
Abstract

Keywords
Dear Editor,
We read with interest the above publication by Merkl et al. 1 Merkl et al. 1 stated that all procedures had been performed “properly” by a pediatric trauma surgeon with at least 6 years of experience in pediatric trauma. A definition for “properly” was not provided, leaving it open if all fractures had been fixed in an anatomically reduced position without any postoperative re-displacement, that is, the anterior humeral line (AHL) going through the center of the capitellum, carrying angle being symmetric to the non-injured arm (normal Baumann’s angle) and no malrotation or if the authors had accepted certain degrees of malalignment. The authors’ 1 abstract does not mention the latter, so that the abstract conclusion that the limitation of elbow movement 1 year after surgery is usually insignificant, regardless of displacement, can therefore give the impression to those who do not read beyond the abstract, that the quality of the reduction and fixation does not matter. Merkl et al. 1 stated that they had evaluated the AHL and that they had compared Baumann’s angle of the injured elbow with the other limb, but did not provide any raw data, and malrotation was not assessed. The authors 1 did not document that the range of movement (ROM) had been measured with a goniometer and did not provide measured degrees of flexion and extension, which suggests that the Flynn criteria for ROM might have been extrapolated from descriptive medical record entries rather than having been based on more accurate and reliable angle measurements. McKay et al. 2 measured a mean elbow flexion of 146° and mean extension of 3° for normal children 3–9 years of age (total ROM of 149°). Rehm et al. 3 highlighted that multiple publications in the literature show that it cannot be assumed that all authors are familiar with the normal values for elbow movements in children, 2 with multiple authors 3 having falsely reported a total ROM of about 130° as good or excellent, despite it being a poor result according to the Flynn classification.
Merkl et al. 1 used the Gartland classification, which does not differentiate between undisplaced and displaced type-2 fractures. We think that it is more appropriate to use the modified Wilkins and Gartland classification, 4 which differentiates between angulated undisplaced type-2a fractures and displaced type-2b fractures with translation and/or malrotation, especially with 67% of the total cohort having been type-2 fractures.
In conclusion, we agree with Merkl et al. 1 that supracondylar humerus fractures should only be operated on by experienced surgeons who have specialized pediatric trauma training in a pediatric trauma center since we unfortunately regularly encounter fractures following inadequate management by surgeons who lack experience and skills (Figure 1). Merkl et al. 1 could have increased the plausibility of their article by providing raw measurement data. Malrotation is unfortunately often not identified as a deformity,1,5 for example, Sandbæk et al. 5 not having recognized that what they had described as a reduced fracture on a lateral radiograph has in fact a large rotational deformity with a Gordon lateral rotation percentage of about 30% which will affect function and cosmesis.
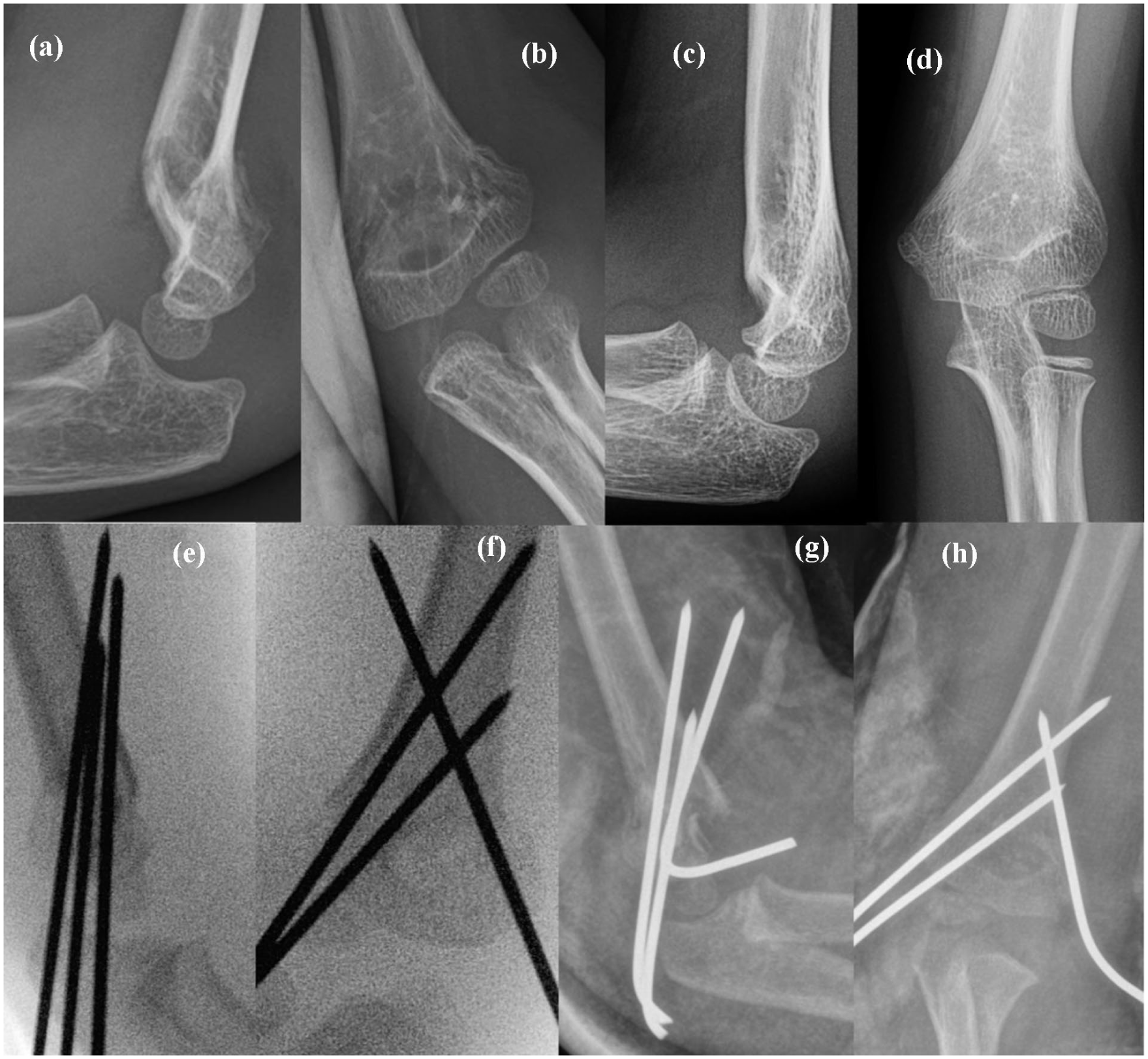
Case 1 (a–d): 4-year-old child with a Wilkins and Gartland type-2b fracture with the AHL missing the capitellum, where two non-POSs decided that the fracture did not need to be reduced (a, b). At 19-month follow-up (c, d), the child had poor elbow function with elbow hyperextension of 25° and elbow flexion of 110° compared to 10° and 145°, respectively, of the uninjured elbow. Case 2 (e–h): 6-year-old patient whose fracture was operated on by two non-POSs with intraoperative mal-reduction (e, f) and displacement within 3 days of the surgery (g, h). The fixation was revised by two POSs.
Footnotes
Author contributions
Andreas Rehm: contribution: literature review and article preparation. John E Lawrence: contribution: literature review and article preparation. Hatem Osman: contribution: literature review and article preparation. Rebecca J Worley: contribution: literature review and article preparation. Felix Morriss: contribution: literature review and article preparation. Ignatius Liew: contribution: literature review and article preparation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This article does not contain any studies with human participants or animals performed by any of the authors.
Licensing and copyright
The Journal of Children’s Orthopaedics publishes articles under a Creative Commons Attribution Non-Commercial license (CC-BY-NC) as standard, which allows others to re-use the work without permission so long as the work is properly referenced and the use is non-commercial.
Data availability statement
No new data were created or analyzed for this “Letter to the Editor.” Therefore, data sharing is not applicable to this article.