
Abstract
Background:
The one-bone forearm procedure has been considered as a potential treatment for severe forearm deformities. However, its primary limitation lies in the elevated risks of nonunion and infection. In order to enhance union rates, a technical modification was introduced, aiming not only to establish end-to-end radio-ulnar fixation but also to incorporate an additional overlay and fixation between the proximal and distal radius osteotomy stumps. This technique, initially applied in a heterogeneous patient population including individuals with neurological, tumoral, and congenital conditions, yielded promising results, achieving a consolidation rate of 100% and enabling supination corrections of up to 120°.
Methods:
In this study, we present a retrospective cohort of 28 patients, with an average age of 9 years, all afflicted by forearm supination contracture exceeding 90° secondary to neonatal brachial plexus injury. These patients underwent treatment with the modified technique.
Results:
The mean correction achieved in forearm rotation was 116°, and the average follow-up period extended to 43 months. Remarkably, all patients exhibited bone union within an average period of 6.6 weeks, without any complications.
Conclusion:
Our findings underscore the efficacy of this modified technique, which enables substantial rotational corrections, boasts a high union rate, and maintains a low incidence of complications. This approach is particularly valuable for young patients suffering from neonatal brachial plexus injury with severe fixed supination deformities.
Case series, Level of evidence:
IV
Introduction
Forearm supination contractures are a source of functional and cosmetic impairment in children suffering from neonatal brachial plexus birth injury (NBPI).1 –4 Several surgical techniques have been described to treat these forearm supination deformities, with the one-bone forearm (OBFA) procedure indicated for severe fixed rotational deformities. 1
OBFA improves upper limb function, enabling the performance of tasks requiring supination or marked pronation through compensatory rotations by other upper limb joints. 5 Risks such as nonunion, fracture, and radial head impingement are significant concerns associated with this technique.6,7 To mitigate these risks, Dr. Kozin has recently developed a novel technique for treating severe fixed rotational deformities in patients without forearm bone defects (NBPI, neurological disorders, and multiple hereditary exostoses).
The technique involves creating an overlay between the proximal and distal radius osteotomy stumps, with slight forearm shortening allowing for further rotational correction and increased bone contact and stability. 2
In this report, we present a retrospective cohort of patients with fixed severe forearm supination contractures treated using this technique in the specific context of NBPI. All patients were operated on by the same surgeon (FS).
Material and methods
Parents provided informed consent following the Declaration of Helsinki guidelines for biomedical research involving humans. The study was approved by our institution’s Institutional Review Board. A retrospective analysis was conducted on children with residual NBPI who underwent OBFA (Kozin’s technique) from June 2014 to July 2022. Inclusion criteria consisted of residual NBPI with severe rigid supination deformities, the presence of active wrist extension, or, if absent, availability of the flexor carpi ulnaris for simultaneous transfer to the extensor carpi radialis longus, and a sensate hand (Kozin THUS techniques for hand and upper surgery, 2006).
Nine patients underwent surgery abroad during surgical missions. Medical records were reviewed for demographic information, level of palsy at birth (C5–C6 or Erb’s Palsy, C5–C6 ± C7 ± C8 or extended Erb’s palsy, and C5-T1 or global plexus palsy), preoperative and postoperative forearm positioning, radiological healing time, and any history of concurrent surgical interventions.
Surgical technique
The surgical technique was previously described in detail (Figures 1 and 2). 2 A volar curvilinear incision was made over the flexor carpi radialis tendon distally, curving toward the ulna proximally. We used a single interval, trans-flexor carpi radialis approach to access the bony level. The pronator quadratus and flexor pollicis longus origins were elevated to expose the radial diaphysis while preserving the periosteum. Then, medial progression was achieved by elevating the flexor digitorum profundus origin to expose the interosseous membrane and the ulna (Figure 1(a)). The periosteum was cut longitudinally, detached from the radius and ulna diaphysis, and kept in continuity (Figure 2). Osteotomies were marked at different levels, with the radial one approximately 5–10 mm more distal. Before bone cutting, a 2.7-mm or 3.5-mm 6-hole LCP plate was provisionally applied to the volar aspect of the ulna to drill the proximal holes (Figure 1(b)) and then partially removed to allow for the osteotomy (Figure 1(c)). After performing the osteotomies (Figure 1(c), Supplemental material Video 1), the plate was secured to the proximal ulna, and the distal radius was brought to the proximal ulna and turned to the desired degree of pronation (20–30° pronation). The end-to-end radioulnar fixation was performed with the six-hole LCP plate by placing the screws into the distal radius. Finally, the proximal radius stump was fixed side to side to the distal radius stump with a compression screw, creating an overlay (Figures 1(d) and 2(b)). After surgery, patients were immobilized in a sugar tongue splint for 4 weeks.
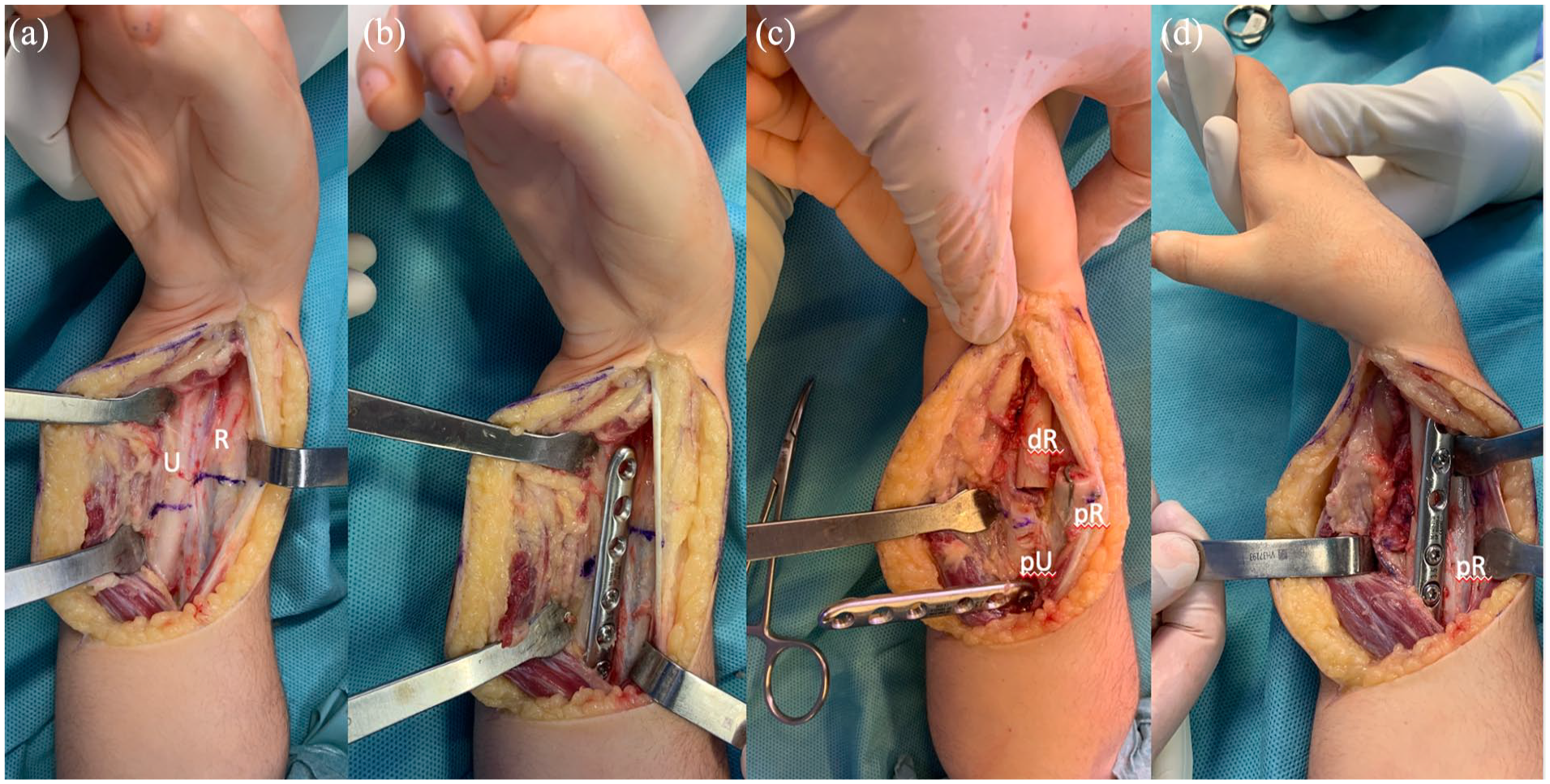
OBFA Kozin’s surgical technique. Through the flexor carpi radialis interval, the bone plane is reached. Osteotomies were marked at different levels with the radial on 5–10 mm more distally (a). Before bone cutting, a 2.7- or 3.5-mm six-hole LCP plate was provisionally applied to the volar aspect of the ulna to drill the proximal holes (b) and then partially removed and turned away to allow for performing the osteotomies (c). After performing the osteotomies (c) and securing the plate into the proximal ulna, the distal radius was brought to the proximal ulna and rotated into the desired pronation (d).
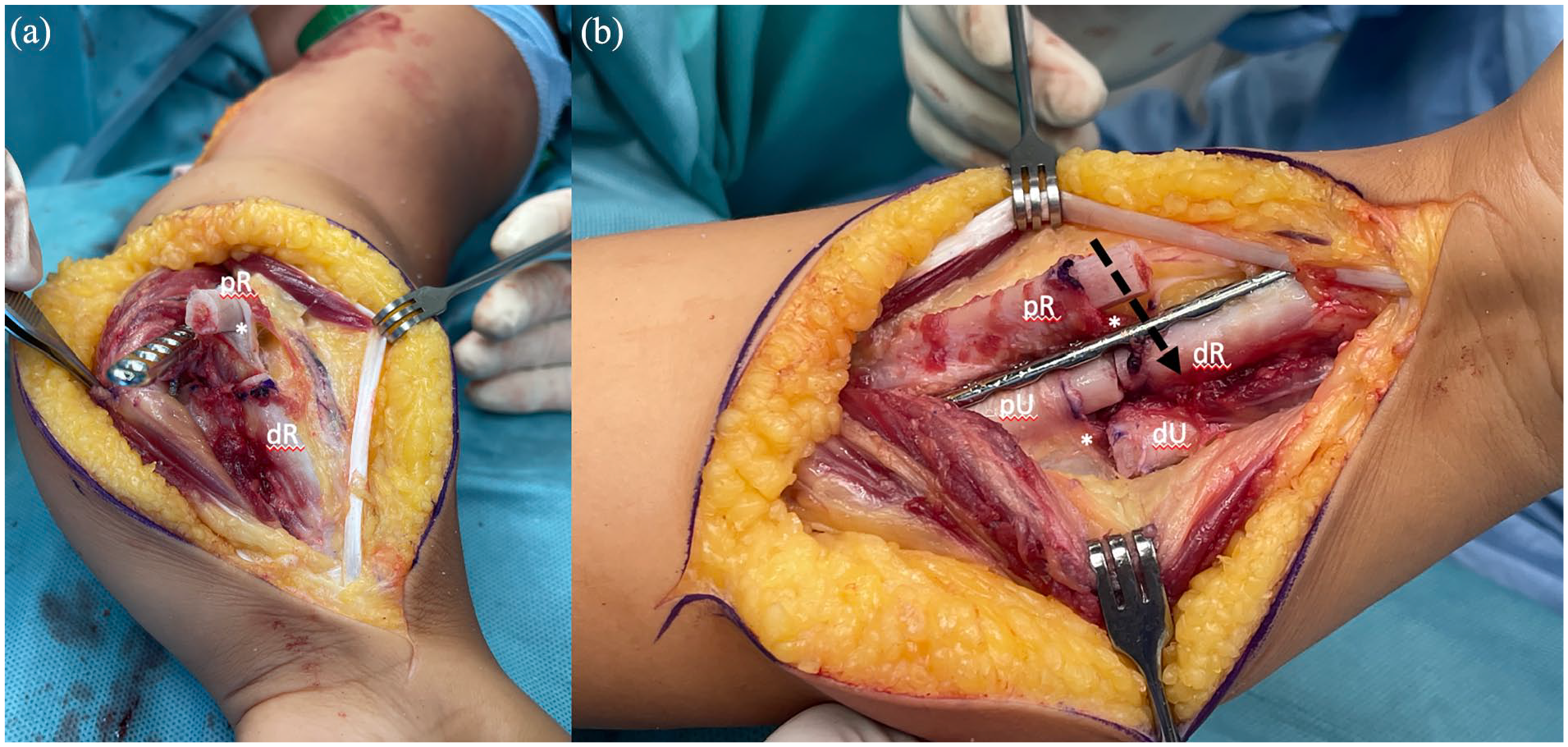
Technical details for OBFA Kozin’s surgical technique. (a) The periosteum (*) remains in continuity after the osteotomies. Distal radius (dR) is ready to be transferred end-to-end to the proximal ulna (pU) already with the fixed LCP plate. (b) Periosteum in continuity (*) will allow for a cross configuration construct after bone callus ossification. Distal radius (dR) has been transferred end-to-end to the proximal ulna (pU) and fixed with a LCP plate. The proximal radius (pR) is superposed to the distal radius (dR) allowing for a side-to-side coaptation, fixated with a compression screw (arrow). The distal ulna (dU) remains free.
Results
This cohort comprised 28 patients (20 males, 15 right sides) with an average age of 9 years and 5 months (range: 4 years and 1 month to 18 years and 5 months) (Table 1). Of these, 24 cases had total NBPI, and four cases presented with extended Erb’s palsy.
Patient characteristics.
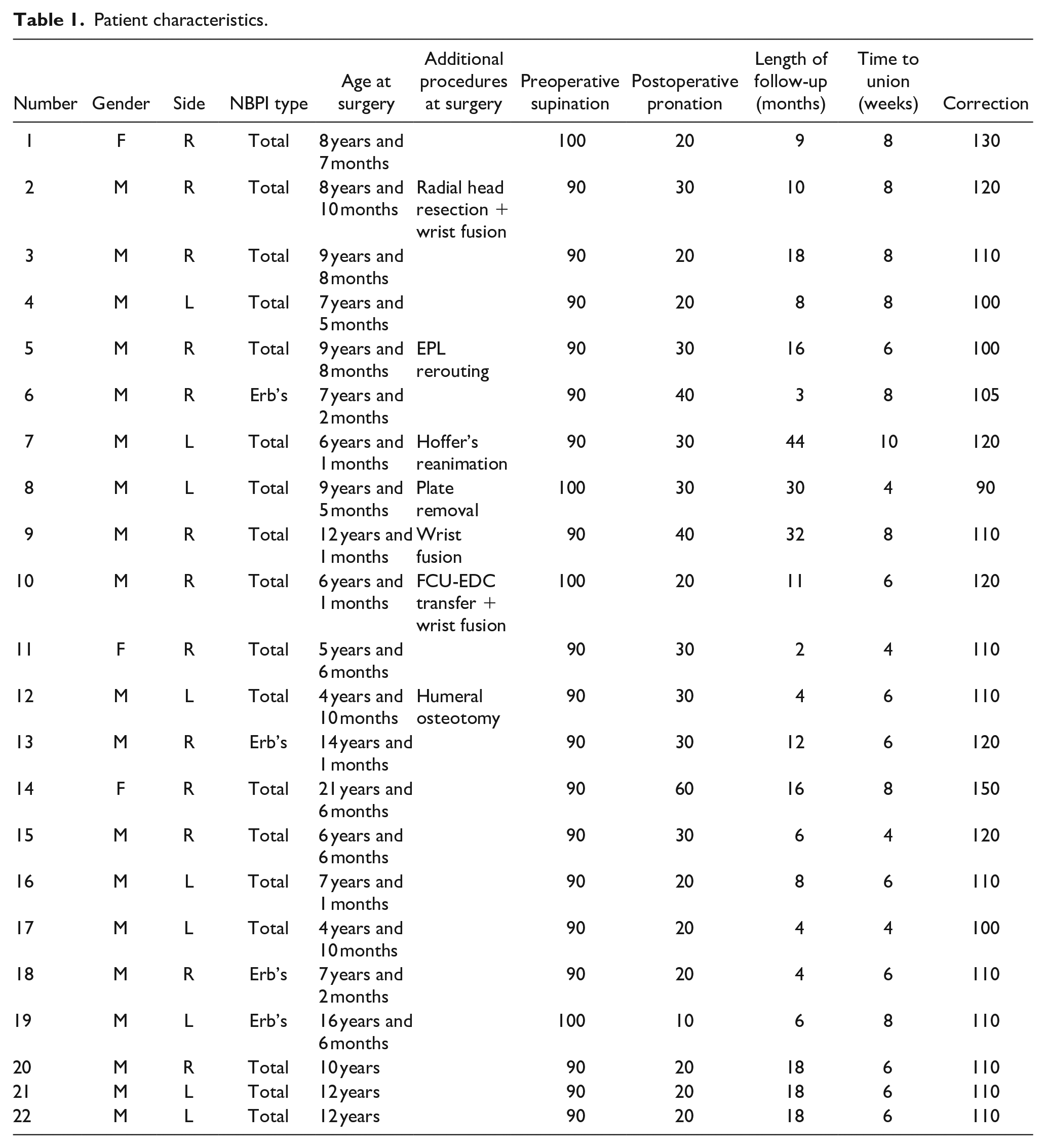
The mean preoperative supination contracture was 96° (range: 90–140). The mean follow-up duration was 42 months (range: 6–99). Associated procedures are detailed in Table 1. The mean correction achieved was 116° (range: 90–160), which remained consistent at the final follow-up assessment. All patients attained bone union within an average period of 6.6 weeks (range: 4–10 weeks) (Figure 3).
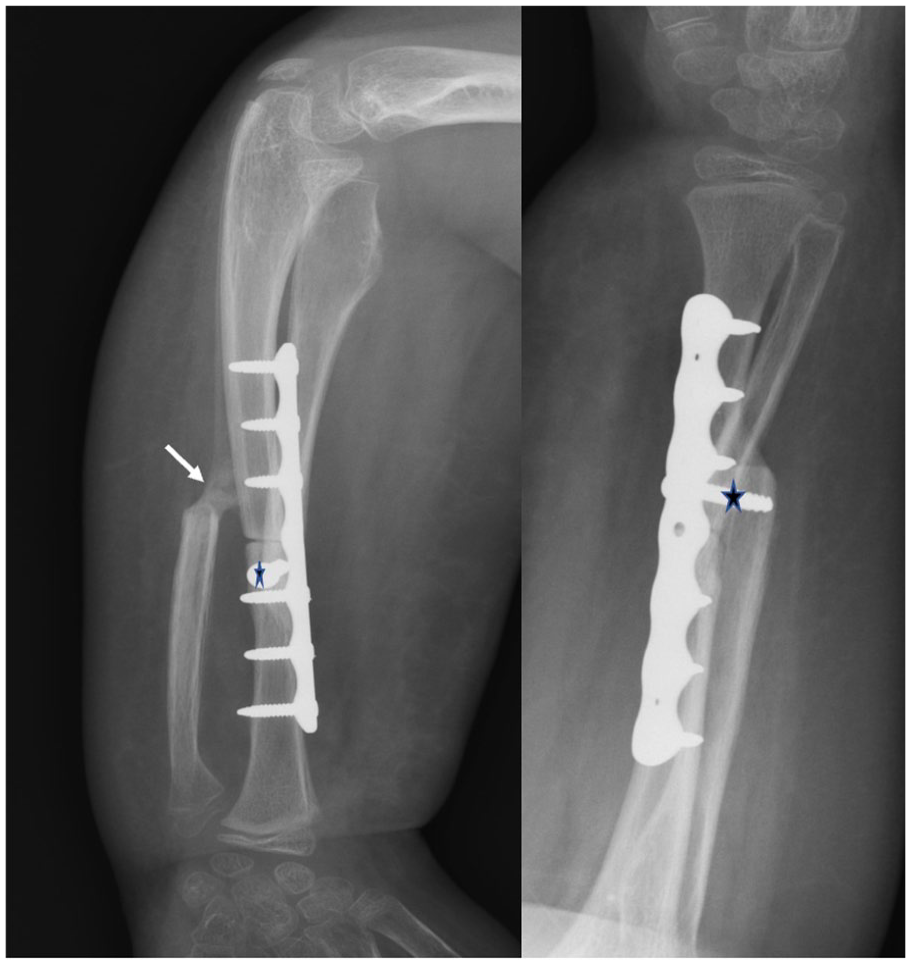
A 9-year-old male’s forearm radiographs 3 weeks after surgery. Initial periosteal ossified callus that will connect the distal ulnar end to the radioulnar union (arrow). The proximal radial end was fixed with a lag screw to the distal radial end (*).
After consolidation, the forearm construct exhibited a radiological cross-shaped appearance (Figure 3). Grossly, no differences were observed between extended Erb’s and complete palsy types.
There were no intraoperative or immediate postoperative neural, vascular, or structural complications. Patient #4 experienced marginal wound necrosis, which subsequently healed through secondary intention. Patient #14 underwent forearm fusion in 60° of pronation, necessitating a subsequent radial derotational osteotomy.
Discussion
Dr. Kozin’s OBFA technique results in a safe procedure with an excellent union rate and allows significant rotational corrections in severe forearm supination deformities in children with NBPI.
The OBFA procedure is indicated for severe and rigid supination deformities following NBPI, as soft tissue procedures are ineffective and radial and ulnar osteotomies do not provide sufficient rotational correction.1,8 Our approach to treating supination deformities is as follows: OBFA is used for complete pronation palsy with severe and rigid supination contracture. Forearm fusion with a pedicled ulnar periosteal flap (unpublished) is employed for supple or partially supple supination deformities with complete pronation palsy, and single- or double-pronation osteotomies are considered when partial pronation palsy is present.1,3,8 –12
We do not utilize biceps rerouting because, especially in younger patients, it may lead to a significant pronation deformity over time and a loss of supination.1,13,14
In our patient cohort, the OBFA following Kozin’s technique did not exhibit the common complications reported in the literature, such as nonunion, radial head impingement, and fractures.6,7,15 To mitigate these risks, Dr. Kozin has recently devised a novel technique to treat severe fixed rotational deformities in patients without forearm bone defects. Initially used in a diverse pediatric population, including patients with neurological deficits, congenital diseases, and tumors, this technique involves cutting the radius 1 cm distal to the ulna, yielding two benefits: (1) an overlay between the proximal and distal radius osteotomy stumps, allowing superposition and side-to-side radius-to-radius fixation, resulting in a more stable OBFA construct fixation; and (2) forearm shortening, enhancing rotational capacity by reducing soft tissue tension. Additionally, the longitudinally preserved detached periosteum contributes to the union of the distal ulnar stump with the forearm construct through an ossified periosteal callus (Figure 1), resulting in a radiological X-shaped forearm construct (Figure 2). The excellent union rate can also be attributed to the heightened healing capacity of the pediatric population.
Our excellent outcomes with Kozin’s technique may not be solely attributed to the technique itself but rather to the enhanced biological healing capacity within this age group. The advantages of the technique will be further clarified through its application in adult cases. 16
Kozin’s technique is applicable in cases with preserved radial and ulnar bone length, such as neurological or multiple hereditary exostosis conditions, but may not be suitable when diaphyseal bone defects are present, as in posttraumatic or congenital disorders. 16 In such instances, a radius-to-ulna side-to-side transfer might be more appropriate. 16
The forearm was positioned between neutral and 30° of as recommended by previous literature.4,17 –19
Our results were comparable to studies reporting on Kozin’s technique for OBFA, showing success in bone union, degree of rotational correction, and absence of complications in pediatric populations. 2 Limited studies are available on OBFA construction in the pediatric age group.19,20 Advantages of Kozin’s technique include its ability to achieve significant rotational correction without the need for proximal radius resection to prevent radial head impingement.2,19,20,21
The main drawback of this study is the absence of preoperative and postoperative functional analysis, although many previous studies have demonstrated its functional benefits.5,9 Other weaknesses of the study include its retrospective nature and relatively short-term follow-up.
In conclusion, Dr. Kozin’s OBFA technique proves reliable for correcting extensive forearm supination deformities in children with NBPI, achieving rapid bone union, and avoiding complications associated with other techniques. The radial diaphyseal cut distal to the ulnar bone cut and the longitudinally preserved detached periosteum constitute the keys to the success of this technique.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241276348 – Supplemental material for One-bone forearm for the treatment of supination contractures secondary to neonatal brachial plexus injury
Supplemental material, sj-pdf-1-cho-10.1177_18632521241276348 for One-bone forearm for the treatment of supination contractures secondary to neonatal brachial plexus injury by Juliana Rojas-Neira, Camilo Chaves, Paula Díaz-Gallardo, Trong-Quynh Nguyen, Juan J Dominguez-Amador and Francisco Soldado in Journal of Children’s Orthopaedics
Footnotes
Author contributions
J.R.-N.: study design, performed measurements, manuscript preparation; C.C.: study design; P.D.-G.: study design, manuscript preparation; T.-Q.N.: performed measurements; J.J.D.-A.: study design, manuscript preparation; F.S.: study design, surgeon who performed surgeries.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.