
Abstract
Background:
The goal of treatment in early onset scoliosis patients is to control the deformity while allowing chest and spinal growth. However, management, either conservative or surgical, remains controversial and require further clinical evidence. The aim of this study was to determine best practice guidelines for the management of early onset scoliosis patients in Europe.
Methods:
A Delphi approach was used among European experts to determine consensus in: (1) identification of progression risk factors, (2) clinical and radiographic evaluation, (3) conservative treatment, and (4) surgical management. Idiopathic and non-idiopathic groups were analyzed separately. Statements were only included in the final agreed consensus if at least 80% of respondents agreed with the statement.
Results:
A total of 22 pediatric orthopedic surgeons completed the first and second surveys, and 21 the third. Out of open-ended questions included in the initial Delphi, 75 statements for 59 multiple-choice questions in the idiopathic group and 47 statements for the 44 multiple-choice questions for the non-idiopathic group were formed for the second round. Of the total 122 statements, 50 (40.9%) reached consensus, and 72 did not. Among the 72 statements re-evaluated in Round 3, consensus was reached on 69 (96%).
Conclusion:
Early onset scoliosis represents a rare, heterogeneous, but life-threatening condition often associated with insufficient relevant evidence. Consensus is difficult to achieve (39.3% of the 122 statements), especially in the non-idiopathic group. However, 48 guidelines (33 for idiopathic and 15 for non-idiopathic) were provided by European experts to improve early onset scoliosis management.
Level of Evidence:
IV
Keywords
Introduction
Early onset scoliosis (EOS) is defined as a spinal deformity before the age of 10 years, often associated with a high progression risk if left untreated. The main etiologies are idiopathic, syndromic, neuromuscular, and congenital. 1 EOS is a very heterogeneous condition in terms of magnitude, curve location, and progression, but also sagittal alignment. The goal of treatment, either conservative or surgical, is to control the deformity while allowing chest and spinal growth, with the least possible negative consequences on patients’ quality of life.
Due to the rarity of this condition, it is often difficult to provide evidence-based treatment guidelines. The standard of care, therefore, greatly varies among but also within countries, and even between surgical departments. In addition, physicians have a tendency to modify their management over time based on the literature and their personal experience. As a matter of fact, Matsumoto et al. have recently shown that the initial enthusiasm that existed with growth-friendly surgical techniques has declined, and that preferences for conservative treatment have increased over the last 10 years. 2 The spectrum of management strategies ranges from observation to casting, full or part-time bracing, and numerous growth-friendly surgical techniques (distraction-based, growth guidance, or compression-based). However, all these procedures remain associated with high rates of complications and unplanned returns to the operating room. 3 Therefore, early spinal fusion is also an option in children with limited growth potential, such as some syndromic etiologies (skeletal dysplasia for example), or with severe neurologic co-morbidity (cerebral palsy).4,5
When no high-quality clinical studies are available (or are even practical to perform), consensus recommendations by specialist organizations are a constructive way forward. The Delphi method is an interactive way for a panel of experts to reach consensus.6–8 It has the advantage that many individuals can contribute anonymously, without the process being dominated by a few individuals who may have particularly strong opinions on a topic. The aim of this study was, therefore, to provide best practice guidelines for EOS (idiopathic and non-idiopathic) from a group of European experts.
Materials and methods
The European Paediatric Orthopaedic Society (EPOS) spine study group identified the need to provide best practice guidelines for EOS management. Therefore, a three-round Delphi process was used to try to obtain consensus among 22 European experts in pediatric spine, representing 11 countries. The experts included 16 members of the EPOS Spine study group, and 6 non EPOS-members, identified and selected by vote by the study group members. All experts were highly specialized in pediatric deformity care, with more than 15 years of practice, and worked in academic environments (20 different departments) with access to the most advanced technologies. The steering committee consisted of three experienced pediatric orthopedic spine surgeons and a biostatistician expert on Delphi. The relevant literature was reviewed, and areas of controversy were established regarding (1) definition, (2) prognostic risk factors, (3) conservative treatment, (4) surgical management, (5) complications, and (6) graduation. Surgeons were surveyed for current practices, presented with the results of the systematic review, and asked to vote anonymously for or against item inclusion during the three iterative rounds.
Delphi process
Round 1 questionnaire included open-ended questions (52 for idiopathic and 57 for non-idiopathic), and the respondents were asked to specify their treatment choices in different scenarios (Figure 1). Round 2 questionnaire included multiple-choice questions (MCQs; 59 for idiopathic and 44 for non-idiopathic) based on the data obtained in the first round. Questions were created as a “5-point Likert-type scale” (strongly agree, agree, neutral, disagree, strongly disagree) or had multiple answers. Threshold value for consensus was initially fixed as 80% at the second round. All the questions below this threshold value were asked again in the third round. In the third round, the response categories were given as “agree-neutral-disagree” in a three-point Likert-type scale, and previous answers from the group were visible. The classification of the consensus rates based on the responses received in the third round was as follows: ≥80% consensus rate: strong agreement or disagreement, 70%–79% consensus rate: moderate agreement or disagreement, 50%–69% consensus rate: weak agreement or disagreement, and <50% consensus rate: cannot be decided.
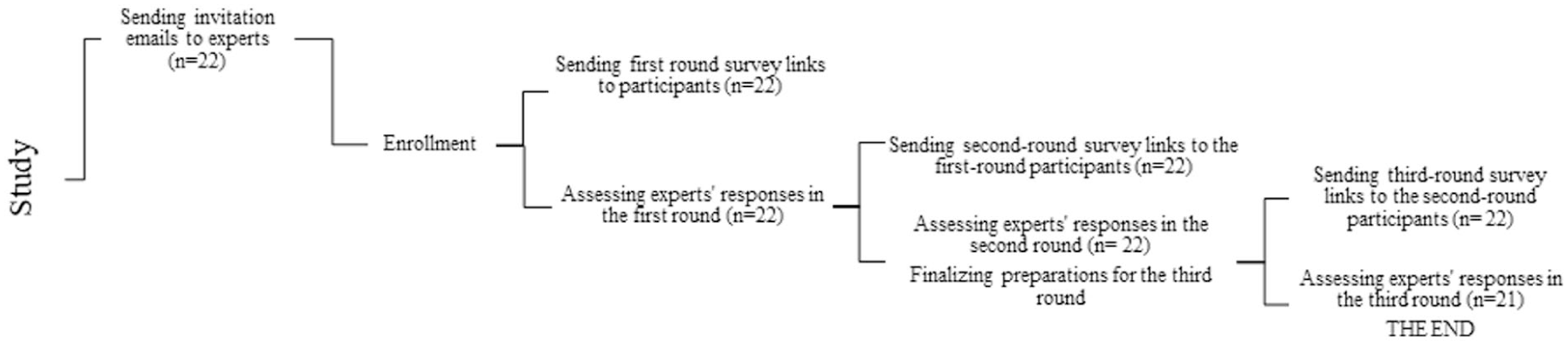
Flowchart on the Delphi method used in the current study.
It is important to note that the response formats varied across the questions. While some questions were presented in an agree–disagree format, others required participants to select from predefined options. For the agree–disagree questions, the level of agreement was quantified and categorized as strong, moderate, or weak based on percentage thresholds. In contrast, for questions requiring a selection among categories, agreement was not applicable; instead, a selection rate was calculated.
The term clear categorization refers to these cases, where the distribution of responses indicated a consistent and unambiguous choice by the majority of participants.
Data collection and management
Questionnaires were submitted online to the respondents consecutively in each round. Study data was collected and managed using Research Electronic Data Capture (REDCap) tools. REDCap is a secure, web-based application designed to support data capture for research studies, providing (a) an intuitive interface for validated data entry; (b) audit trails for tracking data manipulation and export procedures; (c) automated export procedures for seamless data downloads to common statistical packages; and (d) procedures for importing data from external sources.9,10
Results
The questions that reached strong agreement or disagreement are summarized in Tables 1–8, but the answers from experts for each MCQ are reported in Tables 9 and 10.
Statements regarding idiopathic EOS definition.
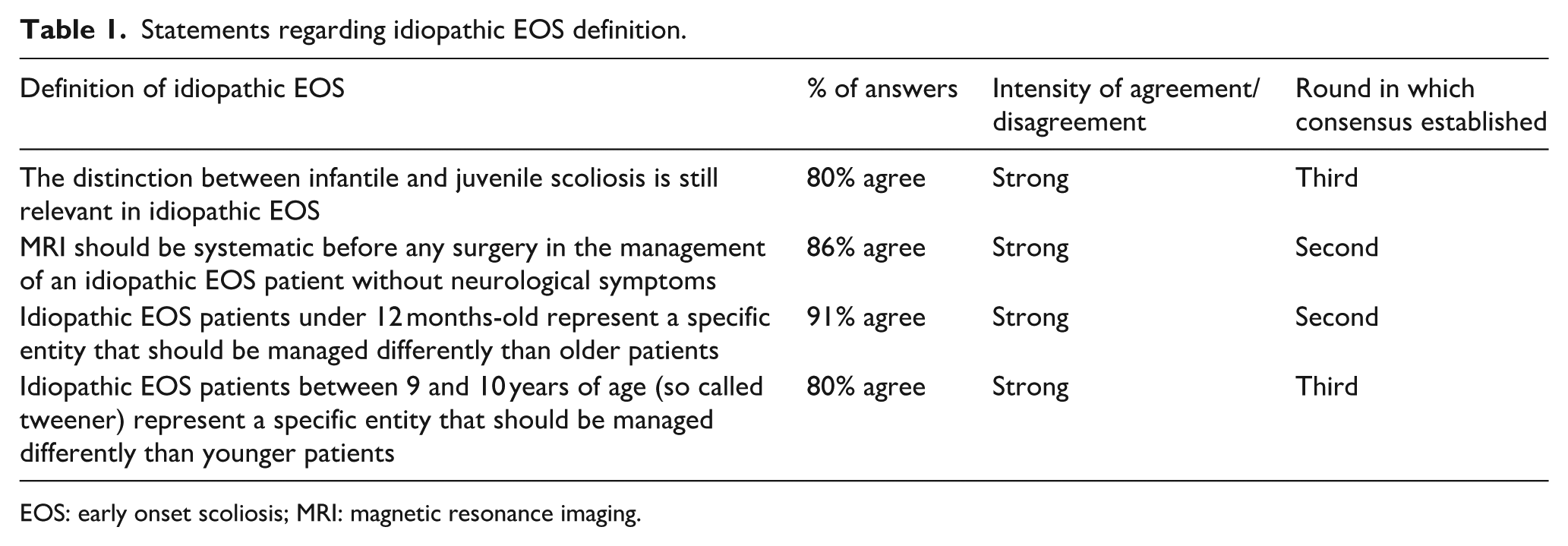
EOS: early onset scoliosis; MRI: magnetic resonance imaging.
Statements regarding idiopathic EOS prognosis factors.
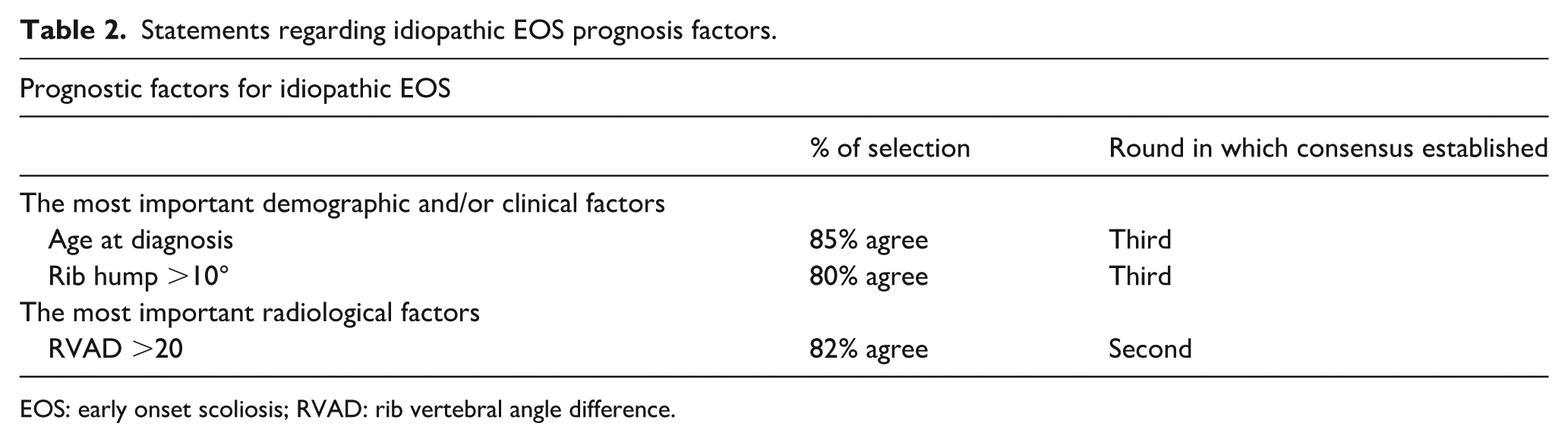
EOS: early onset scoliosis; RVAD: rib vertebral angle difference.
Statements regarding conservative treatment of idiopathic EOS.
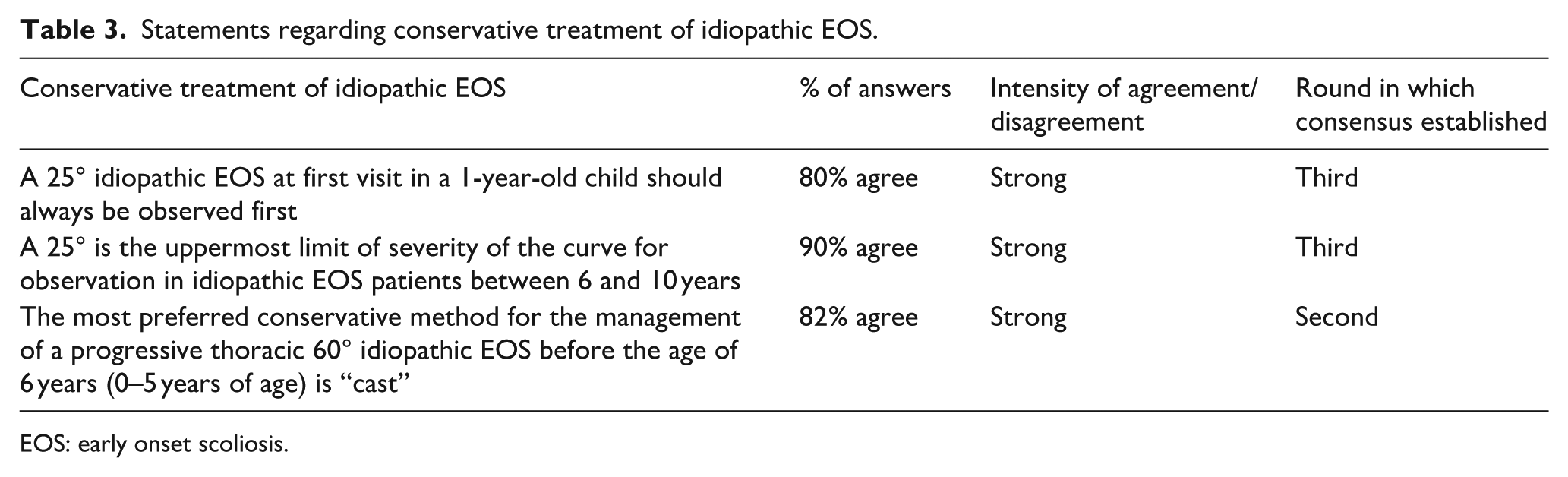
EOS: early onset scoliosis.
Statements regarding surgical treatment of idiopathic EOS.
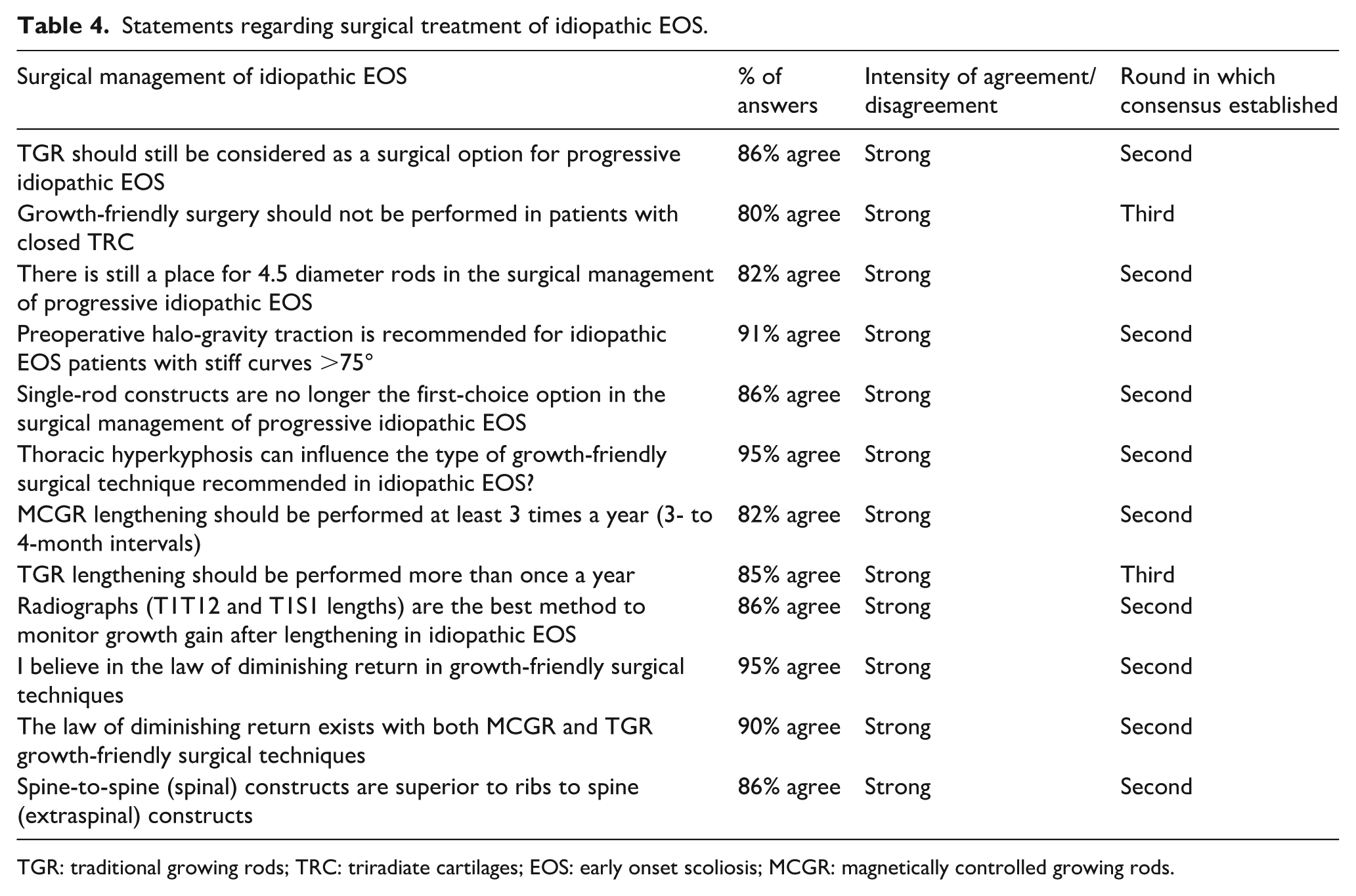
TGR: traditional growing rods; TRC: triradiate cartilages; EOS: early onset scoliosis; MCGR: magnetically controlled growing rods.
Statements regarding complications and graduation for idiopathic EOS.
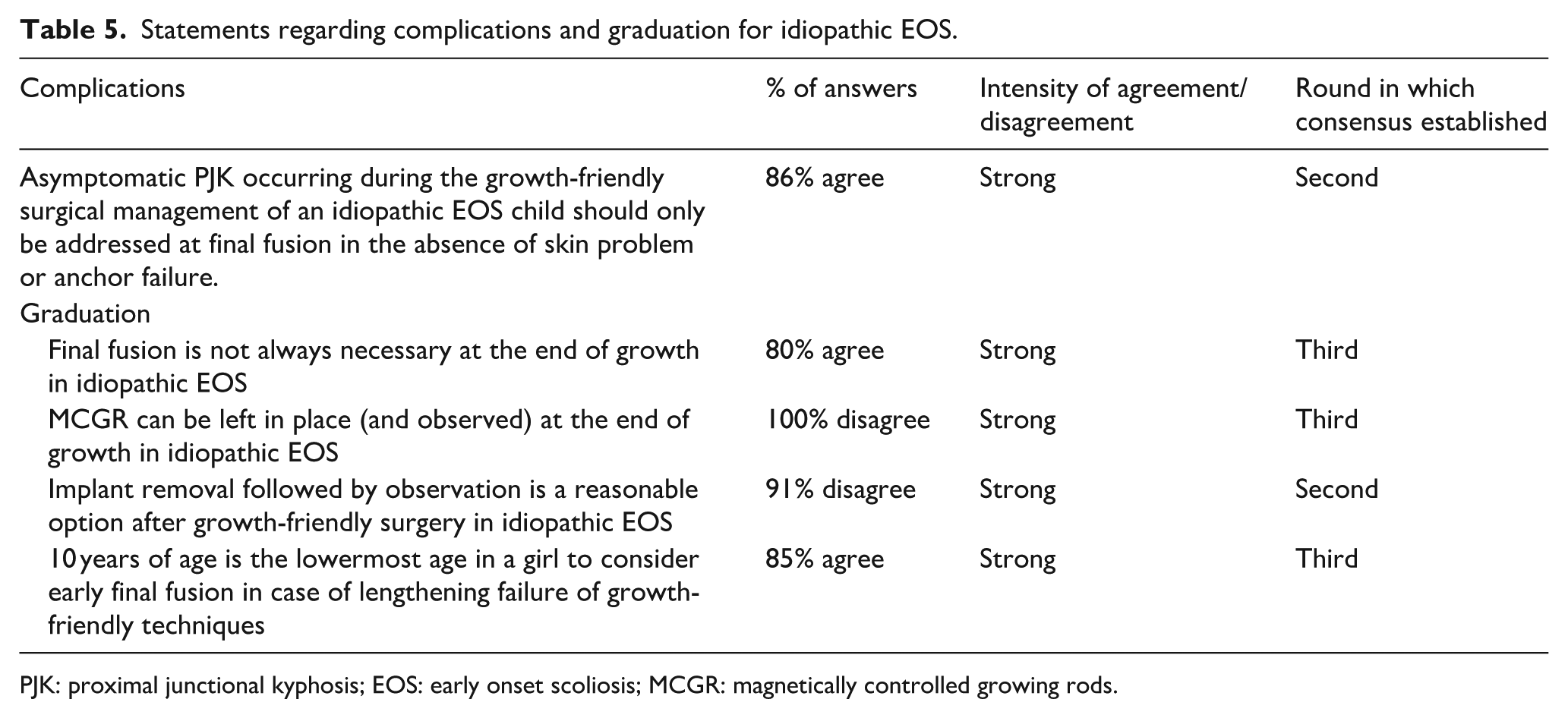
PJK: proximal junctional kyphosis; EOS: early onset scoliosis; MCGR: magnetically controlled growing rods.
Progression risk factors and additional imaging for non-idiopathic EOS patients.
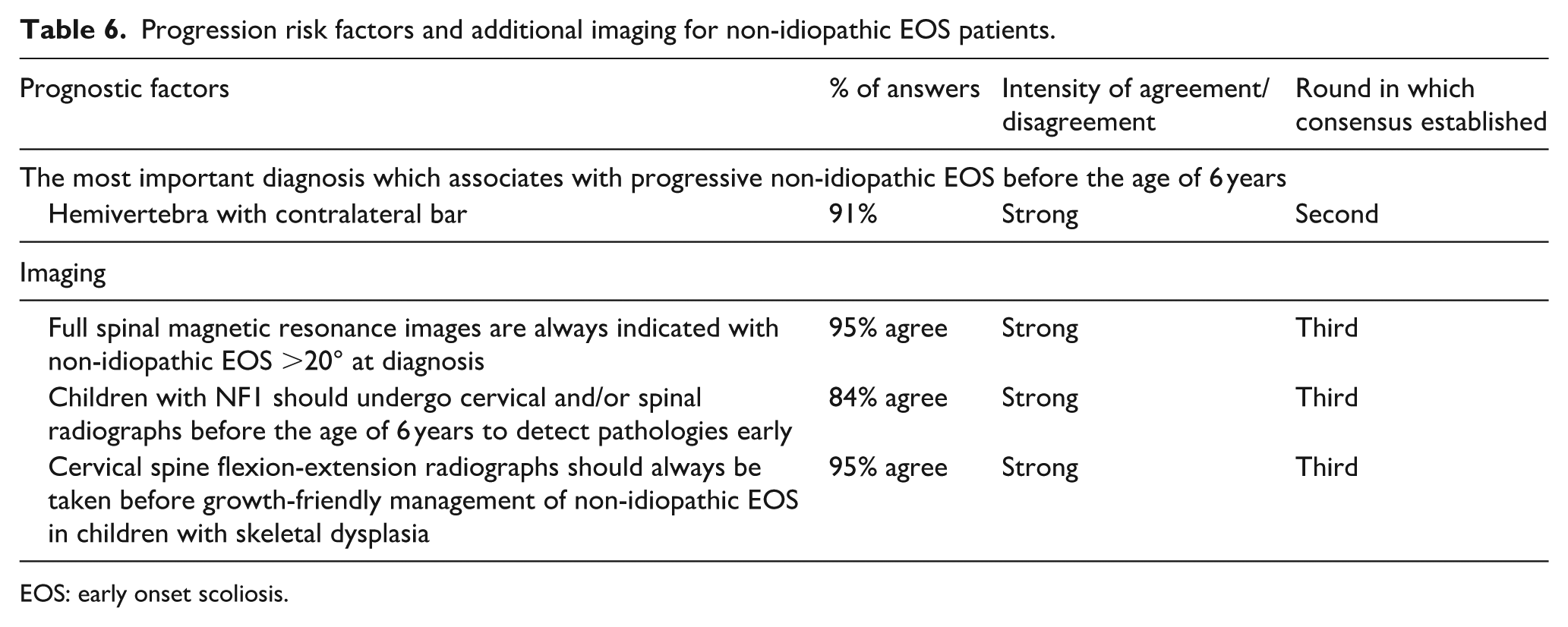
EOS: early onset scoliosis.
Non-idiopathic EOS
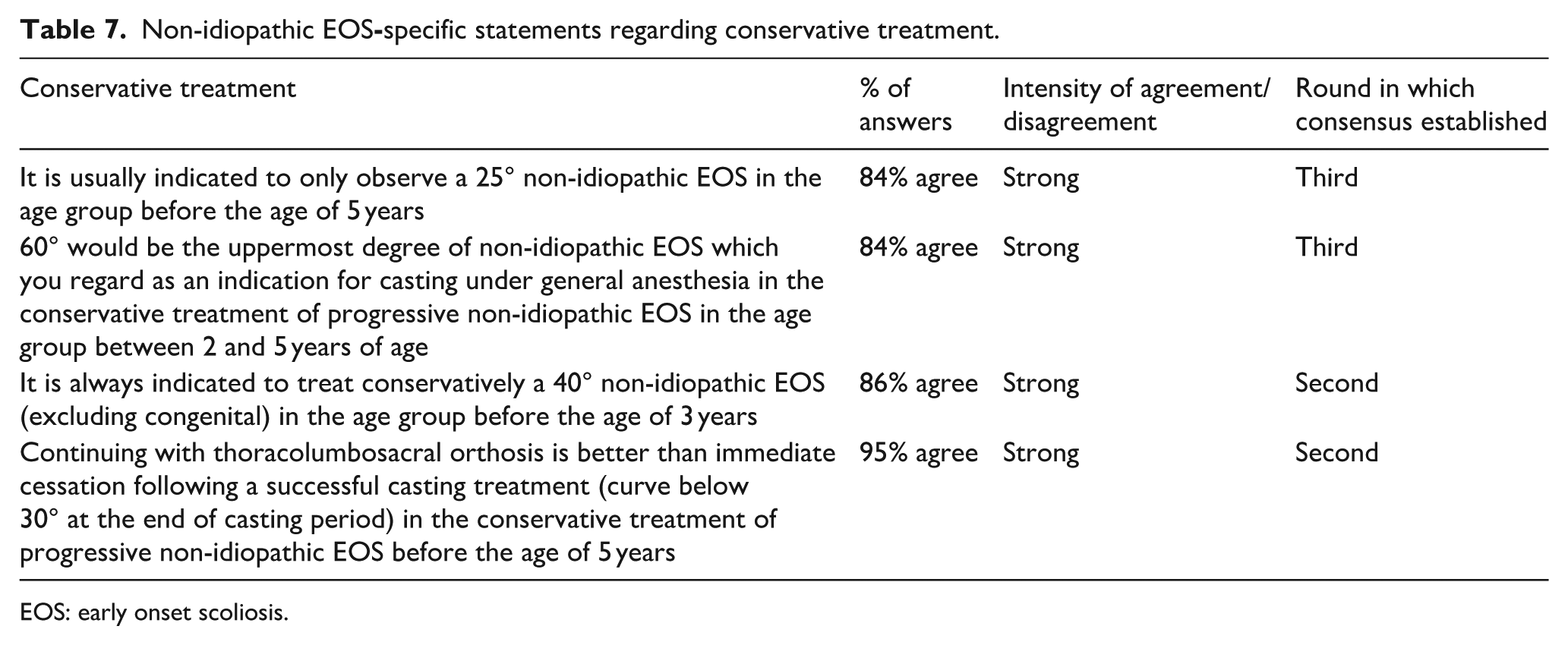
EOS: early onset scoliosis.
Non-idiopathic EOS
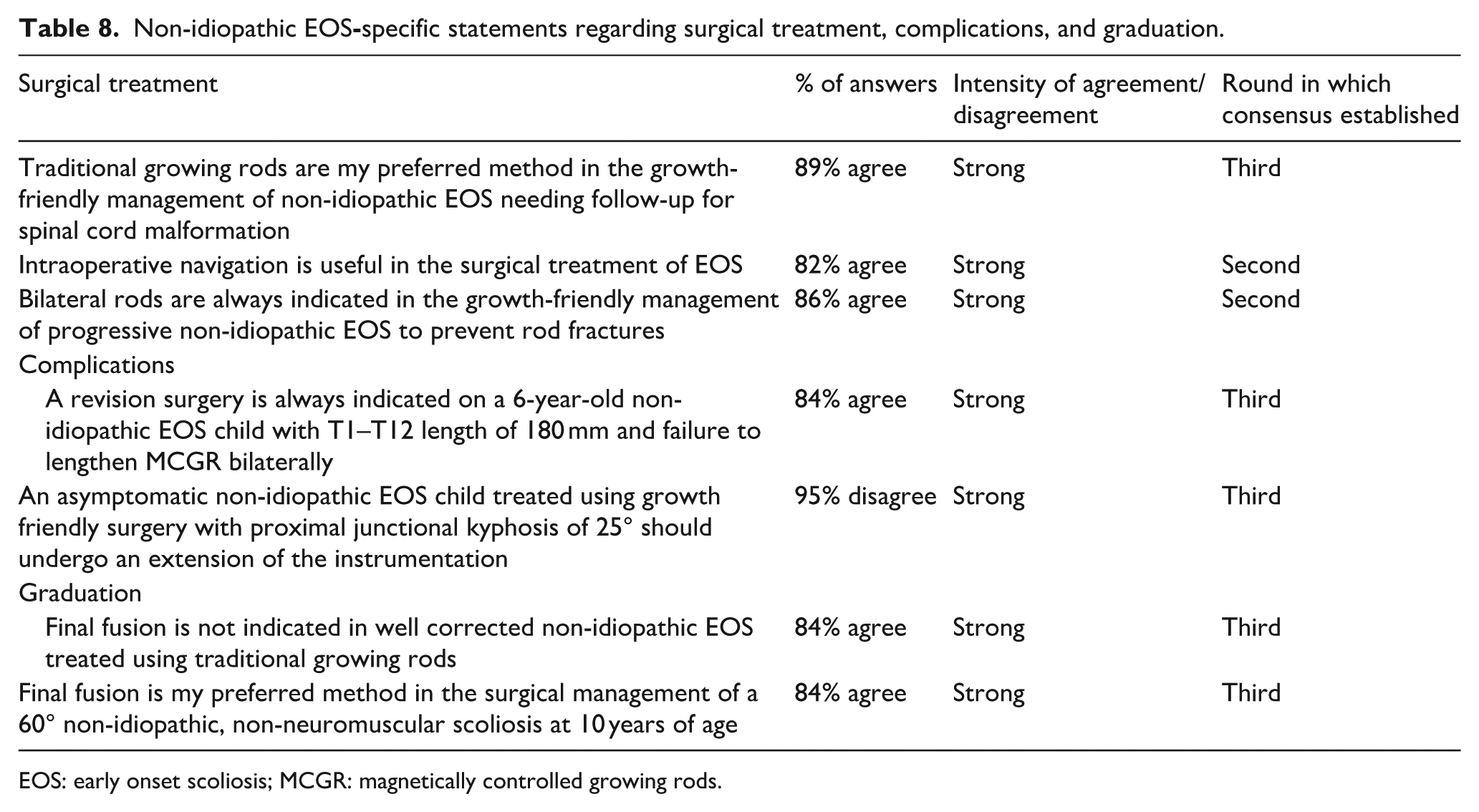
EOS: early onset scoliosis; MCGR: magnetically controlled growing rods.
Results on the 75 statements related to idiopathic EOS management.
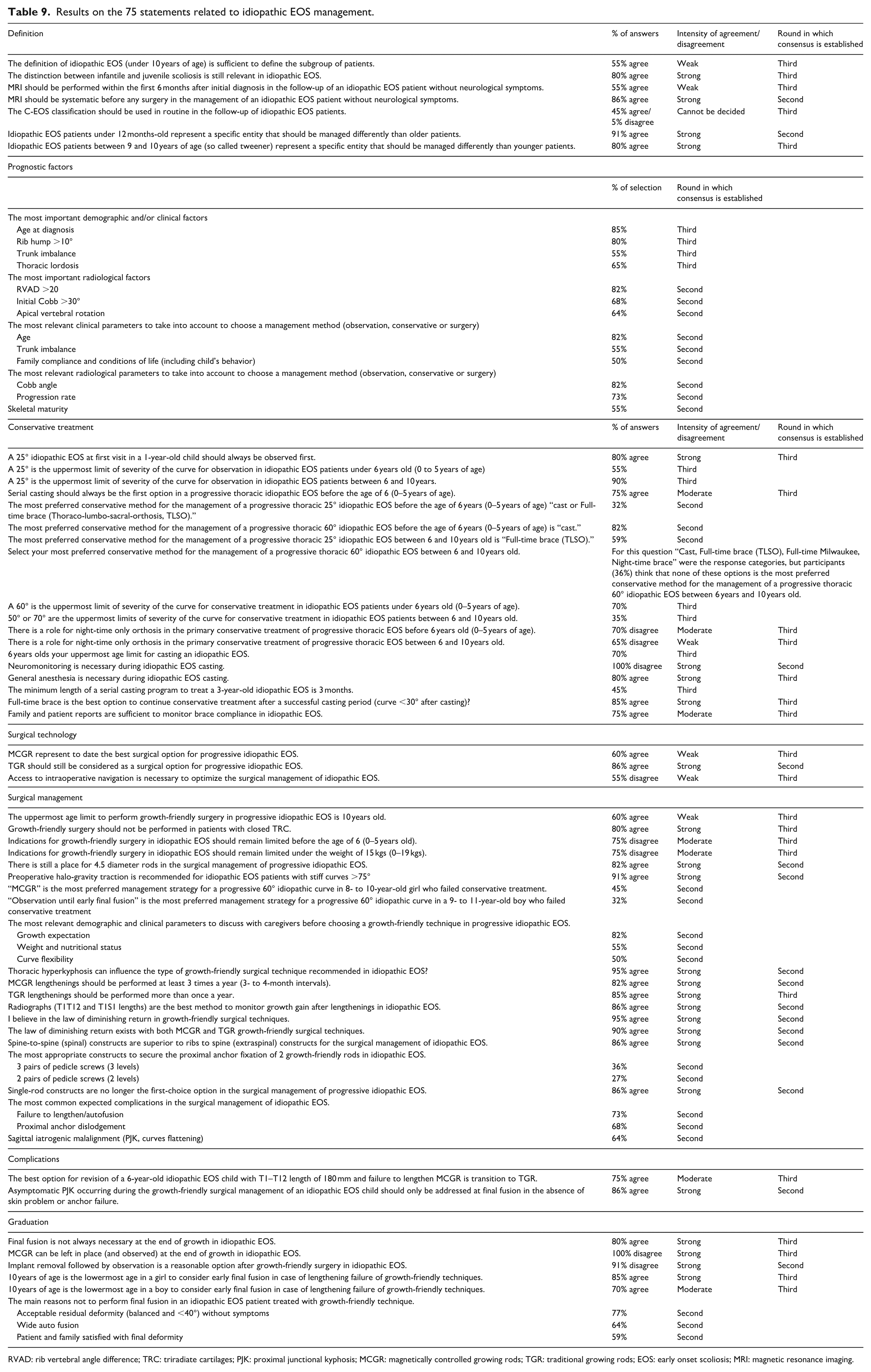
RVAD: rib vertebral angle difference; TRC: triradiate cartilages; PJK: proximal junctional kyphosis; MCGR: magnetically controlled growing rods; TGR: traditional growing rods; EOS: early onset scoliosis; MRI: magnetic resonance imaging.
Results on the 47 statements related to non-idiopathic EOS management.
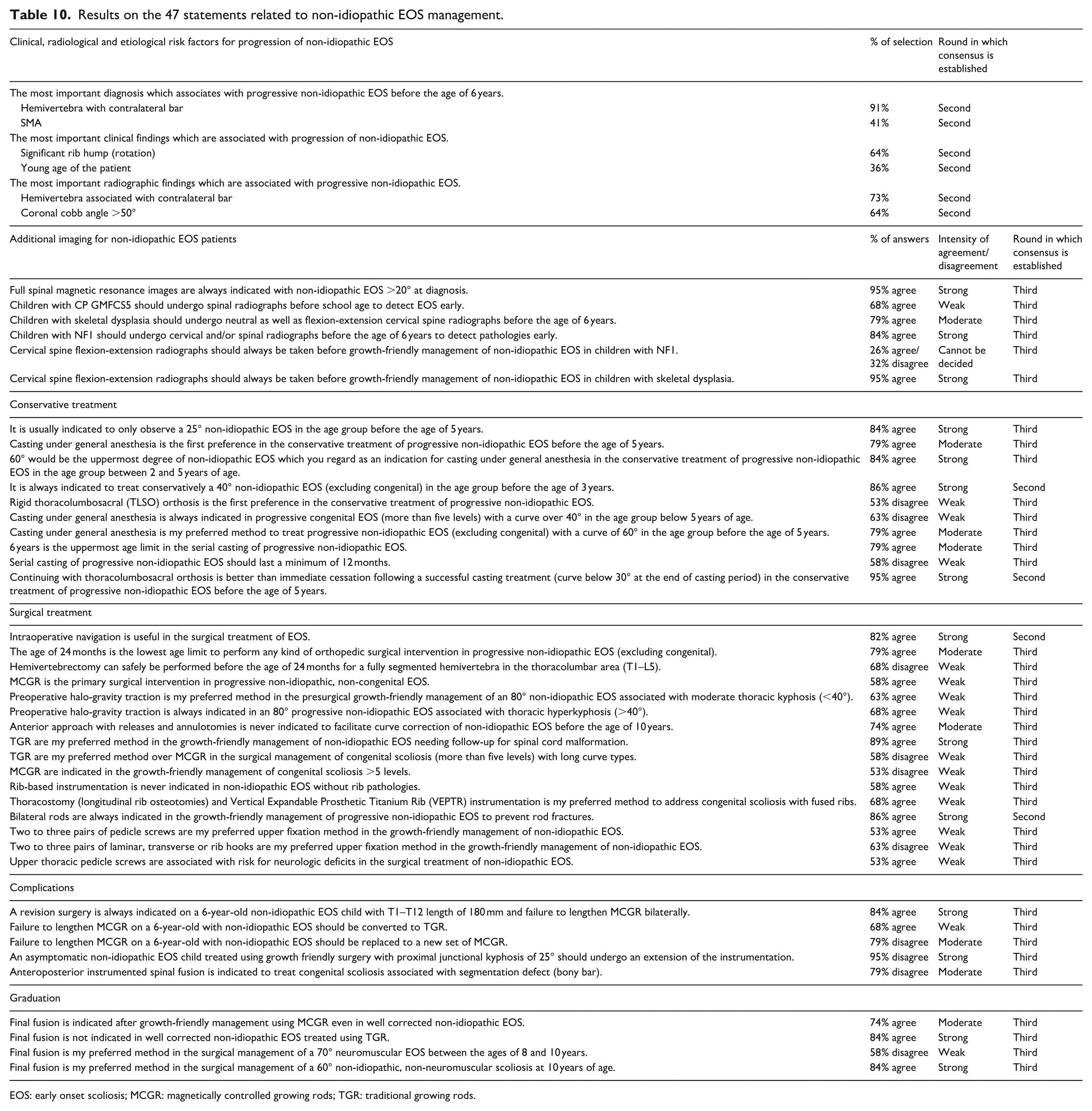
EOS: early onset scoliosis; MCGR: magnetically controlled growing rods; TGR: traditional growing rods.
Idiopathic EOS
Decisions were reached on 40 (53%) of the 75 statements for the 59 questions in the second round. Strong agreement was reached in 15 (38%) of these 40 statements, and clear categorizations were made in 25 (62%) of them. In 10 (29%) of the 35 statements remaining to the third round, a strong agreement was reached in the third round, clear categorizations were revealed in 10 (29%) statements, and weak and moderate agreement was obtained in 13 (37%) statements. At the end of the third round, no consensus was reached on 2 (5%) statements (Table 9).
Non-idiopathic EOS
Decisions were reached in the second round for 10 (21%) of the 47 statements for the 44 questions. Strong agreement was reached in 4 (40%) of these 10 statements and clear categorizations were made in 6 (60%) of them. Out of the 37 remaining statements to the third round, 9 (24%) obtained strong agreement, 1 (3%) had clear categorization, 26 (70%) had weak and moderate agreement, and 1 (3%) had no consensus after the last round (Table 10).
Discussion
The Delphi process led to a strong agreement for 44% of the statements for idiopathic EOS and only 31.9% in the non-idiopathic subgroup. EOS is a rare condition representing less than 10% of all pediatric spine patients, and its treatment is centralized into academic medical centers in Europe, as the risk of complications is significant and requires multiple specialties.
Idiopathic EOS
Twenty-seven guidelines with a high consensus rate (≥80%) were provided by European experts for the management of idiopathic EOS. Four statements with strong agreement were found regarding the definition of EOS (Table 1), but experts recommended to consider patients under 1 year old and tweeners as specific entities, which is currently not described in the EOS classification (C-EOS) reported by Williams et al. 1 Experts also agreed that magnetic resonance imaging was necessary before any surgical management, even without neurological symptoms, but not at initial diagnosis. Interestingly, the C-EOS was only moderately adopted by the European experts (45% of them used it in routine). Age and rotation (both clinical and radiological) were reported as the main prognostic parameters (Table 2). Radiologically, a rib vertebral angle difference >20° also reached strong agreement, while initial Cobb greater than 30° only reached a moderate one (68%).
Regarding conservative management, experts agreed that there was no rush to treat a 12-month patient with idiopathic EOS, and that 25° was the uppermost limit for observation between 6 and 10 years (Table 3). They also concluded that serial casting was the most appropriate treatment for a progressive 60° thoracic curve. The statement to always recommend cast as the first option in a progressive thoracic curve under 6 years old did not reach strong agreement (75%), as some experts preferred to use bracing (full or part-time) as initial management.
Experts agreed that growth-friendly surgery should not be performed in patients with closed triradiate cartilages, and that there is still a place for 4.5 diameter rods (Table 4). Europeans tended to be more surgically aggressive than their peers in the United States, especially in kids younger than 6 years old and under 20 kg (75%, moderate agreement).2,11,12 Preoperative halo-gravity traction is recommended for stiff curves >75°, and growth expectation remains the most relevant demographic and clinical parameter to discuss with caregivers before choosing a growth-friendly technique. Thoracic hyperkyphosis can also influence the type of surgical technique. No consensus was found to consider magnetically controlled growing rods (MCGR) as the best surgical option, and the only final statement was that traditional growing rods (TGRs) should still be considered (primary surgery or revision). Only 45% of experts agreed that navigation was necessary during surgery to optimize outcomes, and robotics was not included in the survey. MCGR lengthening should be performed at least three times a year (3- to 4-month intervals), while TGR lengthening should be considered more than once a year. Radiographs (T1T12 and T1S1 lengths) are the best method to monitor growth gain, and the law of diminishing return exists with both MCGR and TGR, as previously reported. 13 Spine-to-spine (spinal) constructs are preferred to ribs to spine (extraspinal) ones, and single-rod constructs are no longer the first-choice option. Asymptomatic proximal junctional kyphosis (PJK) is frequently observed during treatment, but it should only be addressed at final fusion in the absence of skin problem or anchor failure (Table 5).
Graduation remains a hot topic, with many different opinions and strategies.14–16 However, European experts concluded that implant removal alone and leaving MCGR in place were not options to consider in idiopathic EOS, while early fusion and observing TGR were reasonable in some cases.
Non-idiopathic EOS
Only 15 statements (31.9%) reached a high consensus rate (≥80%) in this heterogeneous and challenging subgroup. Hemivertebra with associated contralateral bar was identified as the situation with the highest progression risk. Full spinal magnetic resonance images should be obtained for all curves >20°, and cervical instability should be ruled out if surgery is considered in patients with skeletal dysplasia or NF1 (Table 6). Early identification and casting can significantly delay the need for surgery. 17 However, experts agreed that a 25° curve can only be observed first in children under 5 years old, while 40° curves require conservative management, and 60° curve represents the upper limit of casting (Table 7). A successful casting period should be followed by thoracolumbar bracing.
In case of surgery, bilateral rods are recommended to prevent rod fracture, and in opposition to the idiopathic group, navigation is considered helpful if available (Table 8). MCGR should not be considered when further spinal cord imaging is necessary during treatment, and radiological PJK is an expected and common phenomenon that does not require revision surgery in the absence of disabling symptoms. Failure to lengthen MCGR is another frequent complication, and revision (MCGR or TGR) is necessary if it happens in immature young children. 18
Final fusion is not always indicated in well-corrected and pain-free non-idiopathic EOS treated with TGR, so further cost/benefit analysis should be performed in fragile patients who remain flexible (Table 8).19–21 In case of successful conservative management, early definitive fusion remains a reasonable alternative in 10-year-old non-neuromuscular patients with curves exceeding 60°, in order to avoid repeated surgeries. 22
Interestingly, the management of congenital scoliosis did not reach any consensus among the experts, reflecting the various options in this subgroup and the lack of clinical evidence to support decisions (Table 10). Even if the level of agreement was weak (63%), casting under general anesthesia was not recommended in this category, even in progressive curves exceeding 40° before 5 years of age.
Limitations
The limitations of this study are inherent to Delphi, such as the bias induced by the selection of participants, the lack of clarity on the meaning of “consensus,” and also the difficulty of generalizing the results to a wider population. However, even though the process was quite time-consuming and laborious, the number of drop-out remained very limited (1 at round 3).
In conclusion, defining best practice guidelines remains difficult among European experts in the field of EOS, especially for the non-idiopathic group, which is a very heterogeneous and challenging condition. A true expert involvement in the management of these uncommon and frequently very challenging conditions remains necessary. However, this Delphi study provided 48 consensus statements which would be a good guide for spinal surgeons who have less space for EOS in their daily practice. Seeing the differences between Europe and other regions of the world will also be a good starting point for developing common solutions in the future to improve patients’ care.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251398742 – Supplemental material for Early onset scoliosis: Can Best Practice Guidelines Be Provided in Europe?
Supplemental material, sj-pdf-1-cho-10.1177_18632521251398742 for Early onset scoliosis: Can Best Practice Guidelines Be Provided in Europe? by Brice Ilharreborde, Muharrem Yazici, Selcen Yüksel, Pervin Demir and Ilkka Helenius in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
EPOS Spine Study Group and European experts involved in the study:
Brice Ilharreborde, France; Ilkka Helenius, Finland; Muharrem Yazici, Turkey; Javier Pizones, Spain; René Castelein, Netherlands; Kiril Mladenov, Germany; Thierry Odent, France; Giedrius Bernotavicius, Lithuania; Marco Brayda-Bruno, Italy; Neil Davidson, United Kingdom; Thanos Tsirikos, United Kingdom; Jorge Mineiro, Portugal; Carol Hasler, Switzerland; Marco Crostelli, Italy; David Farrington, Spain; Daniel Studer, Switzerland; Dror Ovadia, Israel; Kariman Abelin-Genevois, France; Moyo Kruyt, Netherlands; Martin Gehrchen, Denmark; Sebastian Pesenti, France.
Author contributions
Brice Ilharreborde, Muharrem Yazici, Ilkka Helenius: Conception and design.
Pervin Demir: Administrative support.
Brice Ilharreborde, Muharrem Yazici, Ilkka Helenius: Provision of study material.
Selcen Yüksel: Collection and assembly of data.
Selcen Yüksel, Brice Ilharreborde: Data analysis and interpretation.
All authors: Manuscript writing.
All authors: Final approval of manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Brice Ilharreborde declares to perceive royalties and to be a consultant for Medtronic and Implanet and to perceive royalties from Highridge, outside from this work. Ilkka Helenius reports to be a consultant for Medtronic and that his institution has received fundings from Medtronic, Stryker, Nuvasive, Finnish Paediatric Research Foundation and Liv och Hälsa outside from this work. All the other co-authors have no disclosure to declare. All authors have completed the ICMJE uniform disclosure form.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Compliance with ethical standards
The authors declare that the study has not been funded by any grant.
Ethical approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.