
Abstract
Purpose
This study aimed to survey individuals who regularly use urinary catheters to understand health insurance coverage and out-of-pocket costs they experience to advocate for health-policy change.
Methods
Survey content was generated by non-profit organizations and programmed into Qualtrics. It was distributed in Spanish and English via email and social media accounts. The survey was open from 1/19/21–2/15/21 and only included individuals who either used catheters themselves or were the care partner of an individual who used catheters. For non-normally distributed data, log-transformed confidence intervals were used to achieve approximately normal distributions; data was then transformed to be analyzed using an approximate 95% confidence interval (CI), and a Mann-Whitney U test was completed to test the equality of medians between groups. Associations between catheter types and out-of-pocket costs were performed using the Kruskal-Wallace non-parametric test.
Results
One thousand two hundred and forty seven individuals responded. An equal percentage (43%) of catheter users were covered by public/government or private insurance plans only; 14% had both. Among those with public/government insurance, 8% reported their insurance did not cover any catheter costs versus 17% of those with private insurance. The median yearly out-of-pocket costs for privately insured respondents who paid anything was $1200 compared to $540 for those with public/government insurance.
Conclusion
Out-of-pocket expenses for catheters vary. Those with public/government insurance pay less out-of-pocket.
Introduction
Urinary catheters are used by more than 60% of individuals with a spinal cord injury (SCI), 1 and more than 75% of individuals with spina bifida (SB). 2 It is estimated that over 160,000 individuals with SB and about 299,000 individuals with SCI live in the United States (US).3,4 Catheters are used by individuals with neurologic or bladder conditions that result in urinary dysfunction and retention, such as multiple sclerosis. Beyond serving as a way to empty the bladder, clean intermittent catheterization (CIC) and indwelling catheters can prevent upper urinary tract changes that can lead to renal failure while also playing a role in reducing urinary tract infections and improving urinary continence.5,6
Recent studies have shown that most children with SB are born with normal upper urinary tracts, which may deteriorate over time.7–10 It is thought this deterioration can be reduced by early CIC initiation. 11 Many individuals with SCI are initially cared for with indwelling bladder catheterization, then transitioning to CIC after rehabilitation or condom catheters for continence.
Despite the clear rationale for catheter use and the prescriptive authority of clinicians to order urinary catheters and supplies, they are not universally covered by health insurance companies and plans in the US. Individuals and their care partners (parents, caregivers, partners) commonly reach out to non-profit patient advocacy organizations and clinicians for guidance regarding catheter supply costs. In response to this community outcry, a collaboration between the non-profit organizations of the Christopher & Dana Reeve Foundation (CDRF), Paralyzed Veterans of America (PVA), Spina Bifida Association (SBA), and United Spinal Association (United Spinal) was formed to advocate on behalf of the individuals they represent (herein referred to as the Collaborators). Together these Collaborators aimed to better understand catheter use, insurance coverage for supplies, out-of-pocket costs, and gaps in insurance coverage in the US. This was done with the goal of advocating for healthcare policy change to reduce the burden to catheter users of costs associated with their healthcare needs. The results of a survey of catheter users in the US are presented, revealing the extent catheters are covered by health insurers and health plans, ascertaining users’ out-of-pocket costs for catheters and catheter supplies, and the use and results of insurance appeals for coverage.
Methods
Survey development
Members of the SBA, CDRF, PVA, United Spinal, and the SB clinic at Duke University generated the survey content. Members from these organizations provided content validity for the final survey and pretested the survey for logic and flow.
The survey was programmed into Qualtrics and had a maximum of 29 questions depending on branching logic from an individual's responses. It was estimated to take 10 min and was available in English and Spanish. The survey and study were approved by Duke University's IRB (Pro00106717).
Survey distribution
The survey was sent via email to addresses registered with the participating Collaborators using their listservs. It was also advertised on social media platforms by the Collaborators and was open from 01/19/21–02/15/21.
Inclusion criteria
Survey respondents self-verified that they were older than 18 years of age. Participants could be the catheter user themselves or a care partner answering on behalf of someone of any age who used catheters regularly. The catheter user had to have insurance coverage and reside in the US or territory to be eligible to complete the survey.
Variables
Insurance plans were divided into public/government, private, or both categories. Public/government plans included Medicaid, Medicare, military, and veteran plans. Individuals with only an employer-provided commercial plan were classified as having private insurance. Those who had government and private coverage were classified as having both.
Statistical analysis
For inference purposes, the naïve method of natural log-transformed 95% approximate CIs was performed to assess the mean out-of-pocket costs associated with insurance type/plan and insurance provider. Non-normal distributions of yearly out-of-pocket costs were observed across individual groups being assessed, motivating the use of this naïve method. 12 Verification that the intervals contained the mean was conducted to ensure an unbiased estimator. The Mann-Whitney U test was performed to assess the equality of medians across two groups using untransformed data. For yearly out-of-pocket expenses, those who paid zero dollars were excluded from the analysis and were reported separately. Associations between seven catheter types and out-of-pocket costs were performed using the Kruskal-Wallace non-parametric test. Descriptive statistics were used to examine the reuse of catheters and the results of insurance appeals.
Results
Respondents
A total of 1236 respondents completed the survey in English and 11 responded in Spanish. Most respondents were, or represented, adults who used catheters regularly (89%); the remainder were care partners of children who used catheters. The average age of the individual using catheters was 45.5 years and 54% of catheter users were male. Respondents reflected all 50 states (Table 1).
Catheter user demographics by type of insurance coverage.
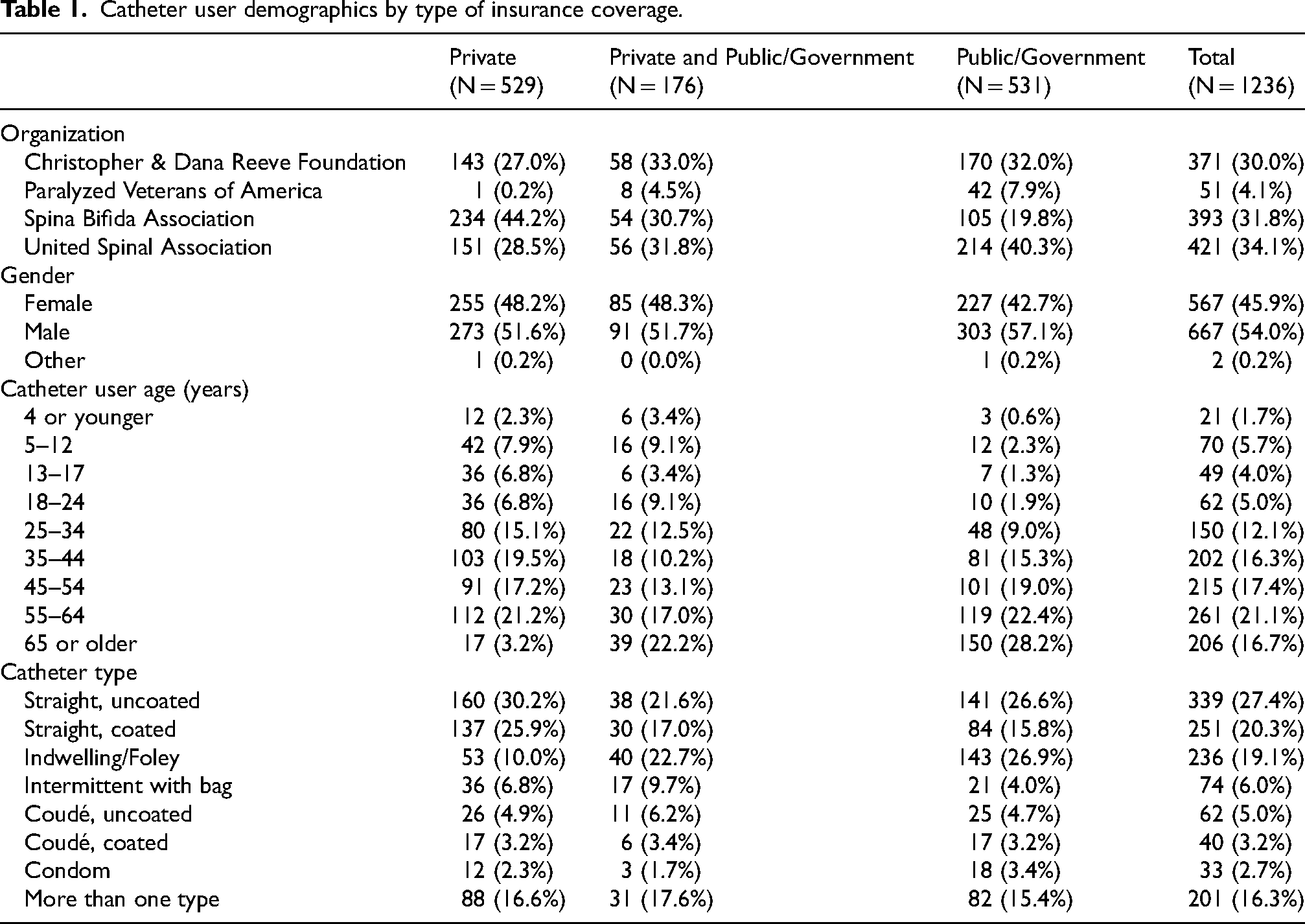
An equal percentage (43%) of catheter users were covered by public/government or private insurance plans only and 14% had both (Table 1). Of those with private insurance plans, 48% reported having a BlueCross BlueShield plan. The next most common types of insurance plans that users reported having were United Healthcare (13%), Aetna (12%), Cigna (8%), and Kaiser (3%). Of those with public/government insurance, most had Medicare only.
The most common type of catheter used amongst all users was reported to be uncoated straight catheters (27%), followed by coated straight catheters (20%). Individuals who used indwelling/Foley catheters were more likely to be covered by public/government insurance plans (Table 1).
The mean number of catheters used per month was 120 for all intermittent catheter types, 42 for condom catheters, and four for indwelling/Foley catheters.
Out-of-pocket costs
Among those with public/government insurance, 8% reported that their plan did not cover any of the costs of their catheters versus 17% of those with private insurance coverage. When the four most reported health insurance plans (Aetna, BlueCross BlueShield, Cigna, and United Healthcare) were considered individually, the percentage of users reporting that their insurance did not cover any of the costs related to their catheters was 11%, 15%, 15%, and 42%, respectively. Conversely, some users reported that their health plans covered all the costs of their catheters and supplies. Those with public/government insurance were more likely to report zero out-of-pocket costs for their catheters compared to those with private insurance (47% vs. 21%).
The median yearly out-of-pocket costs for privately insured respondents who paid anything was significantly more at $1200 (mean $1075; approximate 95% CI $973, $1188), compared to $540 for those with government insurance (mean $531; approximate 95% CI $473, $578; p < 0.001). Those with public/government plans paid the least out-of-pocket (Table 2). Of all respondents, 13% reported paying more than $250 per month out-of-pocket (8% of those with public/government insurance; 19% with private insurance). Most respondents reported paying between $50–149 per month out-of-pocket. The median out-of-pocket costs for individuals with private insurance varied by insurance plan but were not statistically significant between the most commonly reported plans (Table 3).
Yearly out-of-pocket costs by health plan type and private insurance provider.
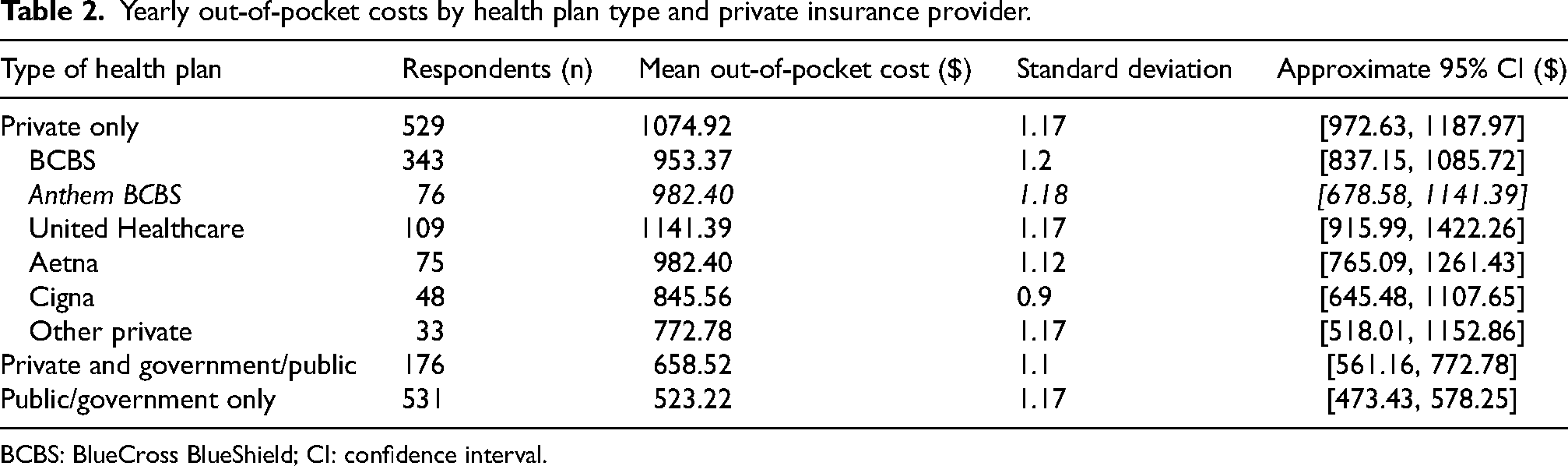
BCBS: BlueCross BlueShield; CI: confidence interval.
Yearly out-of-pocket costs by catheter type used.
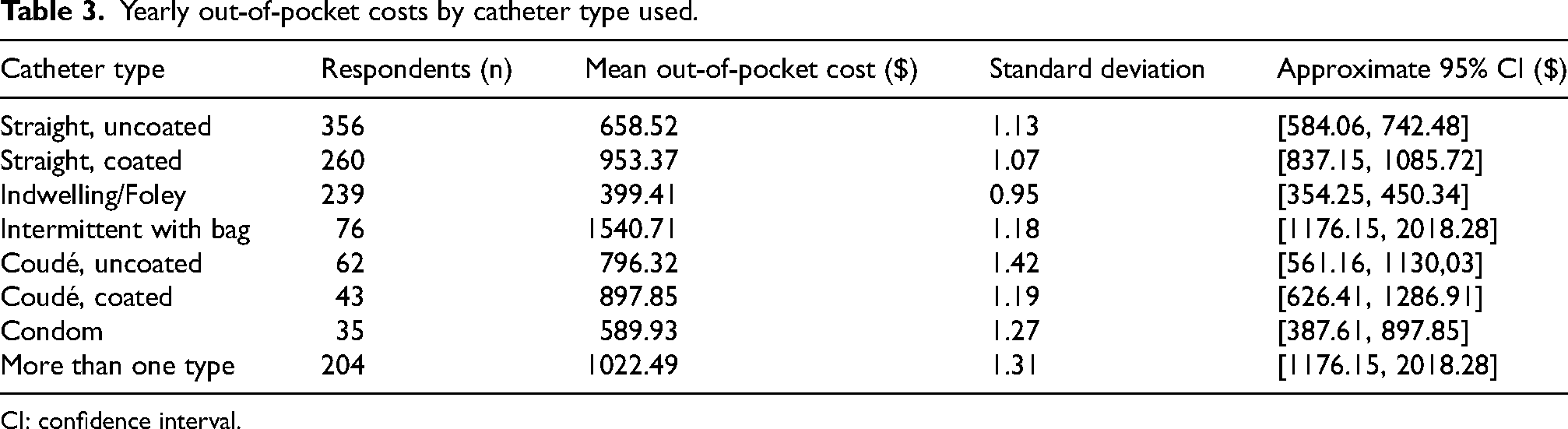
CI: confidence interval.
The Kruskal-Wallace rank sum test was used to compare the median out-of-pocket expense among various catheter types. There was a significant difference in the median out-of-pocket cost for individuals between the various types of catheters reportedly used (p < 0.0001; data not shown). Those using intermittent catheters with bags paid the highest amount out-of-pocket with a median of $1540.71 per year.
Coverage by recommended catheter type
Most (89%) catheter users reported that their health plan covered all or some of the costs of a specific type of catheter recommended for them by their clinician (e.g., straight, coudé, Foley; not a particular brand). Of those with public/government insurance, 61% were able to get full insurance coverage for the recommended catheter, versus 32% of those with private insurance. Of those with public/government insurance, 8% reported they did not have any coverage for the recommended catheter, versus 16% of those with private insurance.
Reusing catheters
Of all catheter users, 12% reported that they regularly reused catheters. The most commonly reported reason to reuse catheters was due to high out-of-pocket costs (58% of respondents). Twenty-seven percent of those who reused them did so secondarily to a recommendation from their clinician. The remainder cited other reasons, such as to reduce environmental waste, convenience, or personal choice. Reuse rates were similar in both those with private and public/government insurance.
Insurance appeal (Figure 1)
About half of the respondents were aware of their ability to appeal for increased coverage of their catheters and supplies (41%). Of these individuals, 149 (29%) had appealed to their insurance plans. Partial or complete approvals were granted in 56% of cases.
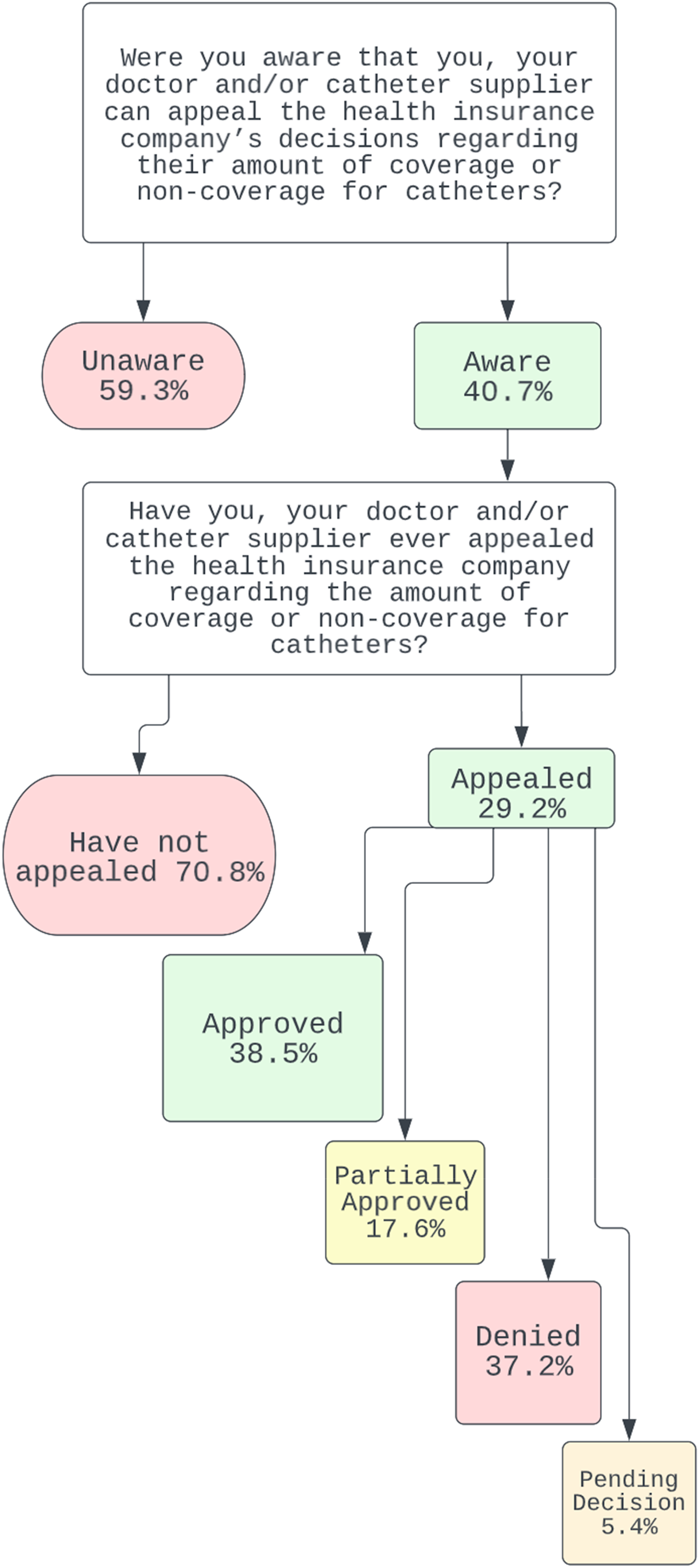
Reported awareness, use and outcomes of insurance appeals.
Discussion
The costs of healthcare to an individual vary significantly in the US due to the myriad health insurance companies, plans, and terms. 13 Different private health insurance plans also have their own requirements for coverage which is dependent on factors such as whether the plan is self-insured or fully insured and whether it is governed by the Essential Health Benefits standard. Bladder catheterization for individuals with bladder dysfunction is recommended by clinicians as the way to empty the bladder of urine and to reduce urinary tract infections, alleviate high urinary storage pressure, improve urinary continence, and relieve urinary retention. Catheters are covered under Medicare's Durable Medical Equipment, Prosthetics, Orthotics and Supplies fee schedule, which regulates some of the coverage for some individuals, especially those with public/government insurance. This survey of urinary catheter users identified significant variations in insurance coverage of urinary catheters and supplies among the most used health insurance types and plans. This survey also reported the results of insurance appeals to improve catheter coverage.
The average intermittent catheter user in this survey reported using 120 catheters a month, about four catheters a day. Intermittent catheters were also the most commonly used catheter type reported. Most respondents did not reuse catheters, so it can be assumed that each catheter was used for one micturition. For those with private insurance, the median out-of-pocket cost was $1200/year, or about $100/month. Those with public/government insurance paid a median of $540/year or about $45/month. Per catheterization amount, it cost an individual with private insurance about $0.83 per void and an individual with public/government insurance $0.38 per void. The out-of-pocket cost per catheter for all individuals, especially those with private insurance, is alarming, considering that uncoated straight catheters, the most commonly used in this survey, can be purchased online for approximately the same cost without insurance.
In this survey, catheter users with public/government insurance plans had lower out-of-pocket costs. They were more likely to be able to obtain the specific catheter recommended by their clinician.
Slightly more individuals who completed the survey were unaware than were aware that they could appeal to an insurance company regarding the coverage of their catheters. Of those aware of the opportunity to appeal, less than a third had submitted an appeal, and just over half of these were successful to some degree. The use of appeals for Medicare and Medicaid has been backlogged for years, and there is concern that this may worsen. 14 The Patient Protection and Affordable Care Act combined with the Healthcare and Education Reconciliation Act of 2010 requires that individuals have the right to an easy-to-understand summary of a health plan's benefits and coverage and have the right to appeal insurance claim denials and have them reviewed by a third party. 15 In 2020, 18% of in-network claims were denied, but these denial rates ranged drastically from 1% to over 80%, depending on the insurer. 16 Appeal rates for private insurance companies are harder to find and are not required to be published. Filing an appeal to insurance companies places a burden on the individual insured and/or their clinician. There is often confusion regarding who should be completing an appeal and what should be included. It takes time on behalf of the individual and the clinician or proxy to find, complete, and follow up on appeals which may be why so many do not file an appeal despite success rates being relatively high. In this survey, over 70% of those who were aware they could appeal opted not to pursue this process. Improvements aimed to increase awareness of the ability to appeal and how to do so are an avenue of advocacy and health policy that could be improved.
The number of individuals reporting private versus public/government insurance in this survey is similar to the reported breakdown of the country as a whole. 13 It is estimated that 10% of Americans do not have health insurance, and the number of catheter users without health insurance was not captured in this survey. The results of this survey must be interpreted in consideration of its limitations. State-level differences exist between public/government health insurance plans, just as private insurance plans vary based on different group plans. Granular data of these nuanced differences in health plans was not captured and, therefore, not reported in this survey. The results provided were generated from a convenience sampling of catheter users, and therefore, responses may not be fully representative of the broader population.
This is the first survey of catheter users on a national scale that examined reported costs to individuals for their urinary catheters and related supplies. Unfortunately, significant discrepancies exist in the costs individuals must pay for these supplies. The results from this survey should be used to advocate for those who require catheterization and to push for health policy changes to reduce the healthcare cost burden on them. Advocacy could focus on asking private insurance companies to utilize the uniform policies from Medicare's Durable Medical Equipment, Prosthetics, Orthotics and Supplies for urinary catheters. Advocacy with Congress to expand urinary catheter coverage within Medicare and Medicaid could also benefit individuals. Clinicians and researchers can start these efforts by contacting their state Medicaid offices, Congress members, and members of the Spina Bifida Caucus. There are also ongoing advocacy efforts from the SBA that individuals can contribute to; they keep an ongoing list of advocacy events on their website. Hosting information sessions on how to submit an appeal would also be helpful to users; the SBA plans to post instructions and host a webinar for individuals, which could then be shared more widely by individuals, clinics, and providers.
Conclusion
Out-of-pocket expenses for urinary catheters and supplies vary based on whether an individual has public/government or private insurance. Those with public/government insurance tended to pay less for their catheters and supplies.
Footnotes
Acknowledgments
Authors and members of the Collaboration reached out to provide the results of this survey before the release to the public to representatives of Aetna, BlueCross BlueShield, Anthem, Cigna, and United Healthcare. Meetings were held with all except Cigna, who failed to respond to meeting requests.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.