
Abstract
Introduction:
The field of pediatric spine surgery has encountered major changes and evolutions lately, with new treatment options available and the development of enabling technologies. This article aims to summarize the most relevant recent literature.
Materials and methods:
The five most relevant topics were selected and assigned to one or two authors who performed a comprehensive Pubmed database search for articles published in the last 4 years (2021–2024). Only studies with a high level of evidence or clinical relevance were reported.
Results:
Thirty-nine articles were selected and analyzed, covering the following subjects: treatment options in tweeners, the impact of new medical treatments in pediatric spine practice, the emergence of new surgical techniques, the development of enabling technologies in scoliosis surgery, and recent relevant randomized controlled trials.
Discussion:
Many new surgical concepts and techniques have been developed lately, but their results need to be further assessed on specific subgroups of patients. Numerous significant medical improvements have been reported in the last 5 years, affecting positively the management of syndromic and neuromuscular patients.
Introduction
The field of pediatric spine surgery has encountered major changes and evolutions lately, with new treatment options (both medical and surgical) available, especially for early onset scoliosis patients, and the development of enabling technologies. Meanwhile, solid randomized controlled trials (RCT) have also been published, and any well-informed pediatric orthopedic surgeon should be aware of these high-level studies. This article focusing on the pediatric spine has been endorsed by the EPOS presidential line and aims to summarize the most relevant recent literature and also gives an objective update on the current open questions and the latest ongoing research directions.
Materials and methods
Members of the EPOS Spine study group were asked (via a survey) to vote for the five most relevant topics to discuss and analyze. After the choice was validated by the group, each selected topic was then assigned to one or two members, who performed a comprehensive Pubmed database search for all English language articles published in the last 4 years (2021–2024). Only studies with a high level of evidence or clinical relevance were reported and discussed in the context of the existing literature and the current practice.
Results
What is the most recent clinical evidence?
Relevant randomized controlled trials
Several interesting studies have been recently published concerning adolescent idiopathic scoliosis (AIS) perioperative care. A systematic review and meta-analysis evaluated the effects of chewing gum on postoperative abdominal pain and nausea in patients undergoing posterior spinal fusion (PSF) for AIS. 1 Three RCTs were included, and no significant effect was observed during the first 48 h postoperative. The length of hospital stay was not impacted either. Therefore, chewing gum does not seem to provide any significant positive effect. Helenius et al. also investigated the effects of subfascial drain (versus no drain) in a randomized trial. 2 Ninety AIS patients were included, and those with drains demonstrated a similar drop in postoperative hemoglobin compared with the no-drain group. However, the absence of drain led to 30% more opioid consumption during the first two postoperative days, while the risk of surgical site infection remained similar, so authors still recommend draining. Finally, the minimize implants maximized outcomes trial randomized 211 patients with Lenke type 1 AIS into high-density (HD, minimum 1.8 implants per vertebra) or low-density (LD, maximum 1.4 implants) constructs. 3 No significant difference was found regarding main curve correction rates (67% in the HD group versus 65% in the LD group), but pain outcomes and lumbar curve correction were better in the HD group. Revision rates were also similar, so the need and cost-effectiveness of such HD constructs remain debatable.
In the field of secondary scoliosis, Ahonen et al. investigated the risk of mortality in children with cerebral palsy and neuromuscular scoliosis (NMS) in a nationwide register cohort of 474 patients. Children who were operated for NMS had a significantly lower mortality as compared with the untreated cohort during a 5-year follow-up. The risk of cause for death due to pulmonary complications was five times higher in the untreated cohort. 4
Finally, in another controversial field of pediatric spine, Virkki et al. 5 prospectively evaluated the effects of rigid thoracolumbar orthosis versus placebo for acute spondylolysis in 57 adolescents, all active in different sports. The study started as a randomized clinical trial but ended in a patient preference design due to difficulties in enrollment. Magnetic resonance imaging images showed bony union in two-thirds of these patients after 4 months of sports restriction, without any difference between groups. The authors therefore concluded that rigid orthosis did not appear to be necessary in the treatment of acute pediatric spondylolysis.
Tweeners: a new subgroup of patients with specific treatment options
Based on a consensus statement, the term “early onset scoliosis” (EOS) was uniformly defined in 2015 as any deformity of the spine diagnosed before the age of 10, independent of the etiology. Due to the evident fatal effects of a short and stiff thoracic spine on pulmonary function, the long-standing principle of early corrective spinal fusion in EOS has been replaced by emerging growth-friendly surgical concepts. However, the initial enthusiasm for growth-friendly options, even when using implants without the need for repetitive surgical lengthening, has faded over time due to the reported high complication and reoperation rates. Apart from reviving conservative treatment approaches, such as serial casting, this has also re-stimulated the debate about the appropriate timing for primary definitive spinal fusion, especially in older, biologically, and skeletally more advanced EOS patients, who are often included in the so-called “tweener” population.
In 2023, a three-round survey to define the term “tweener” provided consensus (≥70% agreement) among international EOS experts regarding chronological age, as well as the inclusion of Sanders maturity stage (SMS). 6 This study suggested that the definition for this subgroup included open triradiate cartilage (TRC), SMS <4 with a chronological age between 8 and 10 years in premenarchal girls, and a chronological age between 9 and 11 years in boys.
While for the “tweeners,” both growth-friendly approaches and early definitive fusion can be considered, patients with SMS ≥4, closed TRC, and postmenarchal should preferably undergo primary arthrodesis.6,7 A recently published consensus study evaluated treatment options for EOS. 8 In 2010, experts were asked to select the treatment choice they believed would lead to the best clinical outcome in a collection of 315 theoretical EOS case scenarios. Ten years later, in 2020, the same surgeons were invited to re-evaluate the same cases. Overall, conservative treatments had the largest increase in frequency, while distraction-based methods had the largest decrease. Due to the known risks of complications following EOS procedures, surgeons appear more likely to avoid and postpone surgery as much as possible. There was only a little increase in the frequency of primary arthrodesis, most likely due to the previously mentioned evidence of poor pulmonary outcomes and high complication rates. Accordingly, the increase in the frequency of early posterior fusion was predominantly seen in older EOS patients, who are now included in the tweener group, particularly those with NMS. So far, these findings mainly represent expert opinions and are not yet evidence-based but underline an apparently lower threshold for a primary definitive spinal fusion in this age group.
What are the ongoing research projects?
Impact of new medical treatments in the pediatric spine practice
Significant progress has been made in recent years, with several promising strategies transitioning from experimental research to clinical practice. Newly implemented treatments for specific pathologies have affected the development and course of spinal deformities in several groups of patients.
Adolescent idiopathic scoliosis
The roles of genetics, neurosensory abnormalities, biomechanics (intervertebral disc), and metabolism in the etiology of AIS are still being investigated all around the world. Within the metabolism category, melatonin and vitamin D have been topics of interest. Melatonin deficiency is known to disturb the symmetrical development of paraspinal muscles, and serum vitamin D levels have been positively correlated with bone mineral density and negatively correlated with Cobb angle. In this respect, it has been postulated that vitamin D insufficiency or deficiency, which may be due to its regulatory effect in calcium-phosphorus metabolism, may play a role in the etiopathogenesis of AIS. 9 Melatonin and vitamin D levels have been demonstrated to be lower in progressive AIS patients compared with controls. 10 Herdea et al. also reported that the progression rate could be slowed down with vitamin D, calcium, and melatonin supplementation in their prospective randomized case–control study of 51 patients. 10 Nevertheless, these findings still need to be validated in larger populations and multicenter studies before being implemented in clinical practice.
Osteogenesis imperfecta
Osteogenesis imperfecta (OI) patients have a noticeably higher risk of developing scoliosis compared to the general population, due to bone fragility, ligamentous laxity, muscle weakness, pelvic obliquity, limb-length discrepancy, and altered vertebral body shape. Treatment with bisphosphonates can promote both vertebral remodeling and increased bone density. When started before the age of 6, bisphosphonate therapy has been demonstrated to modulate curve progression in patients with type III OI. Nevertheless, further investigation was unable to corroborate this observation. 11 This result is not surprising since other soft tissue-related pathologies that also contribute to the deformity persist. There is no evidence that treatments like denosumab and recombinant human parathormone, which have been used recently, impact the course of the spinal deformity, even though it is known that they lower the risk of fracture. 12 However, their use has been limited in children due to potential side effects (hypocalcemia for denosumab and neoplastic risks for teriparatide). Even though new treatments like gene therapy, anti-RANKL antibodies, sclerostin inhibitory antibodies, and mesenchymal stem cells have been shown to improve bone quality in small groups of patients, there are still concerns with their use in the pediatric population.
Mucopolysaccharidosis
In mucopolysaccharidosis (MPS), the progressive sagittal plane deformity is triggered by failures of ossification in the anterosuperior regions of the vertebrae at the thoracolumbar junction. The presence of ligament laxity combined with odontoid hypoplasia or absence exacerbates the instability in the upper cervical region, and the accumulation of glyco-amino-glycans thickens the dura, which worsens the compressive symptoms. The quality of life is significantly impacted by neurological deficits resulting from deformity and direct cord compression. Enzyme replacement therapy (ERT) and hematopoietic stem cell transplantation (HSCT) have proved to have a positive effect on the clinical manifestation of MPS patients, improving their quality of life and slowing down the disease’s progression, especially if started early. 13 However, spinal symptoms respond poorly to current systemic treatments. While the risk of spinal deformity development and progression does not decrease in patients receiving ERT and HSCT treatment, their longer survival time results in a greater need for spinal care. New therapies need to be designed to specifically target pathology in a tissue-specific manner.
Duchenne muscular dystrophy
Patients with Duchenne muscular dystrophy (DMD) are diagnosed around the age of 4, become non-ambulatory usually in their early teens, develop scoliosis after becoming wheelchair dependent, and pass away in their third or fourth decade of life. Since DMD currently has no known cure, the primary goal of the management is to enhance patients’ quality of life. Through a number of mechanisms, glucocorticoids prolong ambulation, improve cardiac and pulmonary functions, and slow the functional decline of DMD patients. 14 They may also lower the risk of progressive spinal deformity. In two distinct time periods, the Toronto group demonstrated that glucocorticoid treatment slowed down the progression of scoliosis and reduced the number of spine surgeries in DMD patients. 15 However, in a comparative study that reflected the clinical experience of a single center, Sussman et. al. stressed that the effect of glucocorticoids on the progression of scoliosis was not as pronounced as previously reported. 16 The most remarkable result was that the same level of functional improvement could be achieved with the use of Deflazacort instead of prednisone, with fewer side effects. Although newly approved drugs such as Edasalonexent have been demonstrated to lead to some functional improvements in the treatment of DMD, no published clinical study has yet to show how these treatments affect spinal deformity. 17
Spinal muscular atrophy
There have been some ground-breaking advancements in spinal muscular atrophy (SMA) treatment in recent years. The advent of Nusinersen, Risdiplam, and gene therapy (onasemnogene abeparvovec) have prolonged patients’ lives and improved their functional abilities. 18 SMA1 patients (who previously died in the first year of life) now have a far higher chance of surviving and becoming more visible in the field of orthopedic surgery. 19 Similarly, some SMA2 patients who would have previously spent their entire lives confined to wheelchairs can now keep a walking ability. Numerous studies have investigated the impact of these novel treatments on the onset and evolution of spinal deformity in recent years. Patients with SMA1 who received gene therapy did not have a lower risk of developing spinal deformities; in fact, in contrast to other SMA types, a deformity pattern dominated by thoracic hyperkyphosis was observed. 19 Nusinersen is the treatment with the longest follow-up and the highest research attention. Muscle function and motor control improvement have been reported in the appendicular skeleton, but this effect has not been observed in the axial skeleton. There are even concerns that a patient’s upright posture could increase the risk of developing a spinal deformity. While some research suggests that early treatment (before age 5) could help reduce the rate of progression, the evidence for these claims remains weak. 20 Currently, there is no published literature on the effect of Risdiplam, notable for its ease of use, on the development of spinal deformity. In conclusion, despite all these exciting advancements, it is still impossible to claim that any novel specific treatment can completely prevent the onset or stop the progression of spinal deformity. There is still hope, though, that much better outcomes in this field will be achievable soon.
Emergence of new surgical techniques
The growth modulation techniques aiming to preserve chest growth and lung development can be divided into three main groups: (1) growth guided (Shilla, Luque trolley), (2) distraction based (traditional or magnetically controlled growing rods, vertical expandable prosthetic titanium rib (VEPTR) and (3) tension based (spinal stapling and tethering). All these procedures still have a high complication rate despite the latest “upgrades.” Recently, several innovative techniques have been introduced that may improve our practice.
Regarding growth guidance, Agarwal et al. introduced the active apex correction (APC) as an alternative to the Shilla technique, based on compressed pedicle screws (PS) on the convex side, above and below the wedged apical vertebrae. 21 In a comparative study between APC and traditional growing rods (TGR) for the treatment of 46 patients, they found equivalent mid-term clinical outcomes, with 2 times fewer complications in the APC group (50% for TGR versus 25% for APC). In 2024, the same group published the results of a prospective multicenter clinical study of 24 patients with more than 2 years of follow-up and confirmed the promising results (spine length, curve correction, complications, unplanned surgeries). However, the biomechanical complication rate was 37%, and concerns have been raised within the spine surgery community regarding the postoperative sagittal alignment obtained with APC. 22
In 2021, Wijdicks et al. introduced a new distraction-based technique called the spring distraction system (SDS) (Figure 1), which consists of compressed springs mounted around conventional sliding rods, providing an active continuous distraction, enhancing growth and further deformity correction without the need for additional surgery. 23 In 2022, Tabeling et al. presented the results of a prospective clinical trial using an improved version of the SDS. 24 In this cohort of 17 patients with various etiologies (mean age of 9.5 years old), SDS yielded 50% of initial correction, which was maintained at follow-up, and spinal growth was near physiological. SDS was associated with reduced severe adverse effects and unplanned return to the operating room, while patients’ quality of life improved. The presented instrumentation has the advantage of using 5.5 mm diameter rods, and three options of springs with different loading capacities (50, 75, and 100 N), allowing us to choose the appropriate rod dynamization onto the concavity or convexity of the curve.
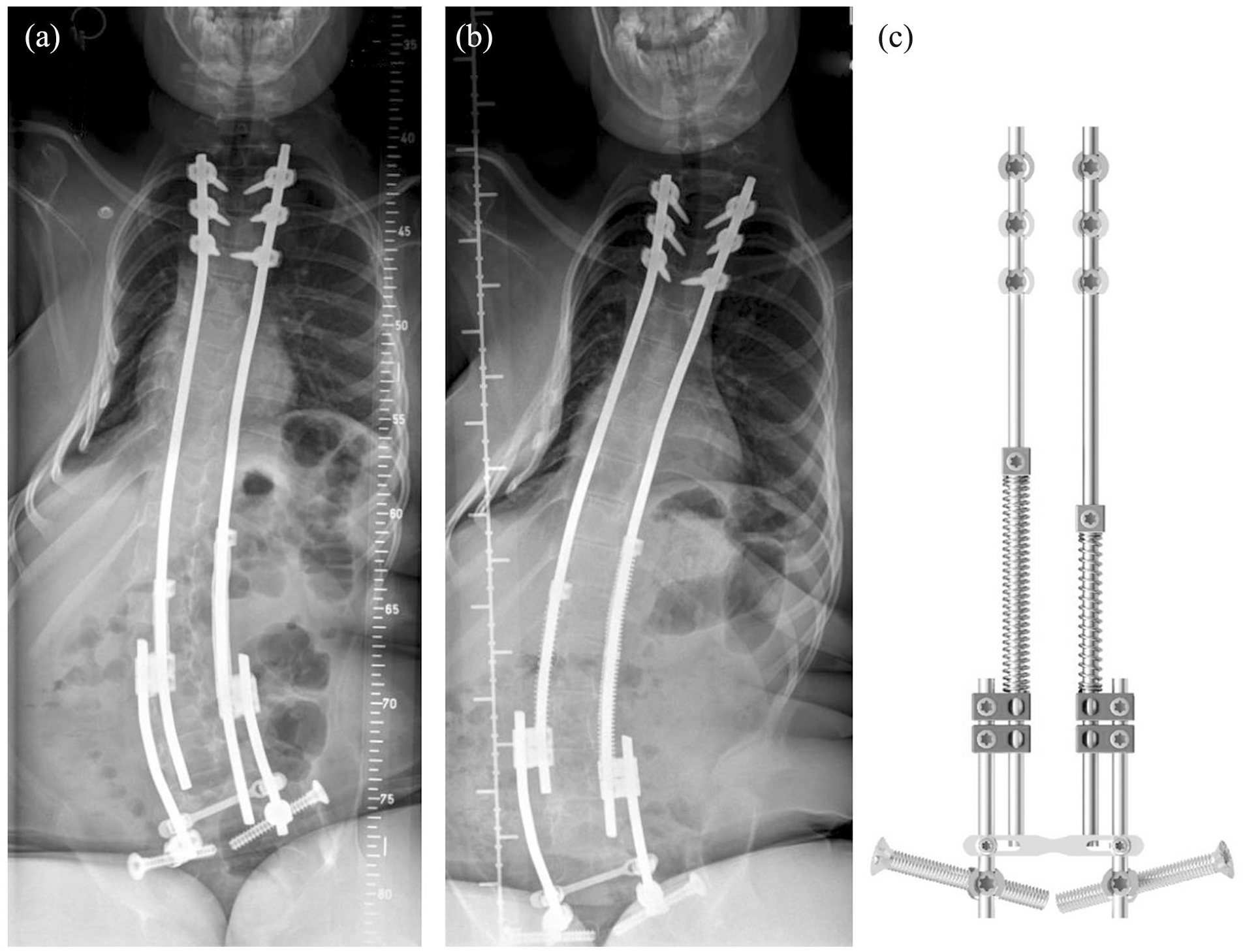
An early postoperative radiograph (a) of a 9-year-old SMA2 patient with bilateral SDS with iliosacral fixation. At a 2-year follow-up (b), spinal length gained 3 cm. Fifty and 100 N springs were used in the construct (c).
The bipolar technique is another distraction concept initially described for NMS, relying on a bilateral rod construct that can be lengthened every 12–24 months, and eventually remain in place (Figure 2). It is anchored proximally by four hook claws and distally to the pelvis by iliosacral screws. The promoter initially reported a 61% correction rate and a 7-cm T1S1 length increase at a 3-year follow-up in a heterogeneous group of young NMS patients (mean age 11). Despite a complication rate of 26%, none of these patients underwent definitive fusion and according to the authors, the technique showed to be safe and effective. In 2021, the technique was modified with a ratchetted one-way self-expanding rod, and the early clinical results of 20 patients (10 NMS and 10 non-NMS) were presented. 25 A unilateral single rod construct was inserted in the non-NMS group and a bilateral rod construct was used in the NMS group, with a 10-min traction session performed every month. At the latest examination, the rod expanded in all NM patients, but not in 50% of the non-NM group that required additional surgery. Further investigation therefore remains necessary, but this technique might be considered in fragile patients with poor general conditions.
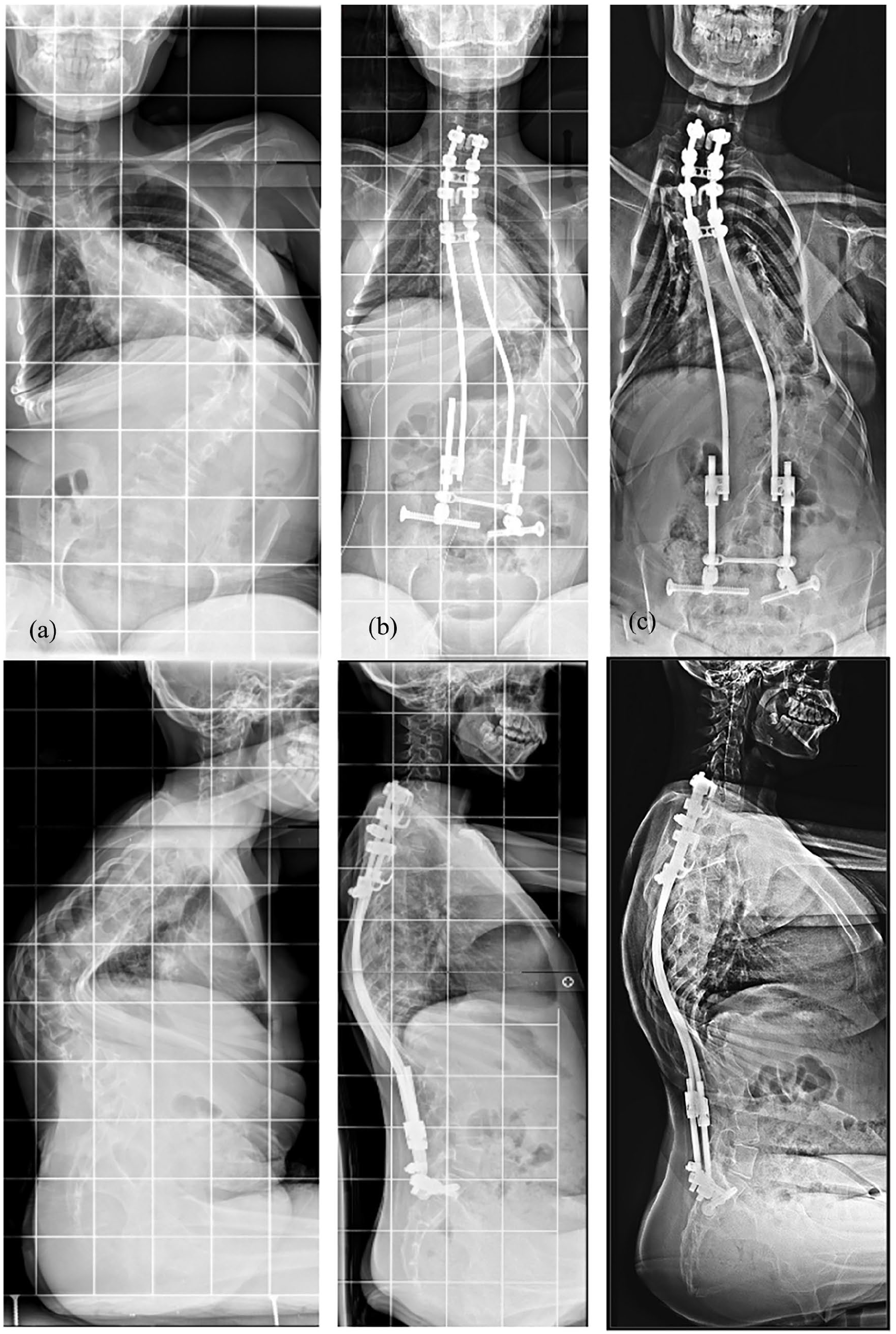
Preoperative (a), postoperative (b), and 4-year follow-up (c) of neuromuscular scoliosis treated by the bipolar technique.
Anterior vertebral body tethering (VBT) is a tension-based technique that has been a hot topic lately, with many small and heterogeneous series, but the most fervent followers often describe the procedure as less invasive and less morbid than posterior fusion. 26 Canbolat et al. randomized 31 patients with AIS into VBT and PSF. 27 Postoperative morphine consumption and numerical rating scale scores during the first 48 h postoperatively were significantly higher in the VBT group. Similarly, the intensive care unit and the hospital length of stays in the VBT group were significantly longer. Although perioperative blood loss was significantly higher in the PSF group, pain at discharge, and patients’ satisfaction were similar between groups. The authors therefore concluded that the VBT mini-thoracotomy approach required more active pain management in the early postoperative period.
Surgeons also recently explored the potential of posterior VBT for lumbar curves. The rationale for this strategy is that the mobility of the lumbar spine is most relevant, the posterior approach is well known, the lordotic effect of a posterior tether is preferable over a kyphotic effect, and release or correction is much easier from the posterior. In a retrospective study, Siu et al. reviewed 14 patients (mean age 11.6 years) with Lenke 1C, 3C, and 6 scoliosis who received anterior VBT for the thoracic and posterior VBT for the lumbar spine. 28 The initial frontal lumbar correction was about 60%, and further improved at 2 years postoperative, while lumbar lordosis remained unchanged. Surgical time was long (420 min) and 50% required reoperation for the lumbar tether, often due to overcorrection. However, the authors concluded that despite a high complication rate, the combined approach was a valuable alternative to fusion. In a recent and limited case series (three patients) with short follow-ups, Mineiro et al. also showed effective use of unilateral posterior tethering for lumbar curves. 29 Based on the literature and their experience, the authors recommended a strict selection of patients with flexible 5C curves <60° and Sanders 3–5. The most recent paper on posterior VBT is from Metaizeau et al., who retrospectively reviewed 22 AIS patients with flexible Lenke 5C curves (35° to 60°). 30 The average initial frontal correction was about 50% and the curves further improved during follow-up, while sagittal alignment remained respected. However, this was at the cost of many reoperations, including material removal and/or final fusion, so the authors concluded that this technique was promising, but required a learning curve and optimization of technique and selection.
More literature is available for anterior VBT of the lumbar spine which has been practiced often in combination with thoracic VBT. Boeyer et al. reported a 50% correction rate at 2-year follow-up in 28 Lenke 5C patients. 31 One severe complication (ureter damage) was recorded, as well as four reoperations, and two more patients ended up with a curve >40°. Results were considered successful in 75%, despite a 57% rate of broken tethers. Even with a significant follow-up of 44 months, the authors remained careful with long-term conclusions and modestly pointed at the success rate of 50% for uncomplicated courses. Similarly, Trobisch et al. recently reviewed 35 immature patients (Sanders <7), with more than 2-year follow-up. 32 Mean frontal correction was 50%, and although they observed tether breakage in 90% of patients, the reoperation rate was low and only two patients were revised (6%). Despite interesting concepts, all the above new developments still require longer-term studies to better understand the sustainability of the clinical and radiographic outcomes, as well as the efficacy of the procedures in the long run. In general, the initial enthusiasm seems to decrease when the follow-up increases, but a revision with posterior fusion remains possible in case of poor outcomes, despite the presence of lateral screws in the vertebral body (Figure 3).
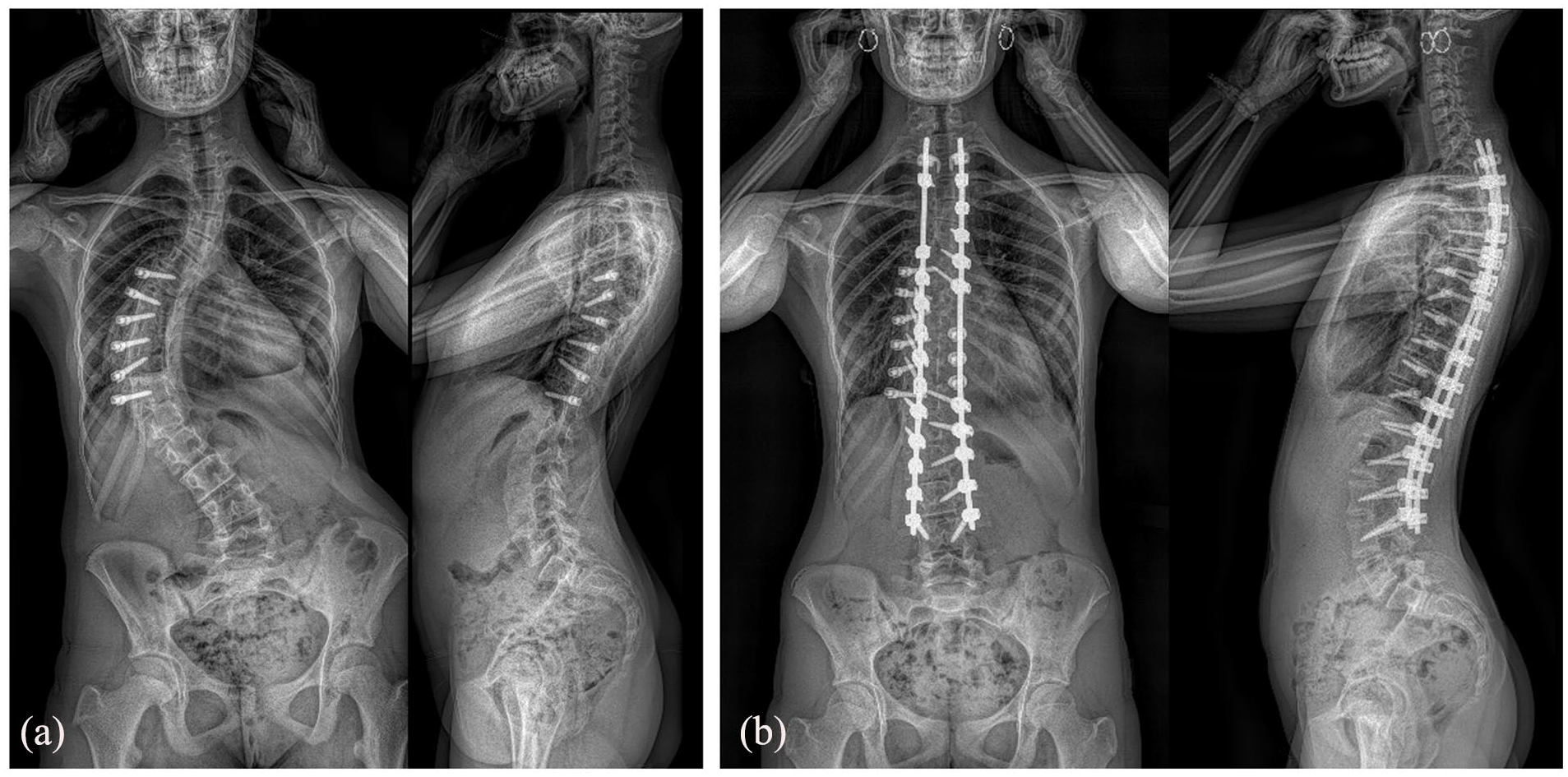
Poor results 1 year after anterior VBT (a) in a 15-year-old girl, revised with T2L3 posterior fusion (b).
What is the future direction?
The development of enabling technologies in scoliosis surgery
Enabling technologies have gained popularity in spine surgery and among the deformity community in the last 5 years. Their use rapidly spread out in adult degenerative surgery, but they are now invading the pediatric practice as well, and some recent evidence can be found about the increased intraoperative safety they provide. Ansorge et al. reviewed the literature on PS placement accuracy using the latest technologies and concluded that the lowest misplacement rate was obtained with robotics (0.4%–7.2%), compared to computed navigation (1.9%–11%) and to free-hand technique (1.5%–50.7%). 33 However, they emphasized that PS misplacement-related complications remained extremely rare for every technique, while robotic and computed navigation induced a significant increase in intraoperative radiation exposure. The authors, therefore, recommended dedicating robotic and computed navigation for complex deformities or revisions with altered landmarks. Interestingly, they also underlined that higher misplacement rates, ranging from 22.2% to 31.5%, were still reported in narrow and dystrophic pedicles, so further studies in complex pediatric deformities are still required. The main issue is that these narrow dysplastic (grade C) or fully corticalized (grade D) are frequent in pediatric scoliosis exceeding 75°, as reported by Chiu et al., especially at L1 and L2, and on the concave side of the thoracic curves. 34
Akazawa et al. also confirmed the superiority of robotics over navigation, in a series of 50 AIS, but the mean main Cobb remained moderate (50° on average), limiting the impact of their conclusion. 35 Not surprisingly, they also noted a higher deviation rate (22.4%) in grade 4 pedicles (<1 mm inner diameter). The most relevant published studies are therefore those focusing on “complex” pediatric deformities, associated with higher complication risk and for which the surgeon’s experience plays a major role. Kothari et al. investigated the benefit of O-arm navigation in 21 patients (all etiologies) with Cobb angles between 65° and 103° and concluded that it reduced the incidence of medial and inferior “critical” (i.e., >2 mm) PS breaches. 36 However, no control group was included in that study. McCormick et al. also recently presented their experience with robotics in spinal deformities, with a consecutive series of 100 complex multilevel posterior fusions (all ages), including 31 revisions. 37 Mean operative time was 303 min, and the failure rates (defined as hardware breakage) of PS and S2AI were 1.7% and 5.7%, respectively. However, no screw malpositioning was reported and the infection rate remained low compared to historical controls. Finally, the most significant pediatric series of scoliosis operated with robotic assistance has been published by Boston’s Children Hospital team, which showed an impressive rate of 99.6% of PS implanted successfully. 38 Interestingly, they also explained how their operative technique had been modified by the technology and described two major changes that helped increase safety and efficiency. First, they started to use high-speed navigated drills to avoid skiving, and second, they decided to drill all pilot holes robotically, before inserting implants, to reduce motion and avoid registration loss. In addition to AIS, which is probably the best situation to learn how to use robotics, indications will probably extend in the future to more complex cases in which some surgical steps remain challenging even for humans. For example, placing without fluoroscopy and in a seamless way long S2AI screws in the asymmetrical pelvis of a neuromuscular patient is clearly a benefit (Figure 4). Similarly, the ability to perform safely (still without intraoperative radiation) a high-density construct in a syndromic patient with very dystrophic vertebrae will dramatically increase the surgical team’s confidence during the procedure (Figure 5).
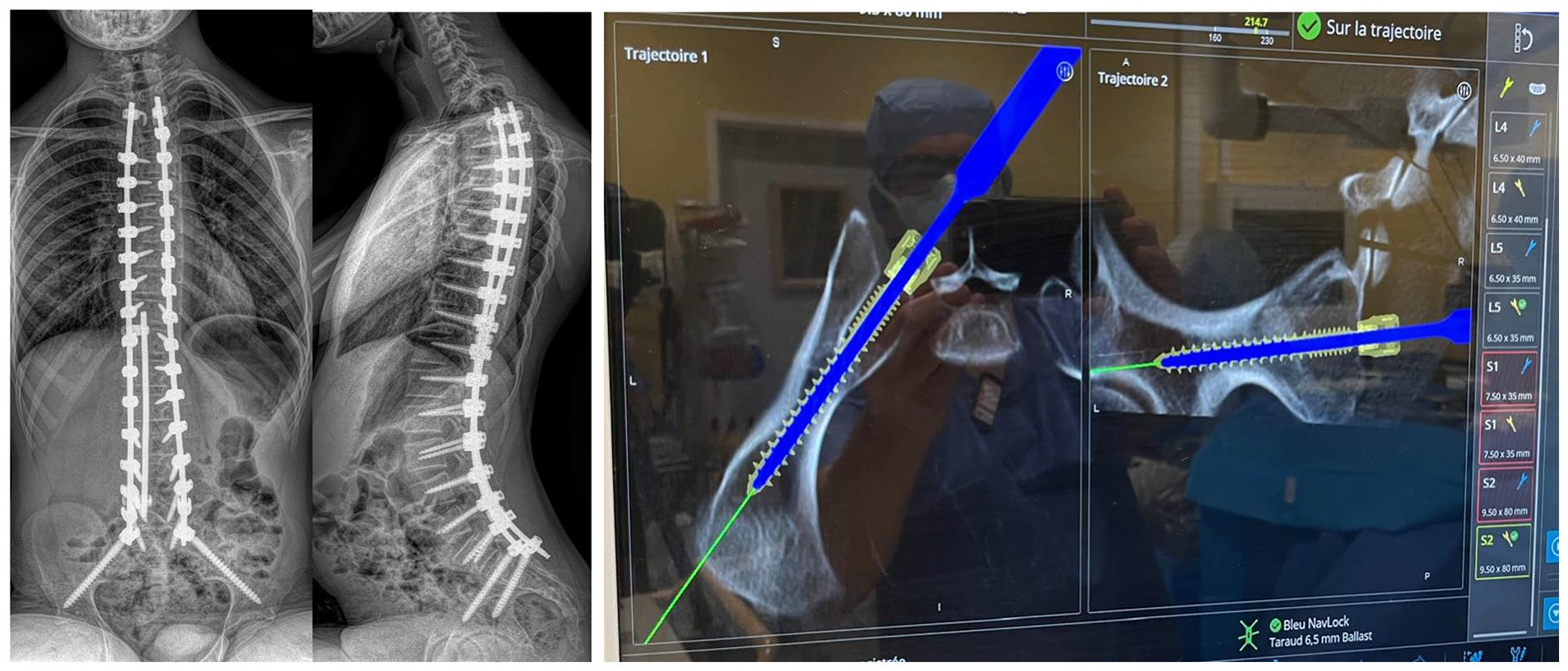
Anteroposterior and lateral postoperative radiographs of a 16-year-old patient with Friedreich’s ataxia who underwent S2AI screw insertion with robotic assistance.
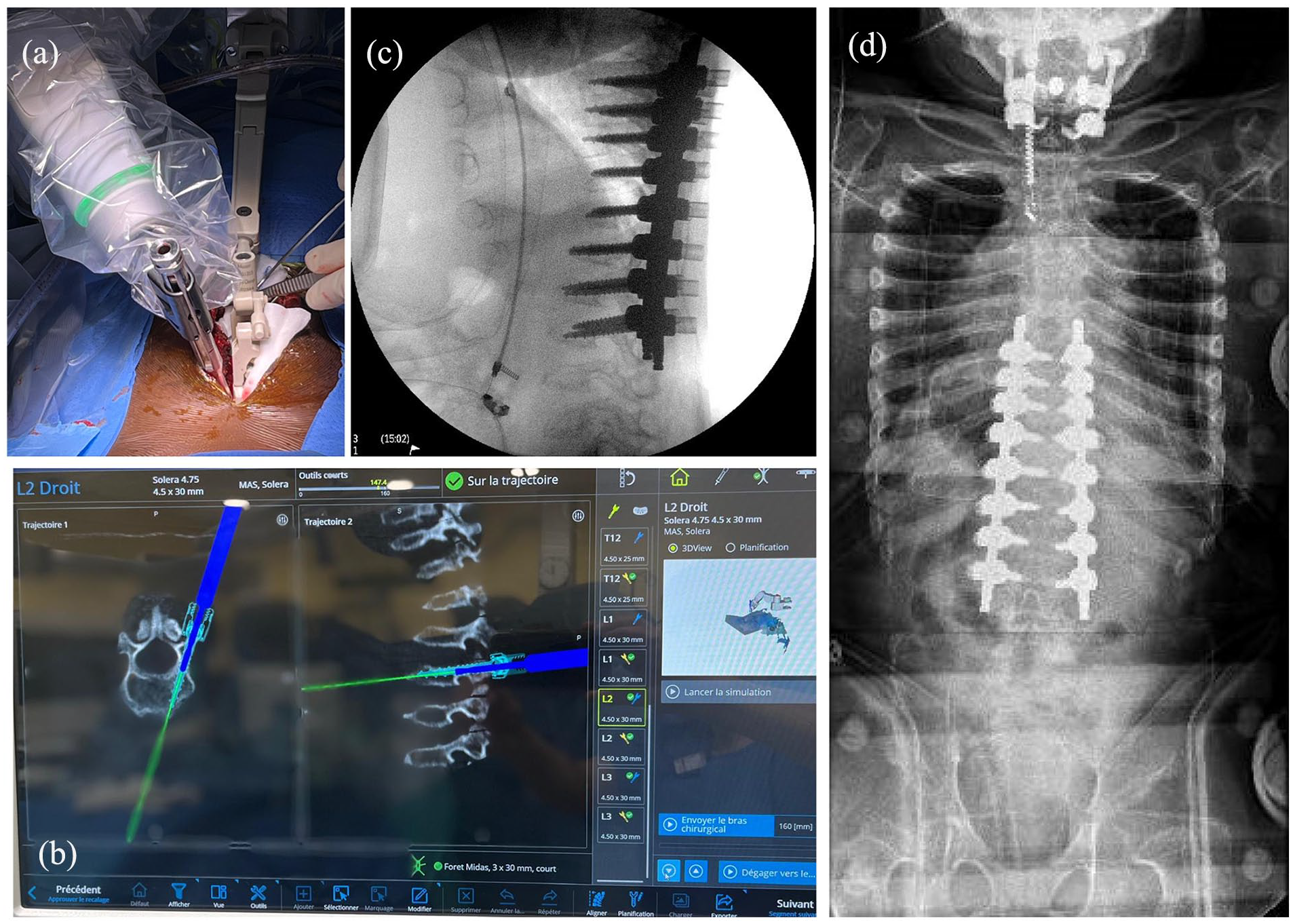
T8L3 posterior fusion was performed on a 9-year-old MPS patient. The procedure was performed via a 15 cm incision (a), and navigation was used to control screws trajectory (b) in such dystrophic pedicles, but excellent lateral (c) and frontal (d) corrections were obtained in less than 4 h.
All these enabling technologies, combined with a patient-specific approach (operative planning and prebent rods), are clearly going to impact and improve our practice in the next decade, but the cost–benefit analysis of such advances will probably be discussed in the future to support the major investments requested. 39
Three-dimensional AIS classification
Another major evolution that will affect our practice is the new 3D AIS classification, currently being developed by the SRS 3D Task Force under the leadership of Carl-Eric Aubinand Larry Lenke (Figure 6). Work began several years ago, to produce a 3D AIS classification system that would be clinically understandable, useful, and available to both SRS members and the global scoliosis community. Although interesting progress has been made, it is only recently that barriers to obtaining and disseminating this classification have been lifted. The new 3D classification will be obtained automatically and based on the sub-analysis of the three curves (proximal thoracic, main thoracic, and lumbar) composing each deformity in the three anatomical planes, including the axial plane. Completion is expected within the next 12 months, with further details to be revealed.
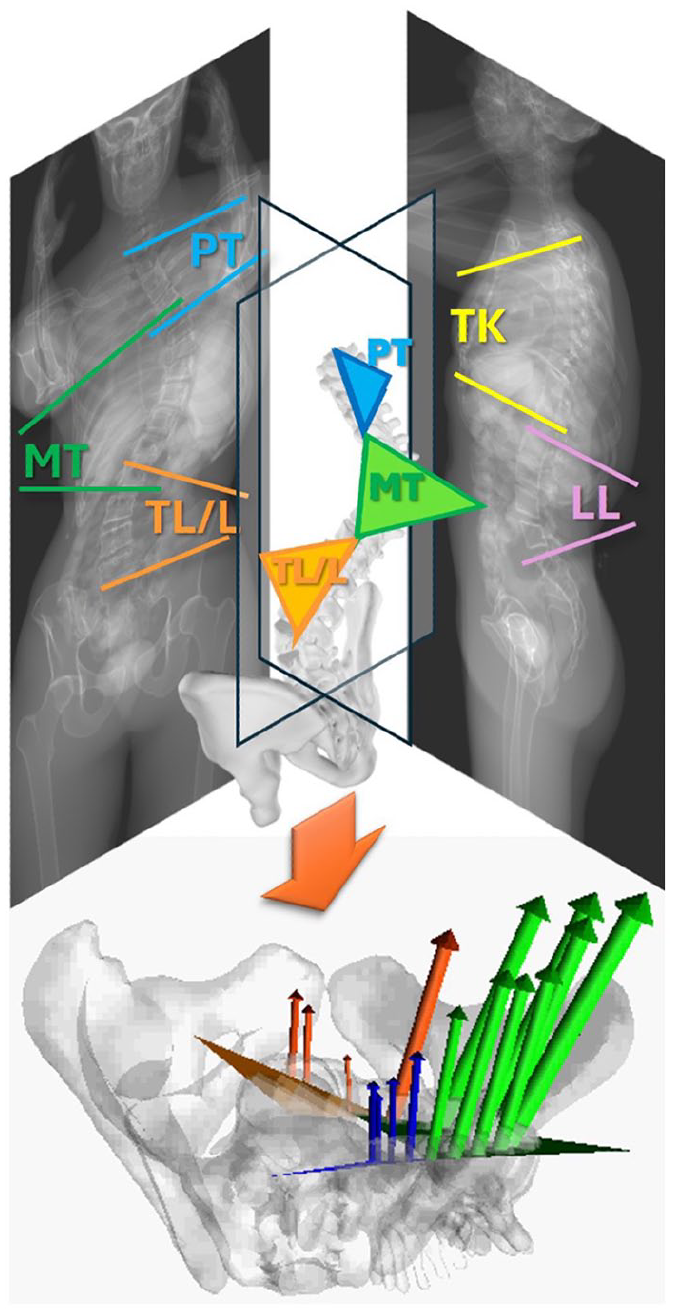
Concept of the new 3D AIS classification, in which each scoliotic curve will be divided and sub-analyzed into three components (proximal thoracic, main thoracic, and lumbar). The orientation in the transverse plane and the apical rotation of each component will be automatically calculated and reported.
Conclusion
In conclusion, many new surgical concepts and techniques have been developed lately, but their results need to be further assessed on specific subgroups of patients. “Tweeners” are definitely the population with the widest variety of options, so there is a need for high-level comparative prospective studies. Enabling technologies are now part of the 4.0 surgical environment, and the spine community needs to better understand their strengths and current limitations. Finally, pediatric spine surgeons should be aware of all the recently published RCTs but also be informed of the numerous significant medical improvements that have been reported in the last 5 years, affecting positively the management of syndromic and neuromuscular patients.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241309531 – Supplemental material for What’s new in the pediatric spine?
Supplemental material, sj-pdf-1-cho-10.1177_18632521241309531 for What’s new in the pediatric spine? by Brice Ilharreborde, Ilkka Helenius, Daniel Studer, Carol Hasler, Moyo Kruyt, Jorge Mineiro, Dror Ovadia, David Farrington, Sebastien Pesenti, Muharrem Yazici and EPOS Spine Study Group in Journal of Children’s Orthopaedics
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Brice Ilharreborde: Paid consulting for Medtronic and Implanet.
Ilkka Helenius: Paid consulting for Medtronic, Globus, and Nuvasive.
Daniel Studer: No COI.
Carol Hasler: No COI.
Moyo Kruyt: Grants from Stryker, Nuvasive, and Kuros Biosciences; Co-founder of Cresco startup company to valorize Sping Distraction System (CDS).
Jorge Mineiro: No COI.
Dror Ovadia: No COI.
David Farrington: No COI.
Sebastien Pesenti: Paid consulting for Stryker and Implanet.
Muharrem Yazici: No COI.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.