
Abstract
Purpose
This study aimed to examine parents' perceptions and experiences navigating their child's chronic health condition diagnosis.
Methods
Researchers used a qualitative research design, applying a phenomenological approach to interview 15 parents of children with a chronic health condition. Researchers analyzed verbatim transcripts to develop themes and report strategies that might inform care of the child and parents.
Results
Parents described a fluid experience navigating their child's diagnosis that involved five interwoven elements: grief, anxiety, unknowing, responsibility, and positivity. Mediating processes of time and experience supported adaptation toward positivity. Experiences appeared to transcend child-specific diagnoses suggesting a common process of parent adaptation to a child's diagnosis.
Conclusion
Findings elucidate parents’ lived experiences surrounding their child's diagnosis of a chronic health condition. Parents are inextricable from their child's care; thus, findings may garner knowledge supporting providers to employ strategies that support favorable outcomes for both children and parents.
Introduction
Chronic health conditions affect 10–30% of children in the United States and likely one in four school children. 1 A chronic health condition exists for longer than one year and is significant enough to limit regular life activities. 2 Pediatric chronic health conditions include, but are not limited to, asthma, autism, cerebral palsy, cystic fibrosis, epilepsy, type 1 diabetes, and severe food allergies. 1
Parents are inextricably linked with their child's care system, and the on-going nature of care navigation can contribute to parental anxiety. 3 Parents of children with chronic health conditions experience elevated levels of anxiety and depression,3,4 stress, and poor physical health. 5 These indicators are particularly elevated for mothers versus fathers, and for parents of children with cancer, HIV-AIDS, neurodegenerative disease, and cerebral palsy.3,4
When a child is diagnosed with a chronic health condition, parents face immediate and unforeseen challenges. Parents may struggle to gain sound footing as they learn to negotiate ordinary routines such as health management, sleep, education, work, and leisure. 6 Parental roles can shift from self or whole family caregiving to supportive and necessary health management routines for their child. 7
While medical approaches are imbued with necessary problem-focused, impairment-fixing approaches toward the child's health and wellbeing, the focus on the child's health condition may inadvertently pathologize the child, resulting in parental experiences of grief and guilt. 8 As parents begin to settle into a new normal, many learn to process emotions and consider their personal well-being while simultaneously supporting their child's needs. However, these ambiguities between parental self-care and care for the child are often interwoven with grief processes. 8
Lalvani and Polvere challenge the origin of grief and stress experiences of families of children with disabilities. 9 Traditional research situates parental grief and stress experiences as resulting from the child's condition or disability itself. The origin of parental grief and stress is considered to be the child's disability, rather than being also situated within the child and family's environmental, social, and cultural contexts. 9 Family relationships, educational systems, and the community may also contribute to parental stress experiences, through cultivating stigma surrounding the child's health condition, disability, and role expectations for the child and family. 9 For example, societal attitudes, values, beliefs, and responses regarding “different” and “other” may influence parents, contributing to grief narratives about what is supposed to be.
Understanding parents experience surrounding their child's diagnosis can inform healthcare, educational, and supportive service personnel in providing relevant services that not only manage the child's chronic health condition, but also provide essential parental support. Therefore, the purpose of this study was to examine parents' perceptions and experiences navigating their child's chronic health condition diagnosis.
Methods
Researchers used a qualitative research design applying a phenomenological approach. Phenomenology is a research approach that provides a methodology for understanding how one experiences and describes a phenomenon of interest, 10 in this case, parents’ experiences navigating their child's chronic health diagnosis. Participants provided written informed consent and received no compensation. The University of New Hampshire's Institutional Review Board reviewed and approved all study procedures.
Recruitment
Researchers recruited potential participants using convenience and snowball sampling via email, phone, or instant messaging to professional and personal contacts in the United States. Inclusion criteria were English-speaking parents who had at least one living child, aged 0-17 years, with a reported chronic health condition that limited or restricted at least one area of the child's life participation, such as school, sports, socialization with family and friends, or work. There were no specific exclusion criteria. This study intentionally included parents of children who were diagnosed both recently and in the past to be able to explore the experiences of parents at different time periods from diagnosis.
For the purposes of this study, Consolini's definition of a chronic health condition was applied: a condition that “lasted more than 12 months and was severe enough to create limitations in usual activity and/or required care or supportive services beyond those normally expected of a similar age child”.2 Parents were defined as those individuals who provided ongoing primary care and support for the child and had a shared history and projected future with the child.
Procedure
When participants contacted researchers, the first author communicated with participants to verify inclusion criteria and provide information regarding the study's purpose, inclusion criteria, and answer questions as needed. If individuals wanted to participate in the study and met inclusion criteria, researchers emailed consent forms and the interview questions. An interview was scheduled at a time of mutual convenience. Written consent was gathered prior to each interview. To protect participant anonymity, researchers assigned each participant an identifying number rather than using names.
Data collection
The first author conducted one 45–60 minute semi-structured in person or virtual interview with each participant parent. Participants also completed an online demographic survey regarding their ethnicity, race, education, income, and family structure. Interview questions fostered reflection about parents’ experiences surrounding their child's diagnosis with a health condition (see appendix). The authors collaboratively developed the interview questions based on the research purpose. The first author is a pediatric occupational therapist with 25 + years’ experience, including five years’ lived experience with a child with a chronic health condition. The second author is an occupational therapy faculty member with 25 + years’ experience, including 10 years’ family health research experience.
At the beginning of each interview, the first author discussed with participants the potential emotional risks inherent in talking about their child's diagnosis. The interviewer shared that participants could decline answering any questions they chose. Researchers intentionally sandwiched emotionally challenging interview questions between easier questions to support participants’ emotional safety. All interviews were audio recorded and transcribed verbatim for analysis. During interview transcription, identifying participant information was removed including names, locations, and situations.
Data analysis
The two authors analyzed demographic data using descriptive statistics to include frequencies and percentages. Interview data were analyzed using an inductive phenomenological approach using Braun's and Clarke's six thematic analysis phases 11 to understand participants’ perceptions and experiences navigating the diagnosis and process surrounding their child's chronic health condition. Researchers met eight times over a 12-month period, and organized data using Dedoose software. 12
In phase one, the two authors read all interview transcripts independently, highlighting words and phrases reflecting participants’ experiences surrounding their child's diagnosis and assigning a code to each piece of data. In phases two and three, the authors met to discuss and organize independent initial codes into 12 code sets, comprised of codes with similar descriptions and meanings. The authors then collapsed the code set to 10 categories through further rereading and chunking of patterned data. In phase four, the first author wrote definitions of each category, considering quotes attached to each data category as well as definitions of emotions within outside literature. 13 In phase five, the authors narrowed data categories into five emerging themes. This process involved rechecking of the emerging codes, categories, and themes with the original data to ensure accurate representation of participants’ intended meaning. Lastly, in phase six, the first author considered the collective meaning of the clustered quotes and defined the final themes titled “elements.” The researchers collaboratively wrote the sections describing the identified five elements.
Results
Participants
Fifteen parents from 15 families participated in the study including 14 parents identifying as mothers and one as a father. The average age of children with a chronic health condition was 10.3 years and they had a variety of conditions, including but not limited to autism spectrum disorder, cancer, cerebral palsy, Down syndrome, fetal alcohol spectrum disorder, seizure disorder, and type 1 diabetes. See Table 1 for participant characteristics.
Characteristics of Parents (n = 15).
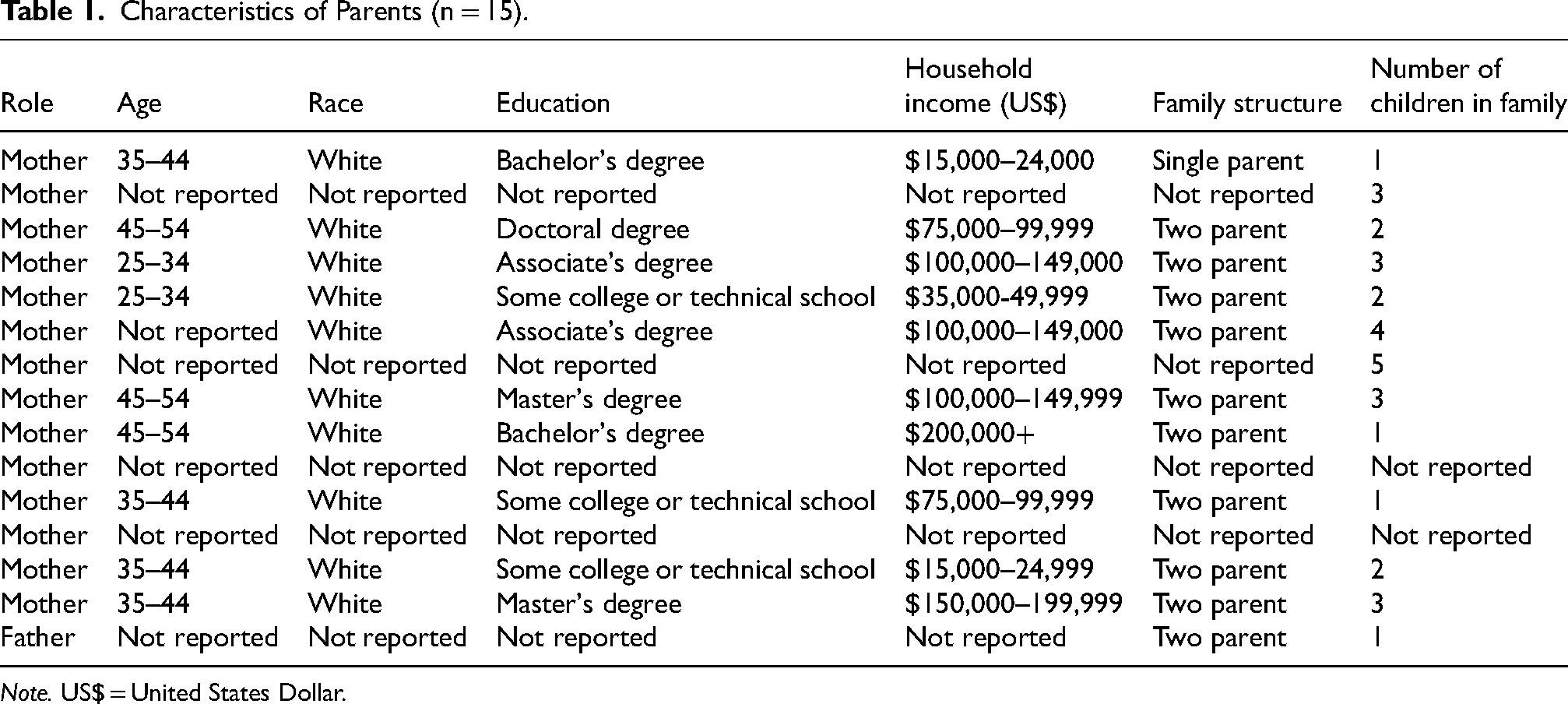
Note. US$ = United States Dollar.
Parent experience following their child's diagnosis
Parents described a fluid experience navigating the diagnosis and subsequent experience of caring for a child with a chronic health condition that involved five interwoven elements described collectively by all parents: 1) Grief, 2) Anxiety, 3) Unknowing, 4) Responsibility, and 5) Positivity. Parents experienced these elements as interwoven: they happened cyclically, with elements coming, going, and returning rather than occurring in linear stages. Mediating processes of time and experience supported adaptation to the first four elements and led to the fifth. Each element is described below, followed by parent excerpts.
Element 1: Grief
Parents overwhelmingly articulated grief along their parenting journey, especially during early experiences with their child's diagnosis. Parents who suspected their child was experiencing something atypical felt grief while searching and waiting for a diagnosis. These parents reported a sense of relief when their child was finally diagnosed. Parents whose children were diagnosed unexpectedly described omnipresent negative emotions that distorted the world around them, coloring everything in darkness and sadness. Parents reported a complex experience of grief because their loss was intangible. Their children continued to live; however, the vision they held for their family was reshaped, which created conflicting emotions and challenged parents to suppress pessimistic thoughts. As one parent described: It's hard to think that you can grieve something that's right in front of you, but it happens…you do, you grieve. You grieve the future, you grieve what could have been, you grieve for your other children because they're forced to grow up way faster than most kids. People kept talking about you need to allow yourself time to mourn what you thought you were going to have. And then what you didn't. You have to mourn that loss. I never really understood it, but eventually that came to me. It just took a long time.
Element 2: Anxiety
Every parent in this study conveyed anxiety in the form of uneasy feelings about an uncertain future. Some parents reported being terrified about their child's immediate health needs, especially in the face of surgeries, invasive treatments, and management of life sustaining medications. One parent described the anxiety element this way: Anxiety is my biggest one though. There will be nights where I will wake up at 1:00 o'clock in the morning and be afraid that he's going to lose his insurance. How am I going to pay for all this? How am I going to support him for the rest of his life? How am I going to make sure his needs are met?
Parents of children with diagnoses that affected behavior, especially aggressive tendencies, noted fear regarding safety for themselves, their other children, and their child with the condition. Some parents’ fear evolved into what some described as hypervigilance, wherein they experienced exaggerated responses to common health threats because their child's physical or emotional equilibrium was so fragile. One parent recalled: [My son] was in a mental health crisis once last summer. I grabbed all the knives out of the house, and I went to my car, and I locked myself in my car, and I cried for two hours. Then it got to a point where I couldn't do it anymore. I called 911 because I thought he was going to harm himself or harm me. I was broken at the time. I had nothing left in me.
Another parent shared: I'm so petrified of the high blood sugars. And then the first time we were at a restaurant, a week after he was diagnosed, we went away with my sister and we were at a restaurant and we had been monitoring his blood sugar like we should have, and then sitting in the restaurant and we took it, and it was 70 and it was so new I just started panicking. I couldn't think straight, my anxiety was off the chart. I didn't know what to do. There's definitely been a few moments and as I'm dealing with my own anxiety and then this person is beside me saying, he's not going to die… And I'm like, “Well it could happen if I don't do something right now.”
Although not every parent reported fear, each parent expressed some degree of worry about their child's future, which morphed with time but never went away. Worries shifted based on current health status, the child's age, and the family's immediate needs or priorities. As parents and their children felt more secure with their ability to meet their child's basic needs, they described turning their attention to less immediate needs, such as security and self-esteem.
Element 3: Unknowing
All parents interviewed reported distress about the unknowns surrounding their child's chronic health condition. Several reported suspecting something atypical about their child's health or development and described the need to independently seek out, and at times convince, healthcare providers that their concerns were warranted. They described how their intuition alerted them to their child's need, but that they did not have the knowledge or resources to attain a definitive answer. Some parents described that their child's diagnosis came as a relief, a first step in alleviating the unknowing. Other parents shared that they received their child's diagnosis without any knowledge base to make sense of the information providers gave. These parents reported lacking the knowledge necessary to make informed decisions regarding their child's care options.
Finally, despite receiving a specific diagnosis, all parents described recognizing the unique nature of their child's particular diagnosis. Even as they gained knowledge, parents shared how they faced the uncertainty of the degree to which their child would be impacted, and how the diagnosis would be manifested in their child's life. Although healthcare providers had knowledge of conditions and diagnoses, parents reported that providers were unable to give answers to many of the questions they had. One parent described this as: “I am still like why, why, why, and nobody knows. It's hard to be comfortable with that uncertainty.” Another parent stated: “We had to wait for the results. The doctor who was supposed to call us, didn't. And it was agonizing because we had to wait and wait and wait.” Another parent recounted their struggle with unknowing this way: The unknown, being told, “We don't know.” At the time, I should say I was very black and white. This is the problem; this is how we fix it. Okay, let's fix it. And to be told that, well, we don't know how, we don't know where it's going to go…I think that was probably living in gray.
In the face of so many unknowns regarding their children's futures, parents described responding by worrying, as noted previously, or by searching. Some parents shared that they searched for a diagnosis. Others gathered as much knowledge as possible so they could make informed care decisions. They sought guidance from healthcare providers, online groups centered around their child's condition, and connections within their personal and professional networks. Parents reported that the searching provided valuable information, and for some, this information alleviated their anxiety by channeling energy toward a productive end. One parent searched for “specialist after specialist in various cities and states.” Another described the process of searching as empowering: “I feel like I have more control if I know all of the information.” Another parent reported a need to search due to a lack of professional support: “The autism diagnosis came with an autism diagnosis. There was nothing after that. It wasn't, ‘Here's the resources you need. This is what you should do.' Which was hard.”
Element 4: Responsibility
Parents described that in addition to a typical sense of accountability for their children's successes and failures, they also took responsibility for managing their child's chronic condition itself. Parents described the weight of making important healthcare decisions that often carried short- and long-term consequences extending well beyond routine care. This pressure sometimes led to what parents described as a sense of being overwhelmed and/or culpable. One parent illustrated responsibility this way: I feel somewhat resentful. I've lately been thinking in my own head, this disease is a mother's disease…because we usually, the buck usually stops with us anyway, when it comes to pretty much everything. And this is just one extra thing on the pile, except this one extra thing on the pile is humongous.
When their child was diagnosed with a chronic condition, parents expressed the need to acknowledge the impact of their increased responsibilities. They developed awareness that their parental responsibilities to make decisions on their child's behalf would likely extend beyond the typical parameters for their child's peers and siblings. One parent described: I can't treat my kids the same. They're not the same. I have to treat [my child with a health condition] differently. If I don't treat her differently, then I'm not giving her what she needs. It was really hard to know that there were boundaries placed on her that weren't boundaries placed on even her younger sisters.
Finally, when parents were unable to identify a cause or a place to lay blame for their child's chronic condition, some parents shared that they assigned it to themselves. About half of parents stated they felt guilt regarding their child's health condition. They either believed they somehow caused the condition, or they were responsible for negative outcomes resulting from the decisions they made on their child's behalf. Others described the need to push back against others’ projection of guilt onto them as the cause of their child's behavior or health.
Many parents described worries about their child's future which were tied to feelings of caregiver responsibility. They expressed worry in the form of conjectures that if something went wrong or their child did not progress according to expectations it would be due to their lack of effort. Others expressed feelings of blame for their perceived failures in other relationships, especially with their other children, due to the need to pour energy into the care of their child with a chronic condition. As one parent shared: I then convinced myself that she [child with chronic condition] was going to die. I convinced myself that she was going to die, and that it was going to be because I wasn't doing enough. So, then you have the guilt and the wonder like was this my fault? Could I have done something different? Well, I was an X-ray tech at the time, maybe I got too much radiation… for me, well it has to be because of something… and so I thought, well, what did I…maybe I should have had my folic acid or something, or maybe I shouldn't have held that patient, or something like that. You just want to make sure that you're making the best choices and doing the best decisions and not letting certain balls drop that you're not really realizing. And it comes in waves, so eventually she'll be back in a phase where she's on the up and up, but when it's in those lulls where there's a bit of regression, it's hard not to like blame yourself as a parent. So as a parent, you look and you think what did I miss? It [cancer] didn't grow just like that. What did I miss? So then you start to, I started to immediately, what did I miss? What were the signs? What was I paying attention to? How did I not add one plus 182,000,000,006 times 16 to the square root of 42 and not come up with the answer?
Element 5: Positivity
As parents described their current perspectives about their child's diagnosis, they articulated a clear shift from persistently experiencing unpleasant emotions toward only intermittent negative feelings. When they began the journey with their child, parents described their child's chronic condition as the first thing they thought about upon waking, with pervasive thoughts continuing throughout their days and nights. Parents shared that eventually their child's condition became an integral thread in the tapestry of their lives. Over time and with both positive and negative experiences, parents shared that they were able to move forward, overcome hurdles, make complex decisions, and survive setbacks.
Parents overwhelmingly identified positive impacts of their experience surrounding their child's health diagnosis on themselves, their child with the condition, and their family. One parent depicted the positivity element this way: “I love all my children, but this love is just completely different. The excitement she got when she started walking was like your heart exploding a million times over.” Another parent portrayed a transition exemplifying movement and progress: “I woke up one day and realized the diagnosis wasn’t the first thing I thought of.” Another parent described the positivity shift this way: So, there's not just gratitude of [my son] being well, but there's gratitude of [my spouse] and I finding each other again, and our bond, and our forgiveness, and our growth. Just the gratitude of finding joy in things again because there was no joy, everything was colored. I remember thinking once we got home, and she was nursing, and we got into a little bit of a rhythm. My mom stayed with us for a couple weeks. I started to finally feel okay. I still had a lot of fear of the unknown, I still had all of that, but it wasn't like my overwhelming feeling anymore. Well, it's always…not always…it's still hard. It's really hard. But it's just become our normal. It's like more than our normal now. It's just our life. She'll always have this soft spot in her because of her extra chromosome. I definitely am so proud of her, but I also… Another emotion I have, I still have fear. I still have fear for her future. So, I think all along the way leading up to now, there's the denial, the acceptance and then you move on to your next step. And then you get to a point where you just throw your hands up and say this is what it is. So, at this point in life, life is good. I wouldn't change it for anything. I don't want to go back to the person I was when she was born, I am a totally different person because of her. I think the strength to accept that this is our life. And it's good; it's a good life.
Discussion
The purpose of this study was to describe parents’ perceptions and experiences navigating their child's diagnosis of a chronic health condition. Although the child becomes part of a complex care system for condition management, results of this study raise important provider considerations regarding parental care within these systems.
Grief, anxiety, and unknowing
Parents in the current study identified grief, anxiety, and unknowing elements as they adapted to their child's chronic health diagnosis. Grief was triggered by comparison to other children, watching their child not meet expected milestones, or healthcare crises. Data depicted that they also experienced fear and worry concerning their child with a chronic diagnosis, and possibly for their other family members and themselves. Parents' descriptions of fear surrounded their child's immediate health and well-being, as in the case of diabetes and cancer, or other anxiety about their child's future, including independent living, health insurance, and future complications from their health condition. These findings strongly align with existing literature, regardless of child health management variations.14–16
Coughlin and Sethares 17 outline specific, supportive, healthcare provider strategies for engaging with parents of children with chronic health conditions including 1) providing relevant information about the child's condition, available interventions, and accessible services; 2) providing empowering care that acknowledges and normalizes parental emotions; and 3) connecting parents to respite care and online support groups.
Parent-provider interactions
Regarding providing information, the quality of the parent-provider interaction is important. Although the child is the focus of healthcare interventions, parents in the current study described that they primarily managed the care. While maximizing the child's health is a priority, findings from this study suggest situational impacts on parents should also be addressed. Previous research examining parents of children with a variety of health conditions supports this, highlighting parents’ desire for providers to consider their emotional needs when providing care for their child.15,17,18 By opening a safe, supportive discussion about parental wellbeing, providers may facilitate parental movement toward positivity. 19
While health management of the child's condition necessitates medical interventions, language and word choice in provider-parent interactions is important to monitoring the discourse tone. How providers share knowledge, results, and resources is as important as what information is shared.17,20 The medicalization of childhood chronic conditions may inadvertently promote narratives of tragedy, burden, and stress. 9 Parent-provider discussions and information sharing that serve to demystify fears, affirm hardships, and decrease the unknowns could alleviate some parents’ anxiety regarding their child's immediate and future needs.17,19,21 Providers may create a trusting, non-judgmental environment that supports parental openness and vulnerability by specific interaction skills such as knowing the child's name and details of their history, sharing balanced information about challenges and positive hopeful outcomes, and recognizing parental strengths. 19
Findings from the current study related to parents' descriptions of angst related to unknowing suggest that when providers present difficult or unexpected news to parents, it may be helpful for providers to provide intentional and vetted resources and access to trusted networks. The current authors suggest that parents’ observations should be acknowledged and investigated, especially if the same or related concerns arise across visits. The authors recommend that providers reassure parents of the vast amount of information available while also encouraging them to focus on the most pertinent information for that moment. Providers can help parents recognize differences between imminent and future needs: distinguishing between near-term decisions that require immediate attention and those that can be set aside for the future. The current authors suggest providers suggest asking open ended questions such as “What is currently on your mind about your child's care?” or “What feels pressing for you right now?” may elucidate and guide parent-provider interactions.
Parent interventions
This study's findings align with previous research outlining the interventions that parents of children with chronic health conditions need to support their own stress reduction, coping, and care navigation.18,22 Parental stress management interventions for children with medical complexity include care coordination, respite care, telemedicine support, peer and emotional support, insurance navigation, and health support. 22 The parent and family wellness framework by King et al. 21 delineates three family-oriented services foci within pediatric rehabilitation: supporting parent-specific needs, helping parents to “co-provide therapy and manage care”, 21 p. 340, and providing intentional resources and education. Reflecting on the referral and support networks providers can share with parents is one step toward meeting this evidenced parental need.
Responsibility
Data in the current study suggest that parents felt overwhelming responsibility for their child, including at times feeling responsible for causing their child's health condition. Previous research highlights that healthcare providers can affirm to parents, when appropriate, the normalization of grief when a child is diagnosed with a chronic health condition.14–16 Additionally, previous evidence suggests that providers may further articulate that grief relates to a loss which may or may not be tangible, such as the loss of their anticipated future. 17 Current strengths-based perspectives of parenting children with health conditions encourage important reframing from historical narratives of tragedy, grief, and guilt toward those of hope, resilience, and adaptation.17,22 Parents experience this adaptiveness toward hope and positivity as a journey or cyclical process evolving over time and involving a wide range of processes within this transformation. 23
The current study suggests that providers have a unique role in facilitating parents’ adaptation process related to the responsibility element identified in this study. Providers can articulate from the medical perspective that parents are not culpable for their child's diagnosis, when appropriate or possible. While negative outcomes of medical decisions do occasionally occur, providers are encouraged to remind parents that they are working together, in good faith with providers, to make sound decisions on their child's behalf, acting on the best information they have at the time. These suggestions align with published evidence that highlight that providing clear information about the child's intervention options decreases decisional conflict 24 and may support shared parental engagement in decision making 25 thus empowering parents’ ability to care for and make decisions on behalf of their child.
Positivity
In the current study, time and experience appeared to afford the parent, child, and their family increasing levels of strength and flexibility. Data from parents’ narratives in the current study suggest that time and experience may be necessary for parents to feel positivity more frequently and develop resiliency. In alignment with these data, DeGrace et al. 7 found that for parents of children with autism, knowledge and experience mediated the shift from the unknown and moments of paralysis toward reengagement in daily family activities and routines. Similarly, Broski and Dunn's Strengths-Based Theory of Parental Transformation 26 outlined three stages parents of children with developmental conditions experience as they make sense of their child's diagnosis: awareness, liminality, and transformation. Liminality, the second stage, reflects parental experiences of being between awareness of their child's condition and recognition of opportunities for the future. This liminal stage aligns with the “shifting” that parents in the current study described. Providers likely have a critical role in this liminal stage in supporting a shift toward the positivity element as extended toward resilience building. Resilience, as described in current literature is no longer considered an innate or achievable trait, but rather one's response to stressors in relation to available resources within the environment. 27 Providers are often the resource givers and thus can have an impactful role in building parental resilience.
Limitations and future directions
This study included a small sample of primarily White parents identifying as mothers of children with chronic health conditions and thus findings may be unique to this parental set. Although broad generalizability is not the intent of qualitative research, among this participant group the elements within adaptation processes were universal. Further study to determine the extent to which these elements apply to a broader group of parents might allow parents to seek support from more universal resources and networks. Future research should include parents with varied ethnicity, parental roles, and economic backgrounds.
Conclusion
When a child is diagnosed with a chronic health condition, many parents initially experience a surge of emotions and information. Although the specifics of their child's care may differ significantly across diagnoses, parents in this study described five common elements in their process of adaptation to living with their child's chronic condition including experiences of grief, anxiety, unknowing, responsibility, and positivity. By recognizing and understanding these commonalities, providers from a variety of specialties may practice ubiquitous strategies to offer holistic care within the parental-child dynamic. Simultaneously, parents may seek and find support from a broad network of people and resources, supporting adaptation processes through extending beyond the boundaries of their child's diagnosis.
Footnotes
Acknowledgements
We thank the participant parents for sharing your time and experiences with us.
Research ethics & patient consent
This study was approved by the University of New Hampshire's Institutional Review Board for the Protection of Human Subjects in Research, IRB #8365 in accordance with the standards outlined in the 2000 Helsinki Declaration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.