
Abstract
Background:
Supracondylar humerus fractures are common in childhood, and postoperative follow-up planning for surgically treated fractures is still controversial. This study aims to investigate the interobserver and intraobserver reliability of the Radiographic Union Score for Tibial Fracture in the postoperative radiological follow-up of pediatric supracondylar humerus fractures and to evaluate the clinical results with the scores obtained during follow-up.
Methods:
In this prospective study, patients who were operated on for supracondylar humerus fractures were called for follow-up three times: postoperative splint removal, pin removal, and final control. A total of 58 patients, 34 boys and 24 girls, who provided regular follow-ups, were included in the study. During follow-ups, the Radiographic Union Score for Tibial Fracture was calculated by evaluating the patients’ elbow anteroposterior and lateral radiographs, and the elbow joint range of motion was recorded with a goniometer. In two experiments, orthopedic surgeons evaluated intraobserver and interobserver reliability using the intraclass correlation coefficient at different times. The patients were evaluated at the last follow-up according to the Flynn criteria.
Results:
The first follow-up Radiographic Union Score for Tibial Fracture (median (range) was 8 (7–10), the second follow-up was 11 (9–12), and the third follow-up was 12 (11–12). Range of motion was 40° at the first follow-up, 90° at the second follow-up, and 120° at the third follow-up. Radiographic Union Score for Tibial Fracture and range of motion increased significantly as the weeks progressed (p < 0.001). Interobserver intraclass correlation coefficient at first follow-up was 0.80 (95% confidence interval 0.69–0.87), second follow-up was 0.85 (0.77–0.91), and third follow-up was 0.79 (0.67–0.87). Intraobserver intraclass correlation coefficient was 0.92 (0.88–0.95) at the first follow-up, 0.93 (0.98–0.96) at the second follow-up, and 1.00 (1.00–1.00) at the third follow-up. Flynn score results are functional; the cosmetic results were excellent in 46 patients, good in 4 patients, fair in 5 patients, poor in 3 patients, and cosmetic results were excellent in 54 patients and good in 4 patients.
Conclusion:
Our study determined that the radiographic union of fractures in pediatric supracondylar humerus fractures is reliably evaluated with the Radiographic Union Score for Tibial Fracture score. Radiographic Union Score for Tibial Fracture can be used to provide data-driven estimates of splint and pin removal.
Level of evidence:
Level II, prospective study.
Introduction
The most common elbow fracture type in childhood and adolescence is supracondylar humerus fracture.1 –3 Gartland type 2–3 pediatric supracondylar humerus fractures are often treated surgically with closed reduction and percutaneous pinning (CRPP) or open reduction (OR) methods.4,5 In the postoperative follow-up of pediatric supracondylar humerus fractures, the quality of reduction and bone union is determined by following radiological and clinical findings.
Today, no objective criteria exist for the exact week, and the K-wires used for pediatric supracondylar fracture fixation should be terminated.6 –9 At this stage, the decision is often made based on the usual routine practice in the relevant clinic and the surgeon’s experience and opinion regarding the union; on the other hand, evaluation of the union using direct radiographs can sometimes be difficult and complex.10 –13 Various scoring systems have been defined in the literature for an objective approach to the radiological evaluation of fracture union. 14 Radiographic Union Score for Tibial Fracture (RUST) is the radiological measure of the union of long bone fractures such as the tibia. It has been defined for objective evaluation, and its reliability has been shown in studies.12,13,15 Previous studies have suggested that RUST can be applied to metaphyseal bones, such as the distal radius. 20 However, no prospective study in the literature investigates the usability of RUST scoring in pediatric supracondylar humerus fractures.
The authors of this study think that scoring such as RUST, which includes objective criteria in the postoperative follow-up of pediatric supracondylar humerus fractures, may contribute to clinical results in terms of detecting adequate bone union and stability earlier and with increased accuracy. Thus, reducing the complications caused by prolonged immobilization or K-wire fixation may be possible.
This prospective study aimed to determine the RUST scoring of fracture healing and when it is safe to release the cast and withdraw the pins after pin fixation.
Materials and methods
Patients (0–12 years old) who were surgically treated for supracondylar humerus fractures at Afyonkarahisar Health Sciences University Hospital, Orthopedics and Traumatology Clinic between February 2019 and February 2020 were included in this prospective study. Exclusion criteria for the study were over 12 years of age, previous surgery on the relevant extremity, congenital deformity, neurological deficit, vascular pathology, tumor, osteomyelitis, soft tissue infections, or a history of accompanying systemic, neurological, or muscular disease. The study protocol was approved by the Medical Faculty of Afyonkarahisar Health Science University Ethics Committee (approval number/date: 2019-29/18.01.2019). Written informed consent was obtained from the legal guardians of each patient.
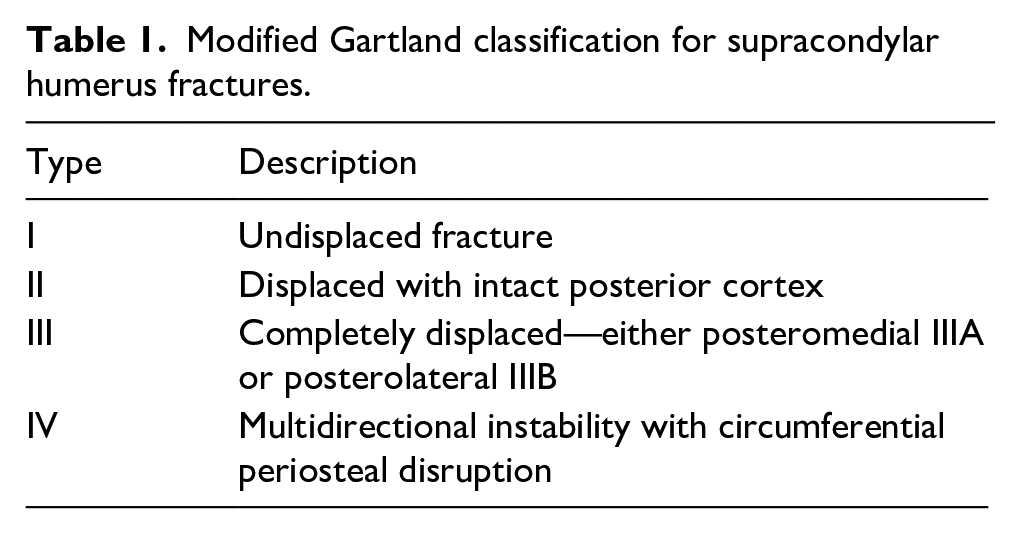
The researchers used the modified Gartland classification, including type 4 fractures, to stage pediatric supracondylar humerus fractures in this study (Table 1). 16 Since fractures type I are stable and treated non-operatively, they were not included in the study. For type 2 fractures, we primarily applied closed reduction and casting. We performed surgical treatment on patients with coronal and sagittal malrotation after casting. 17 For type 3 and type 4 fractures, we first tried closed reduction under anesthesia in the operating room and applied percutaneous pinning in the appropriate position. We performed open surgery on patients whose reduction was not acceptable after closed reduction. We reached the elbow joint through a lateral incision and performed reduction and pinning. We applied a long arm splint in a neutral position to all patients who underwent CRPP or OR.
Modified Gartland classification for supracondylar humerus fractures.
We routinely called the patients for three orthopedic outpatient clinic checks after the surgery: at 2 weeks for pin tract and surgical wound assessment, 4 weeks for pin removal, and the final check at 8 weeks. We invited patients who did not come to the polyclinic on time by calling them. Patients who did not come for routine follow-up were excluded from the study. Finally, we included 58 patients in the study (Figure 1).
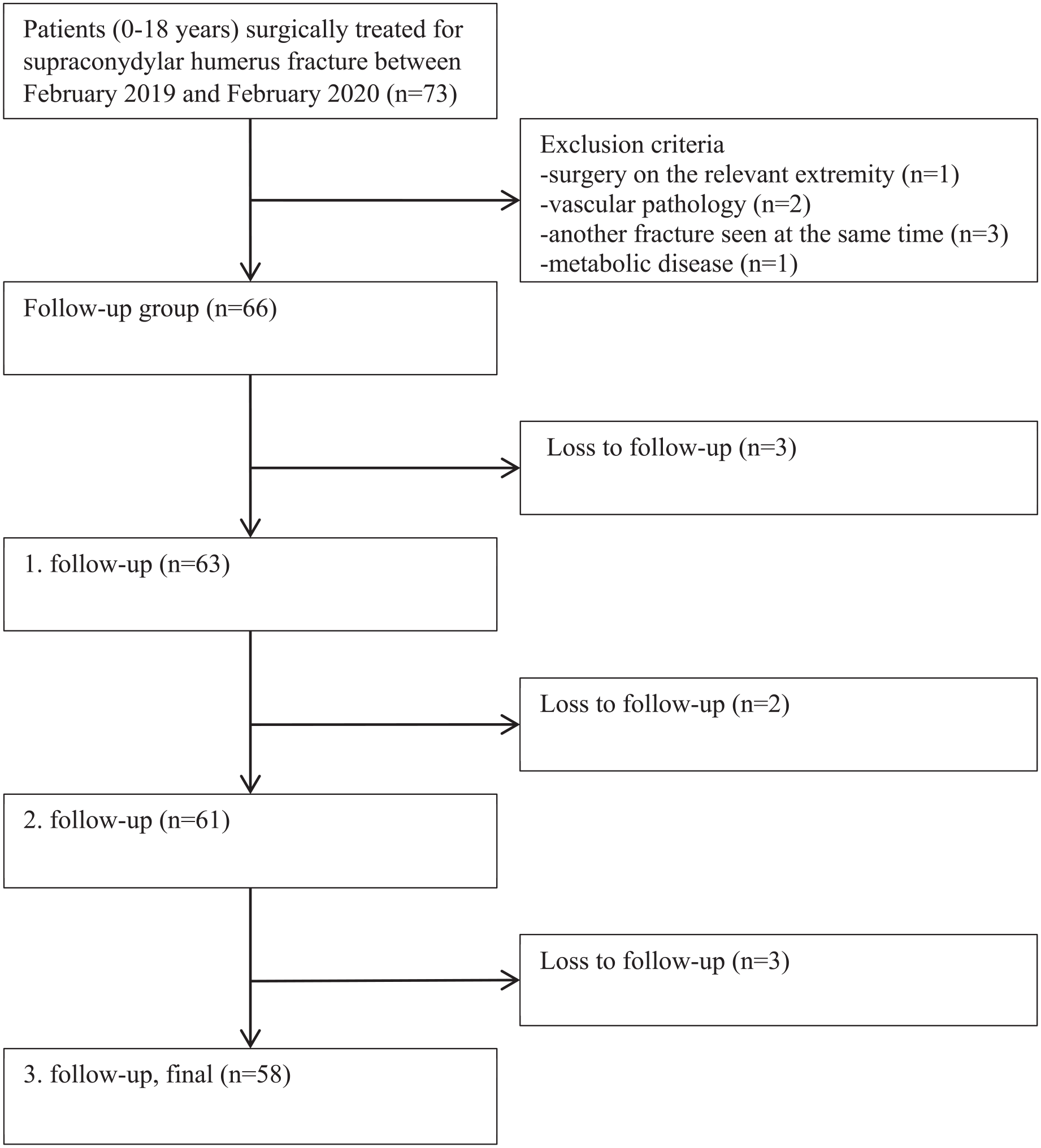
Flowchart showing how to identify patients.
Postoperative evaluation
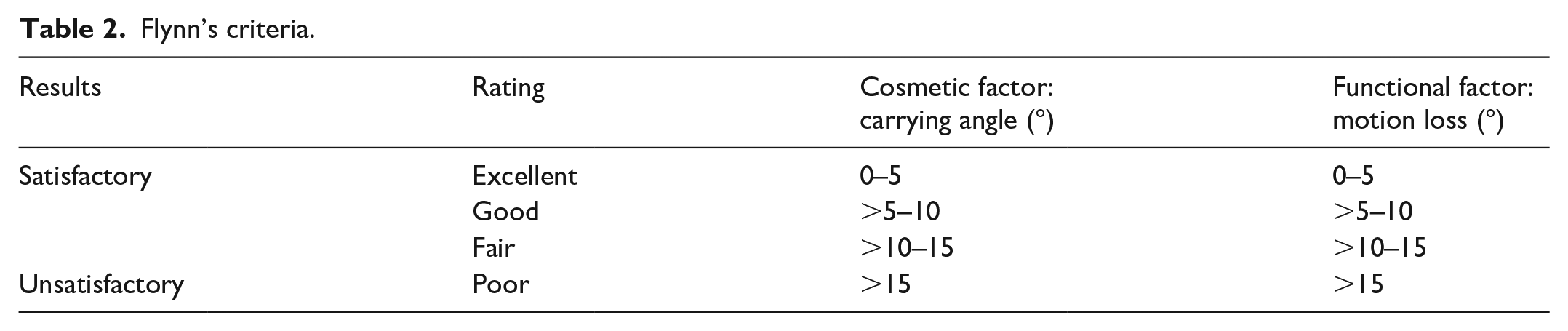
We took the patient’s elbow anteroposterior (AP) and lateral radiographs during the follow-up visits. We measured the patients’ elbow joint range of motion (ROM) with the help of a goniometer and noted them in degrees. We routinely removed K-wires at the second check-up and patients were given home exercises for the elbow joint. At the third follow-up, we evaluated the patients according to the Flynn criteria (Table 2).
Flynn’s criteria.
RUST evaluation
RUST was calculated as a result of measurements made at different times by two orthopedic surgeons with different experience levels (a trauma surgeon and a pediatric orthopedic surgeon), using the patient’s radiographs viewed with the help of Picture Archiving and Communication Systems (Figure 2). To perform RUST, the cortex at the medial and lateral fracture line is examined on the patient’s AP radiograph, and the cortex at the anterior and posterior fracture line is examined on the lateral radiograph. In radiographic evaluation, cortices (medial, lateral, anterior, and posterior) are scored between 1 and 3 according to the RUST score. In the RUST score, the cortex with a visible fracture line and no callus is given 1 point, the cortex with a callus and a visible fracture line receives 2 points, the cortex with a callus and no fracture line forming a bridge within the callus bridge receives 3 points. A minimum score of 4 (unrecovered) and a maximum total score of 12 (fully recovered) can be achieved.
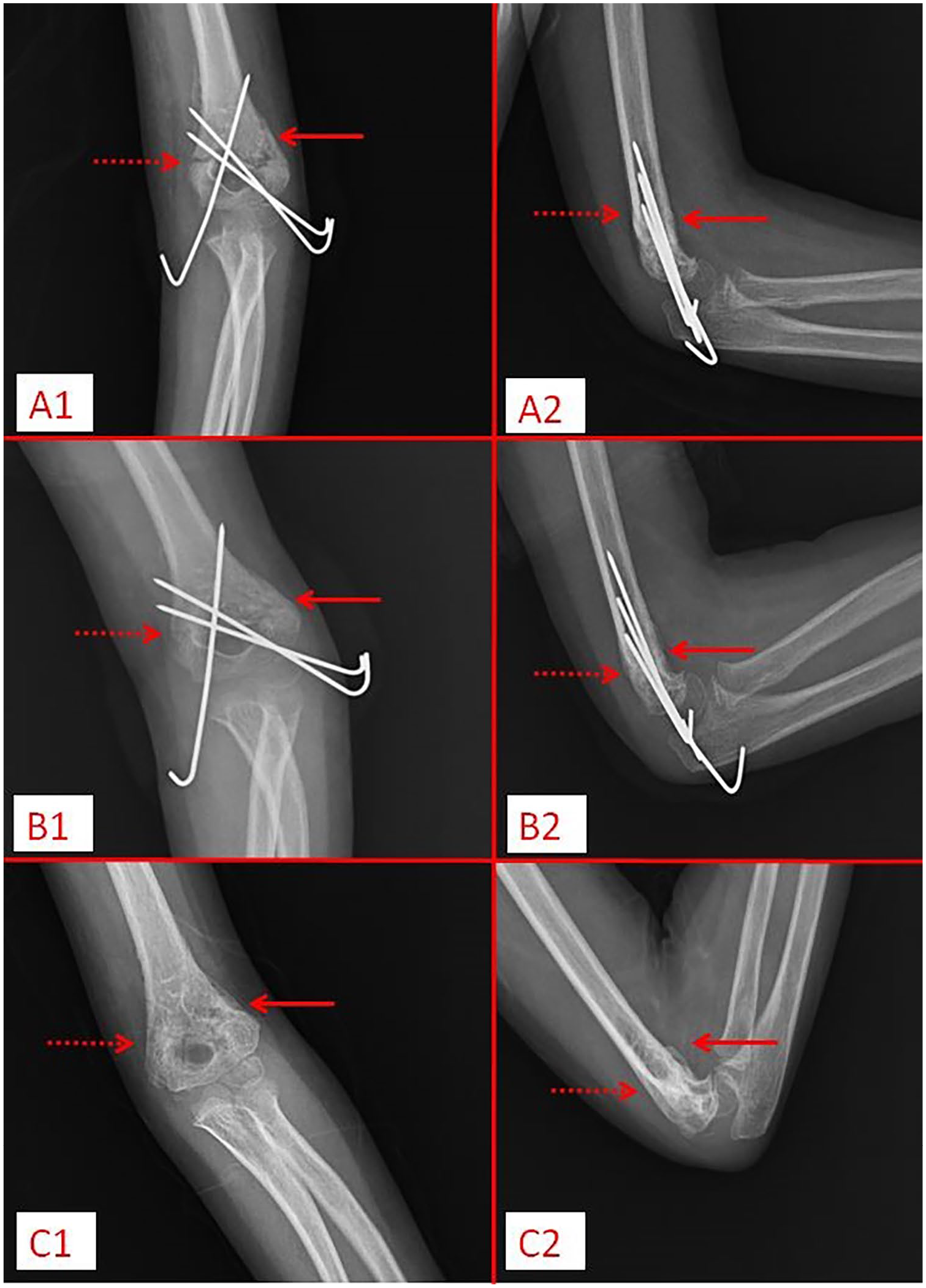
(A1, A2) First control (Day 19) radiographs of the patient who was operated on for supracondylar humerus fracture; (B1, B2) Second control (Day 29) radiographs of the same patient; (C1, C2) Third control (Day 60) radiographs of the same patient.
Statistical analysis
IBM SPSS version 20 (Chicago, IL, USA) program was used in the evaluations, and p < 0.05 was accepted as the limit of statistical significance. Continuous data with normal distribution, mean standard deviation, and data that did not comply with normal distribution, median, and (min–max) values were used in descriptive statistics. Categorical variables were shown with numbers and ratios. When the patient’s ROM values and RUST scores were examined for normal distribution using the Shapiro–Wilk test, it was seen that they were not normally distributed. Therefore, Friedman’s Test (Friedman’s two-way ANOVA by ranks) was used to compare the differences between ROM and RUST values in the first, second, and third controls.
The time at which the difference occurred was examined with Friedman’s Multiple Comparisons Test.
Mann–Whitney U-test was used to compare patients’ ROM values and RUST scores between surgical types. Kruskal–Wallis’s analysis of variance was used in comparisons between fracture classifications. As a result of the Kruskal–Wallis analysis, the classifications between which the difference existed were examined with the Kruskal–Wallis Multiple Comparison Test.
Intraobserver and interobserver agreement for ROM and RUST scores were examined with the intraclass correlation coefficient. The interpretation was performed as follows: >0.8 represents an almost perfect agreement, 0.7–0.8: strong, 0.5–0.6: moderate, 0.3–0.4: fair, and 0–0.2: poor.
Results
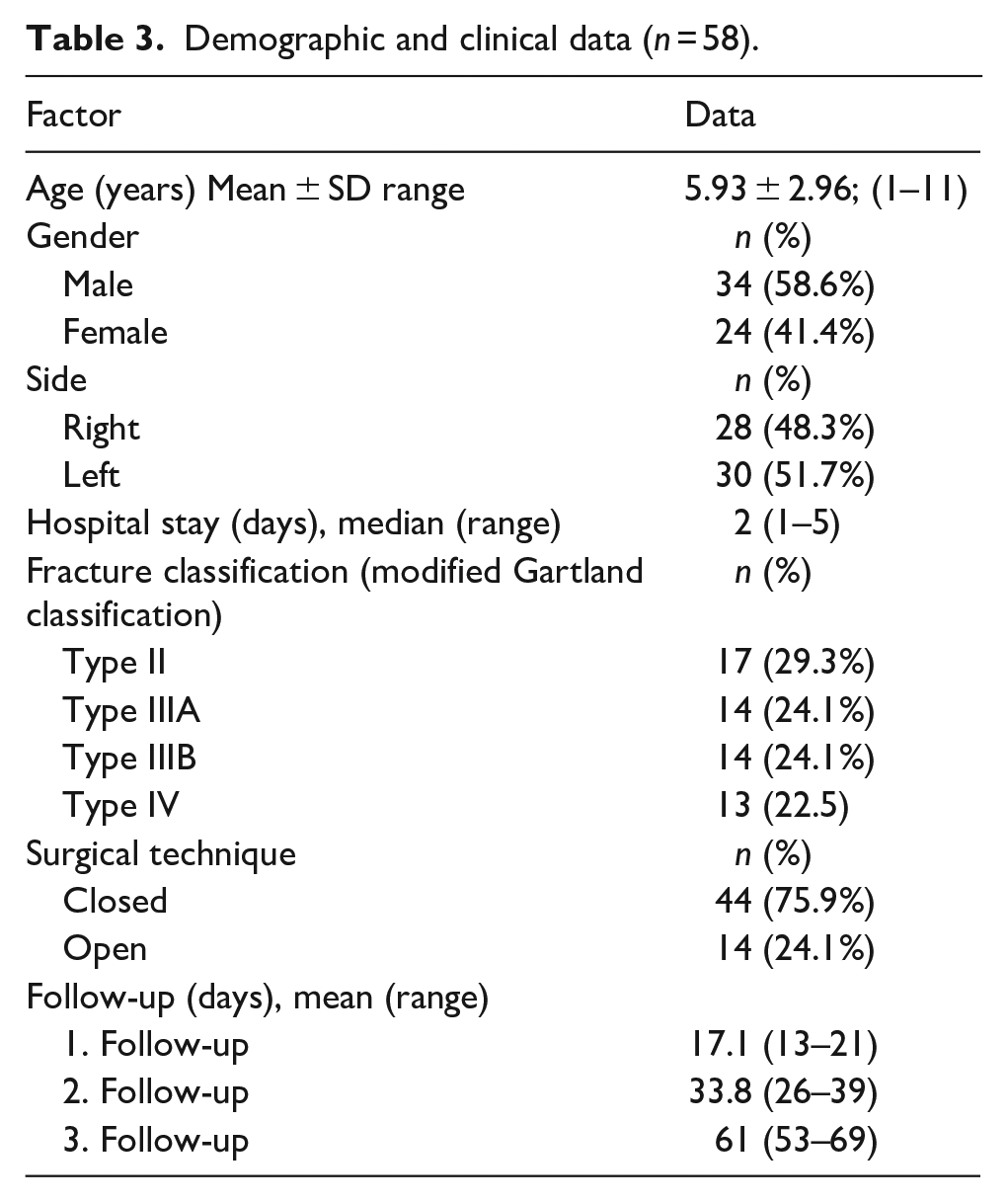
In this prospective study, 66 patients were planned, but 58 (34 males and 24 females) with regular postoperative follow-up were included (Figure 1). These patients without regular radiographs, measurements, and scoring were excluded to standardize the postoperative follow-up pattern and avoid distortion of statistical results. The mean patient age was 5.93 ± 2.96 years (1–11). The characteristics and clinical information of the patients are shown in Table 3.
Demographic and clinical data (n = 58).
ROM and RUST values obtained during patient follow-up are shown in Figures 3 and 4.
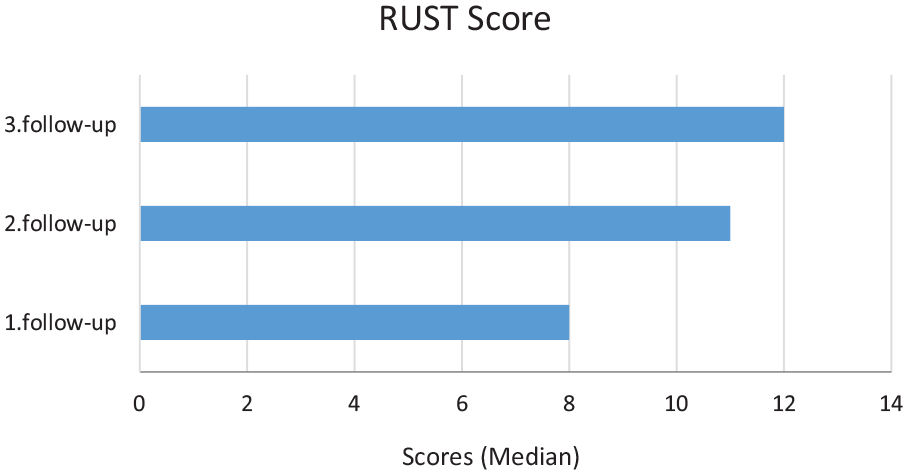
RUST scores at first, second, and third follow-ups.
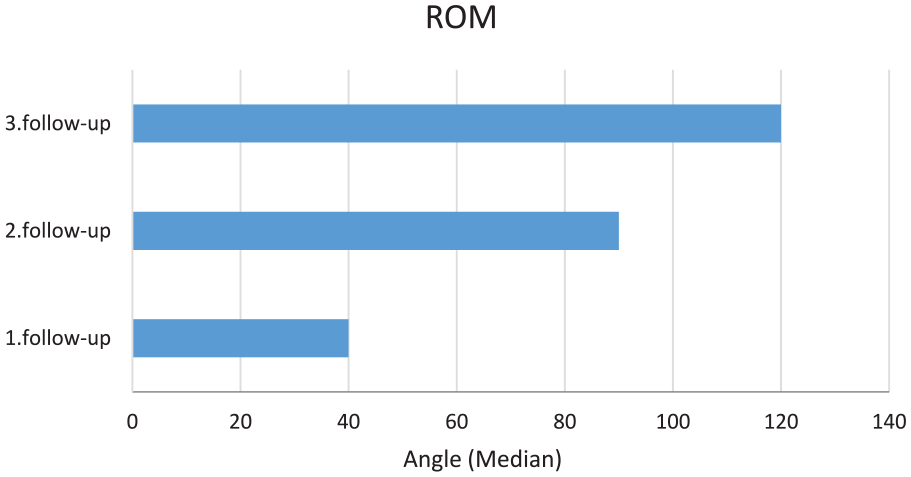
ROM values at the first, second, and third follow-ups.
RUST scores and ROM values increased significantly in all follow-ups (p < 0.001).
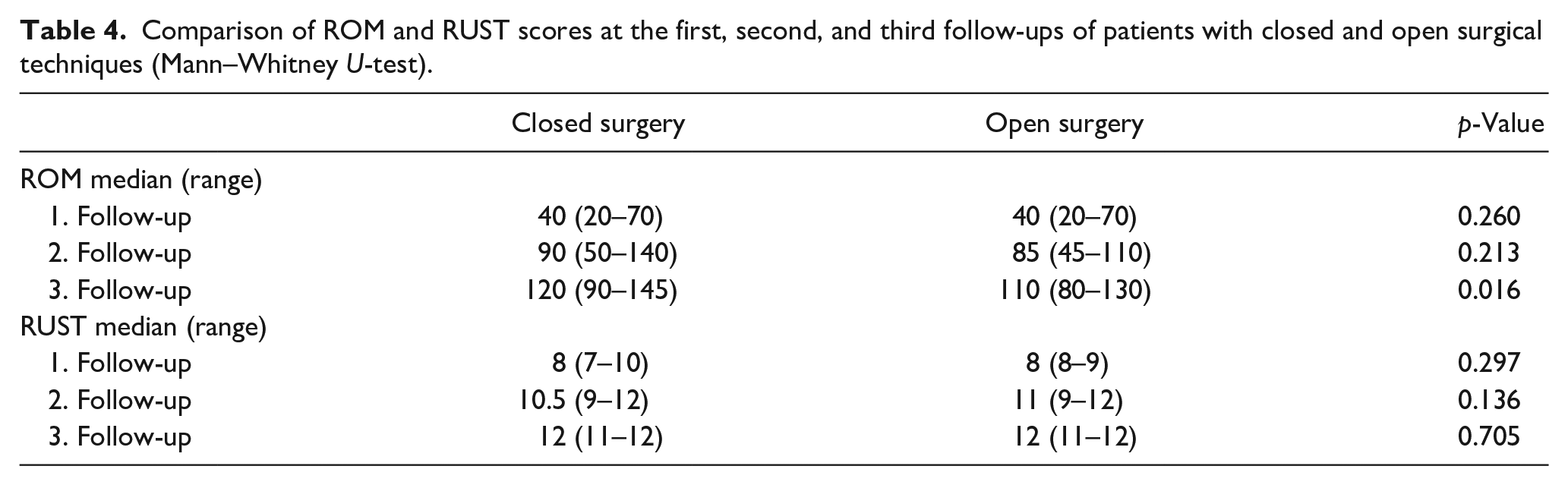
There was a difference between the ROM scores at the third follow-up of patients with closed and open surgical techniques (p < 0.05). ROM scores at the third follow-up of patients who underwent closed surgery were higher than those who underwent open surgery. There was no difference between RUST values in the follow-up of patients with closed and open surgical techniques (p > 0.05; Table 4).
Comparison of ROM and RUST scores at the first, second, and third follow-ups of patients with closed and open surgical techniques (Mann–Whitney U-test).
A difference was detected between the ROM values of patients classified as Type II, Type IIIA, Type IIIB, and Type IV at their second follow-up (p < 0.05). When examining which classification types the differences arise from, ROM values of Type IV patients at their second follow-up were lower than those of Type II patients (p < 0.05). There was no difference between the other classification types regarding ROM values at the second follow-up (Table 5).
Comparison of ROM and RUST scores of patients at their first, second, and third follow-ups between fracture classification levels (Kruskal Wallis Variance Analysis).
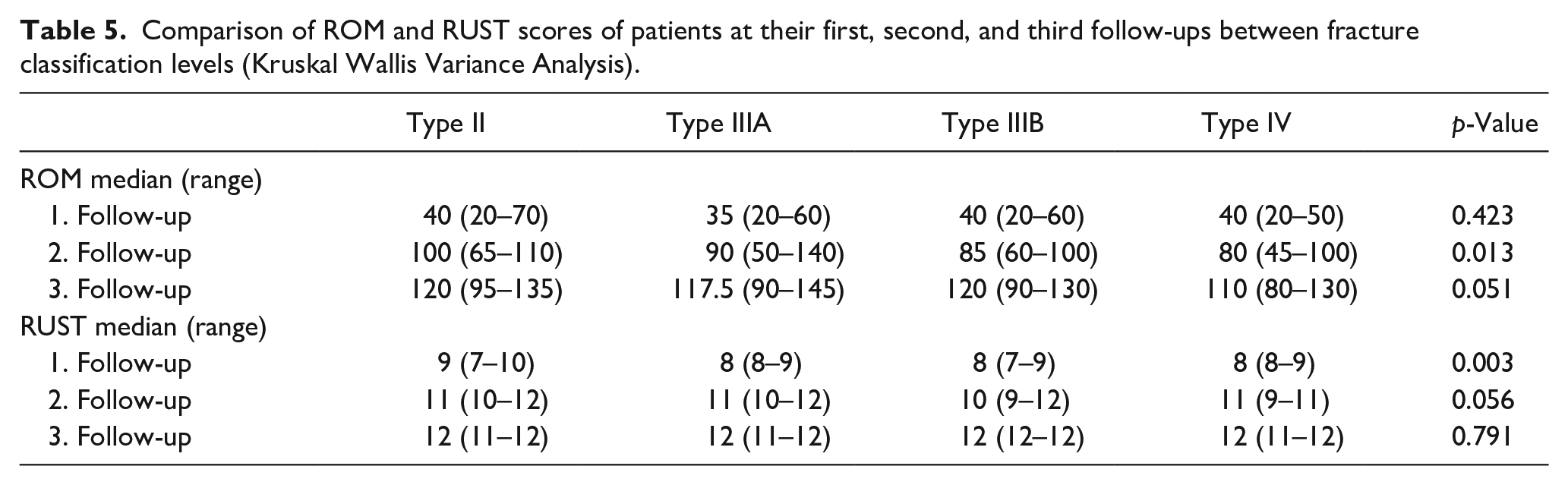
There was a difference between the RUST values at the first follow-up of patients classified as Type II, Type IIIA, Type IIIB, and Type IV (p < 0.05). When examining which classification types the differences arise from, RUST values at the first follow-up of patients with Type II classification were higher than those with Type IIIA, Type IIIB, and Type IV (Table 5).
At the last follow-up, the patients’ Flynn scores were checked. The Flynn score results of 58 patients were functional; 46 patients were excellent, 4 were good, 5 were fair, and 3 were poor. Cosmetic results were excellent in 54 patients and good in 4 patients. No significant correlation was found between the Flynn score and the RUST score. Interobserver and intraobserver agreement of RUST scores are given in Table 6.
Interobserver and intraobserver agreement of RUST scores according to the ICC method.
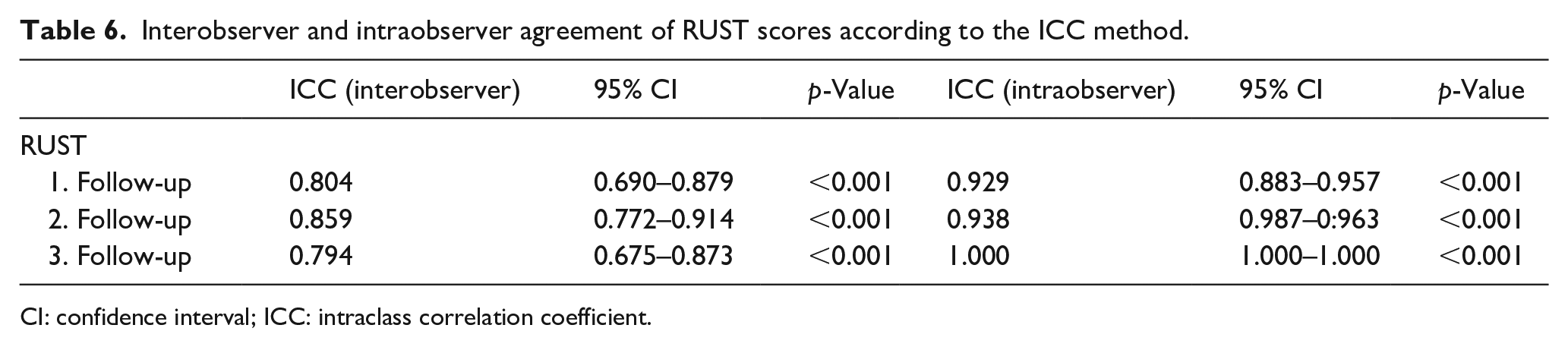
CI: confidence interval; ICC: intraclass correlation coefficient.
Discussion
Radiographic union score can objectively guide surgeons in evaluating bone union. 11 When we look at the literature, we see that radiographic union scores have been studied in tibia, humerus, radius, and hip fractures.18 –21 The authors calculated RUST from the elbow radiographs of the patients during follow-up and found that RUST increased continuously and regularly in the radiographs taken at the fracture follow-up. The authors determined RUST scores from the elbow radiographs of the patients during follow-up. The study results indicate that RUST scores exhibit a continuous and regular increase during the follow-up period. This study also showed that the RUST score can be used in pediatric supracondylar humerus fractures with excellent intraobserver agreement of 0.88–1.0 (95% CI) and strong interobserver agreement of 0.79–0.85 (95% CI).
Litrenta et al. applied the RUST score and modified RUST score to metaphyseal fractures treated with plate and intramedullary nails, evaluated interobserver agreement, and determined the radiographic union threshold. 22 Although the modified RUST score has a slightly higher interobserver agreement than the RUST score in metaphyseal fractures, they stated that it can be used in both. 22 More than 90% of reviewers claimed that a RUST score of 10 predicted decent bone union. 22 The study above was the first to attempt to correlate radiographic assessment of union with RUST scores in metadiaphyseal fractures. No similar studies exist in the non-weight-bearing upper limb. This or even a lower RUST value may predict union in humeral fractures. In our study, we removed the pins on the average 34th day and found a median (range) RUST value of 11 (9–12). No fracture complications were observed after the removal of the wires, indicating that union occurred, which is consistent with the literature.
Traditionally, removing splints and pins 3–4 weeks postoperatively has been recommended.3,23 In the European Pediatric Orthopaedic Association survey study, 40% of the participants stated that they removed the pins at week 3 and 58% at week 4. 10 Although many publications support this, this issue is still debatable. The 2012 American Academy of Orthopaedic Surgeons (AAOS) guideline has no recommendation regarding the pin removal time. 9 Early removal of the pins may increase the risk of sudden loss of reduction and re-fracture, while late removal may cause joint stiffness and loss of ROM. 9 The second follow-up average was the 34th day, and the pins were removed. According to the recommended literature, this time indicates that we were a little late for pin removal. This may have had a short-term negative effect on ROM. Type II fractures had significantly higher RUST values than Type IIIA, Type IIIB, and Type IV fractures at the first follow-up. We suggest that the pin can be removed quickly, especially in surgically treated Type II fractures. Future studies with larger patient groups may further clarify the timing of pin removal.
In their prospective study of 375 patients, Spencer et al. evaluated the ROM of patients treated with a cast or surgery due to supracondylar humerus fractures. 24 They stated that there were significant increases in ROM within the first month after cast removal, but the improvement continued for up to 1 year. They stated that surgically treated fractures had a 10% loss of motion compared to those treated with plaster. 24 In another publication, when Flynn functional scores of fractures operated with closed and open reduction were compared, the difference was significantly higher in fractures used with closed reduction. 25 In our study. ROM was significantly lower in patients treated with open reduction at their third follow-up. The relatively high rate of Type 4 fractures in our patient series and the higher rate of treatment of these fractures with open reduction, in line with the literature, may have caused this difference. 26
Gartland classification is also compatible with the severity of the fracture, and the difference in the type of fracture affects the healing time, complications, and functional results. 27 The results of this study indicate differences in the ROM and RUST values of type 2 fractures, particularly in the early follow-up period. Despite the differences in fracture types, the union and functional scores are equalized in the subsequent periods following appropriate reduction and treatment.
This study is the first to evaluate the intraobserver and interobserver reliability of the RUST score. The RUST score showed good interobserver reliability and excellent intraobserver reliability. Thus, its usability in pediatric supracondylar humerus fractures has been demonstrated.
This study has several limitations. We know that multidisciplinary studies are needed to confirm the reliability of using the RUST score in pediatric supracondylar humerus fractures. In addition, not performing a non-orthopedic observer evaluation may reduce the possibility of bias.
Our study is the first to evaluate pediatric supracondylar humerus fracture healing using RUST scores. Our study strengthened RUST scores by correlating them with fracture type, surgical method, and physical examination findings. However, following our clinical routine, the pins were removed in the fourth week. Evaluation of findings depending on different clinical routines may lead to different results.
Conclusions
Our study is the first to evaluate the radiographic union score in pediatric supracondylar humeral fractures. The RUST score showed good interobserver reliability and excellent intraobserver reliability. These scores can be used to provide data-based predictions of radiographic union for splint and pin removal.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251331773 – Supplemental material for Reliability of radiographic union score and correlation of clinical outcomes in children operated for supracondylar humerus fracture: A prospective study
Supplemental material, sj-pdf-1-cho-10.1177_18632521251331773 for Reliability of radiographic union score and correlation of clinical outcomes in children operated for supracondylar humerus fracture: A prospective study by Uğur Yüzügüldü, Murat Yeşil, Özal Özcan, Gökhan Maralcan and Mehmet Nuri Konya in Journal of Children’s Orthopaedics
Footnotes
Correction (November 2025):
Article updated to correct the section head from “Current Concept Review” to “Original Clinical Article”.
Author contributions
All authors have made substantial contributions to the conception and design, or acquisition of data, or analysis and interpretation of data, drafting the article or revising it critically for important intellectual content, final approval of the version to be published, and agree to be accountable for all aspects of the work if questions arise related to its accuracy or integrity.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Medical Faculty of Afyonkarahisar Health Science University Ethics Committee (approval number/date: 2019-29/18.01.2019). Written informed consent was obtained from the legal guardians of each patient.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.