
Abstract
Purpose:
A majority of ambulant children with cerebral palsy (CP) develop progressive musculoskeletal pathology (MSP) during growth. Fixed flexion deformity at the knee joint (FFDKn) contributes to flexed knee gait and is prone to relapse after index multi-level surgery. This perspective introduces the concept of “knee surveillance” (KS), defined as a repeated systematic assessment of gait and knee range of motion until skeletal maturity. KS aims to detect early FFDKn, allowing for early intervention with minimally invasive techniques such as anterior distal femur hemiepiphysiodesis (ADFH), and reduce the need for higher-risk surgery such as distal femoral extension osteotomy (DFEO) and patellar tendon shortening (PTS).
Methods:
Recent literature on the assessment of ambulant children with CP, consensus statements on indications for dose-based knee surgery, and the indications for ADFH have been reviewed and synthesized. These provide a preliminary evidence base for the concept of KS in ambulant children with CP.
Conclusion:
We propose the concept of KS for ambulant children with CP. The goals of KS are early detection of knee flexion deformity, early intervention, less invasive surgery, and better long-term outcomes. There is preliminary evidence to suggest that soft-tissue surgery, in combination with ADFH, can reduce, or perhaps replace, the need for more invasive surgery such as DFEO and PTS.
Level of evidence:
IV.
This is a visual representation of the abstract.
Keywords
Introduction
Cerebral palsy (CP) is the most common cause of upper motor neuron syndrome (UMNS) in childhood.1,2 The positive features of the UMNS are spasticity, hyperreflexia, and co-contraction. The negative features are weakness, loss of selective motor control, sensory deficits, and impaired balance.1,2 While the brain lesion in CP is a “static” encephalopathy, the musculoskeletal pathology (MSP) is progressive and changes as a consequence of growth and development.3 –6
Spasticity precedes contractures in children with CP
Recent longitudinal studies from Sweden have provided information on long-term trajectories and outcomes of MSP in children with CP. Hagglund et al. have shown that spasticity increases from birth until age 4 years in children with CP and then decreases each year until age 12 years. 7 Cloodt et al. found that contractures developed in 34% of lower limbs of children with CP, with the frequency increasing with severity of motor impairment as described by the gross motor function classification system (GMFCS) level.8,9 The timing and distribution of contractures were closely related to GMFCS levels. 9 The key feature of MSP in CP is the failure of longitudinal growth of skeletal muscle.3 –5,10 The prerequisites for normal muscle growth are regular stretching of relaxed muscle under physiological loading conditions and normal levels of activity. 10 Activity levels decrease with increasing GMFCS level.1,9,10
The first flexion contracture in the lower limbs of children functioning at GMFCS levels I and II was at the ankle, and for children functioning at GMFCS levels III to V, it was at the knee. 8 The development of secondary contractures at adjacent joints occurred in 44% of lower limbs.3 –5,8 These studies suggest the need for surveillance for joint contractures in the lower limbs of children with CP, with frequency based on GMFCS level.5,8 –10
Knee contractures in children and adolescents with CP
Fixed flexion deformity at the knee (FFDKn) significantly affects the biomechanics of gait, leading to flexed knee gait, quadriceps overload, and pain.3,4 Sagittal plane gait deviations most strongly correlate with long-term gait function and are the focus of several classification systems for bilateral and unilateral CP.10 –14 Increased dynamic knee flexion in stance phase exists in three of the gait patterns—jump knee with equinus, jump knee with apparent equinus, and crouch.12 –14 Crouch gait, characterized by increased hip flexion, knee flexion, and ankle dorsiflexion in the stance phase, should be considered an “end-stage gait phenotype” because it can lead to severe impairment or loss of walking ability.12,13,15,16 Crouch gait may be part of natural history in children with bilateral spastic cerebral palsy (BSCP) without treatment (Figure 1) but can also be iatrogenic. 17 Isolated lengthening of the gastrocsoleus muscle tendon unit (MTU) may impair Ankle Plantar Flexion-Knee Extension (PF-KE) coupling, leading to the development of an FFDKn and progressive crouch gait.16 –21
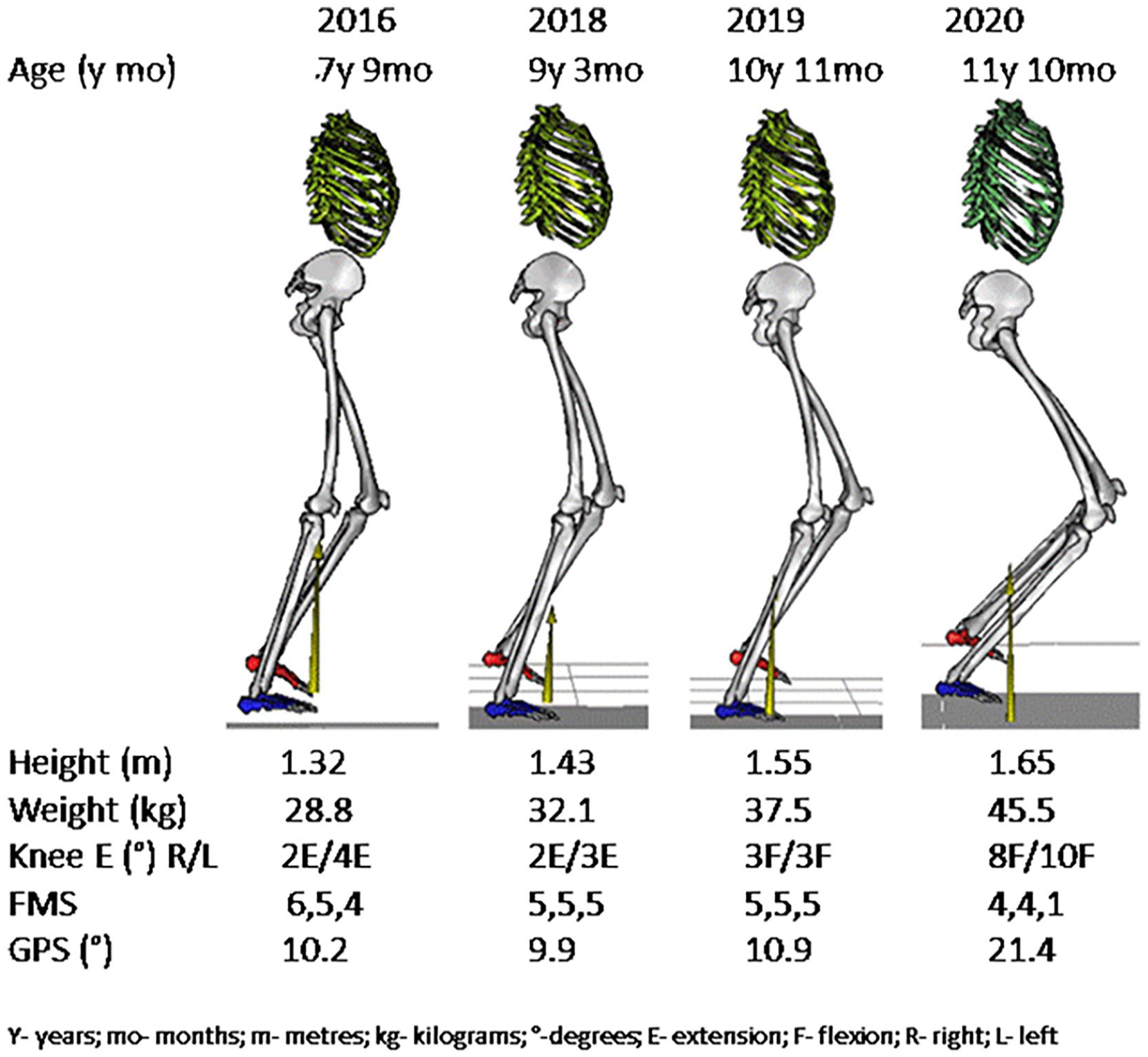
Progressive crouch gait in bilateral cerebral palsy.
The development of FFDKn is often multifactorial.16 –21 Weakness of the gastroc-soleus complex, either as a result of natural history or gastrocsoleus lengthening, is the most common cause of progressive crouch gait.16 –18 The development of torsional deformities in long bones and instability of joints, including the hip and subtalar joints, are also important in the development of FFDKn.21 –23 Increased external tibial torsion and pes valgus may compromise the generation of a plantarflexion moment by the gastrocsoleus.15,22 This may contribute to defective PF-KE coupling and habitual knee flexion during gait, leading to the development of FFDKn.21,22
There are three important longitudinal studies of gait in children with bilateral spastic CP, which confirm that the MSP, gait impairment, and flexed knee gait, are progressive during childhood.24 –26 This evidence, combined with the recent studies from Sweden, provides a framework for the development of KS in the lower limbs of children with BSCP.7,8,24 –26
Methods
Recent literature on the assessment of ambulant children with CP, Delphi consensus statements on indications for dose-based knee surgery, and the indications for anterior distal femur hemiepiphysiodesis (ADFH) were reviewed and synthesized. The study was approved by the institution’s Human Research Ethics Committee: QA/51280/RCHM-2019. No external funding was received in support of this study (Supplemental Material).
Results
A recent classification of MSP has identified four principal stages in children with CP. 5
Stage I: Hypertonia and dynamic contractures. Hypertonia includes spasticity, mixed tone, and dystonia.
Stage II: Fixed contractures particularly in the gastrocsoleus, hamstrings, and hip flexors.
Stage III: Contractures combined with torsional deformities affecting the femur and tibia, and foot segmental malalignments.
Stage IV: Decompensation of the musculoskeletal system with more severe MSP requiring salvage surgery for correction (Figure 2).
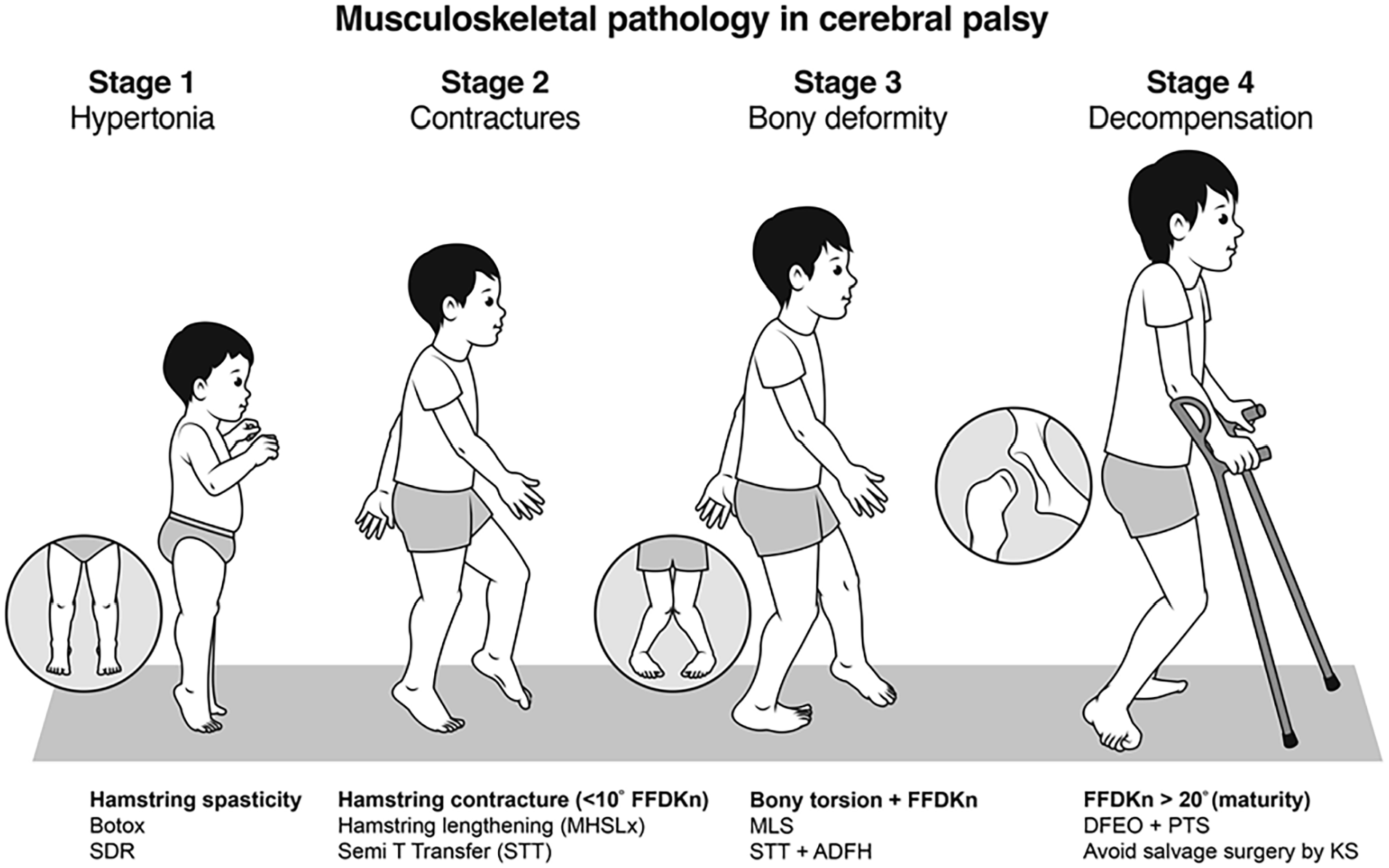
MSP in diplegia with an emphasis on knee involvement and knee management.
The stage and severity of MSP are directly relevant to management.5,6 Our management algorithm (Figure 2) indicates that a therapeutic window exists for spasticity management before the development of fixed contractures.1 –6 A second therapeutic window exists for the correction of fixed musculoskeletal deformities before the onset of decompensation.5,10
The rationale for KS
The concept of surveillance
Surveillance is the systematic ongoing collection, collation, and analysis of appropriate data with timely dissemination of information to those who need to know so that appropriate action can be taken. 27 “Systematic” and “appropriate data” imply that evidence exists as to which data should be collected and when it should be collected. “Appropriate data” should have the features of construct validity, reliability, and sensitivity to change. “Timely” and “appropriate action” suggest that early identification can allow for earlier treatments that possess lower risks and improved benefits at the individual and societal levels. Early identification and treatment of FFDKn fulfill the criteria to be considered as surveillance. 27
To date, no programs have been developed for early detection of lower limb deformities and gait deterioration for ambulant children with CP. The Cerebral Palsy Follow-Up Program group has emphasized the value of regular physical examinations for all children with CP and has popularized the concept of hip surveillance.7,8,28 There is substantial evidence for the progression of lower limb deformities, leading to deterioration in gait and function.24 –26
Successful management of dynamic knee flexion in ambulant children with CP requires a competent PF-KE.20,21 The principles to minimize the prevalence and severity of crouch gait in children with CP are to avoid early single-level surgery at any MSP Stage, maintenance of a competent PF-KE couple with appropriate tone management and AFO prescription in MSP Stage I, and perform timely multi-level surgery (MLS) in MSP Stage II or III before the onset of decompensation.29 –34 Even with this comprehensive approach, knee function may deteriorate during adolescent growth due to the development of FFDKn.3,4,17,29 We propose an active program of KS from childhood until skeletal maturity.3 –5
Proposed KS frequency
We propose that knee surveillance (KS) evaluations begin at age 5 years, corresponding to when a stable gait pattern is established and when changes in function and range of motion (ROM) are likely.35,36 Between the ages of 5 and 9 years, KS evaluations may be timed every 24 months, allowing for identification of early declines in knee range of motion and function so that timely intervention is possible (Table 1).5,8
Proposed knee surveillance guidelines.
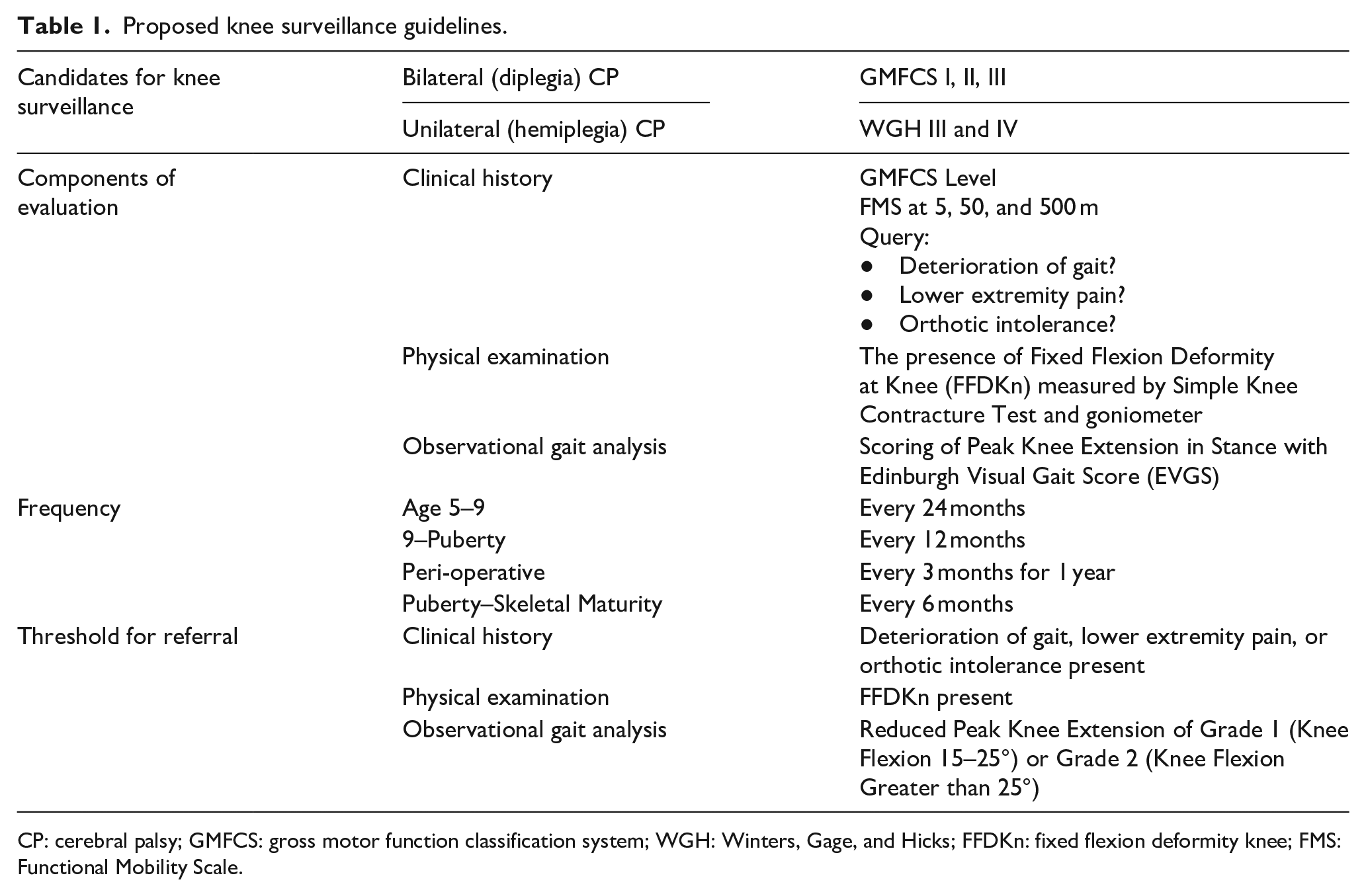
CP: cerebral palsy; GMFCS: gross motor function classification system; WGH: Winters, Gage, and Hicks; FFDKn: fixed flexion deformity knee; FMS: Functional Mobility Scale.
The timing of the adolescent growth spurt is critical for the development of KS guidelines (Figure 3). 37 Age at the start of the pubertal growth spurt is variable and sex-dependent. The period of sustained increase in height is referred to as peak height velocity (PHV), which varies in studies but averages 9.5 cm/year in boys and 8.3 cm/year in girls. The time when the annual height increase reaches a maximum is referred to as the PHV age, which is 13–15 years for boys and 11–12 years for girls. The contribution of pubertal growth to final height is approximately 30 cm in boys, accounting for approximately 18% of adult height, and 28 cm in girls, accounting for 17% of adult height. 37
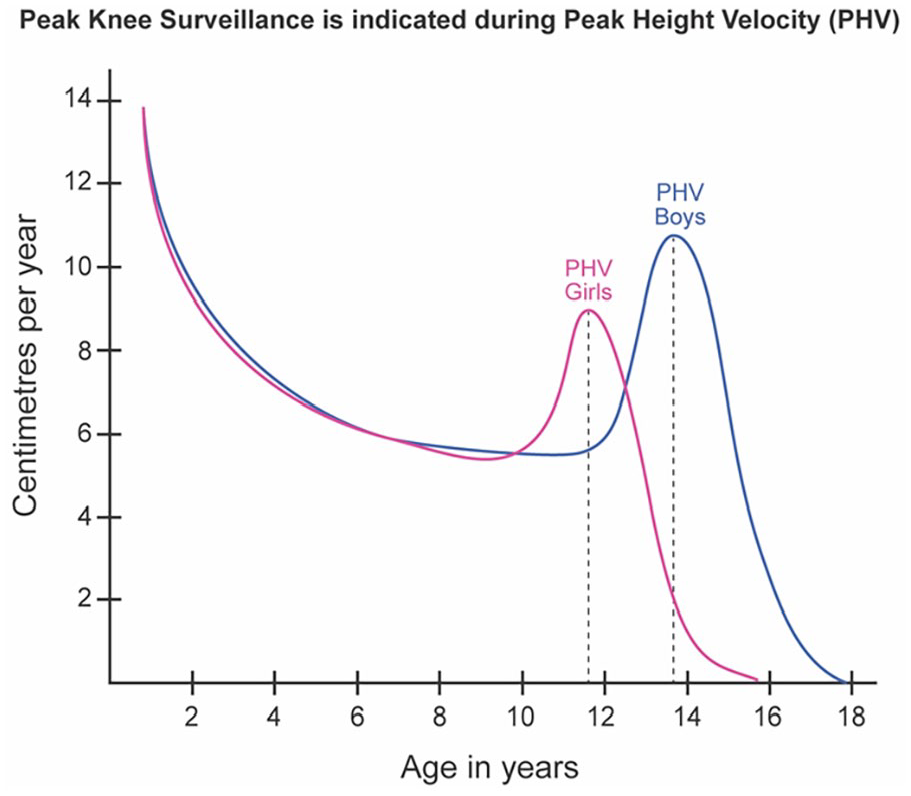
The relationship of peak knee surveillance to peak height velocity.
Based on these data, we suggest that KS evaluations increase in frequency to every 12 months after age 9, as this generally correlates to the period just before PHV when rapid growth and changes to ROM are most likely to occur.5,37 KS evaluations should again increase in frequency to every 6 months during the PHV until skeletal maturity, enabling timely referral during a critical window where growth modulation techniques may be effective in improving knee ROM. If the child has MLS, KS evaluations should increase to every 3 months for the first 12 months after surgery to closely monitor anticipated changes in knee ROM and function (Table 1 and Figure 3).31 –33
Proposed KS clinical evaluation
The ideal KS evaluation should have several important features:
It can be performed in an outpatient clinic by a broad set of providers familiar with musculoskeletal system and gait evaluation. These providers may include physiotherapists, nurse practitioners, physician assistants, physicians, and surgeons.
The evaluation should be sensitive to change and easy to perform.
The evaluation should employ inexpensive and readily available diagnostic tools.
We propose a KS evaluation that includes a focused clinical history, physical examination, and observational gait analysis.
Clinical history
The initial KS clinical history should include the following: birth history, age at independent walking, topographical distribution of CP, GMFCS level, functional mobility as assessed by the Functional Mobility Scale (FMS), prior interventions for spasticity, and surgical history.1,8,38,39 Prior lengthening of the gastrocsoleus muscle-tendon unit is especially important.18,19
Follow-up KS clinical history should document GMFCS and FMS, as well as an inquiry into whether any of the following “red flags” are present: decreased speed and distance of walking, lower extremity pain, orthotic intolerance, and increased dependence on assistive devices or wheelchair mobility, on serial FMS data.38 –40
Physical examination
Simple Knee Contracture Test (SKCT, Figures 4 and 5): We propose the SKCT for detecting a clinically significant FFDKn. The child is supine on a firm examination table, with the hips in extension, knees in neutral rotation (patellae facing upwards), and heel rests in a stable position on the table. Downward pressure is applied to the femur immediately above the patella, taking care to stabilize the leg and keep it from rotating during the test. Pressure should be applied in a firm but gentle manner to reach maximum knee extension, recognizing that the knee may spring back into mild resting flexion with the release of the pressure. At maximum knee extension, the examiner looks for a “popliteal gap sign,” a gap between the popliteal fossa and the examination table where the hand can pass behind the popliteal fossa without any contact. When a clinically relevant FFDKn is present, a positive popliteal gap sign is present (Figure 5). In a flexible knee, the knee may rest in mild flexion but with downward pressure, there is full knee extension and no popliteal gap (Figure 4). It has been our experience that an FFDKn greater than 10 degrees can be easily ascertained with this SKCT. To paraphrase another common public safety recommendation, we should “mind the (popliteal) gap.” [https://en.wikipedia.org/wiki/Mind_the_gap]

Simple knee contracture test: Negative. (a) 8-year-old female with unilateral cerebral palsy showing mid-stance ankle equinus and knee flexion (right side). (b) Supine examination shows resting knee flexion of 10°, right knee. (c) Compression of the knee demonstrates no gap behind the popliteal fossa with an inability to pass the hand behind the knee. No clinically relevant fixed knee flexion contracture is present.

Simple knee contracture test: Positive. (a) A 13-year-old male with bilateral cerebral palsy showing mid-stance ankle dorsiflexion and knee flexion. (b) Supine examination shows resting knee flexion of 15°. (c) Compression of the knee demonstrates a persistent gap allowing for the passage of the hand behind the popliteal fossa. A clinically relevant fixed knee flexion contracture is present.
Measurement of knee flexion deformity with goniometer: The key measure during physical examination is accurate measurement of passive knee extension range for FFDKn. An FFDKn as little as 5° may be of interest and significance to gait and long-term prognosis.41,42 A measurement of knee ROM by a single examiner can give vital information, but a systematic examination protocol conducted by two trained examiners may improve reliability. 41 Change in serial measurements over time is much more valuable than a single measurement (Figure 3). With serial evaluation, FFDKn trending higher can be identified and treated in a timely manner.
Popliteal angle: Examination of the popliteal angle is widely used, and we consider it important, despite the poor correlation between popliteal angle and knee kinematic function.23,29 We recommend using both unilateral and bilateral popliteal angle measurements.40,41 Measurement of passive range and dynamic catch of the popliteal angle gives a guide to the degree of spasticity and contracture in the hamstring muscles.1,2 Joint ROM may be referenced to the profiles of both typically developing children and the trajectories identified for children with CP.41,42 Intra- and inter-observer reliability of physical examination measures at the knee are acceptable when conducted by trained observers, using standardized protocols. 41 The reliability of measurement of FFDKn is better than for popliteal angle and intra-observer agreement is generally better than inter-observer agreement. 41
Physical examination measures require further routine checks under anesthesia, prior to MLS.41,46,47
Observational gait analysis
While observational gait analysis (OGA) cannot replace the quantitative information gained from 3DGA, it provides a valuable assessment when a full 3DGA may not be feasible or required and plays an important role in the implementation of KS. 43 OGA can be facilitated by the use of mobile devices and standardized observational gait systems such as the Edinburgh Visual Gait Score (EVGS).44,45 For increasing efficiency, we suggest utilizing a recently published protocol that can improve accuracy using mobile device cameras and video annotation tools. 44
The most important EVGS gait measurement for KS is the maximum knee extension in stance, as this correlates best with the development of crouch gait. 44 Additional EVGS gait measurements of interest include knee flexion at initial contact, foot initial contact, heel lift, and maximum ankle dorsiflexion in stance.43 –45
We recommend documentation of peak knee extension in the stance of each limb in every KS evaluation using both the angle measurement and the EVGS grading system as follows: Grade 0 = Less than 15° flexion; Grade 1 = 15–25° flexion; Grade 2 = Greater than 25° flexion. 44
Referral to orthopedic surgery and 3DGA
A referral to pediatric orthopedic surgery and, when available, 3DGA should be made with any of the following positive findings:
Clinical history: Deterioration of gait, presence of lower extremity pain, and orthotic device intolerance.
Physical examination: The presence of an FFDKn was identified either with the SKCT or goniometer.
Observational gait analysis: Reduced peak knee extension in stance phase identified at Grade 1 (15°–25° knee flexion) or Grade 2 (greater than 25° knee flexion).
Once any of these KS-positive findings have been identified, it is the goal of the pediatric orthopedic surgeon and their team utilizing 3DGA to determine the stage and severity of MSP impacting gait function, the factors driving the development of FFDKn, and the optimal management to address the functional deterioration.5,46
Optimal treatment for knee pathology
MLS and the diagnostic matrix
Randomized clinical trials and prospective cohort studies have established that MLS in children with CP is safe and effective, improves gait function, and produces results that are durable over time.31 –33 The approach used in the preoperative evaluation of children for MLS involves the identification of all gait impairments utilizing information from multiple domains so that surgical planning and rehabilitation are optimized for the individual child, an approach known as the “diagnostic matrix” 47 (Figure 6).
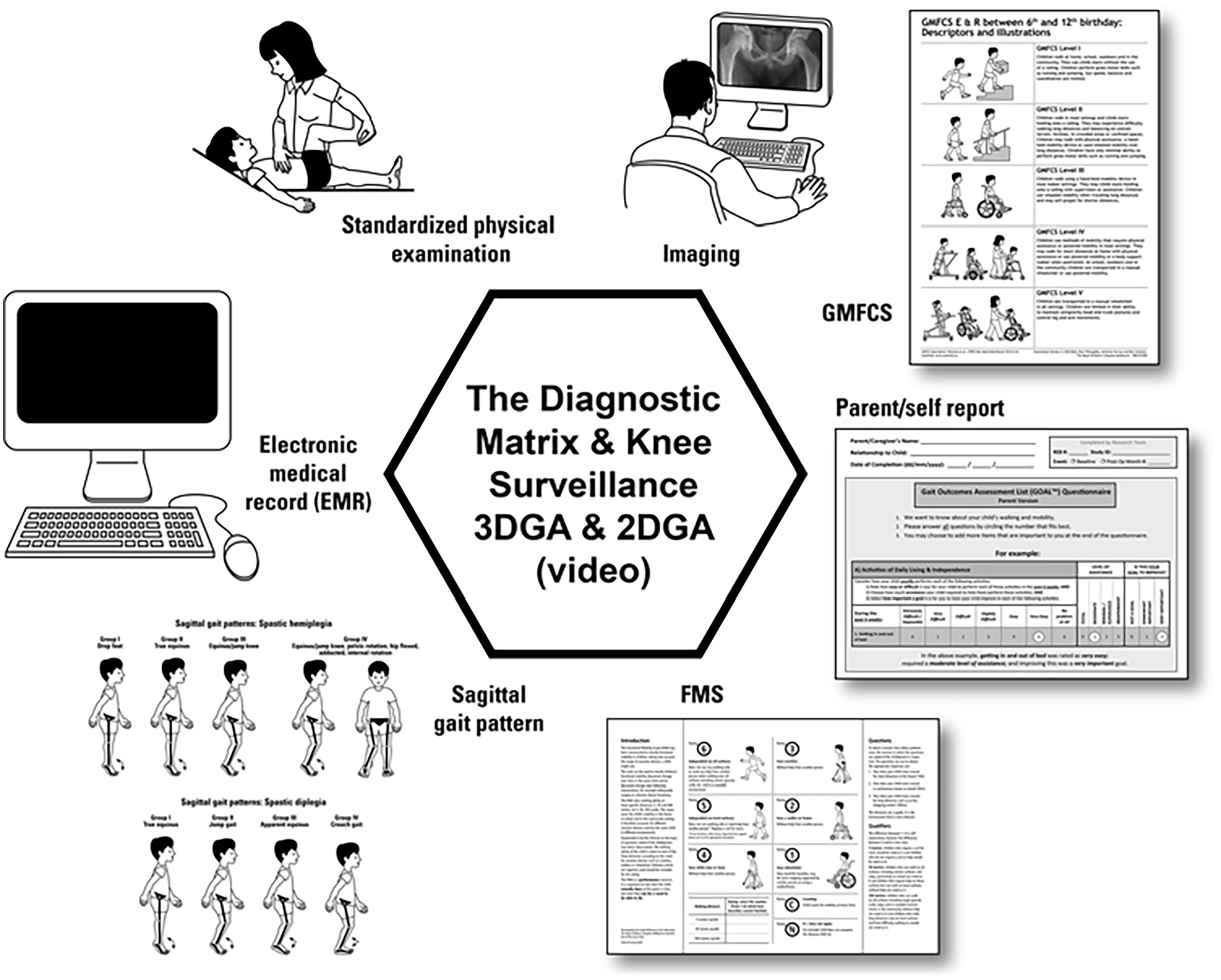
The diagnostic matrix and knee surveillance.
The diagnostic matrix includes combining information from the clinical history, standardized physical examination of the lower limbs, gait analysis, radiographic imaging, and assessment of the child and family’s goals and expectations. 47 The standardized physical exam includes a careful appraisal of static and dynamic function at all anatomic levels—spine, hip, knee, ankle, and foot. For gait analysis, we propose a combination of 2DGA and 3DGA, at key intervals tailored to the individual needs of each child.43 –45 Standardized imaging of the lower extremities should include evaluation of the hips, ankles, and feet. Additional views could include an anteroposterior long-leg standing X-ray for evaluating coronal plane deformity, lateral maximum extension views of the knees for assessing FFDKn, and an X-ray of the hand, pelvis, knee, or foot to determine the temporal relation to PHV and growth remaining. In addition to a general inquiry into the child and family’s goals and expectations, we recommend the use of patient-reported outcome measures (PROMS) such as the GOAL®. 48
Utilizing the diagnostic matrix, gait disruption can be classified by anatomic plane and by whether the gait deviation is a primary or compensatory phenomenon.14,15 The precise surgical prescription gained from the use of the diagnostic matrix targets primary gait disruptions and predicts spontaneous improvement of compensatory deviations, limiting surgical burden and producing reliable improvements in gait function. It is important to note that surgery for the knee is frequently a part of an index MLS intervention but may also be used for fine-tuning post-MLS or in the case of salvage surgery as a last resort to maintain gait and function.5,46
Important components of a successful MLS program are:
Planning based on information from the “diagnostic matrix.” 47
Assessment of the child and family goals and priorities. 48
Preparation and education of the child and family. 40
Optimal perioperative care, including multi-modal pain control. 34
Carefully planned and supervised rehabilitation. 40
Appropriate orthotic prescription. 34
Close monitoring of functional recovery. 40
Follow-up gait analysis at 12 to 24 months after MLS to ascertain the effectiveness of the intervention and to identify additional gait deviations for treatment. 31
Follow-up until skeletal maturity for new or recurrent deformities. 33
Dose-based interventions for the knee in ambulant BSCP
The surgical dose is dictated by four main factors: the MSP stage, the severity of pathology at the knee, the patient’s age, and the patient and family goals and priorities.5,46,48 We propose guidelines for knee pathology treatment in Table 2 that incorporate soft tissue surgery and guided growth for most children, reserving extension osteotomy for children with significant FFDKn who did not undergo KS and present after skeletal maturity.5,46
Dose-based soft tissue and bony surgery at the knee.
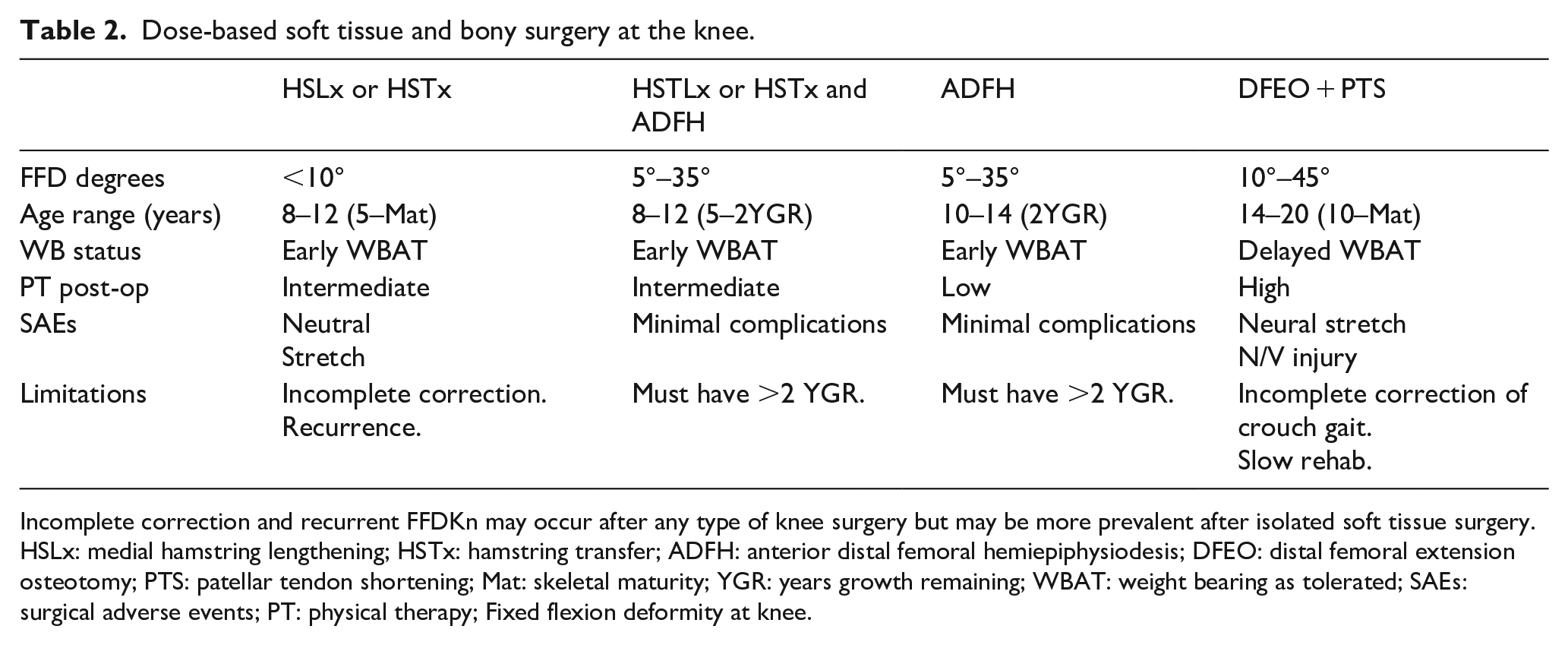
Incomplete correction and recurrent FFDKn may occur after any type of knee surgery but may be more prevalent after isolated soft tissue surgery. HSLx: medial hamstring lengthening; HSTx: hamstring transfer; ADFH: anterior distal femoral hemiepiphysiodesis; DFEO: distal femoral extension osteotomy; PTS: patellar tendon shortening; Mat: skeletal maturity; YGR: years growth remaining; WBAT: weight bearing as tolerated; SAEs: surgical adverse events; PT: physical therapy; Fixed flexion deformity at knee.
Spasticity management
Spasticity management can be focal or regional. Focal spasticity management is usually by intramuscular injection of Botulinum Neurotoxin A (BoNT-A) to the hamstrings. Selective dorsal rhizotomy is effective for regional (lower limb) management of spasticity and is effective for co-spasticity at the knee level. 2 Spasticity management for flexed knee gait is limited by the development of knee contracture, in early childhood.1 –5,7
Soft tissue surgery
Distal hamstring lengthening has been widely used for the correction of flexed knee gait in children with CP.49 –52 Distal hamstring lengthening is effective in the short term and medium term but with limitations.50,51 These include some reports of increased anterior pelvic tilt and limited benefit when there is an FFDKn. 52 The effectiveness of medial hamstring lengthening can be enhanced by optimizing postoperative care by including serial stretching of residual FFDKn by serial casting. Serial casting is effective but requires close attention to detail to avoid skin sores and nerve stretch injury. 52 The recurrence rate after hamstring surgery can be high in long-term follow-up, and revision hamstring surgery has even more limitations than index surgery. In one study, the success rate of hamstring surgery was 71% for index surgery but this dropped to 21% for revision surgery. 51
To enhance the effect of medial hamstring lengthening and to minimize the effects on pelvic position, transfer of the semitendinosus to the adductor tubercle has been reported in several studies.53 –57 Studies on hamstring transfer were heterogeneous with respect to the number of tendons transferred and lengthening of the remaining hamstrings. There is currently no consensus in the literature as to the benefits of semitendinosus transfer over conventional distal hamstring lengthening.53 –57 In our centers, we perform medial hamstring fractional lengthening without assessment of a popliteal angle intra-operatively, as this can increase the rate of overlengthening and sciatic neuropraxia. 10 Postoperative knee immobilizers and long-leg sitting are prescribed in the first 4 weeks after surgery to slowly and safely improve hamstring length, a protocol we have demonstrated improves kinematic knee function and maintains muscle strength.31 –33,40,49 We also recommend consideration of a semitendinosus transfer (STT) to the adductor tubercle as part of a medial hamstring lengthening to maintain its function as a hip extensor (Figure 7). 53 We avoid lateral hamstring lengthening in ambulant children with bilateral CP, a practice supported by recent Delphi studies seeking to establish clinical consensus.58,59 Musculoskeletal modeling is a useful adjunct to decision-making when hamstring lengthening is being considered. 60 Adding a posterior capsulotomy to distal hamstring lengthening would seem to be logical as this is where the principal restraint to full knee extension may be. However, there have been few reports in the recent literature, and we have no experience of this procedure. 61
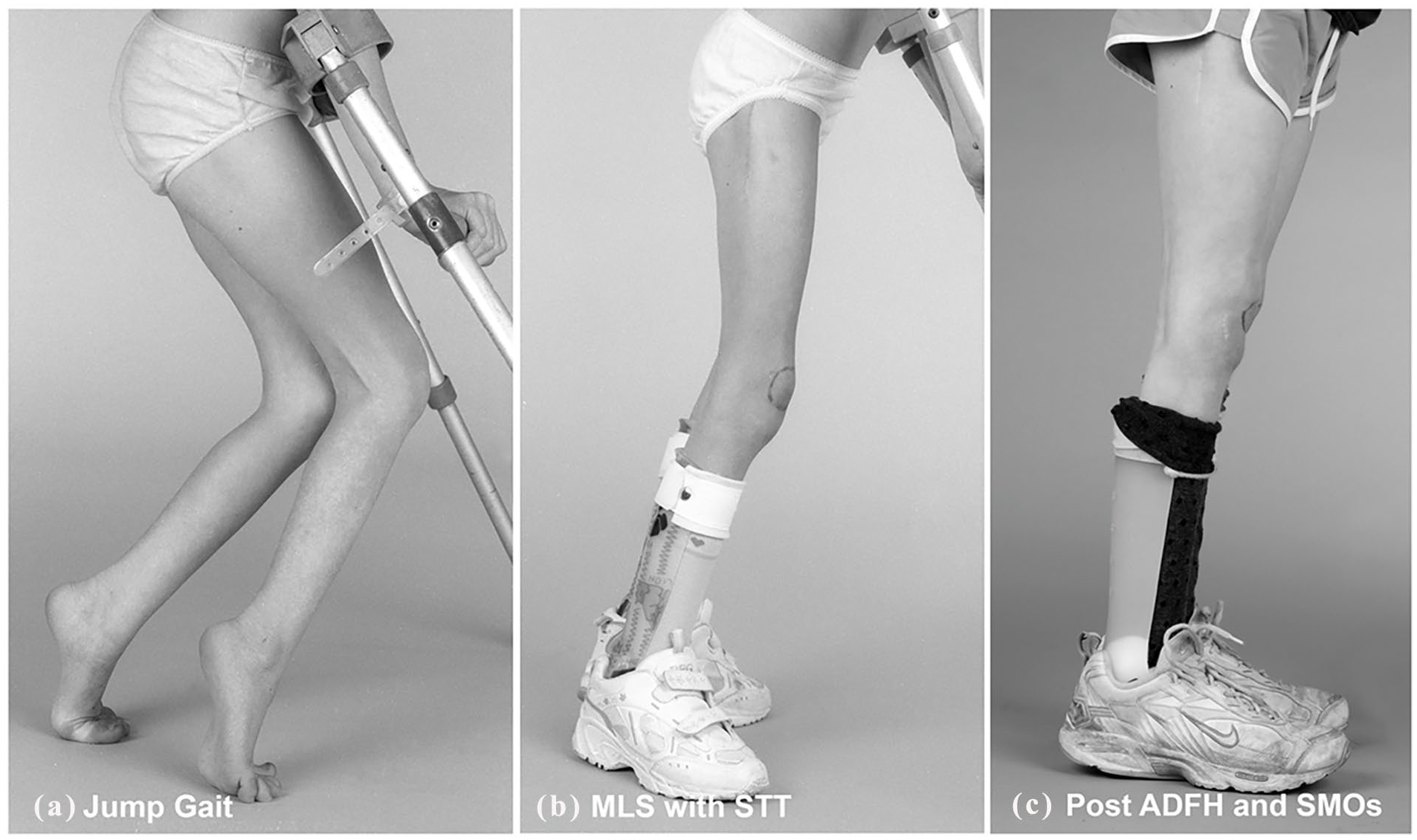
Multilevel surgery for jump gait with second-stage ADFH.
ADFH: an overview
Guided growth at the knee in the sagittal plane is usually referred to as ADFH. ADFH restricts the growth of the anterior part of the distal femoral physis by application of compression through surgical implants including staples, tension band plates, or cannulated screws.62 –69 With unopposed growth of the posterior physis creating a secondary corrective deformity, the distal femur grows into increased extension. The FFDKn corrects at a rate of 0.5°–1.0° per month in children with CP with 2 or more years of growth remaining (Figure 7).64,65
ADFH can be achieved with a range of surgical implants. Staples and 8-Plates are effective but use has been limited because of the frequency of anterior knee pain due to bursitis over the intra-synovial implants.66,67 Cannulated screws inserted through small incisions in the anterior part of the distal thigh have shown a similar ability to correct FFDKn with improved tolerance and low rates of knee pain.64,65 Non-metallic suture-anchor implants have also been described for ADFH but do have the challenge of being difficult to monitor for early implant failure due to their radiolucent nature. 68
Few adverse events have been reported for ADFH, but most studies have short-term follow-up.62 –68 Given the rapid growth of the distal femoral physis during PHV, there is the potential for both under-correction and overcorrection of FFDKn.69,70 There is also the potential for asymmetric correction, resulting in coronal plane deformities such as genu varum or valgum. 70 Close clinical and radiographic monitoring of both coronal and sagittal plane alignment is advisable in the postoperative period until skeletal maturity, including after the removal of implants. 70 The requirement for continued KS post-surgical intervention is important to build into the knee surveillance program. The relative safety of ADFH to date may relate to good surgical technique and careful follow-up by the surgeons who have innovated this procedure. A recent systematic review reported the results of ADFH in 279 patients with neuromuscular disease. 70 The mean improvement in FFDKn was 15° and with a low complication rate. In studies with gait analysis, the Gait Deviation Index improved by 8.5 points, and the minimum knee flexion angle improved by 22°.63,65,71 These improvements are close in magnitude to improvements reported after DFEO, with much lower surgical risks and faster rehabilitation.70 –75
Several studies support the combination of soft tissue surgery and ADFH which seems a logical combination to manage hamstring shortening and FFDKn.76,77 The role of simultaneous or delayed PTS is also under investigation.78,79 The optimum implants for ADFH, timing for surgery, and adjunctive procedures are yet to be determined by prospective long-term studies. 70
Timing for ADFH
The largest contribution to the length of the lower limbs comes from the distal femoral physis; however, longitudinal growth in children with CP may be reduced when compared to typically developing children (TDC).37,80,81 Muscle stiffness increases in TDC during PHV and there is anecdotal opinion that this is more pronounced in children with CP.4,82 PHV is a key period when knee contractures may increase rapidly in children with CP but also offers an opportunity for surgical correction by ADFH.3 –5,37,80,82
The window or optimum age for ADFH is very limited when compared to either soft tissue or skeletal surgery. In a systematic review, the mean age for performing ADFH was 11 years. 70 For some children, bone age may be a more reliable guide to skeletal maturity than chronological age. 71 Radiography of the hand and wrist is widely used to calculate bone age, but many other methods have been proposed. A recent review proposed that the White-Menelaus method was the best method to predict growth remaining and the timing of epiphysiodesis in children between 10 and 17 years of age. 83 It is currently not known whether the timing of ADFH would be improved using bone age rather than chronological age. However, if the child has clinical features suggesting premature or delayed onset of puberty, bone age estimations are strongly advised. There is a need for prospective research into PHV stratified by GMFCS level, to optimize decision-making regarding the timing of ADFH for ambulant children with CP. With effective KS, an FFDKn should be identified with enough growth remaining to avoid missing the opportunity for a successful minimally invasive surgery with ADFH.
Bony surgery
Prior to the routine use of sagittal plane knee correction with ADFH, the principal option for FFDKn >20° had been DFEO combined with patellar tendon advancement (PTA) or patellar tendon shortening (PTS).72 –74 These are powerful techniques and are effective in correcting both FFDKn and patella alta. They require prolonged intensive rehabilitation, are associated with significant complications, and do not always achieve long-term improvements in gait, reduction in knee pain, and improvements in health-related quality of life. 75 While this surgery remains critically important for severe FFDKn in the skeletally mature patient, we propose the introduction of formal KS to reduce or eliminate the need for DFEO with PTA/PTS, in children with 2 or more years of growth remaining.
Conclusion
We report the concept of KS in children with CP for early identification of FFDKn and gait dysfunction so that timely, minimally invasive techniques can be utilized to improve function. We propose KS every 24 months from age 5 to 9 years, every 12 months from 10 years to the onset of the pubertal growth spurt, and every 6 months thereafter until skeletal maturity. Once an FFDKn is identified, ADFH offers a minimally invasive, safe, and effective means for deformity correction and functional improvement. There is early evidence that the application of the principles of KS can permit ambulant children with CP to reach skeletal maturity with good knee motion and excellent gait function. KS is a concept that is early in its evolution and should be validated with prospective studies with long-term follow-up that include PROMS. Specifically, the efficacy of KS could be determined prospectively by an increase in the utilization of ADFH, and a decrease in the need for DFEO/PTS while aiming for optimum gait function, determined by motion analysis and PROMs.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251330448 – Supplemental material for Knee surveillance for ambulant children with cerebral palsy
Supplemental material, sj-pdf-1-cho-10.1177_18632521251330448 for Knee surveillance for ambulant children with cerebral palsy by Pam Thomason, Kerr Graham, Ken Ye, Annette O’Donnell, Vedant Kulkarni, Jon R. Davids and Erich Rutz in Journal of Children’s Orthopaedics
Supplemental Material
sj-png-2-cho-10.1177_18632521251330448 – Supplemental material for Knee surveillance for ambulant children with cerebral palsy
Supplemental material, sj-png-2-cho-10.1177_18632521251330448 for Knee surveillance for ambulant children with cerebral palsy by Pam Thomason, Kerr Graham, Ken Ye, Annette O’Donnell, Vedant Kulkarni, Jon R. Davids and Erich Rutz in Journal of Children’s Orthopaedics
Footnotes
Correction (July 2025):
Article updated with the addition of online supplemental material.
Author contributions
PT: Study conception and design, data collection and analysis, manuscript drafting and editing, and approval of the final version of the manuscript. KG: Study conception and design, manuscript drafting and editing, and approval of the final version of the manuscript. AO’D: Study design, data collection, and analysis, manuscript drafting and editing, and approval of the final version of the manuscript. KY: Study design, manuscript drafting and editing, and approval of the final version of the manuscript. VK: Study conception and design, data collection and analysis, manuscript drafting and editing, and approval of the final version of the manuscript. JD: Study conception and design, data collection and analysis, manuscript drafting and editing, and approval of the final version of the manuscript. ER: Study conception and design, manuscript drafting and editing, and approval of the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Royal Children’s Hospital Melbourne Human Research Ethics Committee (HREC) approved this study under the provisions of quality assurance: QA/51280/RCHM-2019.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.