
Abstract
Purpose
This project aimed to describe the current status and future needs for the management of pediatric neural tube defects (NTDs) at a referral center in Mwanza, Tanzania, and thus can offer a model for other affected areas in sub-Saharan Africa.
Methods
A descriptive study design was used to collect and describe data from pediatric patients with NTDs admitted to and treated at Bugando Medical Center in collaboration with Mwanangu Development Tanzania in Mwanza, Tanzania.
Results
Between January 2018 and August 2022, a total number of 3160 children with NTDs presented to a referral medical center. Thirty-one percent of the patients were from Mwanza, 13% from Geita, 11% from Tabora, 10% from Simiyu, and the rest came from more distant regions of Tanzania. Hydrocephalus and spina bifida were the most common NTD diagnoses recorded that required ventriculoperitoneal shunt interventions in the neurosurgical services.
Conclusion
Early neural development disorders are common in sub-Saharan Africa, with spina bifida and hydrocephalus being the most prominent NTDs. The treatment and special education of affected children and adolescents are major public health challenges. As the development of protocols and guidelines for neurosurgical procedures is needed to improve the burden of pediatric hydrocephalus in sub-Saharan Africa, a report on how this is done simply, practically, and effectively here at a referral medical center in Tanzania may benefit countries with similar health issues.
This study was approved by the Regional Ethic Review Board in Mwanza Tanzania (Certificate No. CREC/682b/2023).
Introduction
Myelomeningocele arises from a disorder in development of the nervous system. Neural tube defects (NTDs) are major causes of fetal loss and considerable disabilities in infants. In sub-Saharan Africa (SSA), spina bifida myelomeningocele is a major cause of disability among adolescents. Multiple factors are involved in the development of NTDs, which are thought to result in part from environmental factors such as nutritional deficiency, poverty, maternal health, and genetic susceptibility. 1 In a systematic review analysis, the worldwide prevalence of NTDs was estimated and diagnoses of spina bifida, anencephaly, and encephalocele were found to be increased in lower-income countries, with a prevalence of NTDs in Africa of 11.7 per 10,000 births. 2 Spina bifida is a general term for NTDs affecting the spinal cord. In a recent review analysis, the prevalence of spina bifida was determined to be 0.13% in Africa overall and 0.26% in Tanzania. 3 Hydrocephalus remains one of the most commonly treated neurosurgical conditions worldwide. Almost one-half of the estimated 400,000 new global cases of pediatric hydrocephalus annually are expected to occur in Africa.4,5 There are preventable cases of NTDs due to a lack of awareness of risk factors, maternal folate deficiency, and poverty. A study of mothers of children with spina bifida and hydrocephalus in Tanzania determined that the mother's diet was predominantly maize-based, and only 3% had taken folic acid supplements. 6 Untreated hydrocephalus has a high mortality rate of 20%–87%. 7 Complicating matters further is the need for life-long follow-up care after neurosurgery, which is a major problem in rural Africa with low accessibility to hospitals and emergency services. In Tanzania, infants with NTDs often present late to the neurosurgery service. Delayed closure of myelomeningoceles increases the risk of cerebrospinal fluid leak, central nervous system infection, and postinfectious hydrocephalus. Further serious consequences are cognitive impairments and physical disabilities. Health strategies to improve outcomes of pediatric hydrocephalus include the availability of early neonatal neurosurgery.
Neurosurgical services have been offered in Tanzania since the early 1970s.8,9 Global health initiatives were established, 10 multi-institutional neurosurgical training programs were held, 11 and a surgical database was created in Mwanza. 12 Thus, neurosurgical competencies and qualifications were already well established in the Bugando Medical Centre (BMC), located in Mwanza. 13
The BMC is a government-funded and patient cost-shared referral center and is one of two tertiary care hospitals in the country providing neurosurgical care to the rural Lake and Western regions of Tanzania. The referral area for the BMC captures approximately 13 million people and about 600–800 children are treated annually in association with NTDs. In cross-sectional studies, pediatric hydrocephalus patients receiving ventriculoperitoneal shunt (VPS) insertions in the BMC were described in 38 cases in 2013 14 and in another published study in 125 cases, treated in 2016. 15
The development of guidelines and feasible protocols for neurosurgical procedures is necessary to reduce the complications, disability, and mortality associated with pediatric hydrocephalus in SSA. Currently, at the BMC in Mwanza, Dr Gerald Mayaya from the Department of Neurosurgery has developed a surgical protocol and guideline concept including a peri- and post-operative care program to minimize complication rates and shunt-related morbidity in children. This observational study is the first presentation of data collected on children with NTDs in Northwest Tanzania, presented to the BMC in Mwanza.
Methods
This is a descriptive study of sampled data from pediatric patients with NTDs who presented at the BMC between January 2018 and August 2022. Patients with NTDs in the surrounding regions are usually referred to the BMC, which specializes in neurosurgery. Mwanangu Inclusive Community was founded by Mwanangu Development Tanzania (MWADETA), a non-governmental organization (Reg. No 00NGO/00010215) that supports the needs of vulnerable children in Tanzania. Within the MWADETA network, a rehabilitation unit, the House of Hope, has been established to provide peri- and post-operative care and long-term rehabilitation to children and their families, complementing clinical treatment at the BMC in Mwanza. Age, geographic origin, demographics, and clinical data were collected at the BMC and in collaboration with MWADETA using data sheets. All descriptive statistical analyses were performed using Excel 2010 (Microsoft, Redmond, WA, USA).
This study complies with principles laid down in the Declaration of Helsinki 16 and was approved by the BMC and Catholic University of Health and Allied Sciences (CUHAS), the ethical committees of Mwanza, Tanzania (research clearance certificate number CREC/682b/2023).
Results
Here the first data from a large neurosurgical medical center with more than nine supra-regional referral outpatient centers is presented (Figure 1). Between January 2018 and August 2022, a total number of 3160 hydrocephalus patients presented to the neurosurgical services of the BMC and were treated in relation to VPS insertions. Most patients (31%) were inhabitants of Mwanza, 13% came from Geita, 11% from Tabora, 10% from Simiyu, 9% from Mara, and the remainder came from more distant regions of Tanzania (Figure 1). Twenty-five percent of patients were younger than six months, 34% were between six and 24 months, and 57% were male (Table 1). The patients had different combinations of NTD diagnoses and various reasons for visiting the referral center. Hydrocephalus and spina bifida were most commonly diagnosed. Other NTD diagnoses included anencephaly, encephalocele, and combined or unspecified diagnoses. In some cases, the exact diagnoses and specifications were unfortunately not clearly recorded. Hydrocephalus requiring VPS intervention was noted in 84% of the listed cases. In 814 of the cases (26%), spina bifida was explicitly reported as a reason for treatment interventions.
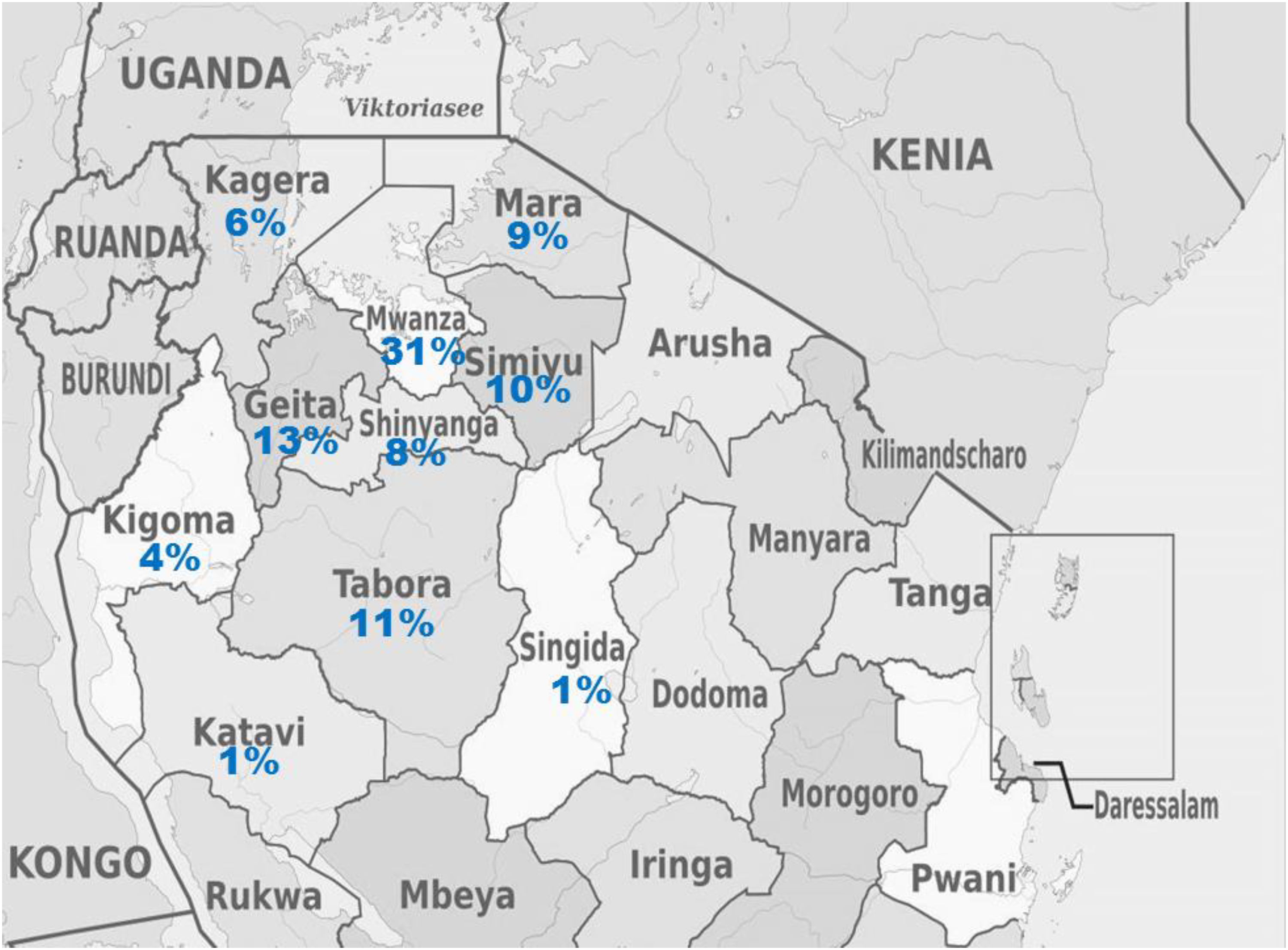
Map of study area of pediatric neural tube defects in the Bugando medical center in Mwanza in Tanzania. The percentages of origin of the patients treated at BMC in Mwanza, Tanzania, are as indicated. (Map images are adapted from https://de.maps-tanzania.com).
Summary of the patients with neural tube defects.
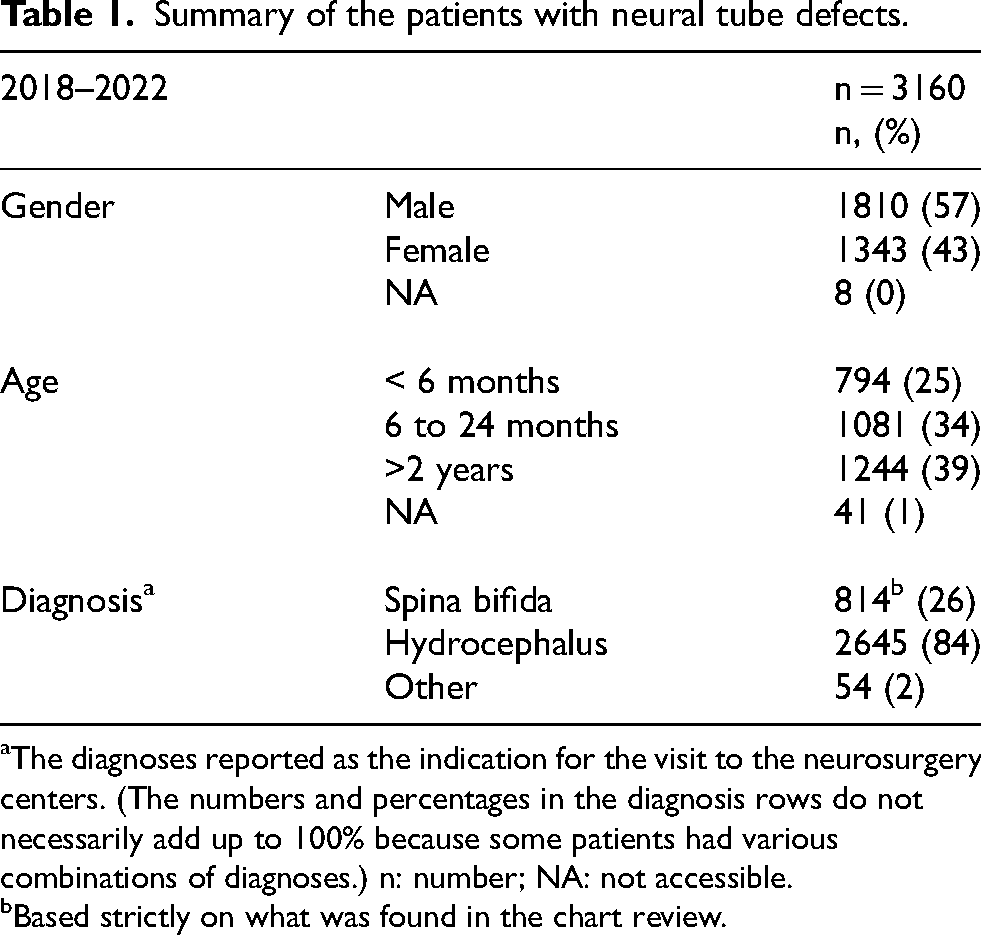
The diagnoses reported as the indication for the visit to the neurosurgery centers. (The numbers and percentages in the diagnosis rows do not necessarily add up to 100% because some patients had various combinations of diagnoses.) n: number; NA: not accessible.
Based strictly on what was found in the chart review.
Discussions
Myelomeningocele is a severe congenital anomaly of the central nervous system. The health burden of hydrocephalus in infants is substantial in SSA, requiring neurosurgical interventions. It is estimated that 200,000 newborns are diagnosed with or born with NTDs in Africa each year. Less than 10% of them are provided with VPSs, and those who do receive a shunt generally do so under poor conditions and with a very high complication rate. 5 The prevention and treatment of pediatric hydrocephalus in SSA should be recognized as an important public health priority issue. The placement of a VPS is the standard of care for treating pediatric hydrocephalus, but the high long-term risk of failure makes shunt dependency problematic in low-resource settings if emergency neurosurgical care is limited. Endoscopic third ventriculostomy (ETV) with or without choroid plexus coagulation (CPC) is an appealing alternate strategy that avoids long-term complications associated with shunts. 17 As part of a global public health initiative, the CURE protocol was developed in Uganda and employs endoscopic treatment, rather than shunt placement, as the primary approach. 18 In an initiated longitudinal prospective study, the clinical outcomes of 300 cases of pediatric hydrocephalus in Uganda treated with ETV/CPC will be followed and analyzed in detail. 19 There is uncertainty regarding the relative benefits of the treatment of hydrocephalus with VPS or ETV. Shunting is technically simpler and has a lower rate of failure in the months immediately after surgery than endoscopic procedures but is more prone to complications in the long term. 20 The complication rate for pediatric hydrocephalus shunts was reported to be 40%. 21 An overall complication rate of 33.6% (with a median follow-up of 36.9 days) was reported in 2016. 15 Unfortunately, the number of deaths, usually due to complications, is also to be noted, with overall mortality rates of 15–20%.8,15
Evidence from studies in Uganda suggest that treatment of hydrocephalus in infants can be effective and sustainable in a developing country. 22 Since VPS infections are still among the most common complications and risks of death, the implementation of organized perioperative protocols and care and treatment concepts to minimize such infections were proposed. 15 Also, in a study of a surgical institute in Zanzibar, a series of perioperative care protocols were described and implemented in hydrocephalus patients to achieve better outcomes. 23
In order to evaluate the effectiveness of hydrocephalus interventions in rural areas of SSA in the future, it is important to obtain high-quality data. Therefore, a future project in Tanzania is planned to follow up on the interventions, care, nutrition, education including preventive folic acid intake, and outcomes of children with NTDs who are treated at the BMC over the next years.
A limitation of this study is that there has not yet been systematic registration and complete collection of clinical data on all cases treated. The risk of bias due to underreporting can be reduced by prospectively collecting evidence-based clinical data and systematically monitoring disease progression and follow-up. To this end, a registry database should be established to prospectively and systematically record treated NTD cases and clinical parameters of a large number of affected children (approximately 600–800 per year). It is anticipated that these assessments will contribute to future progress in the health, care, and education of children with NTDs, not only in Tanzania, but also in other affected African countries.
Conclusions
In conclusion, the development and implementation of a guideline protocol for preoperative, perioperative, and postoperative procedures, as well as nutrition education, nursing care, and interventions are needed. Practical solutions that have already been introduced in other countries in SSA15,19,23 and can be implemented in emergency departments are particularly important and are not only limited to the hydrocephalus surgery, but also to the long-term health care that follows. Such concepts should be developed and integrated into the training of medical staff with specialized nursing and anesthesia personnel. This study is a novel report of more than 3000 children with hydrocephalus from a high-volume African clinic. This systematic and structured documentation of surgical procedures in an established registry study at a referral medical center in Tanzania will be the first real-world data collection of its kind and can also serve as an example for future healthcare research in other affected countries. Furthermore, follow-up care for these children who have undergone surgery is also planned, and long-term outcomes would also be monitored as part of rehabilitation projects. This may help to achieve future improvements for children with hydrocephalus and their families in other affected areas.
Footnotes
Acknowledgements
We would like to thank the staff of the BMC and MWADETA for data collection. Mwanangu Development Tanzania, Child Help International, ASBAHT, Bugando Medical Centre, Director General, Research Department CUHAS, Vice Chancellor of CUHAS, Nurse C6, theatre nurse, Pediatrics Department, neonatal unit, House of Hope Nyegezi and Kitongo, Desk and Chair Tanzania.
Ethical considerations
This study was approved by the Regional Ethic Review Board in Mwanza Tanzania (Certificate No. CREC/682b/2023).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.