
Abstract
Purpose
This study aimed to compare tumour microbiota characteristics as potential recurrence predictors in estrogen receptor-positive (ER+) and progesterone receptor-positive (PR+) breast cancer.
Methods
Formalin-fixed paraffin-embedded (FFPE) tumour tissues were obtained from 52 patients with ER + PR + breast cancer, and patients were retrospectively followed up for over 7 years. Patients were categorized into three groups: local recurrence (n = 13), distant metastasis (n = 17), and no recurrence (n = 22). Gene expression profiles and microbial activity in tumour tissues were analyzed by microarray and 16S rRNA sequencing, respectively, from the same total RNA extracted from FFPE samples.
Results
Compared to nonrecurrent tumours, the ratio of strict anaerobic bacteria Muribaculaceae to aerobic bacteria Pseudomonas activity was significantly upregulated in tumours with local recurrence, while no significant difference was observed in the distant metastasis group. Furthermore, the Muribaculaceae/Pseudomonas activity ratio showed a significant correlation with the cancer relating genes expression of PLA2G5, MSMO1, and three small nuclear RNAs across all 52 tumours.
Conclusion
This study provided the first evidence of distinctive features of tumor-associated microbiota in ER+/PR + breast cancer patients with local recurrence, suggesting their potential as predictive biomarker for local recurrence. However, these findings require further validation in larger cohorts due to the limited sample size.
Introduction
Advances in the treatment of breast cancer have decreased the rate of isolated locoregional recurrence. 1 Lumpectomy followed by radiotherapy reduces the recurrence of ipsilateral breast tumours by 52% compared with lumpectomy alone, and lumpectomy followed by radiotherapy and tamoxifen treatment reduces the incidence of recurrence by 32% compared with lumpectomy followed by radiotherapy. 2 Moreover, young age, node positivity, larger tumour size, and hormone receptor-negative tumours status are associated with a higher risk of recurrence. 3 The median times to locoregional recurrences of breast cancer, measured over 20 years, 4 are as follows: estrogen receptor-positive (ER+), 6.8 years; estrogen receptor-negative (ER-), 3.6 years. 5
The relationship between tumour gene expression and recurrence in breast cancer is well studied, and the findings may contribute to identigying targets for therapy designed to prevent cancer relapse. The 21-gene recurrence score (RS) provides a probability of distant recurrence for patients with ER+, human epidermal growth factor receptor 2 (HER2) negative (-) breast cancers, 6 as well as for women <40 years of age with node-negative and limited node-positive breast cancer. 7 Recent studies indicate the higher expression of fructosamine-3-kinase, nuclear factor erythroid 2-related factor 2, and NAD(P)H Quinone oxidoreductase in luminal A, luminal B when compared to HER 2+, triple negative and adjacent normal breast tissue. 8 Other studies indicate the mutations in the PI3K/AKT/mTOR pathway for metastatic triple-negative and ER + HER2- metastatic breast cancer patients, 9 and the lower systemic immune-inflammation index is associated with better survival outcomes among HER2-positive metastatic breast cancer patients. 10 Otherwise, these studies analyzed populations in Europe or the United States. In contrast, limited data are available for populations in Asia, excluding a study conducted in China that showed that Ki-67 expression level is significantly associated with early relapse of breast cancer. 11
Furthermore, tissue microbiota has been considered as an important part for breast cancer microenvironment. The most abundant phyla in both healthy breast tissue and breast tumours are Proteobacteria (more than 50%), followed by Firmicutes, Actinobacteria and Bacteroidetes, as revealed by Canadian, Irish studies, non-Hispanic White women and non-Hispanic Black women.12,13 The bacterial genera abundance varied significantly between Black and White women, but no significant difference between Asian and white groups. 14 In animal experiments using a murine spontaneous breast-tumour model, bacteria carried by circulating tumour cells promoted host-cell survival by enhancing resistance to fluid shear stress during metastatic colonization. 15 Other evidences suggest that, tumour tissue microbes may influence breast cancer progression through immune modulation, direct carcinogenic activity by bacterial toxin, and effects on cellular pathways involved in cell proliferation or apoptosis. 16
Here we analyzed the tumour microbial activity associated with recurrence status within 7 years after surgery from patients with ER + and progesterone receptor positive (PR+) ductal breast cancer. This will contribute to improving therapy designed to prevent the recurrence of ER+/PR + breast cancer in patients.
Methods
Study design and subjects
The present retrospective study included 52 ER+/PR + patients who underwent breast cancer surgery at Huangpu District Central Hospital of Shanghai, China. Inclusion criteria: Patients were initially screened based on hospital pathology records according to the following criteria. 1, Who underwent surgery between 2005–2008 and followed-up data for occurrence of local recurrence or distant metastasis within 7 years post-surgery; 2, Who underwent surgery in the last two months in 2008 and followed-up data for no recurrence within 7 years post-surgery; 3, ER+/PR + status confirmed by immunohistochemistry; 4, Age at surgery >40 years; 5, Confirmed histologically ductal breast cancer. Patients were then divided into three groups, local recurrence group, distant matastasis group and no recurrence group. Archived FFPE pathological sections from enrolled patients were utilized for this study. The tumour tissues have been collected in operation room and preserved in formalin and transferred to the laboratory immediately after surgery. FFPE processing was performed in the sterile clean room using sterilized materials and new open reagents. The histologic grade was assessed according to the World Health Organization criteria. Lymph nodes were confirmed during surgery. These patients were administered tamoxifen starting immediately after surgery and continuing for more than 7 years or until cancer recurrence or metastasis. Exclusion criteria included loss to follow-up, or lack of informed consent.
RNA extraction, microarray hybridization and data analysis
The method of RNA extraction from FFPE samples are described by previous study, 17 together with the methods of microarray hybridization and data analysis. RNA samples with an A260/A280 ratio between 1.9 and 2.1 and an A260/A230 ratio greater than 1.8 were considered to be of sufficient quality, and were used for double-stranded cDNA synthesis and microarray hybridization. The microarray data were deposited in the Gene Expression Omnibus (GEO) database under accession codes GSE183231 and GSE185439, which were obtained from the same cohort experiment. Differentially expressed genes (DEGs) were identified using a paired t-test with a false-discovery rate (FDR) adjustment. A gene was considered significantly differentially expressed if it exhibited a > 1.5-fold change in expression compared to the reference group (FDR p < 0.05).
16S rRNA sequencing, bacterial diversity, and taxonomic analysis
The same RNA extracted to perform microarray hybridizations was also used for 16 s rRNA sequencing, followed the method reported previously. 17 Sequencing was performed on the Illumina Hiseq 2500 platform using paired-end 250 bp reads, generating 2 × 250 bp reads per fragment. The 16S rRNA sequencing data have been uploaded to GenBank Sequence Read Archive under accession number PRJNA769523. To eliminate RNA sequences originating from environmental contaminants (laboratory reagents); the R package Decontam (https://github.com/benjjneb/decontam) was employed in the microbiota activities analysis. 18
Statistical analyses
The correlation between gene expressions and the relative activity of bacteria was calculated by Pearson's correlation coefficient using SPSS 27.0. The threshold set for a significant correlation was p < 0.05.
Results
Clinical and pathological features of breast cancer patients
The included 52 FFPE samples were prepared from breast cancer patients who underwent breast cancer surgery between 2005 and 2008. Among the patients, 17 showed evidence of distant metastasis, 13 showed local recurrence and 22 showed no evidence of recurrence within 7 years. The clinical and pathological features of the patients are summarized in Table 1.
Clinical and pathological features of patients with ER+/PR + breast cancer treated with surgery and postsurgical chemotherapy.
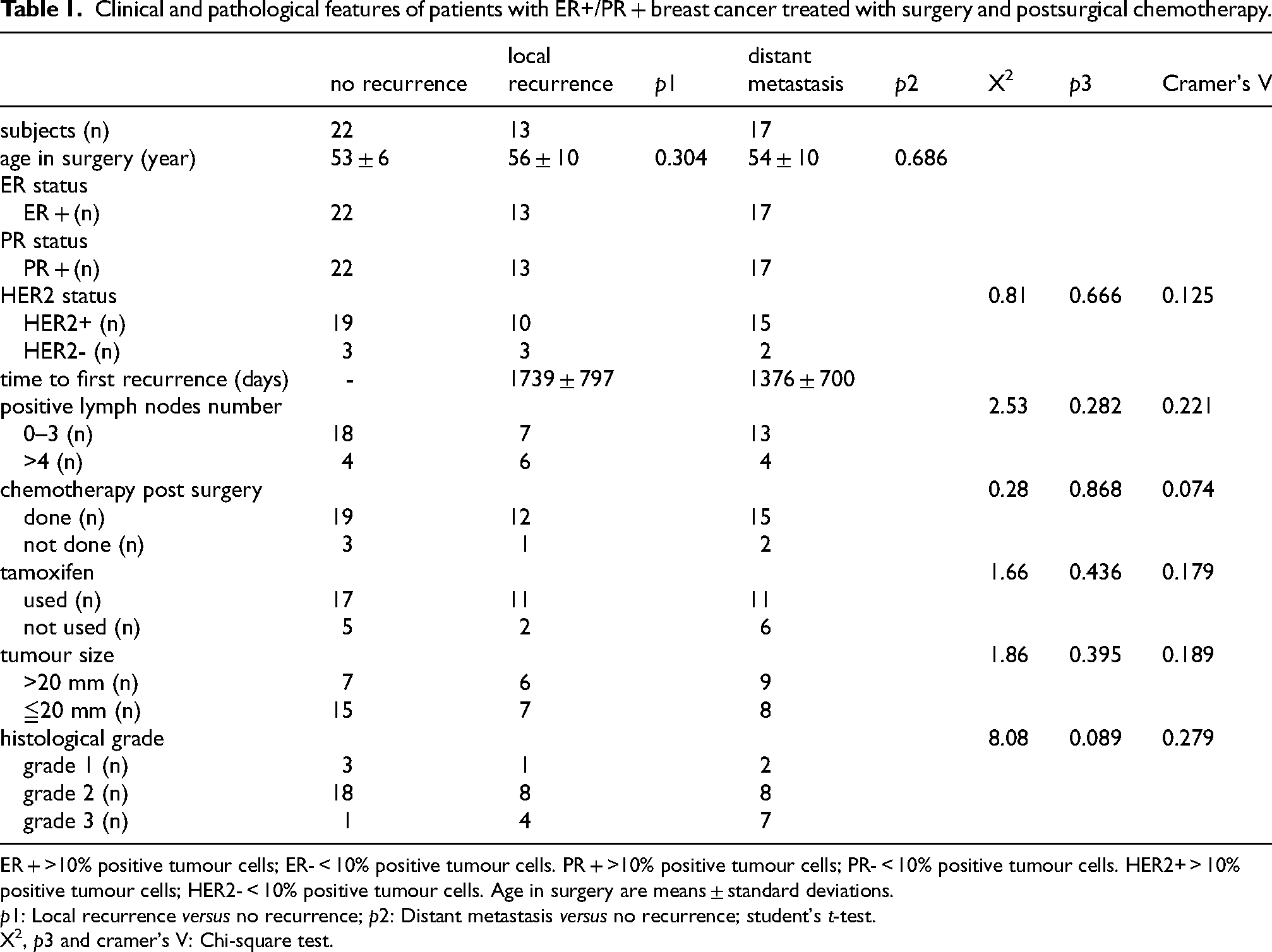
ER + >10% positive tumour cells; ER- < 10% positive tumour cells. PR + >10% positive tumour cells; PR- < 10% positive tumour cells. HER2+ > 10% positive tumour cells; HER2- < 10% positive tumour cells. Age in surgery are means ± standard deviations.
p1: Local recurrence versus no recurrence; p2: Distant metastasis versus no recurrence; student's t-test.
X2, p3 and cramer's V: Chi-square test.
Bacterial 16S rRNA sequencing in er+/pr + breast tumours with local recurrence, with distant metastasis, and without recurrence
16S rRNA amplicon sequencing of the V3-V4 hypervariable regions was performed using cDNA samples from 55 tumour tissues. In total, 3,114,797 (42,254∼66,072) high-quality sequences of the 16S rRNA from 55 samples were obtained by high-throughput DNA sequencing. After the 55 ER+/PR + breast tumour samples were classified into three groups (local recurrence, distant metastasis and no recurrence), 16,785 OTUs were obtained, of which 54.9% of OTUs were shared by all three groups (Figure 1). The Good's coverage index exceeded 96.0% for the three groups (Figure 2A), indicating that the sequencing depth was sufficient for investigation of the tumour tissue microbiota. Analysis of the alpha diversity showed that there was no significant difference in the richness indicated by the Chao index (Figure 2B) and observed species (Figure 2C), and no significant difference in the diversity indicated by the Shannon values among the three groups (Figure 2D). More than 99.7% of the microbiota could be aligned to 8 phyla, more than 98.8% to 23 orders, more than 98.4% to 36 families and more than 96.7% to 52 genera. There was no significant difference among these three groups of tumours (Figure 3).
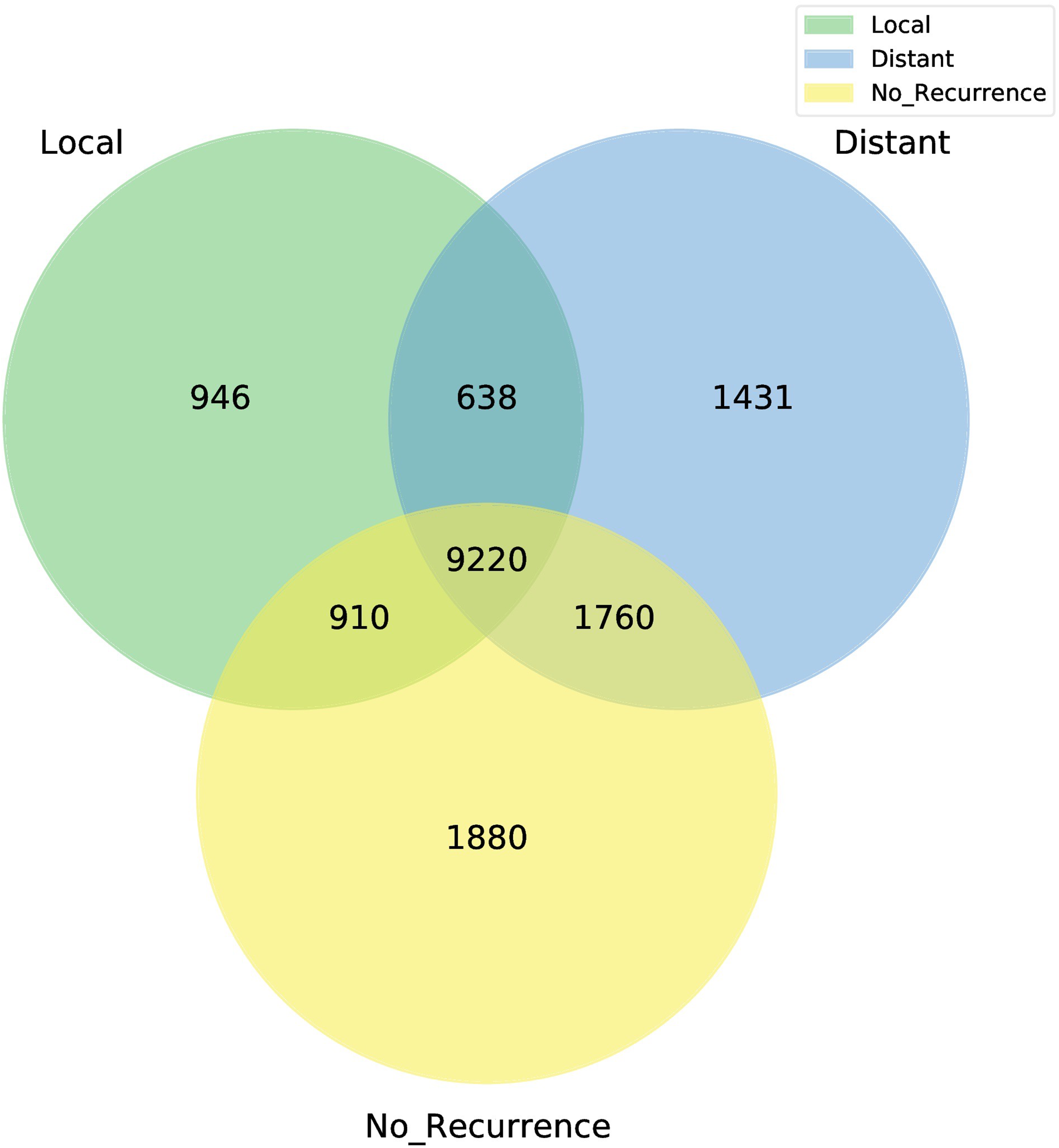
Venn diagram showing the common and unique OTUs among the local recurrence, distant metastasis and no recurrence groups.
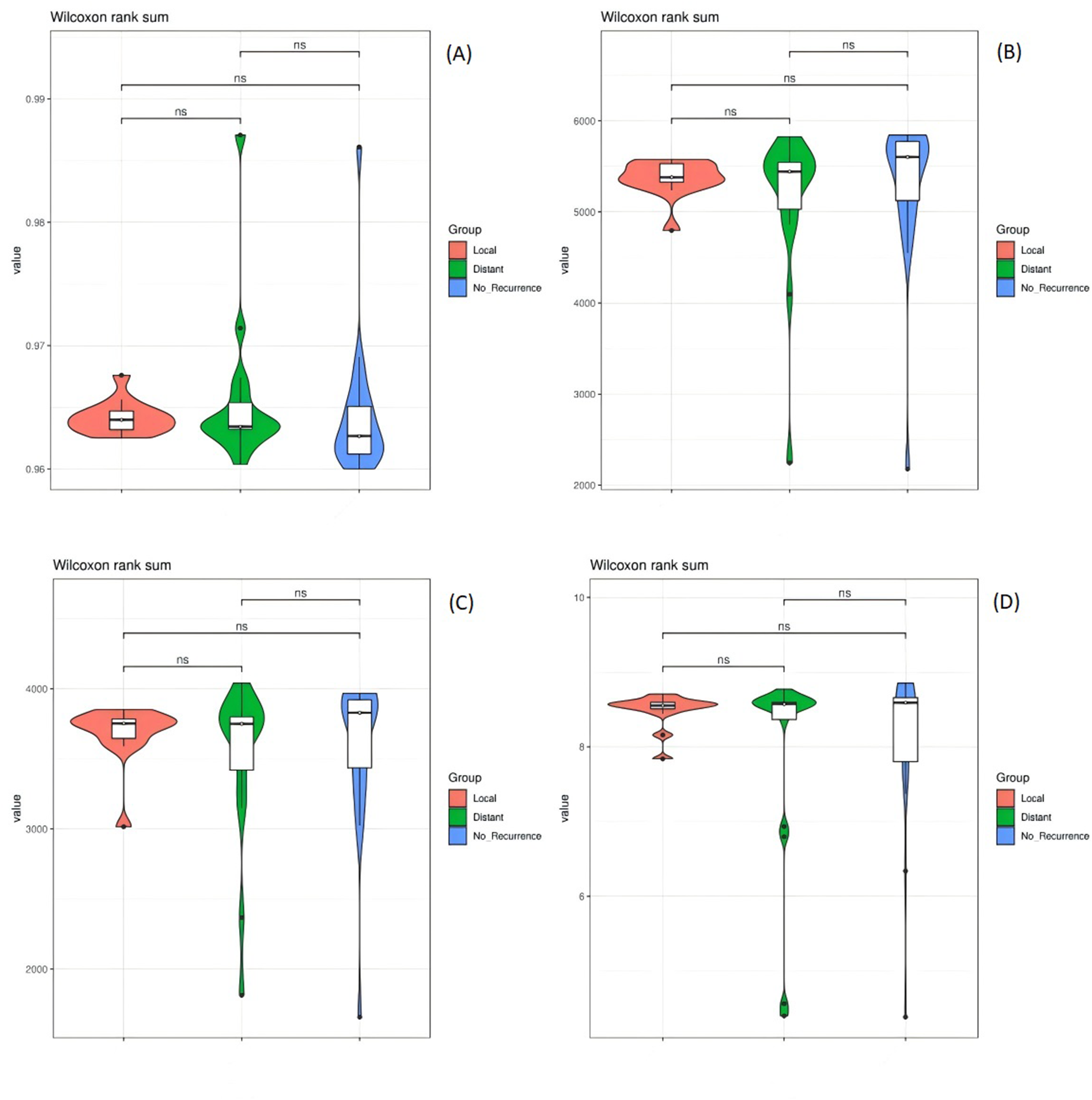
Analysis of bacterial profiles in the local recurrence, distant metastasis and no recurrence groups. A. Good's coverage indices for the three groups; B. comparison of bacterial richness (Chao 1) among the three groups; C. comparison of bacterial richness (observed species) among the three groups; D. comparison of bacterial diversity (Shannon) among the three groups. The Wilcoxon rank sum test was used for comparisons. * p value <0.05; ns p value >0.05.

Major active phyla (A), orders (B), families (C) and genera (D) in the local recurrence, distant metastasis and no recurrence groups.
Differences in gene expression profiles between er+/pr + tumour tissues of patients with and without recurrence/metastasis
Gene expression profiles were determined using RNA samples from breast tumour tissues of patients with ER+/PR + breast cancer. The Affymetrix Clariom D Human Assay contains 135,750 probe sets, including 18,858 Entrez Gene RNAs and 66,845 lncRNAs. When we defined a DEG as a gene with a > 1.5-fold change in expression compared with the reference (FDR p < 0.05), we identified 728 DEGs between the distant metastasis group and the no recurrence group, while only 4 DEGs was identified between the local recurrence group and the no recurrence group including Phospholipase A2, group V (PLA2G5, fold change 3.35, FDR p = 0.0000), PHD finger protein 11 (PHF11, fold change 1.62, FDR p = 0.0219) (supplementary file S1), microRNA 3689c and one noncoding gene. Among the 728 DEGs, specially, 338 upregulated genes and 390 downregulated genes, the most upregulated coding gene was PLA2G5 (2.70-fold) (supplementary file S1).
Discussion
Microbiota characteristics of tissue from tumours with local recurrence compared to tumours without recurrence
The analysis of 16S RNA sequencing of the solvent used in this study showed a much lower and completely different microbial content than that in FFPE samples, following the method described by Enuo Liu et al. 17 As environmental controls, two blank digestion buffer added protease were processed in parallel with the FFPE samples. The two environmental controls contained completely different microbiota abundance compared to the FFPE samples, except Muribaclaceae had a 38% relative abundance (Supplementary file S2). Therefore, the relative activities of microbiota in each group were calculated after excluding the contaminant RNA sequences (Table 2). In addition, the process was performed in clean room mainly involved deparaffinization, protease digestion, nucleic acid isolation, DNase digestion, and final purification. Paraffin can preserve microorganisms, but microorganisms will not proliferate in paraffin. Therefore, the results regarding bacteria obtained from our results are convincing.
Relative activities and ratios of tumour microbes in the no recurrence, distant metastasis and local recurrence groups.
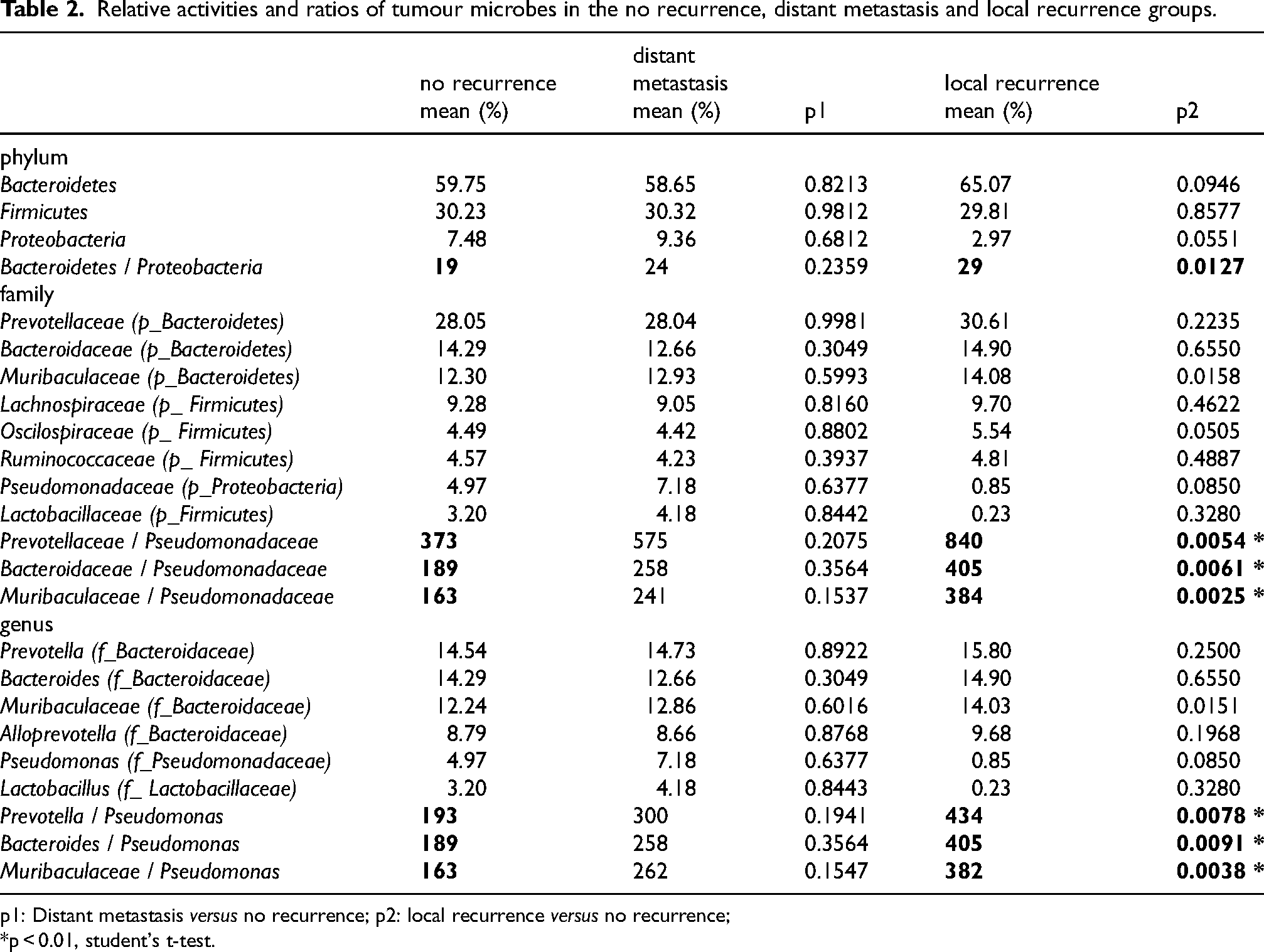
p1: Distant metastasis versus no recurrence; p2: local recurrence versus no recurrence;
*p < 0.01, student's t-test.
In contrast to freshly frozen tissues, RNA degradation in FFPE samples requires special consideration. Notably, all FFPE samples were processed under standardized sterile conditions and identical preservation methods (10μm sections, sealed and refrigerated storage), ensuring comparability across the groups. Regarding microbial analysis, we targeted the V3-V4 hypervariable regions (343F: 5′-TACGGRAGGCAGCAG-3′; 798R: 5′-AGGGTATCTAATCCT-3′) as the amplification region, which provides two advantages: 1, a relatively short amplicon length (≈460 bp) and 2, a mid-gene targeting strategy avoiding the more degradation-prone 5’ and 3’ terminal. These characteristics substantially reduce the impact of RNA degradation on amplification efficiency.
At the phylum level, Bacteroidetes (average 61.05%, ± 1.0119), Firmicutes (average 30.16%, ± 0.0075) and Proteobacteria (average 6.61%, ± 1.1770) were the most active phyla in all samples in the present study (Table 2). However, the most abundant phyla in both healthy breast tissue and breast tumours are Proteobacteria (more than 50%) in previous studies.12,13 The differences between the results in this study and those reported before for White women were considered to arise from the different methods used. In this study, total RNA was reverse transcribed into cDNA and used for PCR amplification of the bacterial 16S rRNA, instead of total DNA. The higher Bacteroidetes and Firmicutes activity in this study might indicate the higher transcriptional activity but not higher abundance in tumour tissues.
There are 8 main families in the tumour tissues over 80% activities, including anaerobic bacteria Preotellaceae, Bacteroidaceae, Muribaculaceae, Lachnospiraceae, Oscilospiraceae, Ruminococcaceae and aerobic bacteria Pseudomonadaceae, facultative anaerobic bacteria Lactobacillaceae. Interestingly, anaerobic bacteria Oscilospiraceae was more active in local recurrence group than no recurrence group (5.53% vs 4.48%, p = 0.0324), while aerobic bacteria Pseudomonadaceae (0.85% vs 4.96%) and facultative anaerobic bacteria Lactobacillaceae (0.23% vs 3.14%) showed decreasing trend in local recurrence group than no recurrence group (p > 0.05). Similarly for the genus level, Pseudomonas (0.85% vs 4.96%) and Lactobacillus (0.23% vs 3.14%) showed decreasing trend in local recurrence group than no recurrence group (p > 0.05), while anaerobic bacteria Prevotella, Bacteroides, Muribaculaceae and Alloprevotella 19 showed increasing trend with no significant difference.
Since hypoxia (low oxygen concentration) in tumour tissues is the characteristic of breast cancer and is supposed to associate with a significantly higher risk of metastasis and patient mortality,20,21 the more serious hypoxic microenvironment might contribute to the lower ratio of strict aerobic bacteria activities in local recurrence group. According to this hypothesis, the representative strict anaerobic bacteria Muribaculaceae and aerobic bacteria Pseudomonas were calculated their ratio of activities, which indeed had a significant higher ratio in local recurrence group compared to no recurrence group (p < 0.01) (Table 2) and no significant difference was shown between distant metastasis and no recurrence group. Muribaculaceae was reclassified in 2019 based on genomic data. This bacterial family is predominantly found in the gut microbiota of warm-blooded animals, where it often represents a major constituent of the Bacteroidetes phylum. Elevated fecal abundance of Muribaculaceae has been linked to anti-inflammatory effects in both diet-induced insulin-resistant mice 22 and gastric cancer models, 23 suggesting its potential regulatory roles in immunoseppression. The breast tissue microbiota shares similar dominant phyla with gut microbiota-primarily Proteobacteria, Firmicutes, Actinobacteria and Bacteroidetes, 12 and the hypoxic microenvironment may enhance microbial colonization, 24 such as Muribaculaceae (Bacteroidetes phylum) in breast tumour. While the anaerobic conditions within tumours create an inhospitable niche for aerobic Pseudomonas. On the other hand, early from 1980's, nonpathogenic and anaerobic bacteria has been used to proliferate specifically targeting a solid tumour following administration and carrying anti-tumour drugs. 25 This from one side indicated that, the hypoxic microenvironment within tumour tissues is more conductive to the colonization of strict anaerobic bacteria than facultative anaerobic bacteria. The ratio of strict anaerobic bacteria and facultative anaerobic bacteria activities could be a risk prediction factor for local recurrence in breast cancer, which needs to be further verified with large samples.
On the other hand, potential confounders including HER2 status, number of positive lymph nodes, receipt of post-surgery chemotherapy, tamoxifen use, tumour size and histological grade, were examined with Chi-square test. None of these confounders showed a significant association with recurrence status, since a Cramer's V value >0.5 or p < 0.01 was considered indicative of significant association (Table 1). Regarding axillary lymph node involvement, patients were categorized into those with 0–3 positive nodes and those with more than 4 positive nodes. This stratification was based on evidence that the risk of local recurrence after mastectomy increases with the number of affected lymph nodes. 26 Current guidelines recommend postmastectomy radiotherapy as adjuvant treatment for women with breast cancer who have four or more positive axillary lymph nodes. Among patients with 1 to 3 positive lymph nodes, the incidence of local recurrence were lower (approximately 1%) and were not associated with receipt of regional nodal irradiation.27,28
Gene expression correlated with microbiota characteristics of breast tumour with local recurrence
The expression of 31 coding genes was upregulated in the distant metastasis group compared with the no recurrence group, including 5 that were already reported as breast cancer biomarkers or markers of distant metastasis, including PLA2G5, GLS,29–31 HDAC6,32–34 IL5 35 and ZRANB1. 36 However, only 2 coding genes were upregulated in the local recurrence group compared to the no recurrence group, PLA2G5 and PHF11 (supplementary file S1).
As described previously, there was a difference between local recurrence and no recurrence groups as increasing activities of anaerobic bacteria and decreasing activities of aerobic bacteria. Analysis of correlation with the activities of Muribaculaceae / Pseudomonas ratio among all of the 52 tumour tissue samples indicated methylsterol monooxygenase 1 (MSMO1) (local recurrence vs no recurrence, fold change 2.32, p = 0.0011, FDR p = 0.1968) and PLA2G5 had significantly positive correlations (Table 3). MSMO1 is an enzyme of cholesterol biosynthesis, whose overexpression enhances resistance of paclitaxel and doxorubicin in breast cancer.37,38 The higher expression of MSMO1 also associates with poor survival in cervical cancer.39,40 Plasma sPLA2s are the biomarker of breast cancer, 41 and low oxygen concentration is a simulator of releasing sPLA2s into extracellular. 42 PLA2s compose a superfamily that is generally divided into six subfamilies: cytosolic PLA2s (cPLA2s), calcium-independent PLA2s (iPLA2s), secreted PLA2 s (sPLA2s), lysosomal PLA2s, platelet-activating factor acetylhydrolases, and adipose-specific PLA2s. 43 PLA2G5 was significantly higher in both the local recurrence (fold change 3.35, FDR p = 0.0000) and distant metastasis groups (fold change 2.70, FDR p = 0.0002) than in the no recurrence group in the present study, indicated higher express of PLA2G5 relating to carcinogenesis.
Gene's expressions that significantly correlated with the ratio of Muribaculaceae and Pseudomonas activities in ER + PR + tumour samples among all of the 52 patients.
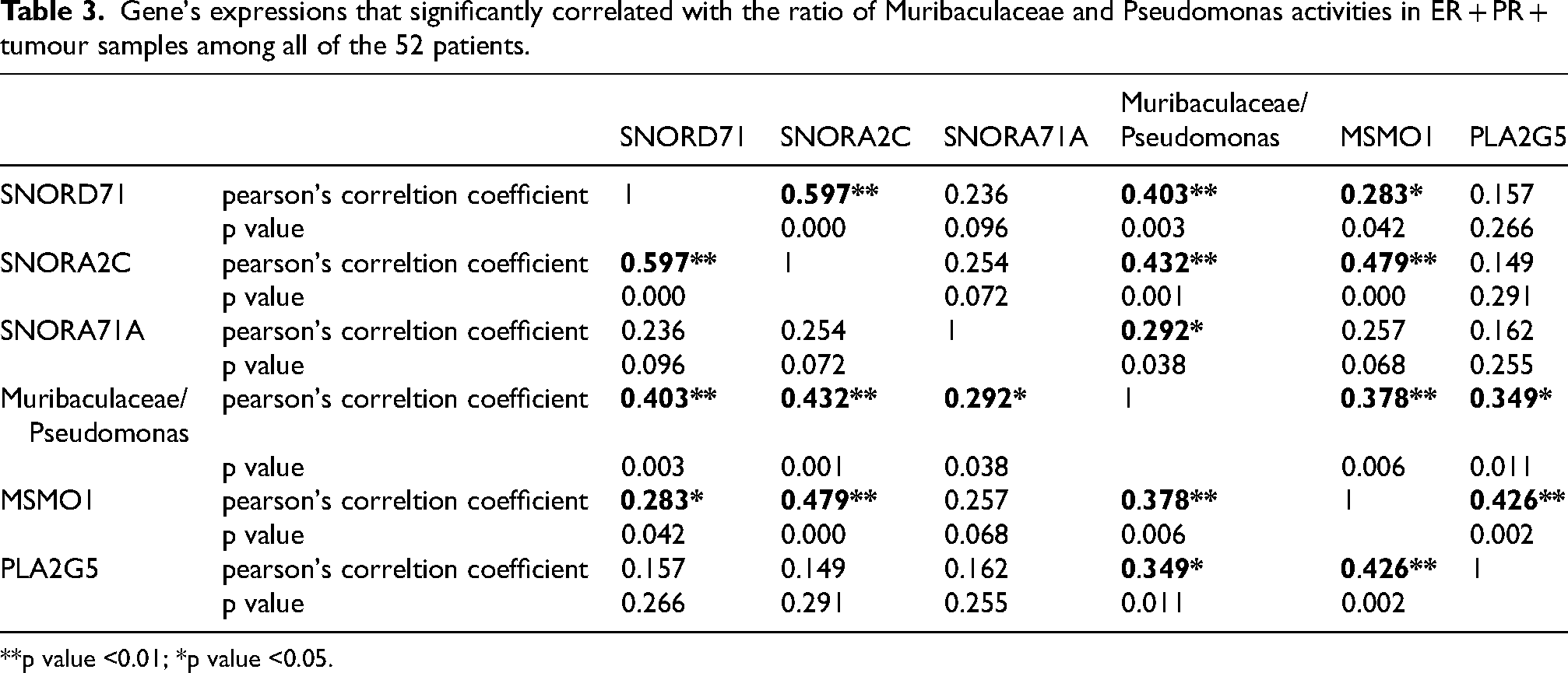
**p value <0.01; *p value <0.05.
Moreover, the activities of Muribaculaceae / Pseudomonas ratio also positively correlated with three small nucleolar RNA, including SNORD71 (small nucleolar RNA, C/D box 71), SNORA2C (small nucleolar RNA, H/ACA box 2C) and SNORA71A (small nucleolar RNA, H/ACA box 71A) (Table 3). They are all higher expressed in local recurrence than no recurrence group, with 9.00 fold change for SNORD71 (p = 0.0190, FDR p = 0.3659) and 2.68 fold change for SNORA2C (p = 0.0106, FDR p = 0.3149), 1.16 fold change for SNORA71A (p = 0.1719, FDR p = 0.6432). Small nucleolar RNA are conserved 60–300 nucleotide noncoding RNAs locating in the eukaryotic cell nucleolus, and involved in post-transcriptional regulation of mRNAs. Some of them had been demonstrated in cancer, such as SNORA71A, whose overexpression promoted breast tumour growth and metastasis in vivo. 44 The characteristic microbiota in tumour tissues for local recurrence correlated to genes expression for mRNA post-transcriptional regulation, drug resistance, and carcinogenesis in ER + PR + breast cancer. The mechanism needs further studies.
Evidence suggests that bacteria residing in the human gut may translocate to mammary tissue. These microorganisms may have reached the mammary gland through the nipple's skin, 45 or they could be transported by host cells 46 and then colonization in the tissue. In breast tumour tissue, microbiota changes due to alteration in the microenvironment, while casino genes expression alteration could also be a response to hypoxia, 47 and they exhibit a significant correlation. 17 However, there is no definitive evidence proving that these microorganisms directly influence genes expression. It is more likely that the microbiota changes from the adapting to the microenvironment. On the other hand, the tumour microenvironment may be influenced by complex reasons including gut microbiota through the modulation of immune cells’ activity 48 or bacterial metabolites. 49 Therefore, changes in the tumour tissue microbiota can predict alterations in the microenvironment 24 and may help forecast the future risk of cancer recurrence.
Limitations in this study
Due to the limited sample size (n = 52), our study lacked sufficient statistical power to perform subgroup analyses stratified by menopausal status, age, or breastfeeding history. Furthermore, while we identified several potential confounding factors (including Chinese medicine use, chemotherapy, and radiotherapy treatments, as summarized in Supplementary file S3); the restricted sample size similarly precluded meaningful investigation of these variables’ potential influences. As all study participants (n = 52) were ethnically Chinese, these findings require validation in more diverse populations.
Technical limitations may introduce bias for microbiota analysis due to potential RNA degradation, since only FFPE samples were available for this retrospective study. While uniform preservation conditions and standardized processing protocols improved inter-group comparability. Further studies should utilize fresh frozen tissue samples with larger cohorts for prospective validation, together with key genes confirmation by qPCR, which linked to local recurrence-specific microbiota patterns in this study. Furthermore, mechanistic insight is required under hypoxic conditions in vitro, as it remains unclear whether the characteristic microbiota merely reflect tumour microenvironment alterations or directly modulate the carcinogenic-related genes expression.
Conclusion
As indicated by the present study, the characteristics of the tumour microbiota was firstly studied here with respect to recurrence in ER+/PR + type breast cancer. The increased ratio of strict anaerobic bacteria and aerobic bacteria activities in tumour tissues, such as Muribaculaceae / Pseudomonas ratio, could be one of the predictors for local recurrence within 7 years following first surgery.
Supplemental Material
sj-docx-1-cbm-10.1177_18758592251381084 - Supplemental material for Tumour microbiota activities associated with local recurrence in ER + PR + breast cancer
Supplemental material, sj-docx-1-cbm-10.1177_18758592251381084 for Tumour microbiota activities associated with local recurrence in ER + PR + breast cancer by Sean Si Qian Ma, Luyi Ye, Fan Zhang, Tiansheng Xu, Zai-Si Ji and Enuo Liu in Cancer Biomarkers
Supplemental Material
sj-jpg-2-cbm-10.1177_18758592251381084 - Supplemental material for Tumour microbiota activities associated with local recurrence in ER + PR + breast cancer
Supplemental material, sj-jpg-2-cbm-10.1177_18758592251381084 for Tumour microbiota activities associated with local recurrence in ER + PR + breast cancer by Sean Si Qian Ma, Luyi Ye, Fan Zhang, Tiansheng Xu, Zai-Si Ji and Enuo Liu in Cancer Biomarkers
Supplemental Material
sj-xlsx-3-cbm-10.1177_18758592251381084 - Supplemental material for Tumour microbiota activities associated with local recurrence in ER + PR + breast cancer
Supplemental material, sj-xlsx-3-cbm-10.1177_18758592251381084 for Tumour microbiota activities associated with local recurrence in ER + PR + breast cancer by Sean Si Qian Ma, Luyi Ye, Fan Zhang, Tiansheng Xu, Zai-Si Ji and Enuo Liu in Cancer Biomarkers
Footnotes
Abbreviations
Acknowledgements
We thank Drs. Ming Xu and Jianyu Pei of the Central Hospital of Huangpu District, Shanghai, and Dr Xiaolin Wang of Shanghai Meiji Health Science and Technology Co., Ltd for their assistance with FFPE sample preparation.
Ethics approval and informed consent statements
The Medical Ethics Committee, Shanghai Institute of Planned Parenthood Research approved the protocols for RNA extraction, microarray hybridization, 16s rRNA gene amplicon sequencing, and data analysis (approval number PJ2019-18). The study was performed in accordance with the guidelines of the Declaration of Helsinki. All patients or their legal guardians provided written informed consent to participate in this study.
Authors’ contributions
ZSJ designed the study and helped preparing the manuscript. LY and SSM performed the data analysis and prepared Figures. FZ and TX performed the experiments. EL wrote the manuscript. FZ, TX and EL have seen and can confirm the authenticity of the raw data. All authors reviewed the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The microarray data were deposited in the Gene Expression Omnibus (GEO) database under accession codes GSE183231 and GSE185439, which were obtained from the same cohort experiment. The 16S rRNA sequencing data have been uploaded to GenBank Sequence Read Archive under accession number PRJNA769523. The other data and materials used in this study are available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.