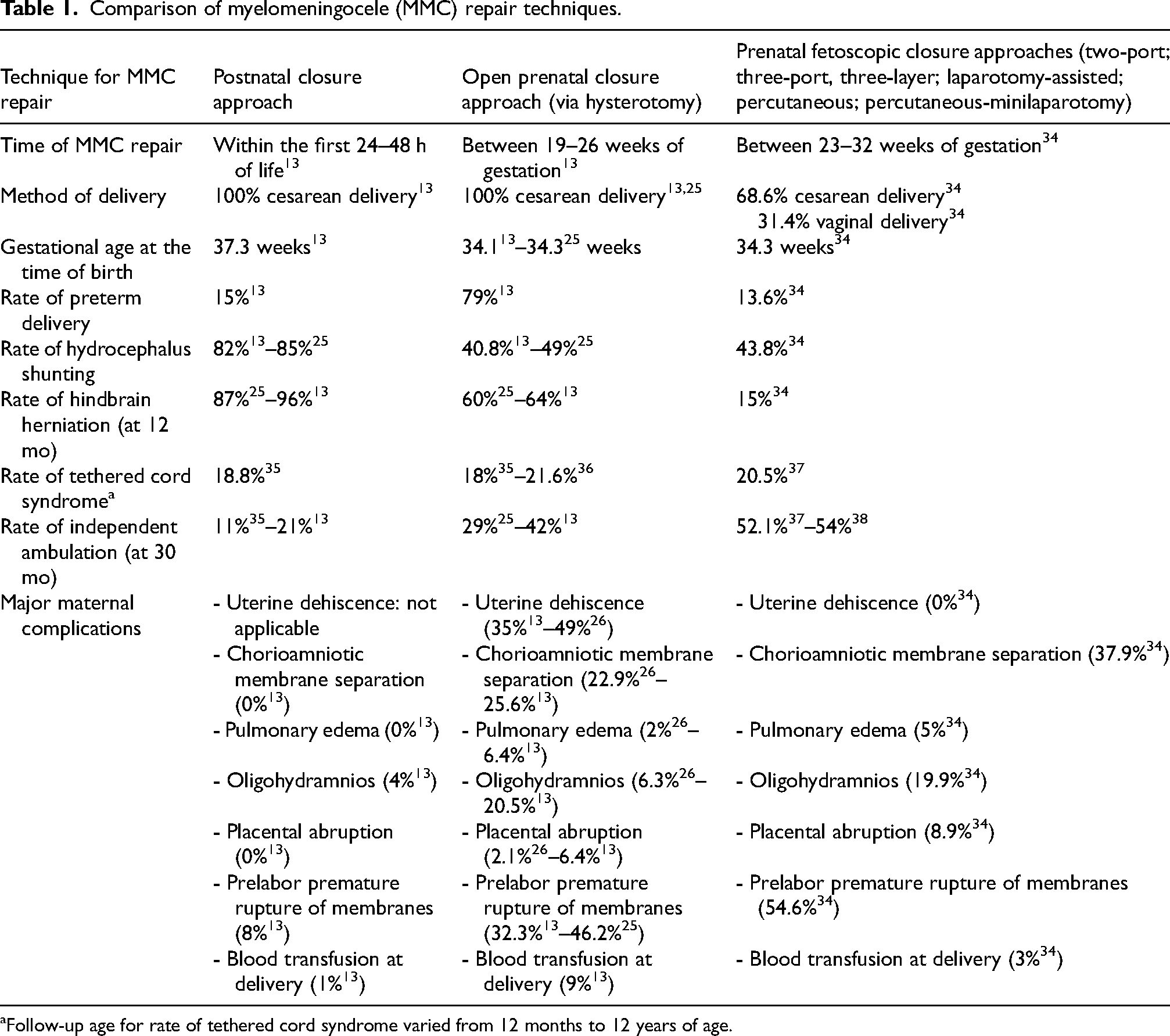
Follow-up age for rate of tethered cord syndrome varied from 12 months to 12 years of age.
Therefore, aiming to better understand which components of each technique are more beneficial in improving outcomes, the International Fetoscopic Myelomeningocele Repair Consortium was established in 2018. 34 The initial related study included 300 patients from 14 centers. The cohort included participants who underwent prenatal fetoscopic repair by laparotomy-assisted fetoscopic or total percutaneous fetoscopic approaches. The work aimed to assess the core obstetrical, perinatal, and neurosurgical outcomes up to 12 months of age and to compare these outcomes with those observed after open hysterotomy MMC repair as reported in the MOMS cohort.13,26 Patients who underwent fetoscopic repair (of any type) delivered at an average gestational age of 34.3 weeks, which was similar to the average delivery gestational ages for those who underwent open hysterotomy repair in the MOMS and post-MOMS studies (34.1 weeks and 34.3 weeks, respectively).13,26 However, fetoscopically repaired mothers demonstrated a significantly higher percentage of vaginal delivery (31.4% vs. 0% in the MOMS trial and post-MOMS trial studies). It is theorized that fetoscopic surgery allows for later vaginal delivery as performing the repair through small incisions in the uterus minimizes damage to the uterine wall, as compared to the larger incisions required in traditional open fetal surgery.
Patients who underwent fetoscopic repair did have a greater risk of prelabor premature rupture of membranes compared with those who underwent open hysterotomy MMC repair (54.6% vs. 32.3–46.2% in MOMS and post-MOMS, p < 0.0002),13,26,34 and higher rates of placental abruption (8.9%, p = 0.02), chorioamniotic membrane separation (37.9%, p = 0.01), and oligohydramnios (19.9%, p < 0.01) compared to the MOMS trial. 34 However, the incidence of pulmonary edema, placental abruption, chorioamniotic membrane separation, and oligohydramnios was not significantly different between the fetoscopic registry and the MOMS. Conversely, the frequency of dehiscence at the time of cesarean delivery was greater in the MOMS (34%) and the post-MOMS (49%) studies compared to the fetoscopic registry (0%). The need for post-partum maternal blood transfusion was 3.5-fold higher in the MOMS group.
Development of concerns regarding longitudinal follow-up beyond prenatal repair
The MOMS trial inspired spina bifida care communities worldwide to expand access to open fetal surgery for MMC. Proliferating fetal therapy centers (FTCs) now offer this option. However, as surgical techniques for prenatal MMC closure continue to evolve and advance, critical consideration of both the positive effects and complications are ethically imperative. Despite significant improvement in neurological outcomes, prenatal MMC repair is not a cure and affected children will still experience neurologic, cognitive, bowel, and bladder morbidity, and require lifelong medical care. Fetal interventions are completed at a relatively smaller number of institutions, leading many families to travel outside of their geographical areas. When they return home, it is crucial that those who follow these children in local institutions are well-informed about the advancements, outcomes, and potential complications associated with these new techniques.
Regarding neurological outcomes, the two groups (fetoscopic vs. open hysterotomy) had similar neurological presentation at the time of surgery and at 12 months of age. Short-term adverse neurologic outcomes occurred in 43.8% of patients who underwent fetoscopic repair requiring a ventriculoperitoneal shunt, compared with 40.8% of patients in the original MOMS cohort.13,34 More recently, several collaborating centers have published long-term neurologic outcomes measured at 30 months of age. These outcomes demonstrate no difference between those with fetoscopic (52.1%) vs. open (51.4%) prenatal repair (p = 0.66), 37 compared with a 42% independent ambulation rate in the original MOMS cohort at 30 months of age. 13 Lastly, 61% of patients who underwent total percutaneous fetoscopic repair demonstrated independent voiding without clean intermittent catheter use at 30 months of age 38 compared with 38% of patients after open prenatal repair (mean age 7.4 years). 13
Notably, 20.5% of the children who undergo fetoscopic repair are expected to require re-intervention for spinal cord detethering, as the rate of secondary tethering is increased following prenatal repair compared to postnatal repair.13,37 Symptomatic tethered cord can be heralded by changes in bowel and bladder function, lower extremity function/positioning, and pain in the back/lower extremities. Raising awareness of these more frequent complications among the professionals who care for children at institutions where fetal surgeries are not performed (in addition to family education) will facilitate early detection and, consequently, better management, leading to improved outcomes and quality of life. To this end, multidisciplinary long-term follow-up programs will help improve the management and follow-up of patients who have undergone in-utero surgery.
Overall, outcomes after fetoscopic and open fetal surgery repair of MMC are similar at up to 12 months of age. However, fetoscopic repair provides significant advantages in terms of maternal health and obstetric complications, since it allows vaginal delivery and is not as highly associated with dehiscence of the uterine scar. 34 Avoiding complications associated with hysterotomy benefits both the index and subsequent pregnancies and is especially preferred for patients in lower resource settings 34 since cesarean delivery is not required in the index or subsequent pregnancy. Fetoscopy also eliminates the risk of uterine rupture,27,39 and lessens the risk of developing placenta accreta, of which hysterotomy is one of the main risk factors.27,39–42
Global development of collaboration between fetal centers and cohorts
To facilitate the acquisition of knowledge, keep up with new developments, standardize practices, and improve postnatal care coordination, it is essential to unify practices and evaluations across institutions. This can be achieved by consolidating outcomes in collaborative registries and developing comprehensive training programs. Such programs should include simulation exercises, evaluation methods, research initiatives, and quality improvement strategies. Implementation of these measures can ensure that practitioners remain informed about advancements, achieve consistent outcomes, and continuously enhance the quality of care provided.
Beyond North America and Europe, experts from four established FTCs in Thailand, Hong Kong, India, and Singapore established the Singapore Consensus, a framework for prenatal surgery for MMC in Asia. 43 The consensus recommendation was to develop a regional approach for addressing the issue of follow-up for prenatal surgery for MMC, one that supports case pooling and reasonable resource allocation. 43 The goal is that this framework can be applied to other parts of Asia, and perhaps other parts of the world that are beginning to offer prenatal surgery for MMC. Creating a standardized approach for the establishment of prenatal surgery for MMC in Asia, and perhaps far beyond that region, helps ensure that the expanded use of these interventions is accompanied by consistent diagnosis and management, thus continuously improving long-term outcomes for children with MMC.
The Singapore Consensus set forth a practical stepwise protocol for establishing FTCs throughout the region. This international recommendation stressed five elements of focus: (1) measuring the impact of MMC in Asia, (2) setting a standard for appropriate training for in-utero repair, (3) establishing best practices for operationalizing a local FTC (e.g., defining organizational reach, setting up counseling programs, managing personnel, developing surgical skills, expanding existing programs), (4) collecting short- and long-term follow-up data, and (5) documenting regional issues affecting adoption of this procedure. 43 It is key to note that the Singapore Consensus calls for the development of a team to provide longitudinal follow-up. In the US and Europe, it is recognized that many families travel significant distances to seek care and monitoring post-operative outcomes back home is paramount for these new technologies.
Development and role of a multidisciplinary team
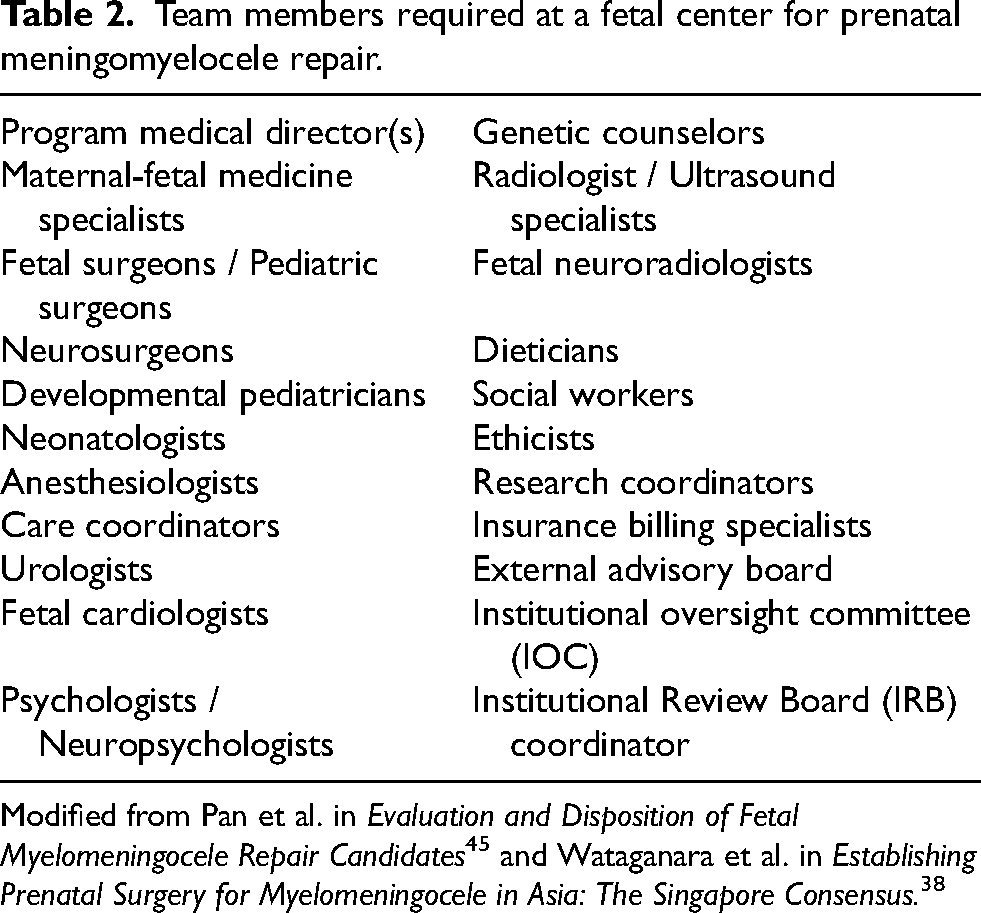
Since publication of the MOMS in 2011, offering the option of prenatal repair for spina bifida has become common in the US. The provision of family-centered counseling with an emphasis on shared decision-making is critical to convey the maternal and pregnancy risks associated with the open versus fetoscopic maternal-fetal surgery techniques. In the US, the Spina Bifida Association supports a standard of care that involves a multidisciplinary approach to longitudinal follow-up. 44 However, as more fetal centers are providing prenatal repair for MMC, there is an increasing risk of fragmentation in care. 43 Multidisciplinary care for pregnant patients with fetuses affected by MMC is essential, and continuation of this care post-delivery and throughout the lifespan is of equal importance (Table 2).
Team members required at a fetal center for prenatal meningomyelocele repair.
Irrespective of prenatal repair status, multidisciplinary lifespan care for children, adolescents, and adults living with spina bifida is key to optimizing outcomes and quality of life. Longitudinal neurologic surveillance is critical for monitoring signs of deterioration, including shunt complications and tethered cord syndrome.18,46–49 Lifespan urologic care is important to ensure and protect postnatal renal, bladder, and bowel function.50–53 Orthopedic care to address foot or other musculoskeletal deformities include bracing, surgical intervention, physical therapy, assistive technology, and other rehabilitation services, with the goal to facilitate ambulation and improve positioning if possible.54–56 Sexual health concerns emerge in adolescence and adulthood, and greater than 60% of individuals living with spina bifida report experiencing some degree of sexual dysfunction.45,57–60 The literature indicates that improvement in physician communication and awareness regarding patient education and treatment options is warranted (Figure 1). 16 Within the US, the National Spina Bifida Patient Registry (NSBPR) provides a network of multidisciplinary clinics that could offer the opportunity to further compare outcomes in participating individuals after a fetal surgery. 8 This registry collects information from a national sample containing thousands of individuals with spina bifida to understand the associations between medical procedures and health outcomes. It has already begun to compare neurosurgical outcomes of individuals who had an in-utero repair of MMC. 61 Thus, longitudinal follow-up is needed through transnational multicenter collaborations (e.g., the International Fetoscopic Myelomeningocele Repair Consortium, NSBPR, North American Fetal Therapy Network [NAFTNet], Latin American Spina Bifida Consortium, etc.) to compare outcomes of all techniques (both pre- and postnatal) across institutions.35,62
Guide to spina bifida for expectant and new parents – reused with permission from the Spina Bifida Association. 63
In addition to medical subspecialty care, people living with spina bifida typically benefit from a myriad of additional services, including social work; neuropsychology; nutrition; physical therapy; occupational therapy; seating, positioning, and/or bracing; transition; and family support services. 36 Comprehensive and longitudinal care coordination is essential for organizing these services (including imaging and laboratory studies), with the overarching goal of maximizing the health and quality of life of individuals living with spina bifida. 64 Care coordinators are responsible for facilitating visits with medical and surgical subspecialists during the clinic day, planning future clinic visits with providers, and sharing information with patients and families about the wide array of community resources that are available. The literature indicates that effective care coordination provides tangible benefits for families, including more robust connections with community resources, enhanced understanding of the goals for care, increased communication, and stronger relationships with health care providers. 65 Overall, these benefits help to reduce caregiver burden, improve access to and continuity of care, increase self-care and independence, and facilitate holistic care for individuals living with spina bifida. 36
Conclusions and future directions
Regardless of how, where, or when an MMC is repaired, multidisciplinary longitudinal follow-up is needed in collaboration with consortiums and registries (e.g., the International Fetoscopic Myelomeningocele Repair Consortium, NSBPR, Latin American Spina Bifida Consortium, NAFTNet, etc.) to consolidate and compare outcomes between techniques across centers. This is particularly critical in light of the growing fragmentation of care experienced by many families as they travel to undergo prenatal surgeries outside their home institutions. Therefore, a plan for longitudinal follow-up care must be established after fetal surgery in order to mitigate fragmentation, evaluate and compare techniques, engage health care professionals, and provide evidence-based multidisciplinary longitudinal outcomes reporting in the era of prenatal repair.
Footnotes
Acknowledgment
We remain indebted to Dr Nienke Dosa and the Spina Bifida Global Learning Collaborative for their vision, guidance, and support of a transnational dialogue on improving spina bifida care.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.