
Abstract
Purpose:
To describe the curve patterns and behaviors, clinical presentation, treatment modalities, and complications for adolescents with both scoliosis and autism spectrum disorders, but no additional concomitant diagnoses.
Methods:
A single-center, retrospective review of adolescents with scoliosis and autism spectrum disorder treated between 2001 and 2021. Patient demographics, clinical characteristics, and radiographic assessments were described across the scoliosis treatment plans (i.e. observation, bracing, and surgery).
Results:
Forty patients with scoliosis and autism spectrum disorder (80% male, mean age at 13.2 ± 1.7) met eligibility criteria. Twenty-one patients were managed with observation initially. Of these patients, 55% (n = 11) didn’t require further treatment and had an average change in curvature of 5° ± 6°. Twenty-one total patients were managed with bracing. In this group, 76% (n = 16) did not receive further treatments and had an average increase in curvature of 15° ± 11°. Five patients (24%) proceeded to surgery following brace treatment. Thirteen patients (33%) in total required surgery, with n = 5 requiring surgery as their initial treatment. The initial curve magnitude for this group was 55° ± 7° and had an average correction of 47% following posterior spinal fusion.
Conclusions:
Although curves in adolescents with scoliosis and autism spectrum disorder had a similar presentation to adolescents with just scoliosis, the current cohort did have an increase in curve progression when managed with bracing, with an unclear explanation. Further study is warranted in this unique population, and families should be counseled that the prognosis may not be the same as adolescents with scoliosis alone.
Levels of evidence:
Level IV.
Introduction
Adolescent idiopathic scoliosis (AIS) is a lateral curvature of the spine >10° with no known explanation in children over 10 years old.1,2 AIS is common, with a prevalence of 0.5%–5.2% and accounts for 90% of cases of idiopathic scoliosis in children. 2 Mild curves are seen in boys and girls equally; however, boys are less likely to present with severe curves (≥40°) compared to girls. 3 Despite being common, the etiology and pathogenesis of AIS are not well understood. The management of AIS is multifactorial but dependent on curve morphology, signs of progression, and skeletal maturity. 4
Treatment goals are to prevent curve progression, correct deformities, and avoid short-and long-term complications.4,5 Depending on clinical and radiographic presentation, these goals can be achieved with non-operative management (e.g. observation, bracing, and physical therapy) or surgery.5,6 However, the presentation and management may be more complex for adolescent patients with scoliosis and a co-diagnosis of autism spectrum disorders (ASD) with no other concomitant diagnoses (e.g. Rett syndrome), and there is limited evidence to guide care. 7
ASD is a group of common neurodevelopmental disorders that can present with mild to severe communication deficits, social disengagement, and repetitive behaviors. 8 The prevalence of ASD is rising due to earlier detection and is currently in the range of 0.9%–1.5%. 9 A recent publication found that patients with ASD and scoliosis presented with less lumbar lordosis preoperatively and had a higher percent correction at 2-year follow-up following spinal fusion compared to patients with AIS. 10 However, to our knowledge, no publications have described the outcomes of conservative scoliosis treatments for these patients or treatment pathways for adolescent patients with scoliosis and ASD. 7
In the current study, we describe the clinical presentation, treatment modalities, and complications for a series of patients with concurrent diagnosis of both scoliosis and ASD and no additional concomitant diagnoses. This case series provides insights into how a co-diagnosis of ASD may affect curve behavior in those with scoliosis and how these patients respond to scoliosis treatment. We hypothesize that the described patterns of scoliosis curves in patients with ASD behave and respond to treatments differently (e.g. larger curves at presentation, less responsive to bracing, higher rates of surgical intervention) compared to patients with strictly scoliosis. Results from this study will help determine if these patients with ASD and no additional concomitant diagnoses should be managed or counseled differently from patients with AIS.
Methods
Study design
This retrospective case series examined electronic medical records from a single specialty care center to identify patients with scoliosis and a diagnosis of autism, but no additional concomitant diagnoses. It was reviewed and determined to be exempt by an Institutional Review Board.
Patient identification and eligibility criteria
Patients who had appointments with spine providers between January, 2001 and May, 2021 were identified. Duplicate patients and non-spine-related appointments were removed from the list, as were patients who have opted out of having their medical records retrospectively reviewed.
Charts for the resulting list of patients were reviewed for eligibility. Eligibility criteria included: (1) age between 10 and 17 years, (2) diagnosis of ASD, (3) no diagnoses associated with neuromuscular, syndromic, or congenital scoliosis (e.g. chromosomal abnormalities, neuromuscular diseases, congenital spine deformities), (3) documentation of scoliosis, defined as a coronal spinal curve >10°, and (4) >2 years of follow-up. Patients were identified as having a diagnosis of ASD if it was on the diagnosis list in the medical record. Diagnosis of ASD was recorded in the medical record by one of the treating physicians at our institution, either by patient report in intake, through chart notes sent over by outside providers, or through diagnosis by a psychologist at our institution. Not all patients were diagnosed at our institution. Patients were excluded if they had not reached skeletal maturity by their final follow-up (i.e. >Risser stage 4, >Sanders stage 7, proximal humerus ossification stage 5, or > 2 years postmenarchal). Patients who received an MRI were excluded if they had signs of neural axis abnormalities.
Data extraction
Data collected from the chart included age at identification of scoliosis and final follow-up, scoliosis treatments (i.e. observation, orthotic, and/or operative treatments), complications, and coronal radiographic measurements. A physician assistant who specializes in pediatric spine deformity reviewed coronal radiographs across scoliosis treatments, including initial, pre-bracing (if applicable), first in-brace (3–4 months after receiving their brace), and final (or presurgery for those who required surgical scoliosis correction) radiographs. Radiographs reviewed depended on the series of treatments that each patient received across their care. Radiographs were reviewed for curve magnitude, location, and direction of the major and minor curves.
At our institution, adolescents with scoliosis and ASD and no additional concomitant diagnoses were treated with the same care pathway as those with AIS: observation was recommended for patients with curve magnitudes <25°, bracing (18–20 h/day) was recommended for patients with curves between 25° and 50°, and surgery was recommended for patients with curves >50°. Failure of observation was defined as progression to a curve >25° prior to skeletal maturity and resulted in transition to scoliosis bracing; progression in bracing was defined as >5° increase in curve magnitude prior to skeletal maturity; failure of bracing was defined as surgery or progression to >50°. Initial sagittal radiographs were reviewed to identify patients with thoracic hyper-kyphosis (>50°), thoracic hypo-kyphosis (<10°), lumbar hyper-lordosis (>75°), and lumbar hypo-lordosis (<15°).
All patient data were recorded in a Research Electronic Data Capture11,12 database. Two investigators tested the database with a subset of patients to assess database design and functionality, and training was provided for all members of the data collection team.
Analysis
Descriptive statistics were calculated for patient characteristics, including demographic, radiographic, and clinical data. Frequencies and percentages were calculated for patients who received each treatment type (e.g. observation only, bracing, and surgery) and treatment pathway (e.g. transition from observation to bracing, transition from bracing to surgery).
Results
Participants
Forty patients with co-diagnoses of scoliosis and ASD were eligible (Figure 1). The average age was 13.2 ± 1.7 years and most (n = 32, 80%) were male. Based on clinical documentation, most were able to use verbal or nonverbal communication with their providers (n = 31, 78%), and about one-third (38%) were noted to have cognitive delay. Self-injurious tendencies (n = 2, 5%) and sensory sensitivity (n = 2, 5%) were infrequently noted in clinical documentation (Table 1).
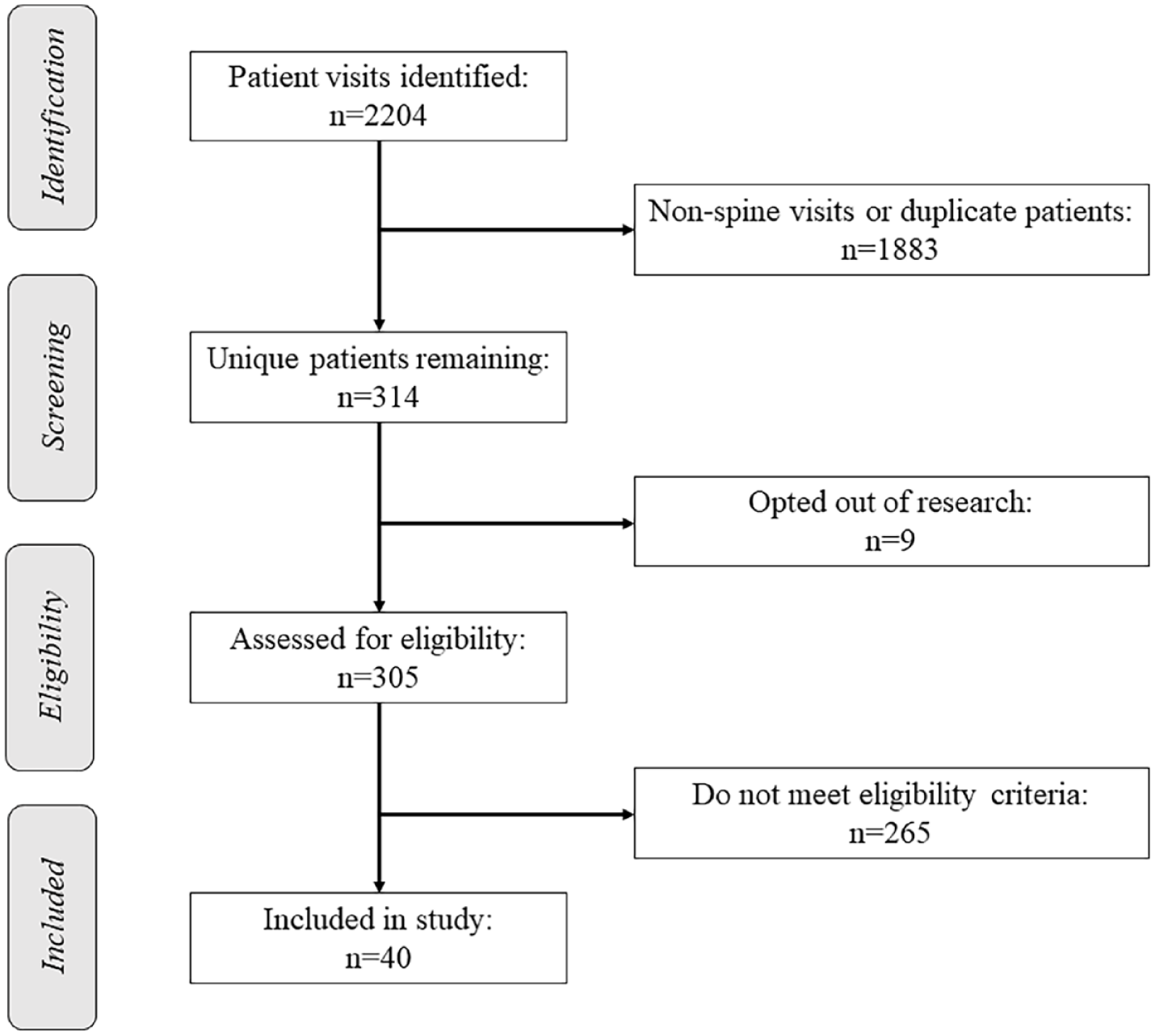
Flowchart illustrating the number of patients identified, screened, eligible, and included in the study.
Demographics for patients in all groups based on plan at initial presentation.
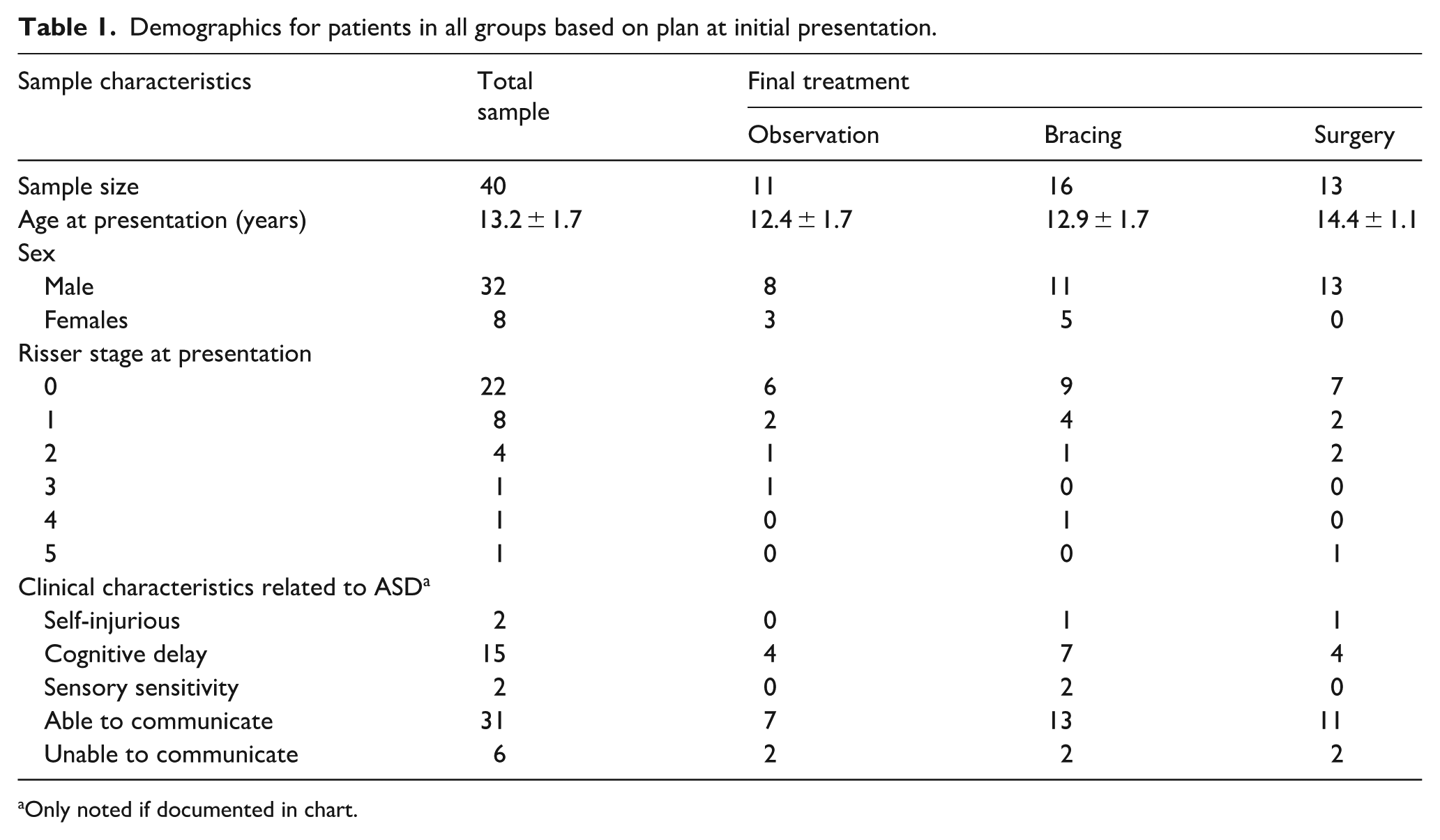
Only noted if documented in chart.
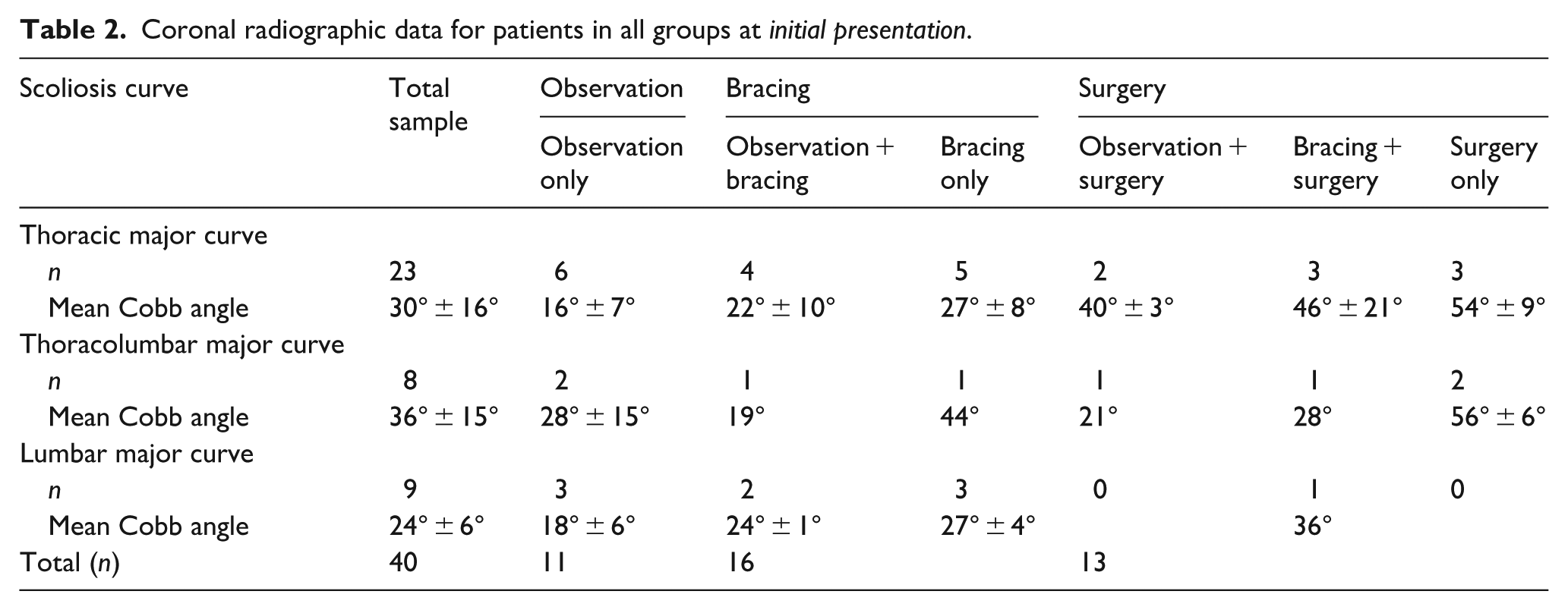
Patients presented with an average major coronal curve magnitude of 30 ± 15°, with most patients presenting with a major curve in the thoracic region (n = 23, 58%, Table 2). Of patients with sagittal radiographs that were clear enough to measure, 52% had hypokyphosis, 22% had hyperkyphosis, and 26% had kyphosis within normal ranges. For lordosis, 40% had hypolordosis, 15% had hyperlordosis, and 45% had lordosis within normal ranges.
Coronal radiographic data for patients in all groups at initial presentation.
Scoliosis treatments and outcomes
Observation
Twenty-one patients were initially managed with observation. The initial major curve magnitude for this group was 22° ± 10°. Of these patients, 52% (n = 11) didn’t require further treatment and had an average change in curvature of 5° ± 6° (Figure 2(a)). Six patients in the observation group had initial curves over 25°; two continued with observation and did not have surgery, two later underwent bracing, and two later had surgery. For the two that continued with observation, both families decided against bracing, preferring to wait to see if the curve progressed. One of these observation-only patients had an initial curve of 26° which increased to 47° by the end of observation, and was one of two that was noted to be unable to communicate their needs. This patient was asked to return for a follow-up and treatment plan after their initial visit, but ultimately did not return until they were no longer a good candidate for bracing. For the two that started with observation and eventually moved to bracing, both families decided against bracing at the initial visit, one due to concerns with sensory sensitivity. For the two that started with observation and moved to surgery, both families decided against bracing at the initial visit, one because they did not want to use a Cervical-Thoracolumbosarcal Orthosis (CTLSO) to treat the patient’s high thoracic curve, and the other because of behavioral concerns.
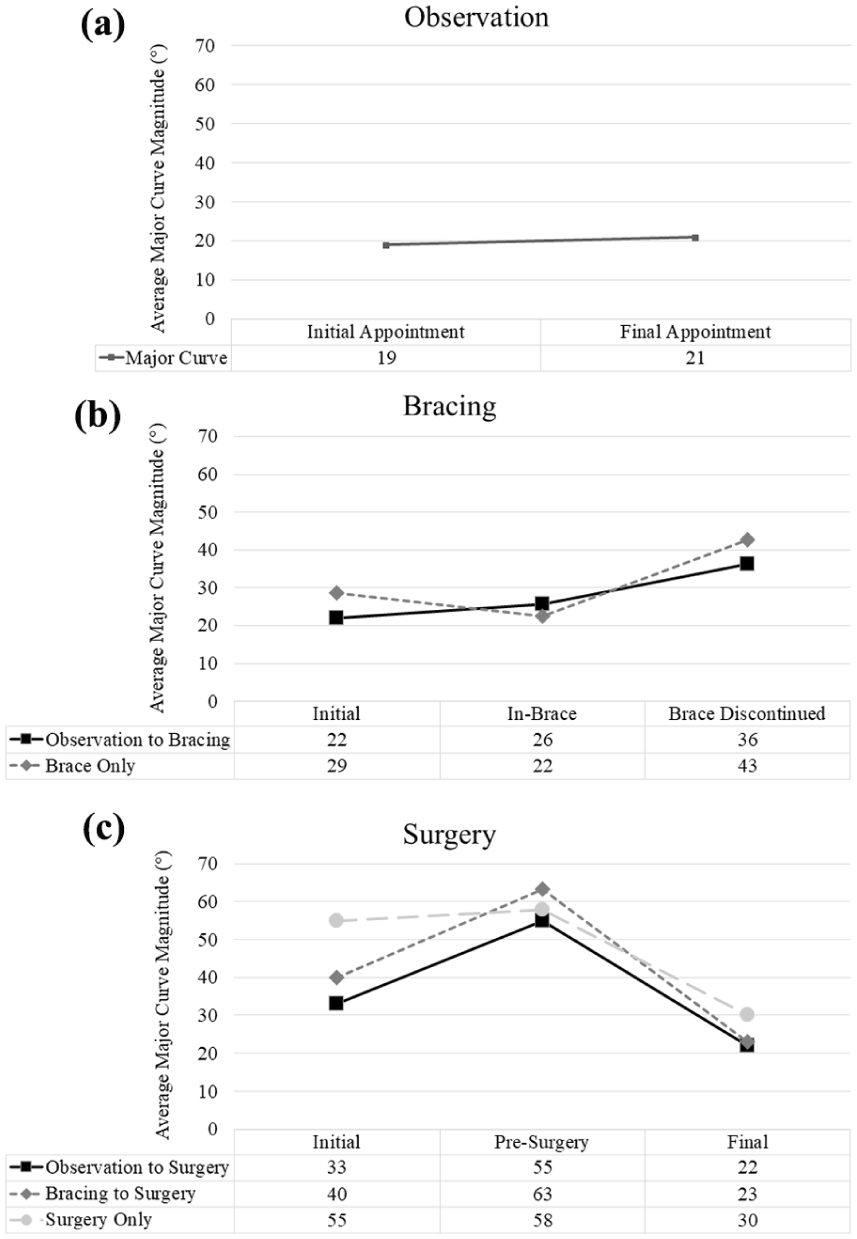
Curve magnitude for patients with scoliosis and ASD who received different treatments: (a) observation, (b) bracing, and (c) surgery.
Seven patients (33%) transitioned to bracing, and three (14%) proceeded to surgery due to substantial curve progression in the observation period. In the observation to bracing cohort, the average increase in curve magnitude from the initial appointment to pre-bracing was 12° ± 7° with a mean pre-bracing curve magnitude of 33° ± 7° and by the final appointment, there was an average change of 14° (Figure 2(b)). In those that proceeded with surgery, the curve magnitude increased an average of 21° ± 12° from the initial appointment to the presurgery appointment, with a mean presurgical curve magnitude of 55° ± 6° (Figure 2(c)).
Bracing
Twenty-one total patients were managed with bracing. The initial major curve magnitude for this entire group was 29° ± 12°. Of these patients, 76% (n = 16) didn’t require further treatments and had an average change in curvature of 14° ± 12° with initial curves presenting at 26° on average and 40° by the final appointment (Figure 2(b)). Bracing was generally tolerated well by most patients, with patients reporting full (18+ h) or partial (12–18 h) wear time. However, two patients were intolerant to bracing and experienced curve progression to >50°. One of these patients progressed to surgery, and the other was ineligible for operative management due to self-injurious behaviors. This patient had no expressive language and was not adherent with bracing due to inability to tolerate it, so their curve progressed from 22° to 69° by the final appointment.
Five total patients (24%) proceeded to surgery following brace treatment. In this cohort, curve magnitudes increased an average of 23° ± 9° from the initial appointment to the presurgery appointment, with a mean presurgical curve magnitude of 63° ± 10° (Figure 2(c)).
Surgery
Of the whole cohort, 33% (n = 13) required surgery (Table 2) and had an average correction rate of 56%. Of those, 38% (n = 5) proceeded with surgery as their initial treatment. Initial major curve magnitude for this group was 55° ± 7° and postoperative major curve magnitude was 30° ± 13° (average correction rate 47%; Figure 2(c)). One patient was kept sedated in the intensive care unit for 9 days due to self-injurious and aggressive behavior and was braced upon discontinuation of the sedation. For this patient, there were no post-op complications noted by the 2-year follow-up.
There was one complication that required revision surgery for partial removal of instrumentation and reimplantation. Another patient developed distal junctional kyphosis and had to undergo extension of posterior instrumented spinal fusion and revision of rods.
Discussion
The prevalence of ASD continues to increase as screening and awareness of common characteristics continue to improve. 13 As a result, there will be an increase in patients with ASD who also have a concurrent diagnosis of scoliosis with no additional underlying neuromuscular, syndromic, or congenital pathologies. The association between scoliosis and ASD remains unclear, with little evidence to inform spinal curvature presentation in this group and response to treatment. Thus, the goal of the study was to demonstrate how curves present in adolescents with scoliosis and ASD respond differently to observation, bracing, and surgery treatments compared to reports of patients with AIS in the literature.
The current cohort presented with clinical characteristics that differ from those with AIS. For instance, 80% of the patients were male, and of those patients who required surgery initially, all were male. Historically, it has been found that girls have a 2.4 times higher AIS prevalence rate, and the female-to-male ratio is up to 7.2:1 in curves >40°.2,14 However, the male-to-female ratio for a diagnosis of ASD is roughly 4.3:1, 15 which explains the presence of more males in our cohort. With regards to severe curves presenting at the initial visit and curve progression, the decreased bone mineral density seen in male patients with ASD and scoliosis16–18 may affect curve behavior and make them progress quicker compared to male patients with AIS, which is something to keep in mind when choosing the best treatment modality.
With conservative management, 55% of the current cohort had success with observation only. This proportion is similar to prior literature in AIS, where the average observation success rate was 45% for patients with AIS.19–21 For those managed with bracing, the success rate was 76% which is similar to bracing success rates in prior studies (~74%).22–24 Conversely, the average curve magnitude increased from the initial to final appointment by about 14° for patients with ASD treated with bracing (Figure 2(b)), which differs from patients with AIS, where the average reduction or increase was between 1° and 8°.22,25–29 In-brace correction and adherence to prescribed time in brace may be factors that contribute to this finding, though it could not be assessed as sensors were not used for all patients included in the retrospective study. Furthermore, brace compliance may have been affected by the sensory component observed in patients with ASD. In the current study, only two patients in the brace group were documented to have mild sensory disturbances, though it is possible that these symptoms were not assessed and/or documented for others. Since sensory processing has been associated with being the single strongest predictor for adverse behaviors in patients with ASD, it should be evaluated prior to bracing, as this could lead to anxiety and self-injurious behaviors. 30
Besides sensory responsivity, cognitive delays are also a manifestation seen in patients with ASD, where the prevalence of mild to moderate intellectual impairments ranges between 20% and 60% in current literature.31–33 Historically, social communication and interactions are components used as markers to evaluate cognitive function.34,35 In the current study, 38% of patients presented with cognitive impairments, and 22.5% could not communicate their needs with their providers. Although there weren’t significant findings in those who could communicate versus those who could not, the communication barrier between the patient and provider could have resulted in avoidable adverse events. Hence, it’s important to know that children with ASD may have different methods of communicating their needs, whether it is through verbal language, gestures, electronic devices, or picture exchange communication systems. 36 Understanding the different means of communication and behaviors commonly seen in patients with ASD will allow orthopedic surgeons to manage scoliosis more efficiently and enable good nonsurgical and surgical outcomes.
Those patients who did not have success with observation or bracing, or those who initially presented with severe curves, proceeded with spinal fusion. At the final postoperative appointment, there was an overall mean correction rate of 56% which is consistent with patients with AIS, where the mean correction rate ranges from 58.5% to 64.1%.37,38 Whereas Orland et al. found a 66% correction rate at 2-year follow-up in patients with scoliosis and ASD and a 57% correction rate in patients with AIS, which was attributed to differences in curve stiffness. 10 Patients with ASD have been associated with increased ligamentous laxity and hypermobility spectrum disorders in prior studies, which could contribute to changes in correction rate over time.39–42 However, with the current findings, it’s unclear whether there is a difference, so larger studies are required to determine relationships between ASD and scoliosis not associated with additional neuromuscular, syndromic, or congenital diagnoses.
Limitations
Although this is the largest case series to date, it has a relatively small sample size with patients from a single center, which may limit the generalizability of these findings. Also, due to the retrospective nature of the study, the research team relied on clinic notes to gather clinical characteristics, and they may not have been complete. Another limitation is that brace adherence and wear time were not assessed, which could have altered curve progression in those managed with bracing. Lastly, evaluation and treatment were at the discretion of the treating provider, and some bias may exist.
Conclusion
Overall, the curves seen in adolescents with scoliosis and ASD were similar to patients with a sole diagnosis of AIS. However, patients with scoliosis and ASD did have an increase in curve progression when managed with bracing. It remains unclear whether it was due to the additional diagnosis of ASD or brace adherence and tolerance of brace correction. It is important to note that special considerations must be undertaken to address communication deficits, sensory challenges, and common behaviors seen in patients with ASD, whether it is adding additional ancillary services or postoperative precautions. Certainly, higher-level studies are needed to elucidate the relationship between scoliosis and ASD and help determine the best course of management for this specific population.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251379277 – Supplemental material for Scoliosis in adolescents with autism spectrum disorder: A retrospective case series
Supplemental material, sj-pdf-1-cho-10.1177_18632521251379277 for Scoliosis in adolescents with autism spectrum disorder: A retrospective case series by Luis Torres-Gonzalez, Sara J Morgan, Walter H Truong, Casey Palmer, Cyrus Nouraee and Danielle C Harding in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
The authors would like to acknowledge Zelphia Brown and Michaela Reardon for assisting with this study.
Author’s Note
Cyrus Nouraee is now affiliated to Department of Internal Medicine, Mayo Clinic, Rochester, MN, USA.
Author contributions
All authors have read and approved this submission. Authorship contributions are as follows: Luis Torres-Gonzalez: data collection, writing/original draft preparation. Sara J Morgan: study design, interpretation of data, article revision, and approval. Walter H Truong: study design, interpretation of data, article revision, and approval. Casey Palmer: data collection, article revision, and approval. Cyrus Nouraee: data collection, article revision, and approval. Danielle C Harding: study conception and design, interpretation of data, article revision, and approval.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this project was provided by the Gillette Children’s Spine Fund.
Ethical considerations
This study was reviewed and determined exempt by a University of Minnesota Institutional Review Board (STUDY00011698). Informed consent was not required for this retrospective chart review.
Clinical trials registration
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.