
Abstract
Purpose:
Osteogenesis imperfecta is a rare disorder characterized by bone fragility. The current gold standard treatment for long bone fractures and deformities is telescopic intramedullary rods. Although the use of plates as a standalone implant has been discouraged, recent research has investigated their use as an adjunct to intramedullary fixation. This scoping review aims to assess the current literature on plates for the treatment of long bone metaphyseal and diaphyseal fractures and deformities in osteogenesis imperfecta.
Methods:
The MEDLINE, Embase, CENTRAL, and CDSR databases were searched via PubMed, Ovid, and Cochrane. Titles and abstracts of studies were screened, followed by full assessment of selected articles. Studies included were peer-reviewed, published in English in the last 20 years, and investigated plating alone or combined with other implants for the treatment of metaphyseal or diaphyseal long bone fractures and deformities in osteogenesis imperfecta.
Results:
Eleven articles were included: four investigated plating alone, two compared different implants, and five assessed plating as an adjunct to intramedullary fixation.
Conclusions:
Using plates alone is not recommended due to the high rate of complications, implant-related complications, and revision surgeries. However, they can be used when deemed appropriate by the surgeon or in narrow canals. Overall, the use of plates as an adjunct to intramedullary nails shows promising results, although further research is required to determine the indications for additional plating and the best timing of plate removal.
Level of evidence:
Level III (scoping review).
Keywords
Introduction
Osteogenesis imperfecta (OI) is a rare connective tissue disorder of genetic etiology that affects collagen, most commonly involving pathogenic variants of the genes that encode type-I collagen. 1 It is characterized by bone fragility and increased susceptibility to bone fractures and limb deformity. 2 The spectrum of the disease is variable, from milder cases to severe forms that are not compatible with life.
The current mainstay of surgical treatment for long bone fractures and deformities in OI is intramedullary (IM) rodding, with telescopic rods showing the lowest revision rate and longest survival period at the present time.3,4 Although plates as a standalone implant have been discouraged since stress fractures can occur above or below the plate, recent studies have investigated plates when used as an adjunct to IM rods.3,5 –7 As such, our team reviewed the use of plates in the surgical treatment of long bone fracture and deformity in OI.
Methods
This scoping review was guided by the methodology framework described by Mak and Thomas for scoping reviews which comprises the following elements: (1) identifying the research question, (2) identifying relevant studies, (3) selecting studies to be included in the review, (4) charting the data, (5) colleting, summarizing, and reporting the results. 8
The MEDLINE, Embase, CENTRAL, and CDSR databases were searched via PubMed, Ovid, and Cochrane, respectively. Articles that were included in this study were peer-reviewed, published in English in the last 20 years, and investigated plating alone or in combination with other implants as the surgical treatment of long bone metaphyseal or diaphyseal fractures and deformities in OI regardless of age. Case reports were included in this review due to the rarity of OI, the usually small sample size of larger studies, and because they can capture surgical techniques, outcomes, and challenges not well represented in broader research. Articles were excluded if they did not investigate the use of plates in OI for the treatment of fracture and deformity in long bone metaphysis or diaphysis, if they were published more than 20 years ago, if the full text was unavailable, or if the full text was published in a language other than English. The main author (YL) screened titles and abstracts of the search results, followed by a full assessment of selected articles. In total, 580 references were found. The details for the number of articles found and the final selection are summarized in the PRISMA diagram (Figure 1). 9 Finally, 11 articles were included in this scoping review. Of those, 4 investigated the use of plates alone, 2 compared different types of implants including plates, and 5 assessed the use of plates as an adjunct to IM rods.
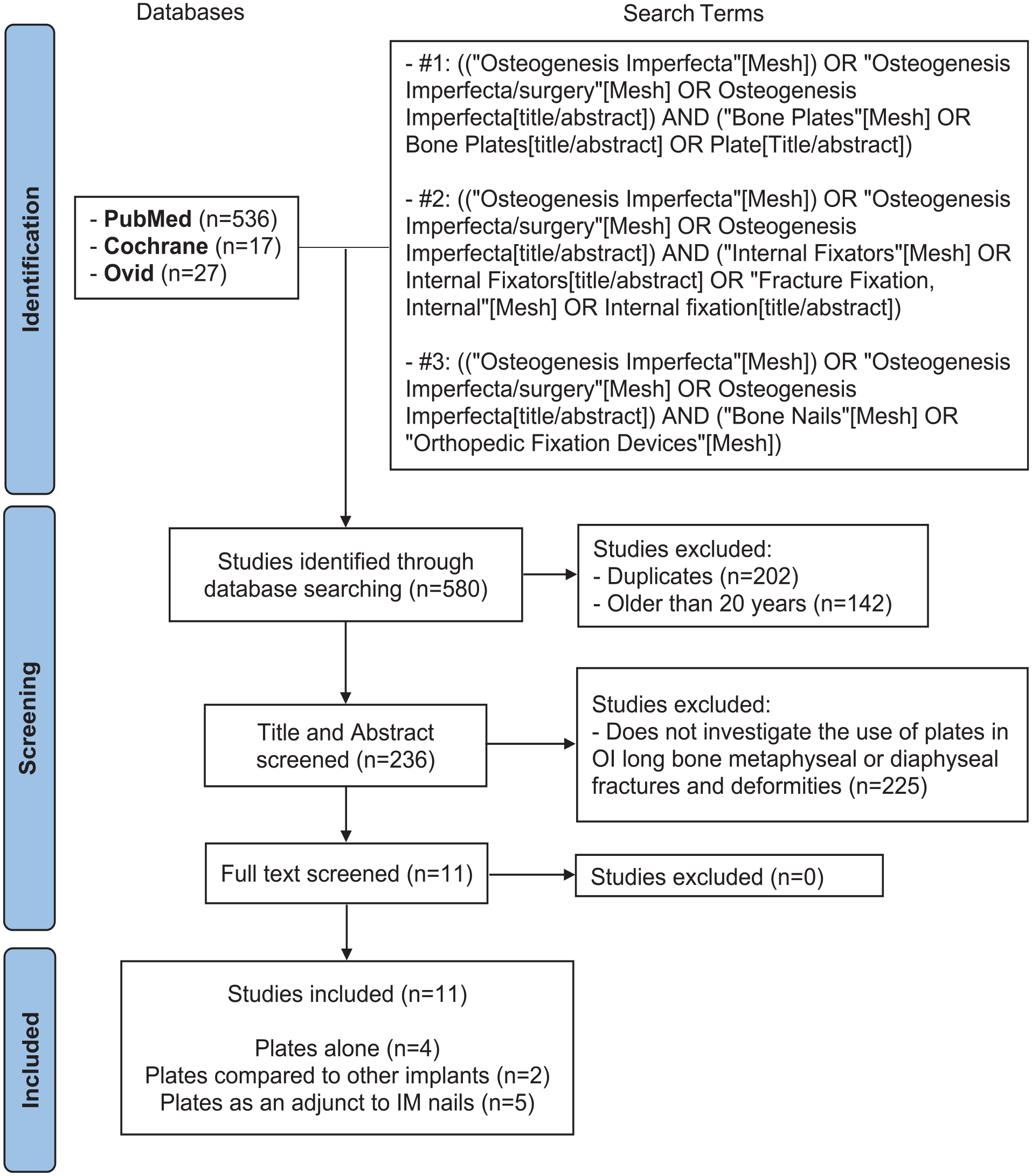
PRISMA flow diagram (PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only). 9
Results
As of January 2025, 11 articles were found, which are separated into three categories: “plates alone,” “plates compared to other implants,” and “plates used as an adjunct to IM fixation.”
Plates alone
Two studies and two case reports investigated the use of plates as the sole implant (Table 1).
Plates alone.
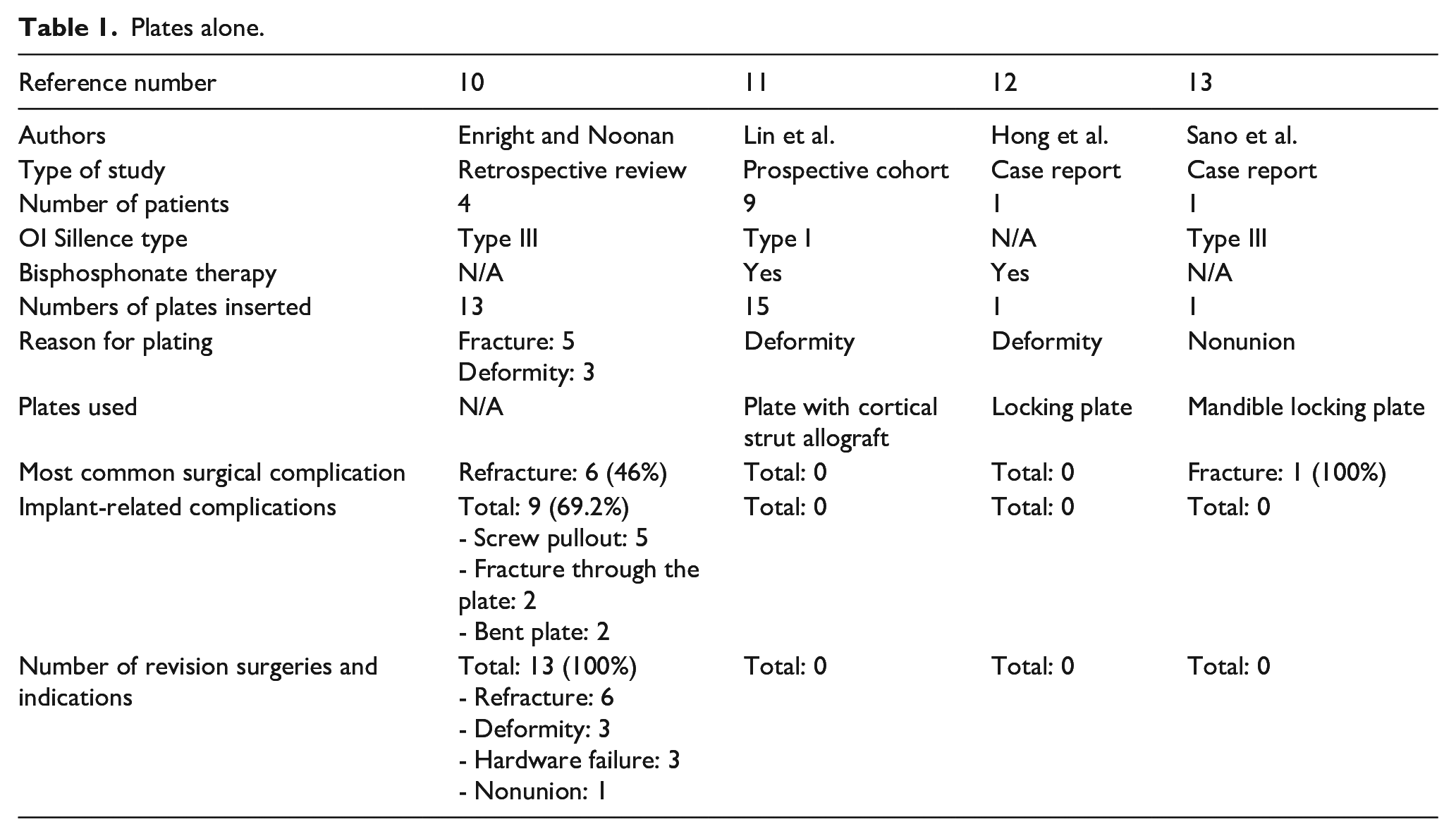
The first study is a retrospective review published by Enright and Noonan which assessed plating as the surgical treatment in four patients with type-III OI in the context of fracture and deformity. 10 The study reported that plating was associated with a high rate of complication, including refracture, deformity, hardware failure, and nonunion. In the end, all patients underwent a revision surgery. Implant-related complications (IRCs) were also present in almost 70% of the plates inserted, with screw pullout being the most common. Other IRCs included fracture through the plate and bending of the plate.
The second study is a prospective cohort study published by Lin et al. which investigated the use of plating with additional cortical strut allograft in nine children with type-I OI in the context of limb deformity. 11 In total, 15 plates were inserted on the lateral side of the involved bone, and an additional cortical strut allograft was placed on the opposite side to cover the weaker part of the shaft. All patients received bisphosphonate therapy. This study reports that all patients showed good fracture healing, that none of the patients experienced further complications nor required revision surgery, and that no IRCs occurred. Upon follow-up 1 year after the surgery, the allograft was mostly incorporated into the host bone.
The first case report by Hong et al. describes a 7-year-old female of unspecified OI type with a cubitus varus deformity in the context of a supracondylar fracture of the left humerus. 12 After receiving bisphosphonate therapy, she underwent fixation with a locking plate. At 3 months, there was uneventful healing of the fracture. No surgical complications nor IRCs occurred. The plate was removed at 11 months due to a left radius fracture that required elastic nail insertion.
The second case report by Sano et al. described the treatment of a 26-year-old man with type-III OI presenting with a right humerus shaft nonunion. 13 The patient had previously undergone a right humerus correction osteotomy with a K-wire at age 8, but non-union occurred due to K-wire breakage. Initial surgical treatment for the nonunion consisted of an IM elastic nail with bone graft, but as union was still not achieved 2 years later, the team decided to perform internal fixation with a mandible locking plate. This led to bony union. In the 4 years following the plating, the only complication was an asymptomatic fracture line on imaging, which was treated with a cast and healed well. At the latest follow-up, slight screw loosening was seen, but no revision surgery was required. No other IRCs occurred.
Plates compared to other implants
Two studies compared different implants including plates (Table 2).
Plates compared to other implants.
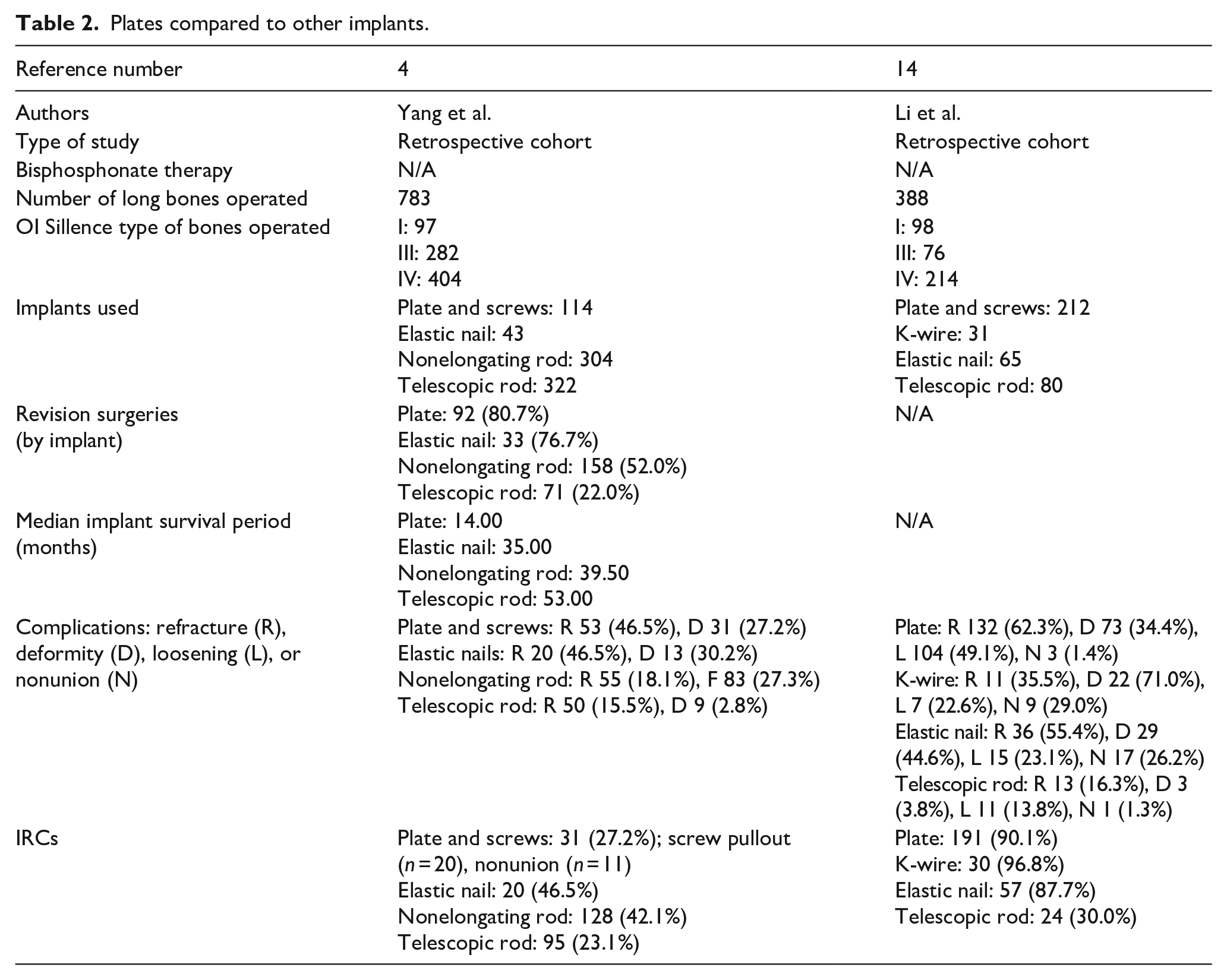
The first study is a retrospective cohort study by Yang et al. comparing telescopic rods, nonelongating rods, plates, and elastic nails to determine which of them is the best femoral implant. 4 This study included 783 femoral procedures in patients with OI type I, III, or IV. Of those, 114 were plates inserted in the context of narrow canals. The results show that plates had the highest rate of revision surgery (81%) and lowest implant survival period. Furthermore, 27% of the plates had IRCs, with screw pullout being the most common. In comparison, telescopic rods performed the best overall, with the lowest complication rate, revision surgery rate, and the longest survival period.
The second study is a retrospective cohort study by Li et al. investigating IRCs in 388 femoral procedures performed in patients with OI type I, III, or IV. 14 The implants used were plates, elastic nails, K-wires, or telescopic rods. Plates had the second highest rate of IRCs (90%) behind K-wires (97%). The number of complications was also high, with the most common ones being refracture (62%), loosening of implant (49%), and deformity (34%). In comparison, telescopic rods had the lowest rate of IRCs (30%) and complications overall.
Plates as an adjunct to IM fixation
Four studies and one case report investigated the use of plates as an adjunct to IM fixation (Table 3).
Plates as an adjunct to IM rods.
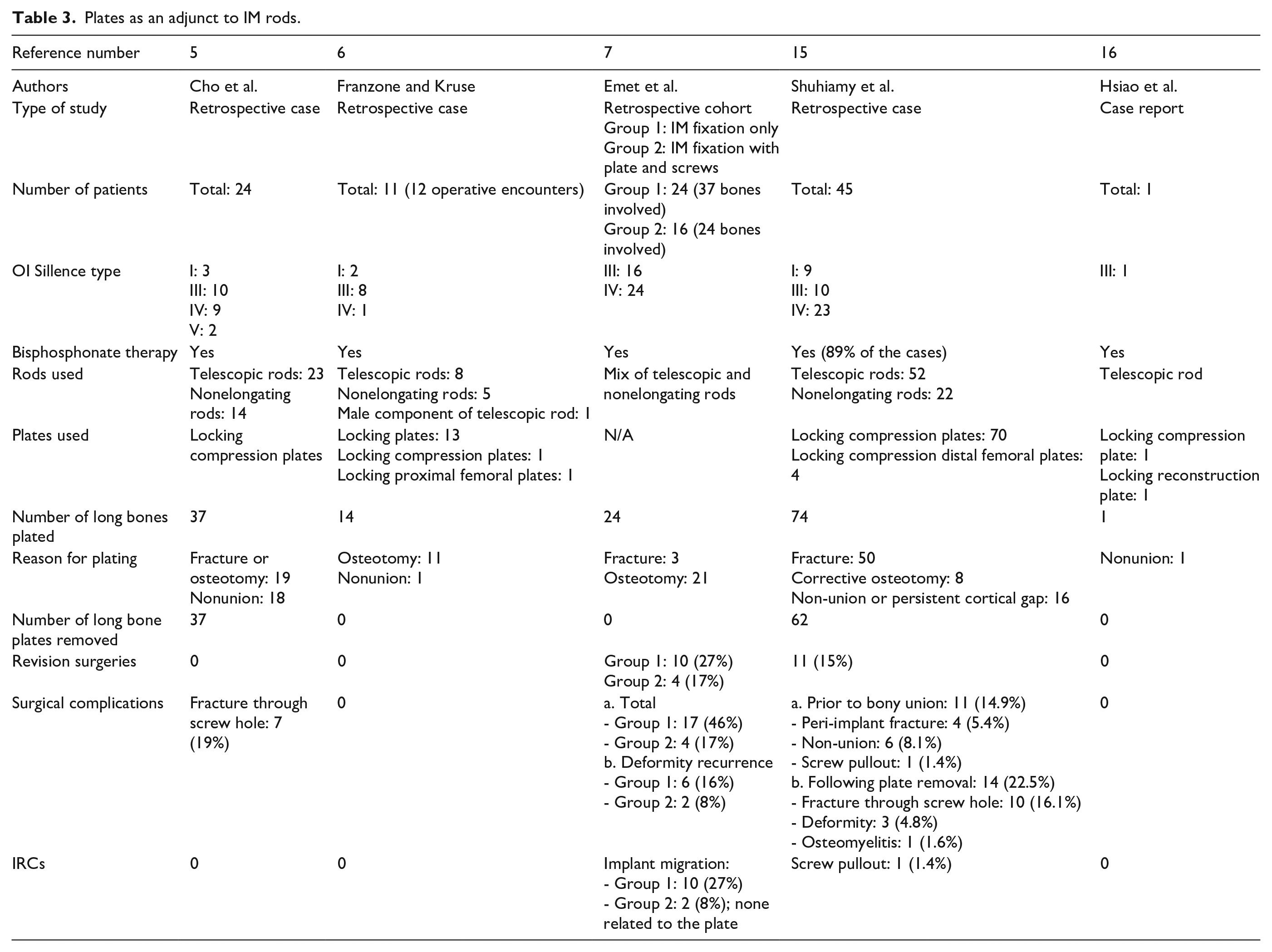
The first study is a retrospective case study by Cho et al. involving 24 patients with OI type I, III, IV, and V. 5 The study involved 37 bones plated with locking compression plates as an adjunct to IM fixation with either telescopic or nontelescopic rods. The indications for plating were fracture, osteotomy, and nonunion. All patients received bisphosphonate therapy. In the end, all fractures and osteotomies healed completely. There were no revision surgeries required, and no complications or IRCs occurred. All the plates were removed following union at a mean time of 1.8 years, and bone matrix was inserted inside the screw holes to accelerate healing. The sole complication following plate removal was fracture through the screw holes in 19% of the cases. In the patients that did not have fractures through the screw holes, most screw holes were fully healed 1 year after plate removal.
The second study conducted by Franzone and Kruse is a retrospective case study involving 11 patients with OI type I, III, and IV who underwent plating using locking, locking compression and locking proximal femoral plates as an adjunct to IM rodding using telescopic and nontelescopic rods. 6 The indications for plating were fracture or deformity requiring an osteotomy and nonunion. All patients received bisphosphonate therapy. The study reports that all the long bones plated achieved radiographic union with no revision surgeries needed, no surgical complications, and no IRCs. At the time of the publication, one patient was scheduled for revision surgery due to snapping of the IT band over a femoral plate.
The third study by Emet et al. is a retrospective cohort study looking at lower extremity IM fixation alone in group 1 in comparison to IM fixation with additional plating in group 2. 7 Forty patients with OI types III and IV were involved in this study, which included 61 long bones: 37 in group 1 and 24 in group 2. IM fixation was performed using a mix of telescopic and nontelescopic rods. The indications for both IM fixation alone and IM fixation with additional plating were fracture and osteotomy. All patients received bisphosphonate therapy. The results show that all patients but one in group 1 and all patients in group 2 had callus formation, and that there was no statistical difference between group 1 and group 2 on that aspect. Complications occurred in 46% of patients in group 1 and 17% of patients in group 2. The most common complications in both groups were implant migration and deformity recurrence. Of note, none of the IRCs that occurred in group 2 were related to the plates. Among the patients that had complications, 59% in group 1 and 100% in group 2 required revision surgery. When comparing both groups, there was a statistically significant difference between group 1 and group 2 in the incidence of complications after femur surgery and in patients who underwent surgery for corrective osteotomy. This was not the case in tibia surgery and in patients who underwent surgery for fracture.
The fourth study by Shuhiamy et al. is a retrospective case series investigating complications related to plating as an adjunct to IM rods before and after plate removal. 15 This study involved 45 patients with OI type I, III, and IV who underwent internal fixation for fracture, corrective osteotomy, and nonunion. The implants used were locking compression and locking compression distal femoral plates, as well as both telescopic and nontelescopic rods. Plates were removed once bony union was achieved with insertion of bone matrix to accelerate healing. Around 90% of the cases received bisphosphonate therapy. The study shows that 85% of the cases achieved union. Complications prior to plate removal were nonunion (8%), peri-implant fracture (5%), and screw pullout in one case (1%). No other IRCs were reported. Following plate removal, the primary complication was fracture through the screw holes, which occurred in 16% of cases. The study suggests that younger age may contribute to complications and notes that all screw-related complications involved 3.5 mm unicortical screws inserted in the diaphysis.
One case report by Hsiao et al. describes the case of a 4-year-old male with type-III OI who underwent plating in addition to IM fixation for atrophic non-union. 16 The mechanism of injury was unknown, and the initial treatment involved a telescopic rod alone. However, due to persisting nonunion, revision surgery was performed. This included the insertion of another telescopic rod, two plates (one locking compression plate and one locking reconstruction plate), and bone matrix protein. The patient received bisphosphonate treatment. The fracture ended up healing completely with no surgical complications, IRCs, or further revision surgeries.
Discussion
This scoping review identified 11 articles that investigated the use of plates in the treatment of long bone diaphyseal and metaphyseal fracture and deformity in OI. These were assessed in three different categories: plates alone, plates compared to other implants, and plates used as an adjunct to IM nails.
When looking at plates alone, their use has been discouraged. This is mostly due to the article by Enright and Noonan that shows a high rate of complications, IRCs (notably screw pullout), and revision surgeries. 10 The team therefore recommends the use of elongating rods, which support the bone as it grows. The study by Lin et al. shows better results when a cortical strut allograft is added to the fixation, with no complications or IRCs reported by the research team. 11 However, it must be considered that the latter involved patients with type-I OI, which is a milder form shown to have fewer complications as opposed to the more severe type-III OI, which formed the sample of Enright and Noonan’s study. 4 This would positively impact Lin et al.’s results. Furthermore, although the use of a graft could prove to be an effective method, one major limitation also described by the authors is the donor shortage for grafts. Additionally, two case reports show good outcomes in the context of cubitus varus deformity and nonunion.12,13 However, they both involve a single patient, which makes it hard to generalize to a larger population.
The two comparative studies by Yang et al. and Li et al. show that plates have a high number of complications, IRCs (mainly screw pullout), revision surgeries, and short implant survival period.4,14 This is especially true when comparing them to telescopic rods, which show significantly better results in those aspects. Yang et al. notably recommends giving priority to telescopic rods, especially in children with type-III and type-IV OI as they showed the highest level of complications. 4 However, it must be considered that plates were used in the context of narrow canals, in which the insertion of rods is not always ideal. In those cases, the main options are elastic nails, K-wires, and plates. When comparing those three options, plates seem to be a reasonable choice.
When looking at plates used in adjunct to IM nails, the results vary. Cho et al. had good results overall, with no IRCs and no revision surgeries. 5 More recently, Shuhiamy et al. reported that close to 15% of the cases had complications, that 15% of the patients underwent revision surgery and that one IRC (screw pullout) occurred. 15 They also suggested that complications could be related to younger age and to 3.5 mm screws inserted in the diaphysis. The common point between both those studies is that plates were removed once bony union was achieved, with additional insertion of bone matrix inside the screw holes to accelerate healing. Screw pullout was still the most common complication following plate removal in both studies, occurring in 19% of the cases in the first and 16% in the latter. Therefore, one aspect to consider in plating as an adjunct to IM fixation is that the removal of the plate can lead to complications. Furthermore, another consideration is the extra procedure required to remove the plate, which exposes patients to additional surgical risks. In the other two studies, plates were not removed, and therefore, complications related to plate removal were not assessed. Franzone and Kruse had good results with no complications, no IRCs, and no revision surgeries in their sample. 6 Emet et al.’s study allowed for comparison between IM rods used alone and IM rods used with plates. 7 Although the implant used did not affect callus formation, their results show that adding a plate with the IM rod could be beneficial, especially when considering that no IRCs related to the plates occurred. Finally, the case report by Hsiao et al. showed appropriate healing of a nonunion without any further complications or IRCs, although as mentioned previously, the presence of a single patient in this article makes it hard to generalize to a broader population. 16
In the case of plates as an adjunct to IM fixation, the indications for plating must also be considered. In all the studies mentioned, the reasoning for the additional plate comprised persistent cortical gap not healed with IM fixation alone, IM rod fitting the cavity being too thin for fixation, fracture, or osteotomies deemed difficult to heal with an IM rod alone including in the metaphyseal area, and rotation instability. In this context, the results are promising, although there is currently no clear indication recommended by the literature to add plating to an IM fixation. There are also no clear indications for plate removal at the current time, with some research teams leaving them in place while others remove them as soon as bony union is achieved.
Conclusion
The use of plates alone in the treatment of long bone diaphyseal and metaphyseal fracture in OI is not recommended due to the high number of complications, IRCs (mainly screw pullout), and revision surgeries, especially when compared to telescopic rods. However, they can be used when deemed appropriate by the surgeon or in the context of a narrow canal.
On the other hand, the use of plates as an adjunct to IM nails shows promising results in selected cases, although further research is required to determine the precise indications for additional plating and the best timing for plate removal, as the latter can lead to fracture through the screw holes.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251332498 – Supplemental material for Plates for the treatment of long bone metaphyseal and diaphyseal fracture and deformity in osteogenesis imperfecta: A scoping review
Supplemental material, sj-pdf-1-cho-10.1177_18632521251332498 for Plates for the treatment of long bone metaphyseal and diaphyseal fracture and deformity in osteogenesis imperfecta: A scoping review by Yacine Louni and Reggie Hamdy in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
The authors sincerely thank the Shriners Hospitals for Children®-Canada for its support.
Author contributions
The authors confirm their contribution to the article as follows: study conception and design: Yacine Louni, Reggie Hamdy; data collection: Yacine Louni; data analysis and interpretation of results: Yacine Louni, Reggie Hamdy; original manuscript draft preparation: Yacine Louni; manuscript review and editing: Reggie Hamdy. All authors reviewed the results, approved the final version of the manuscript, and agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Ethical board committee approval was not necessary to conduct this scoping review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.