
Abstract
Introduction:
Clubfoot is a congenital birth defect affecting musculoskeletal tissues of the affected lower legs, resulting in the typical appearance and changes in muscle-tendon properties. These properties change during development due to growth and activity, but how these properties differ across ages in clubfoot remains not fully understood. This study aimed to describe plantarflexor muscle-tendon volumes between affected and unaffected legs in unilateral clubfoot patients and explore the relationship between muscle volume and age.
Methods:
A prospective cross-sectional study was performed on unilateral clubfoot patients treated with the Ponseti method. Muscle-tendon volumes of the medial and lateral gastrocnemius, soleus, and Achilles tendons in both affected and unaffected legs of clubfoot patients were assessed using ultrasound. Volumetric reconstructions were made using three-dimensional ultrasound (3DUS). Statistical analyses compared muscle-tendon volume between legs and their relationship with age.
Results:
A total of 25 clubfoot patients with good clinical status aged between 2.0 and 11.8 years were analyzed. Smaller plantarflexor muscle and greater Achilles tendon volumes were found in the affected leg compared to the unaffected leg. Furthermore, age was not significantly related to absolute muscle volume difference between the legs.
Discussion and Conclusions:
The findings of this study indicate that changes in muscle and tendon volume are present in treated clubfoot patients of multiple ages, enhancing understanding of their muscle-tendon morphology. The clinical significance of muscle-tendon alterations and their adaptation to targeted interventions remains to be established. Further research should investigate the relationship between muscle-tendon morphology and clinical status of (relapsed) clubfoot patients.
Introduction
Clubfoot, or congenital talipes equinovarus, is a lower extremity deformity, occurring in 1.18 per 1000 children worldwide. 1 A clubfoot is recognizable by its four main clinical components: cavus of the midfoot, adductus of the forefoot, varus of the hindfoot, and equinus. 2 These four components are accompanied by structural changes in the tarsal bones, ligaments, and muscles.3,4 The gold standard treatment in clubfoot care is the Ponseti method, which aims to improve deformities and provide a functional, plantigrade, pain-free foot with adequate mobility.2,5–7 This non-invasive treatment is often started in the first weeks after birth and involves foot manipulation and casting in all patients, and an Achilles tenotomy in most patients to correct the four main clinical components of the clubfoot.2,5,7 Afterwards, a bracing phase is started to maintain the corrected position. 2,5,7
Good correction rates have been reported in clubfoot patients treated with the Ponseti method.4,8–11 Patient satisfaction, pain, and clinical scores were excellent in the short- and long-term after treatment.4,8–11 Nevertheless, functional limitations such as diminished passive ankle mobility, altered ankle joint angles, and lower ankle plantarflexor moments during daily-life activities, such as walking, running, and hopping are reported after treatment.12–16
Even though multiple authors reported functional limitations in clubfoot patients, the origin of the functional limitations remains unclear. Alterations in the lower leg morphology, which are part of the clubfoot deformity might be relevant. These alterations potentially lead to plantarflexor weakness, 12 which could contribute to the functional limitations that previously have been reported in clubfoot patients.13,14 Various studies showed alterations in the lower leg morphology of the clubfoot when compared to a reference, which was either a lower leg of typically developing children17,18 or the unaffected lower leg of unilateral clubfoot patients.18–22 These alterations have been shown to be present before birth and both before and after treatment.3,15,20,21,23 Most frequently, changes in overall tissue composition have been described, where a lower overall muscle volume and higher adipose tissue volume were found in the affected leg.18,21 This lower overall muscle volume is reflected in the previously reported volume reduction of the soleus (44%) and gastrocnemius (27%). 24 Next to the reduction in muscle volume, a shorter medial gastrocnemius muscle belly, with shorter and more pennate muscle fibers, was found in the affected leg. 17 Additionally, multiple studies reported a longer and stiffer Achilles tendon.22,25,26 However, detailed muscle properties of the other plantarflexor muscles, such as the lateral gastrocnemius, have not yet been described in clubfoot patients. A better understanding of individual adaptations of these muscles may be relevant for fully understanding alterations in the plantarflexor complex. 17
Another area that remains uncharted is the change in muscle-tendon properties that occurs during the growth of these patients. Muscle-tendon properties change continuously during a child’s development. During aging in children, the plantarflexor muscles and Achilles tendon increase in volume, due to longitudinal and cross-sectional growth.27–29 In clubfoot patients, the deformity, accompanied by structural changes in lower leg anatomy, and growth might not be the only factors that have an impact on the muscle-tendon properties. In addition to growth, the Ponseti treatment might influence the muscle-tendon properties of clubfoot patients. From the literature, it is known that the Achilles tendon is longer after the tenotomy in clubfoot patients and that there is irregular tissue at the site of the tenotomy.25,26,30–32 Additionally, it is known that immobilization in typically developing adults leads to a decrease in plantarflexor cross-sectional area,33,34 which suggests that the immobilization during the casting and bracing phases of the Ponseti method potentially influences the plantarflexor morphology.
A better understanding of changes in muscle-tendon properties and insight into the occurrence of these changes throughout growth and treatment is necessary to develop additional interventions for optimizing muscle-tendon properties of clubfoot patients in the future. Therefore, this study aimed to determine the differences in plantarflexor muscle-tendon morphology between the affected and unaffected sides of unilateral clubfoot patients between 2 and 11 years old. Overall, we expect altered muscle-tendon morphology, such as a lower volume of the plantarflexor muscles, on the affected side compared to the unaffected side.18,21 A sub-aim of this study was to determine the relationship between the difference in muscle volume of the affected and unaffected side with age, initial clubfoot severity, and number of casts. We expect that older children show a larger difference in muscle volume between the affected and unaffected side, as leg muscle atrophy was found to increase with growth in clubfoot patients. 20
Methods
General
This prospective, cross-sectional study was performed at the Department of Orthopaedics at the Máxima Medical Centre (Veldhoven, the Netherlands). The study was approved by the Medical Ethical Committee of the Máxima MC (NL84721.015.23) and the local review board (W23.074).
Study population
Eligible clubfoot patients with an appointment at the outpatient clinic between January 2024 and July 2024 were consequently invited to participate. Patients were included when they: (1) had idiopathic clubfoot; (2) were unilaterally affected; (3) received initial treatment with the Ponseti method; (4) and were between 2 and 11 years old. Patients were excluded when they: (1) had underlying syndromes; (2) were bilaterally affected; (3) received initial treatment other than the Ponseti method; (4) previously underwent additional operative treatment for a relapse (with the exception of a re-Achilles tenotomy); (5) had a relapse, defined as the need for additional treatment, at the time of enrolment.
Data acquisition and analysis
Ultrasonography was used to investigate the muscle-tendon properties of the medial and lateral gastrocnemius, soleus, and Achilles tendon in the affected and unaffected side of the patients. The measures were performed with an ArtUs EXT-1H Rev.C2 (Telemed) ultrasound scanner and a L15-7H40-A5 (7.5–15 MHz) linear transducer. Ultrasound settings were kept constant for all acquisitions at a depth of 40 mm, focus of 14–21 mm, dynamic range of 54 dB, gain of 86% and frequency of 12 MHz. Patients were asked to lie still, in a prone position on the examination bench with their feet hanging off the table. Ankle angles were measured using a goniometer.
Two static longitudinal ultrasound images were made at the maximum thickness of the muscle belly of the medial gastrocnemius, lateral gastrocnemius, and soleus to determine muscle fiber lengths and pennation angles.35,36 To determine the muscle and tendon volumes, three-dimensional freehand ultrasound (3DfUS) was used. With 3DfUS, the position and orientation of the ultrasound transducer were captured using a motion-tracking camera system (V120: Trio, OptiTrack) and a fixed mount on the transducer with four retroreflective markers. The Stradwin software (v6.03, University of Cambridge, UK) was used and calibrated to combine ultrasound images and the positional data, to reconstruct a three-dimensional volume of the ultrasound images. 37 Three 3DfUS acquisitions were performed on each side; an additional acquisition was performed when the patient moved during one of the acquisitions.
After data acquisition, manual segmentation of the medial and lateral gastrocnemius, soleus and full Achilles tendon was performed at every other ultrasound image (see Figure 1). Estimates of muscle and tendon volumes were determined based on algorithms that were incorporated in the Stradwin software. 38 Muscle lengths were determined based on the distance between the proximal and distal landmarks in the Stradwin software. The Achilles tendon length was measured distally at the calcaneal insertion; proximally, the free tendon length was defined at the soleus musculotendinous junction, and the full length at the gastrocnemii junction. Anatomical cross-sectional area (aCSA) and thickness were determined for all three muscles and the tendon on the segmented image with the largest aCSA. The physiological cross-sectional area (pCSA) was determined for all three muscles using the following formula:

In this formula, V is the volume in cm3, Lf is the fascicle length in cm, and θp is the pennation angle in degrees.
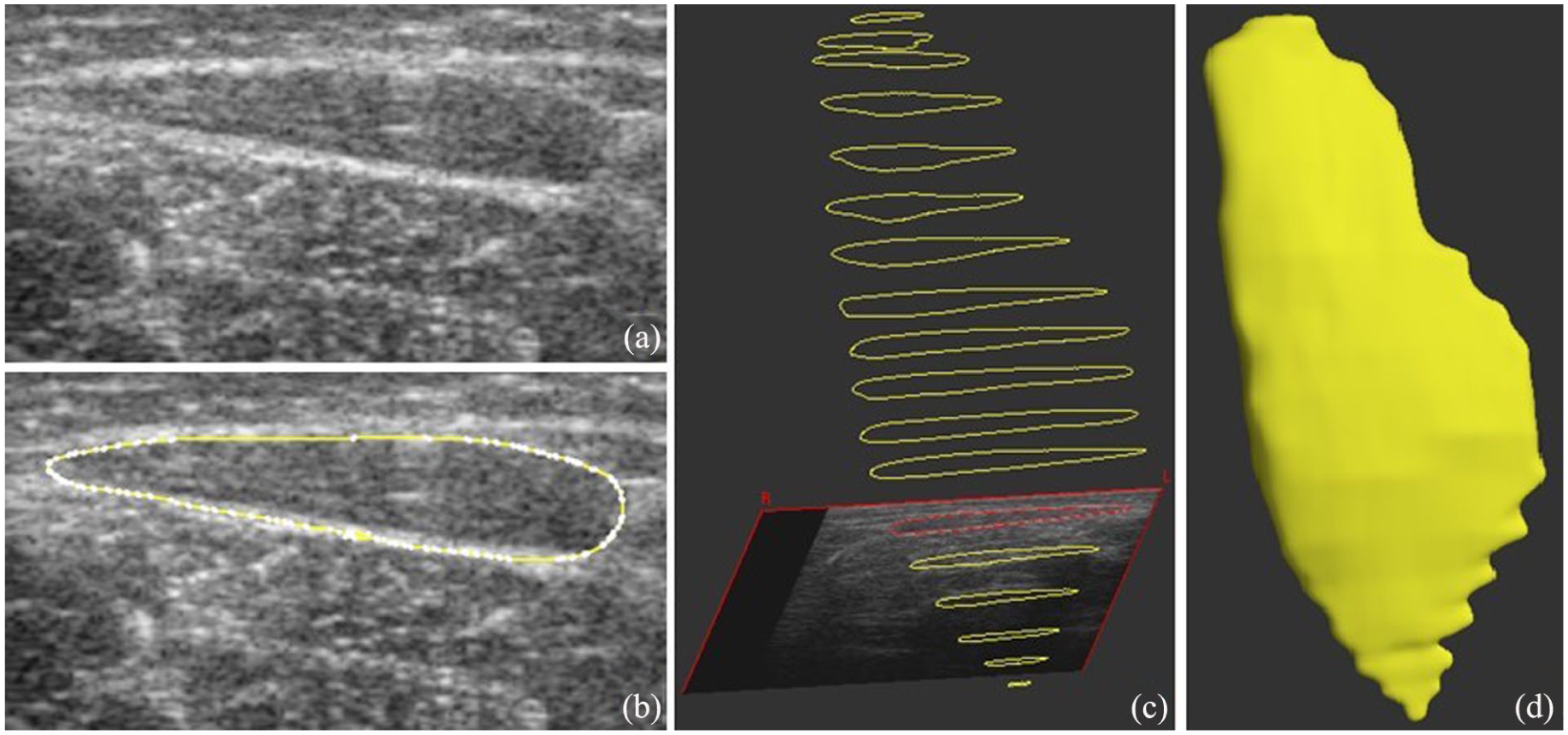
Example of the manual 3DfUS segmentation process: (a) static ultrasound image of the lateral gastrocnemius; (b) outlining of the cross-sectional area of the muscle (c) three-dimensional view of multiple outlines from the distal to the proximal landmark of the muscle; (d) three-dimensional volume reconstruction of the lateral gastrocnemius.
The clubfoot assessment protocol (CAP) was performed to determine the functional status of the affected side of the patient. 39 The CAP includes items that were omitted depending on the age of a patient. Therefore, the percentile CAP scores were calculated by dividing the total score obtained by the maximum age-specific score. 39 Furthermore, the clinical status at the time of the measurement and the treatment history of the patient were extracted from the patient records. In addition, the patient’s body height and weight were recorded. Leg length was measured from the medial knee joint space to the medial malleolus, and the maximum calf circumference was assessed.
Statistical analysis
Statistical analyses were performed using SPSS (IBM Statistics, v23). For all muscle-tendon parameters, ratios were calculated by dividing the value of the affected side by the value of the unaffected side. Absolute volume differences were calculated by subtracting the affected from the unaffected leg volume. Normality was checked using Shapiro–Wilk tests. Mean differences between the affected and unaffected sides were assessed using Wilcoxon signed-rank tests. To determine the relationships between age and volumes of the muscles and tendon, linear regression was performed. Spearman’s rank correlation was applied to assess the association between Pirani scores, number of casts, and muscle-tendon volumes. Significant relationships were interpreted as weak when below 0.2, as fair between 0.21 and 0.4, as moderate between 0.41 and 0.6, as good between 0.61 and 0.8 and as strong when higher than 0.8. 40 Results were considered statistically significant when p-values were below 0.05.
Results
Demographic study parameters
Overall, 25 patients agreed to participate in this study. Demographic characteristics of the patients are shown in Table 1. Patients showed good clubfoot status at the time of the measurement, indicated by the high follow-up CAP scores (Table 1) and no relapse at the time of inclusion. The calf circumference was significantly smaller in the affected leg (p < 0.001). The lower leg length and resting ankle angle at which the ultrasound measurement was performed did not significantly differ between the affected and unaffected leg (p > 0.05).
Demographic characteristics of the study population, presented as median (IQR).
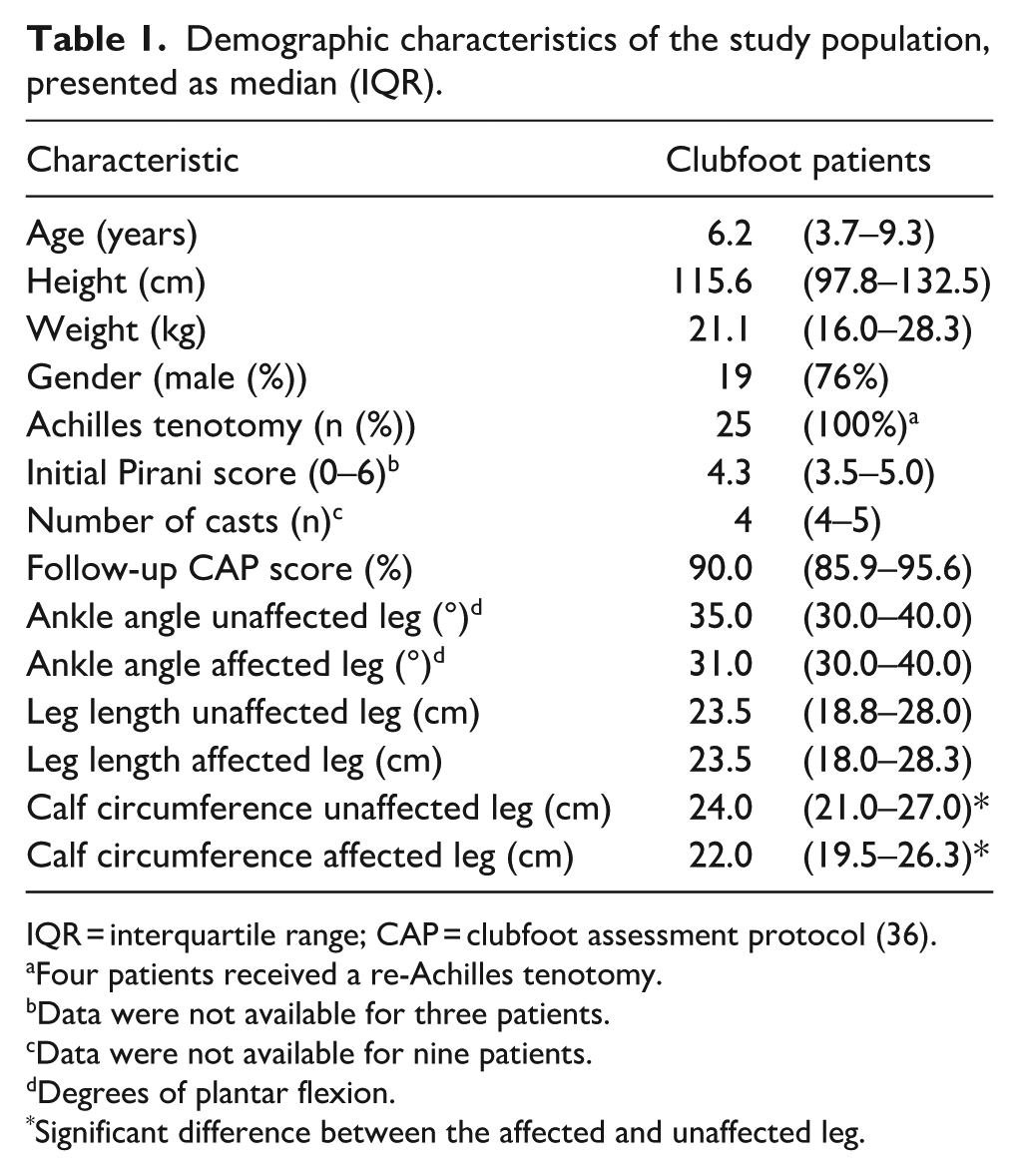
IQR = interquartile range; CAP = clubfoot assessment protocol (36).
Four patients received a re-Achilles tenotomy.
Data were not available for three patients.
Data were not available for nine patients.
Degrees of plantar flexion.
Significant difference between the affected and unaffected leg.
Differences in muscle and tendon volumes between the affected and unaffected sides
Significantly lower muscle volumes of the medial gastrocnemius, lateral gastrocnemius, and soleus were found, which was reflected in a lower total plantarflexor muscle volume of the affected leg when compared to the unaffected leg (Table 2). In contrast, Achilles tendon volume was significantly higher in the affected leg compared to the unaffected leg (Table 2).
Muscle and tendon volumes of the affected and unaffected leg, presented in median (IQR).
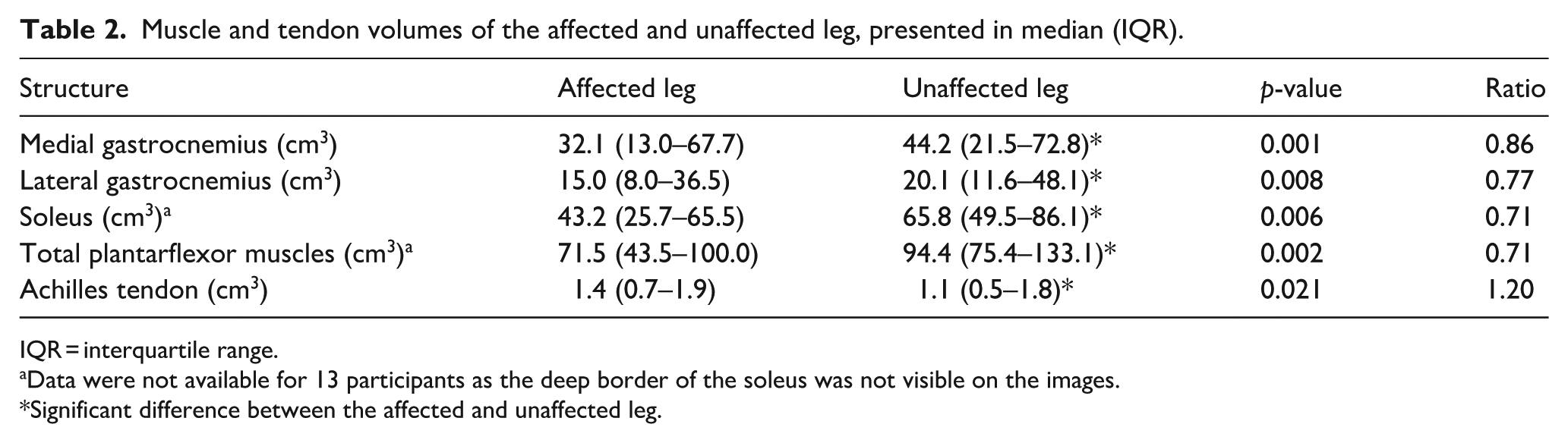
IQR = interquartile range.
Data were not available for 13 participants as the deep border of the soleus was not visible on the images.
Significant difference between the affected and unaffected leg.
Differences in muscle-tendon properties between the affected and unaffected sides
Shorter muscle bellies were found for the medial gastrocnemius, lateral gastrocnemius, and soleus (Table 3). Even though all three separate plantarflexor muscles showed significantly decreased muscle volume and muscle length on the affected side, not all muscle-tendon properties differed between the affected and unaffected leg (Table 3). The fascicle length of the medial and lateral gastrocnemius was significantly shorter in the affected leg compared to the unaffected leg. Furthermore, aCSA was significantly smaller in the lateral gastrocnemius and soleus in the affected leg when compared to the unaffected leg. Additionally, a significantly longer Achilles tendon length was found in the affected leg when compared to the unaffected leg.
Muscle-tendon properties of the affected and unaffected leg, presented in median (IQR).
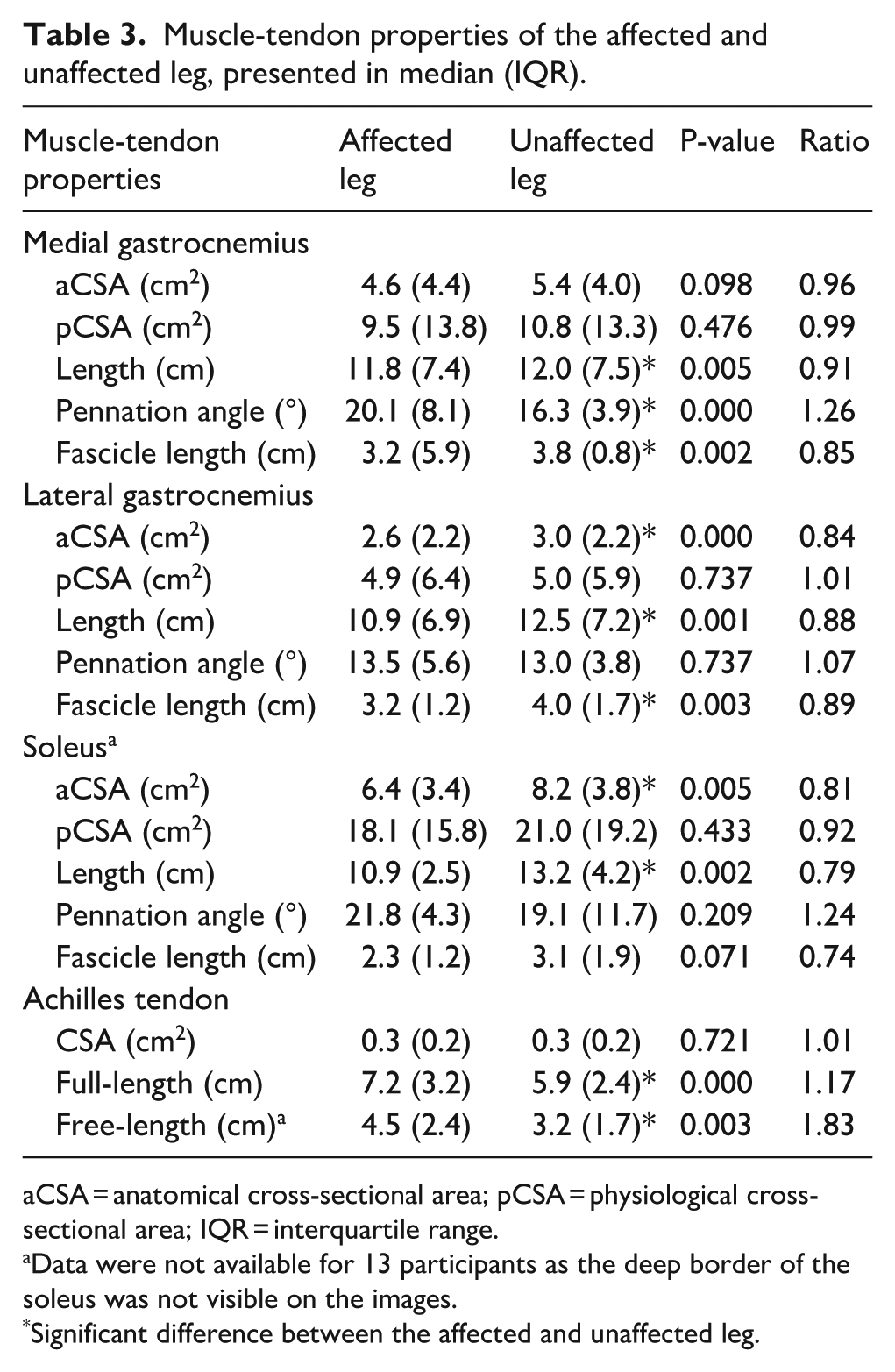
aCSA = anatomical cross-sectional area; pCSA = physiological cross-sectional area; IQR = interquartile range.
Data were not available for 13 participants as the deep border of the soleus was not visible on the images.
Significant difference between the affected and unaffected leg.
Relationships between muscle and tendon volume differences with age, Pirani scores, and number of casts
The absolute volume difference between the affected and unaffected leg was not significantly related to age for the medial gastrocnemius (p = 0.784), lateral gastrocnemius (p = 0.154), and Achilles tendon (p = 0.679) (Figure 2(a)). However, the muscle volume ratio was significantly related to age for the medial gastrocnemius (GM = 0.650 + 0.028*Age, p = 0.018) (Figure 2(b)).
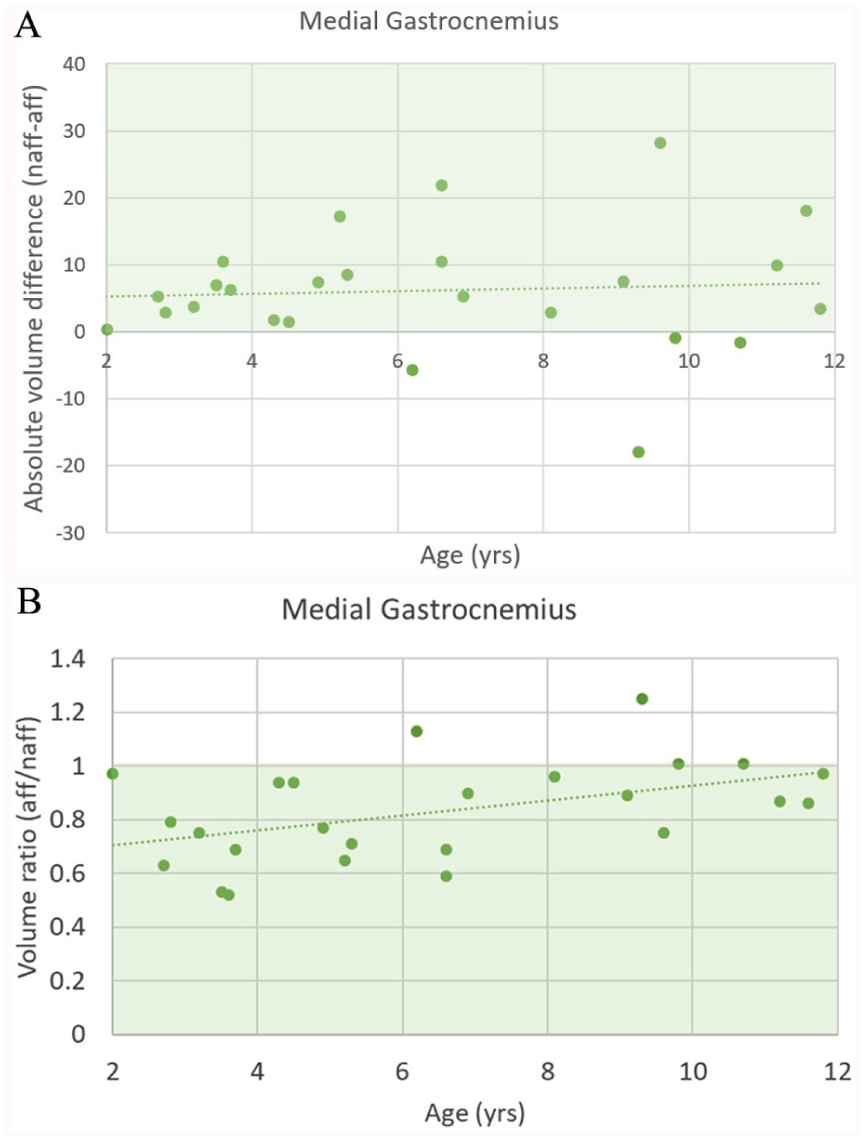
The relationship between age and (a) the absolute difference in medial gastrocnemius volume and (b) the medial gastrocnemius volume ratio between the affected and unaffected leg. Green area reflects lower volume in the affected compared to the unaffected side.
The absolute volume difference between the affected and unaffected leg was moderately associated with initial Pirani scores (n = 22) for the lateral gastrocnemius (rs = 0.44; p = 0.041, Figure 3(a)) but not significantly associated with the medial gastrocnemius (p = 0.070) and Achilles tendon (p = 0.184) or any of the muscle volume ratios (p > 0.05). However, the Achilles tendon ratio was moderately associated with initial Pirani scores (rs = 0.46; p = 0.031, Figure 3(b)). The number of casts (n = 16) during the Ponseti treatment was not significantly related to absolute and relative differences in muscle or tendon volumes (p > 0.05).
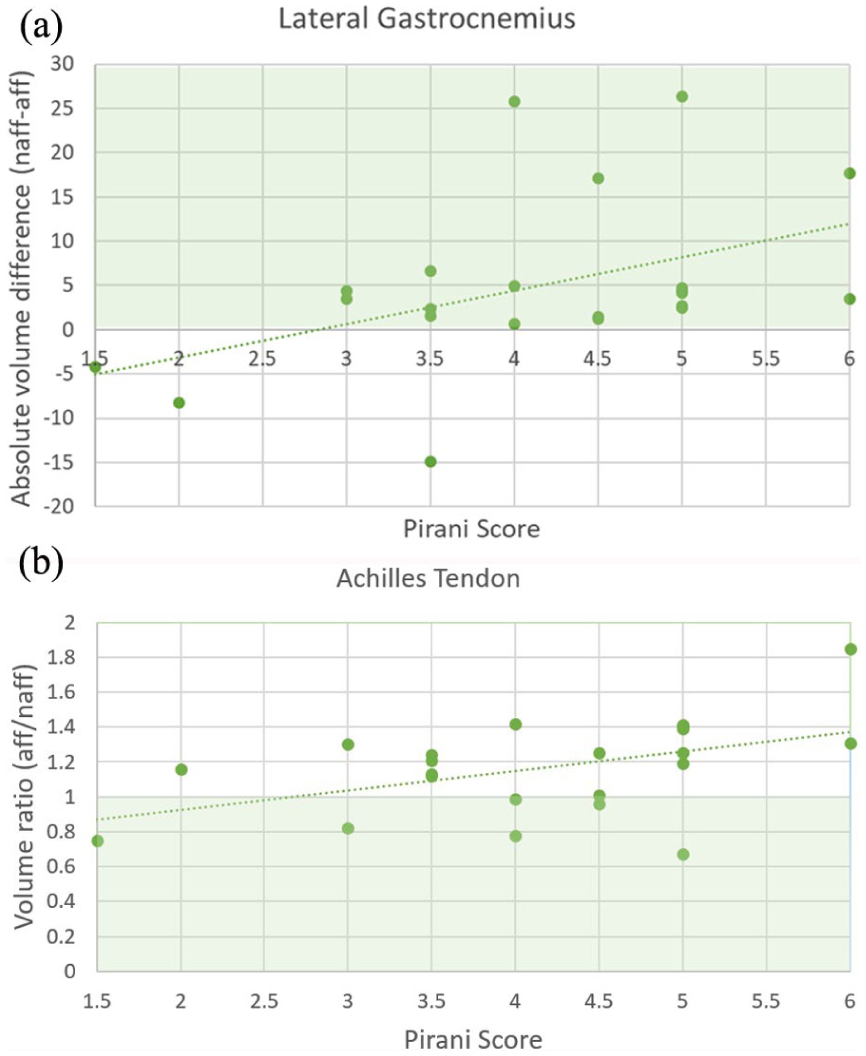
The relationship between Pirani scores and (a) the absolute difference in lateral gastrocnemius volume and (b) the Achilles tendon volume ratio between the affected and unaffected leg. Green area reflects lower volume in the affected compared to the unaffected side.
Discussion
This paper aimed to determine the differences in plantarflexor muscle-tendon morphology between the affected and unaffected sides of well-performing unilateral clubfoot patients between 2 and 11 years old, who were initially treated with the Ponseti method. In this study, all three plantarflexor muscles were smaller in volume and length on the affected side. Muscle architectural properties, such as fascicle length and pennation angle, differed for the three plantarflexor muscles. When examining the Achilles tendon, the tendon on the affected side was found to be larger in volume and length. The difference in volume between the affected and unaffected sides was found to remain consistent over the different ages. The initial severity, assessed using the Pirani score, was associated only with the absolute gastrocnemius volume difference and Achilles tendon volume ratio between the affected leg when compared to the unaffected leg.
Unilateral clubfoot patients between 2 and 11 years old showed a lower plantarflexor muscle volume on their affected side when compared to their unaffected side. This was expected, as previous MRI- and CT-based studies have reported reductions in both, overall lower leg muscle volume18–20,41 and posteromedial compartment muscle volume21,41 on the affected side of unilateral clubfoot patients. The current study showed that a decrease in all three plantarflexor muscles contributed to the lower overall plantarflexor muscle volume. Consistent with the decrease in medial and lateral gastrocnemius and soleus volume, a shorter muscle belly length was found for all three muscles. In the literature, shorter gastrocnemii and soleus lengths have been reported. 3 Previously reported hypotheses for a smaller muscle volume and muscle belly length included theories regarding asymmetrical early development of the lower limb muscles due to the regulatory factors inhibiting the muscle growth potential in clubfoot pathology18–21; and muscle atrophy as a consequence of clubfoot treatment.18,20,21
Even though all three plantarflexor muscles were smaller in length and volume on the affected side when compared to the unaffected side, changes in internal muscle properties between the affected and unaffected sides were different for the three muscles. The medial gastrocnemius of the affected side showed a larger pennation angle and shorter fascicle length compared to the muscle on the unaffected side. The pennation angle (20.1 ± 8.1°) and fascicle length (3.2 ± 5.9 cm) of the medial gastrocnemius on the affected side were comparable to previous results from an ultrasound study where the pennation angle (18.5 ± 3.1°) and fascicle length (3.5 ± 0.3 cm) of uni- and bilateral clubfoot patients were reported. 17 The pennation angle (16.3 ± 3.9°) and fascicle length (3.8 ± 0.8 cm) of the medial gastrocnemius on the unaffected side were significantly different from the affected side but also seemed to differ from previously reported parameters in typically developing children. 17 Suggesting that the unaffected leg of a clubfoot patient is not necessarily the same as the leg of a typically developing child. 18 An MRI study by Moon and colleagues reported a lower overall muscle area in the affected side, which could be linked to the smaller aCSA of the lateral gastrocnemius and soleus that were found in our study. 42 Even though there are differences in the intrinsic properties of the three plantarflexor muscles, the pCSA was similar for the affected and unaffected sides in all three muscles. This seems to imply that the intrinsic muscle properties adapt and compensate for the smaller and shorter muscle belly, thereby optimizing the force-generating capacity of the muscles.43,44 Besides, the study of Moon et al demonstrated larger differences between muscle area in treatment-resistant compared to treatment-responsive clubfoot and illustrated soft-tissue abnormalities between clubfoot patients with and without a relapse, such as muscle hypoplasia and increased intra- and intermuscular fat tissue. 42
In addition to the changes that were found in the plantarflexor muscles, the Achilles tendon exhibited a greater volume on the affected side, which is likely attributable to its significantly increased length, as no differences in CSA were found. This is in agreement with previous MRI- and ultrasound-based studies, which reported a longer Achilles tendon on the affected side of unilateral clubfoot patients.21,45 There is still a debate about the cause of the longer Achilles tendon. On the one side, the longer Achilles tendon was argued to be a consequence of the clubfoot pathology. Even in fetuses and new borns who did not receive treatment yet, longer Achilles tendons with shorter plantarflexor muscle bellies were found. 3 On the other side, it is argued that the longer Achilles tendon could be explained by the tenotomy that is often part of the Ponseti treatment. Clubfoot patients did show Achilles tendon elongation after receiving an Achilles tenotomy. 32 Even though no studies have investigated this yet, the tenotomy could partly explain the changes in the separate plantarflexor muscles as well. The tenotomy is thought to decrease the tension on the muscles, therefore, the muscle belly will retract, and muscle shortening can occur. 46
In contrast to the study of Ippolito and colleagues, 21 no relationship was found between age and the absolute difference in muscle volume of the gastrocnemii and Achilles tendon between the affected and unaffected side. Suggesting that the difference between the sides does not change over the years. Ippolito and colleagues included clubfoot patients between 4 and 6 months, 10 and 12 months, and 4 and 6 years old, where in the latter group a considerably larger difference of the postero-medial muscle compartment was present compared to the other groups. 21 The difference in age groups and ability to walk might be reason for the differences in results with our study. As total muscle volume further increases as the children grow, the relative difference decreases. This was reflected in the significant positively relation between the muscle volume ratio of the medial gastrocnemius and age found in this study.
Previous studies showed that in fetal and new born clubfoot patients already differences in muscle-tendon properties exist.20,23,47 In the current study, this young patient group was not included. However, initial Pirani scores indicate the severity of the clubfoot deformity. In the current study, higher initial Pirani scores were associated with a relatively smaller lateral gastrocnemius and Achilles tendon volume in the affected leg compared to the unaffected leg. The moderate associations observed between initial Pirani scores and both the absolute lateral gastrocnemius volume differences and the relative Achilles tendon volume difference suggest that the amount of alteration in muscle-tendon morphology might be related to the initial severity of the clubfoot. The total number of casts needed to achieve correction of the initial deformity during the Ponseti treatment has also been linked to severity of the clubfoot 48 but the casting is in respect to muscle-tendon properties also relevant in light of immobilization of the leg during the treatment. Immobilization with cast influences muscle morphology.30,31 In the current study, no association between number of casts and muscle-tendon properties was found. However, it must be noted that due to missing data, the available data were limited and with respect to the amount of immobilization also duration of bracing should be investigated.
The previously described changes between the affected and unaffected side provide a better understanding of the plantarflexor muscle-tendon morphology of unilateral clubfoot patients. As changes in morphology directly affect the functioning of the plantarflexor muscle-tendon unit, it is important to monitor changes in plantarflexor morphology as they might be a first indicator for a decline in functioning in clubfoot patients. The lower muscle volume might indicate a loss of force-generating capacity,43,44 and the smaller muscle belly length might lead to a smaller operating range of the muscles,43,44,49 both factors negatively impacting functioning. In addition to affecting function, a persistent retraction of the muscle-tendon complex is thought to be a contributing factor for the development of a relapse. 50 The 3DfUS performed in this study demonstrates that potentially relevant muscle-tendon properties can be obtained in an outpatient setting without the sedation or costs associated with comparative radiology (e.g. MRI), used in previous studies investigating muscle-tendon properties in clubfoot patients.18–21 A better understanding of muscle-tendon properties and their relationship to a patient’s clinical status is necessary to identify and optimize treatment of altered muscle-tendon properties in patients with a clubfoot in the future.
There are a few limitations to this study that still leave room for further research. In this study, the muscle-tendon properties of the plantarflexor muscles of the affected and unaffected side in clubfoot patients were described. However, in 13 of the 25 patients, the muscle volume of the soleus could not be measured. In this study, the ultrasound settings were kept the same for all patients, which meant that the deep border of the soleus was not always visible in the images, especially in the older and larger children. For a follow-up study, it would be recommended to personalize these ultrasound settings per patient, so that the entire soleus could be captured. Besides, this study was restricted to the triceps surae which, according to the literature, has been shown to be involved in clubfoot pathology. 3 However, other muscles and tendons of the lower leg, such as peroneal muscles, may also be affected, and their clinical significance remains to be determined. 3 Another limitation to this study was that only clinically good unilaterally affected clubfoot patients were measured. All patients had a clinical CAP score above 78%, and no patient had a relapse of clubfoot at the time of inclusion. It is, however, estimated that approximately 1 in 3 Ponseti-treated clubfoot patients will experience a relapse, although rates vary widely depending on the applied definition.51–54 Imbalance among muscles and ligaments in clubfoot patients may contribute to the occurrence of a relapse.55,56 As previously described, a study of Moon et al. reported multiple differences in muscle area between treatment-resistant and treatment-responsive clubfoot patients. 42 Therefore, for further research, it would be interesting to include patients with a relapse, to see if the differences in muscle-tendon properties between the affected and unaffected side become more prominent. Moreover, this study only included unilaterally affected clubfoot patients, while approximately 50% of all clubfoot patients is bilaterally affected.51,57,58 Muscle-tendon morphology is likely to be influenced by factors as age, sex and activity level, therefore, a direct comparison with bilaterally affected patients or healthy controls remains difficult.59–61 Also, in previous studies investigating muscle-tendon properties, the unaffected lower leg of unilateral clubfoot patients was used a control.18–25 Lastly, this study explored the relationships between the relative muscle volume differences and the age of clubfoot patients. However, this was a cross-sectional study. To get a better picture of how the muscle-tendon properties change with age, and whether the differences between the affected and unaffected sides increase or decrease, a longitudinal study would give even more insight.
In conclusion, the results from this study provide a first overview of the muscle-tendon morphology in the affected and unaffected sides of clubfoot patients, treated with the Ponseti method, determined with three-dimensional ultrasound. This study illustrated abnormalities in muscle-tendon morphology in clinically good scoring that clubfoot patients. We plan to conduct future studies exploring the relation between muscle-tendon morphology and clinical status of clubfoot patients, such as functional limitation and relapse.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251387519 – Supplemental material for Muscle-tendon properties assessed by three-dimensional ultrasound in clinically well-performing clubfoot patients treated with the Ponseti method
Supplemental material, sj-pdf-1-cho-10.1177_18632521251387519 for Muscle-tendon properties assessed by three-dimensional ultrasound in clinically well-performing clubfoot patients treated with the Ponseti method by Quinten M. P. Vervaart, Saskia D. N. Wijnands, Arnold T. Besselaar, Benedicte Vanwanseele and Maria C. van der Steen in Journal of Children's Orthopaedics
Footnotes
Ethical considerations
Ethical Commission: Medical Ethical Committee of the Máxima Medical Centre. Ethical board committee approval number: NL84721.015.23. Parent(s) or legal representative(s) of all patients gave written informed consent prior to data collection.
Author contributions
Quinten M.P. Vervaart: Methodology; Data Collection; Data Analysis; Interpretation of results; Writing – Original Draft; Writing – Editing. Saskia D. N. Wijnands: Conceptualization; Methodology; Data Analysis; Interpretation of results; Writing – Original Draft; Writing – Review; Writing – Editing; Funding Acquisition. Arnold T. Besselaar: Data Collection; Interpretation of results; Writing – Review. Benedicte Vanwanseele: Methodology; Interpretation of results; Writing – Review; Supervision; Funding Acquisition. Maria C van der Steen: Conceptualization; Methodology; Interpretation of results; Writing – Review.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the Commission of Research and Innovation of the Máxima Medical Centre, the Netherlands; grant no. 2021.coi.015
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, Q.M.P. Vervaart, upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.