
Abstract
Objective:
Osteochondromas are common bone tumors with hyaline cartilage-covered heads, arising from cortical and medullary bone. Solitary medial proximal tibial osteochondromas (MPTOs) can cause pes anserinus syndrome via compression. However, the literature lacks comprehensive studies on MPTO-related pes anserinus syndrome and its surgical outcomes.
Material and Method:
The study reviewed 227 patients diagnosed with osteochondroma between January 2018 and January 2022, with 21 patients meeting inclusion criteria: under 19 years, MPTO, surgical excision, histological diagnosis, ≥1-year follow-up. Cases with irregular follow-ups and multiple hereditary exostoses were excluded. Different surgical techniques were employed based on lesion characteristics. Postoperative weight bearing was allowed, and follow-ups involved postoperative complications assessment, clinical data collection, imaging, and functional evaluations using the International Knee Documentation Committee (IKDC) and Hospital for Special Surgery Pediatric Functional Activity Brief Scale scoring systems.
Results:
The study involved 21 adolescents (15 ± 2 years). Lesion types were predominantly pedunculated (86%) and surgical interventions involved pes anserinus split (76%) or tenoplasty (24%). No significant correlations were observed between lesion dimensions and IKDC scores. Split intervention led to a significant improvement in IKDC scores (p < 0.01), while tenoplasty showed similar results (p < 0.05). Athlete status did not affect IKDC scores significantly, but both athletes and non-athletes demonstrated improvements (p < 0.05).
Conclusion:
The negative impact of MPTOs causing pes anserinus tendinitis on the patient’s quality of life and activity can be completely corrected with surgical treatment. Complete pes anserinus tendon cutting and subsequent repair are recommended if they facilitate surgery. The study underscores the importance of surgical management for MPTO-related pes anserinus syndrome and provides insights into the effectiveness of different surgical techniques.
Introduction
Osteochondromas are common bone tumors that have a head covered with hyaline cartilage and arise from both cortical and medullary bone. 1 Although its exact frequency is not known exactly, it constitutes approximately 40%–50% of benign bone tumors and 10%–15% of all bone tumors.1 –3 Although it is usually seen in the metaphyseal region of long bones, it is most commonly seen around the knee (proximal tibia, distal femur). 4 Osteochondromas can be sessile or pedunculated type. 5 It has two clinical forms (Supplemental Material): solitary osteochondroma and multiple hereditary exocytosis (MHE). 6
Pes anserinus; It is the structure formed by joining the tendinous insertions of the sartorius, gracilis, and semitendinosus muscles in the medial part of the proximal tibia, which means “goose’s foot” in Latin.7,8 The pes anserine bursa is located between the junction of these three tendons and the tibia. 9 Pain in this area is called pes anserinus syndrome or anserine bursitis. 7 Medial proximal tibial osteochondromas (MPTOs) may cause pes anserinus syndrome by causing compression.10,11
Treatment of symptomatic osteochondromas is surgical. When we searched the literature, there were only a few small case series that reported that MPTOs cause pes anserinus syndrome.10 –12 We wanted to investigate whether this situation significantly changes the course of surgical treatment and how it affects it clinically after surgical treatment.
The aim of our study was to reveal that MPTOs may cause pes anserinus tendinitis in children and adolescents and to investigate the effect of osteochondroma size and surgical treatment on clinical and functional outcomes.
Material and method
Following the ethics committee approval, 227 patients who applied to our hospital’s orthopedics outpatient clinic between January 1, 2018 and January 1, 2022, and were diagnosed with osteochondroma were retrospectively reviewed. Patients who were younger than 19 years of age, had MPTO, underwent surgical excision, were diagnosed with osteochondroma histologically, and had at least 1 year of postoperative follow-up were included in the study. Patients who did not attend their clinical follow-ups regularly, patients with a diagnosis of MHE patients diagnosed with chondrosarcoma, and patients with different pathologies in the knee joint (meniscus injury, Baker’s cyst, medial collateral ligament damage, etc.) were excluded from the study. Patients diagnosed with MHE may have more than one osteochondroma located around the knee (distal femur, proximal fibula). Since this situation could affect the accuracy of functional results, it was excluded from the study. Likewise, patients with different pathologies of the knee joint were excluded from the study because they may affect the accuracy of functional results. A total of 21 patients who met the criteria were included in the study (Figure 1).
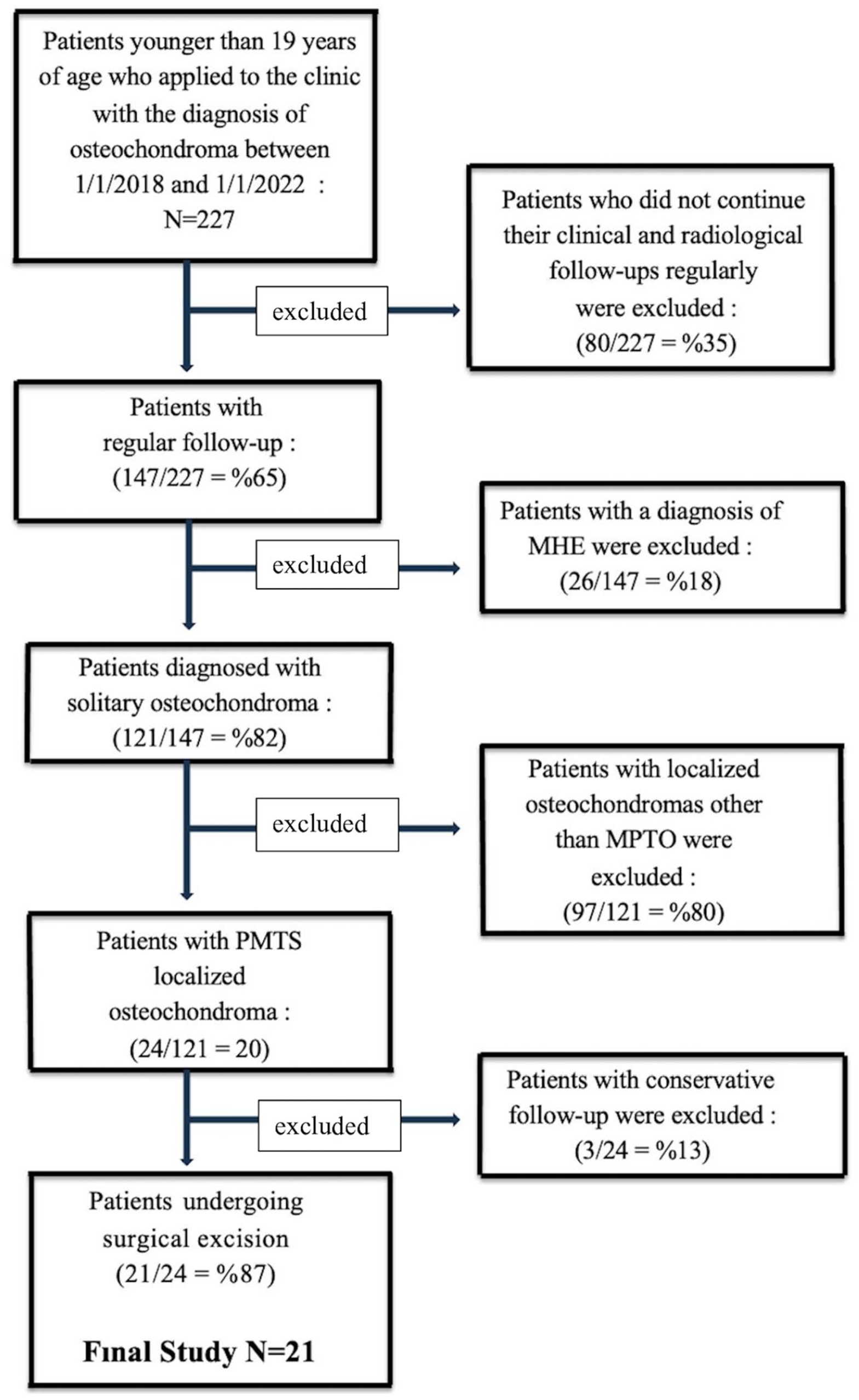
Flowchart demonstrating patient selection and final study cohort.
All surgeries were performed by a single surgeon with training in orthopedic oncology (FS). The reason for surgery in all patients was pain that increased with long walks and physical activity. A medial incision was used surgically in all cases. In this surgical approach; pes anserinus was reached by passing through the subcutaneous fascia and avoiding the neurovascular (saphen nerve and vein) structures. Depending on the size and character of the lesion, pes anserinus was split (Figure 2) and excision was performed with the help of a curved osteotome in 16 patients. In five patients, it was observed that the pes anserinus tendon was attached directly to the osteochondroma. In these patients, the operation was performed by removing the pes anserinus from its attachment site, leaving 5 mm of tendon and repairing it after resection. The repair process was performed by sewing the cut tendons to the attachment points on the bone (tenoplasty; Figure 3). Fluoroscopy was used during resection to ensure that the entire lesion was removed and that the integrity of the tibia was not compromised. In the postoperative period, all patients were allowed to give full weight bearing on the same day. In the tenoplasty group, 0–30 degrees of range of motion was allowed by using an angle-adjustable knee brace for the first 4 weeks, while no movement restriction was applied in the group in which the pes anserinus was split. The patients were evaluated according to the Clavien–Dindo classification in terms of postoperative complications. 13
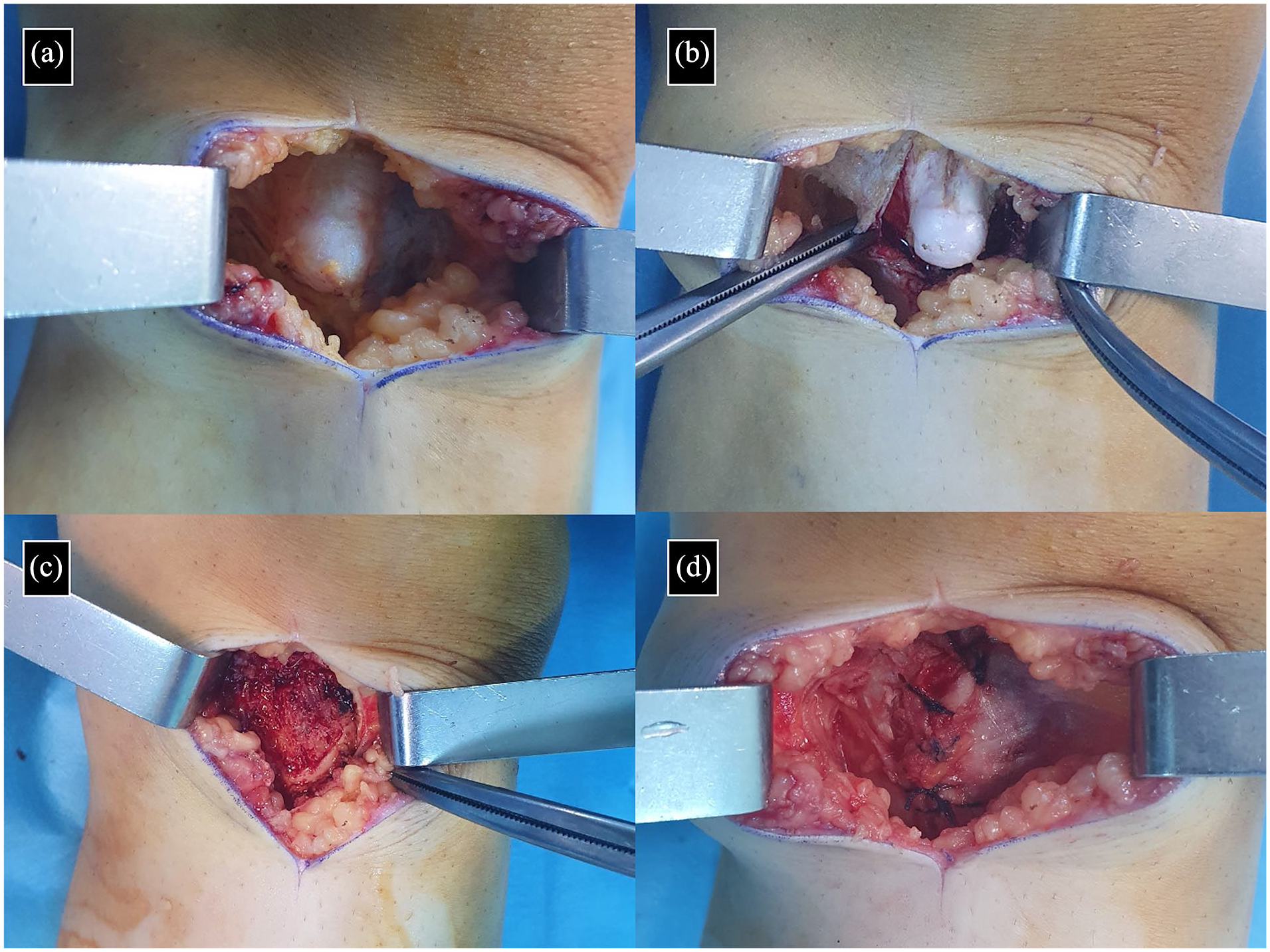
Intraoperative image of a 12-year-old female patient with MPTO (a), image of the osteochondroma after split separation of the pes anserinus (b), intraoperative image after resection (c), and image of the separated tendon after repair.
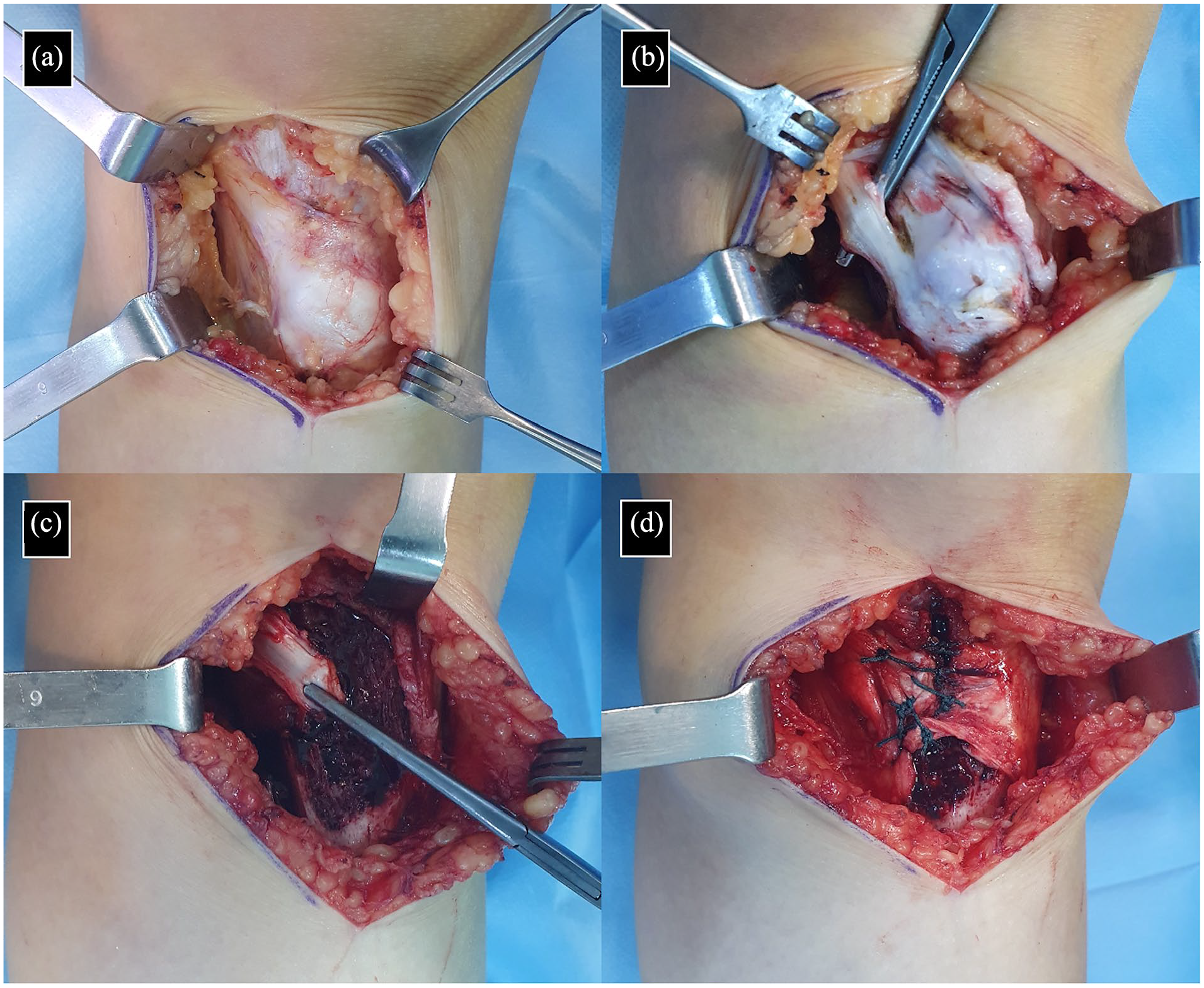
Intraoperative image of a 16-year-old female patient with MPTO (a), it is seen that the semitendinosus tendon is attached directly to the lesion after the fascia of the pes anserinus is removed (b), intraoperative image after the resection of the osteochondroma by cutting the semitendinosus tendon (c), and after the repair of the semitendinosus tendon (tenoplasty) intraoperative image.
The patients’ age, gender, postoperative follow-up period, being an athlete, type of osteochondroma (sessile, pedunculated) and intraoperative pes anserinus tendon intervention (split, tenoplasty) were analyzed. The branches of the patients with an athlete license and the time of their return to sports were questioned and recorded. The longest diameter of the lesion was measured and recorded in the axial, coronal, and sagittal plane sections of the lesion with preoperative MRI images (Figure 4). The tumor volume and surgery volume were calculated by using the formula for a hemiellipsoid using the formula: volume = π/6 × length × width × height and was analyzed on magnetic resonance images before the surgery (contrast-enhanced T1-weighted images). The preoperative and postoperative functional results of the patients were recorded using the International Knee Documentation Committee (IKDC) scoring. 14 The results were recorded using the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) scoring 15 in the final postoperative follow-up of the patients who reported that they were athletes.

Anterior-posterior (a) and lateral (b) radiographs of a 16-year-old male patient with MPTO, showing the pes anserinus fascia adhered to the surface of the osteochondroma (white arrows) in the axial T1-weighted section (c) and coronal T1-weighted section.
Statistical analysis
SPSS 26 (Statistical Package for the Social Sciences) program was used for statistical analysis. Descriptive statistical methods (mean, standard deviation, median, frequency, percentage, minimum, maximum) were used while evaluating the study data. The conformity of the quantitative data to the normal distribution was tested with the Shapiro–Wilk test and graphical examinations. The Mann–Whitney U test was used for comparisons between two groups of quantitative variables that did not show normal distribution. Wilcoxon signed-ranks test was used for in-group comparisons of quantitative variables that did not show normal distribution. Pearson correlation analysis and Spearman correlation analysis were used to evaluate the relationships between quantitative variables. Statistical significance was accepted as p < 0.05.
Results
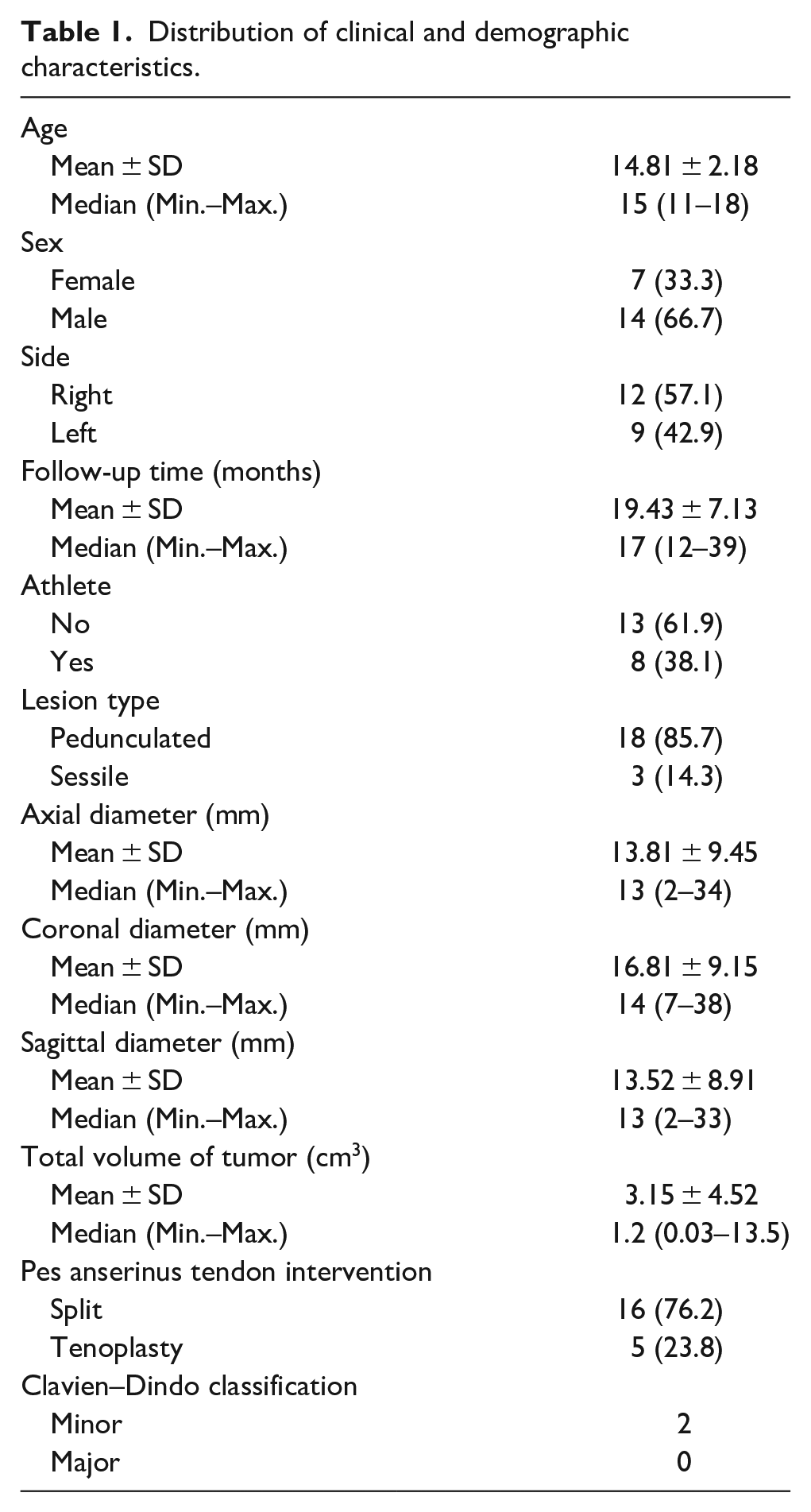
It was observed that the lesion type of 86% (n = 18) of the subjects participating in the study was pedunculated and 14% (n = 3) sessile. It was observed that 76% (n = 16) of the cases had split intervention in the pes anserinus tendon, and tenoplasty in 24% (n = 5). While no major complications were observed in any of the cases according to the Clavien–Dindo classification, minor complications were observed in two of them (Table 1).
Distribution of clinical and demographic characteristics.
No statistically significant correlation was found between the axial diameter, coronal diameter, sagittal diameter, and total tumor volume measurements of the subjects participating in the study and the changes in preoperative IKDC, last follow-up IKDC, and IKDC (p > 0.05; Table 2).
Evaluation of the relationship between preoperative, final follow-up, and difference IKDC measurements and measurements of axial, coronal, sagittal diameter, and tumor total volume.
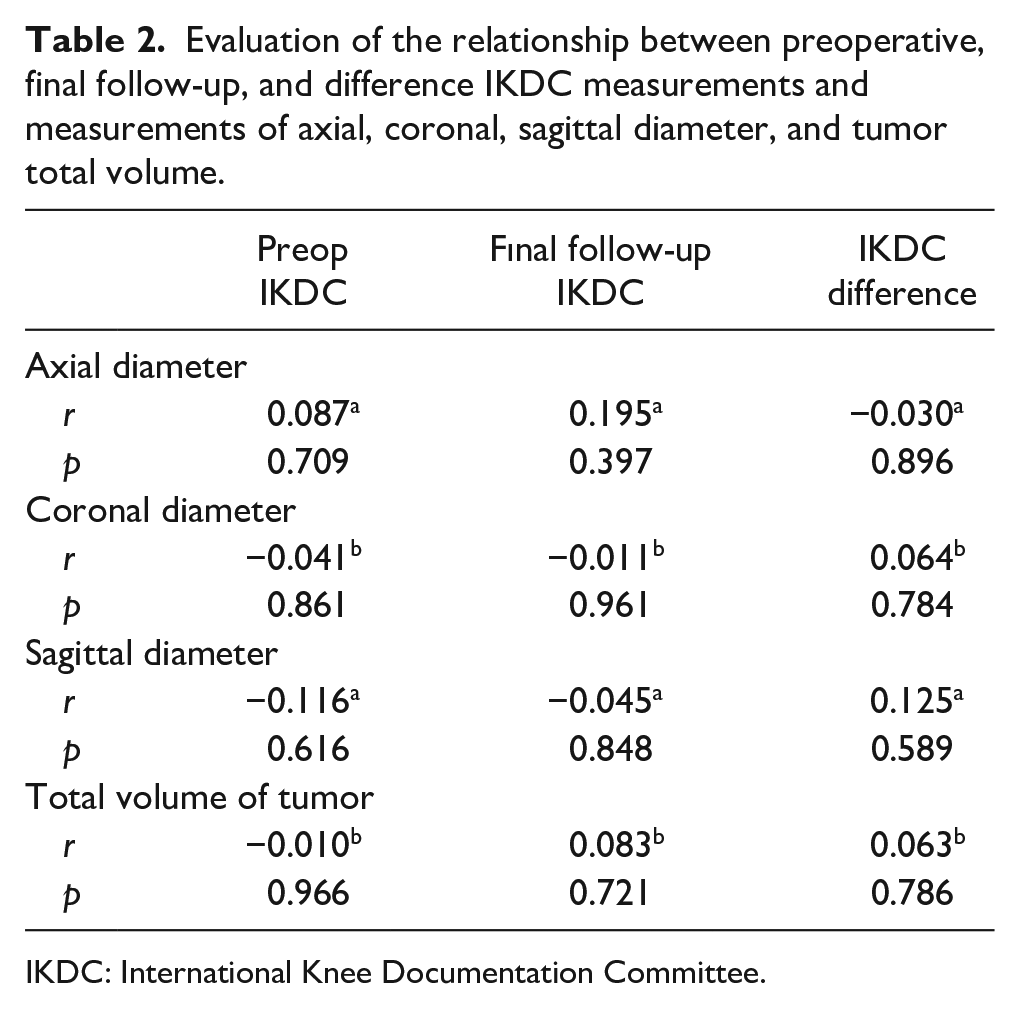
IKDC: International Knee Documentation Committee.
Preoperative and last follow-up IKDC measurements of the cases did not show a statistically significant difference according to the type of intervention to the pes anserinus tendon (p > 0.05). The mean increase of 21 ± 9 units in the last follow-up IKDC measurement was found to be statistically significant in cases with split intervention compared to preop (p < 0.01). The mean increase of 29.40 ± 10.01 units in the last follow-up IKDC measurement of cases with tenoplasty as the intervention was found to be statistically significant (p < 0.05; Table 3).
Evaluation of preoperative and final follow-up IKDC measurements according to the intervention of the pes anserinus tendon.
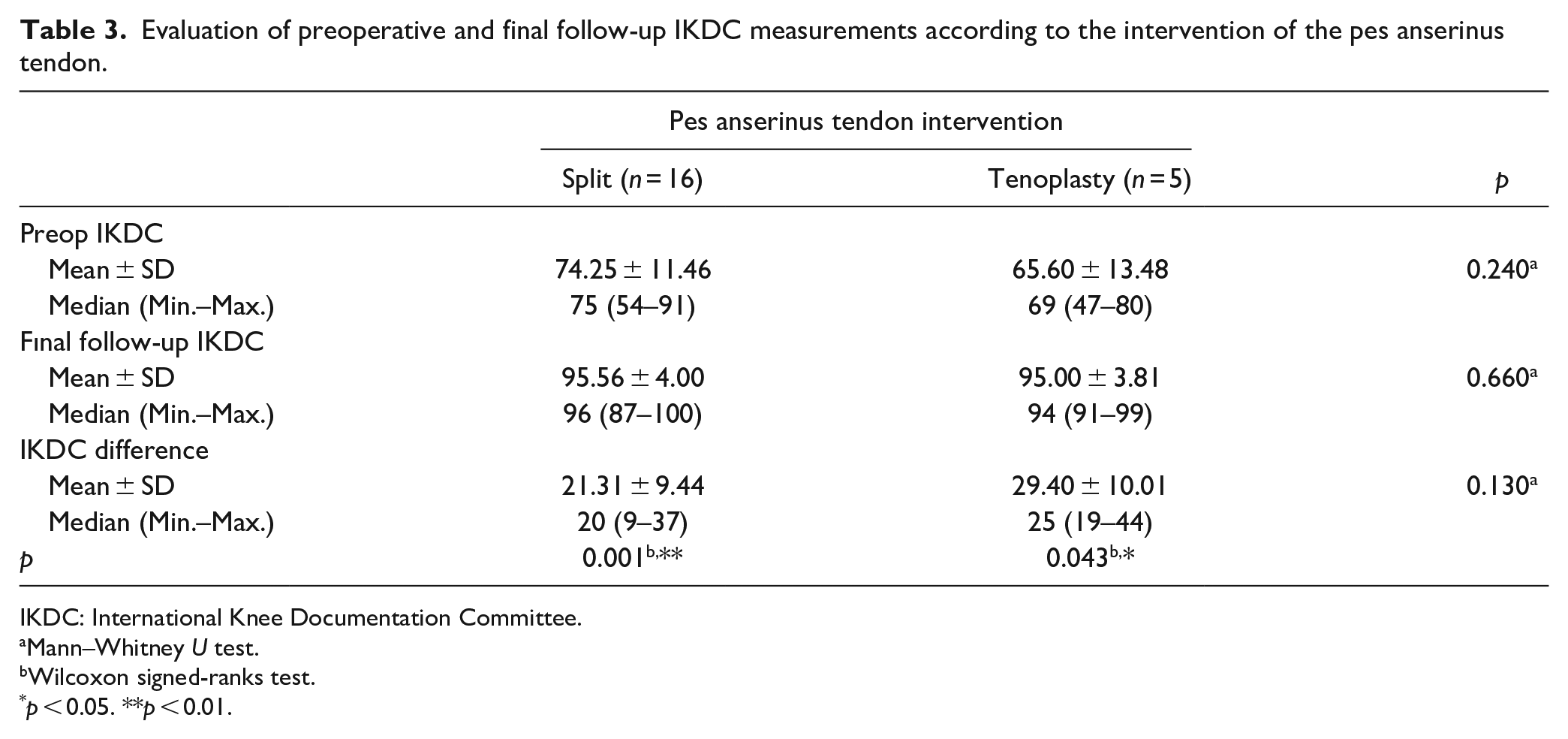
IKDC: International Knee Documentation Committee.
Mann–Whitney U test.
Wilcoxon signed-ranks test.
p < 0.05. **p < 0.01.
Preoperative and last follow-up IKDC measurements of the cases do not show a statistically significant difference according to their status as athletes (p > 0.05). The mean increase of 23 ± 11 units in the last follow-up IKDC measurement of non-athletes compared to preop was found to be statistically significant (p < 0.01). The mean increase of 23 ± 8 units in the last follow-up IKDC measurement of the subjects who were athletes compared to the preop was found to be statistically significant (p < 0.05; Table 4).
Evaluation of preoperative and final follow-up IKDC measurements by athlete status.
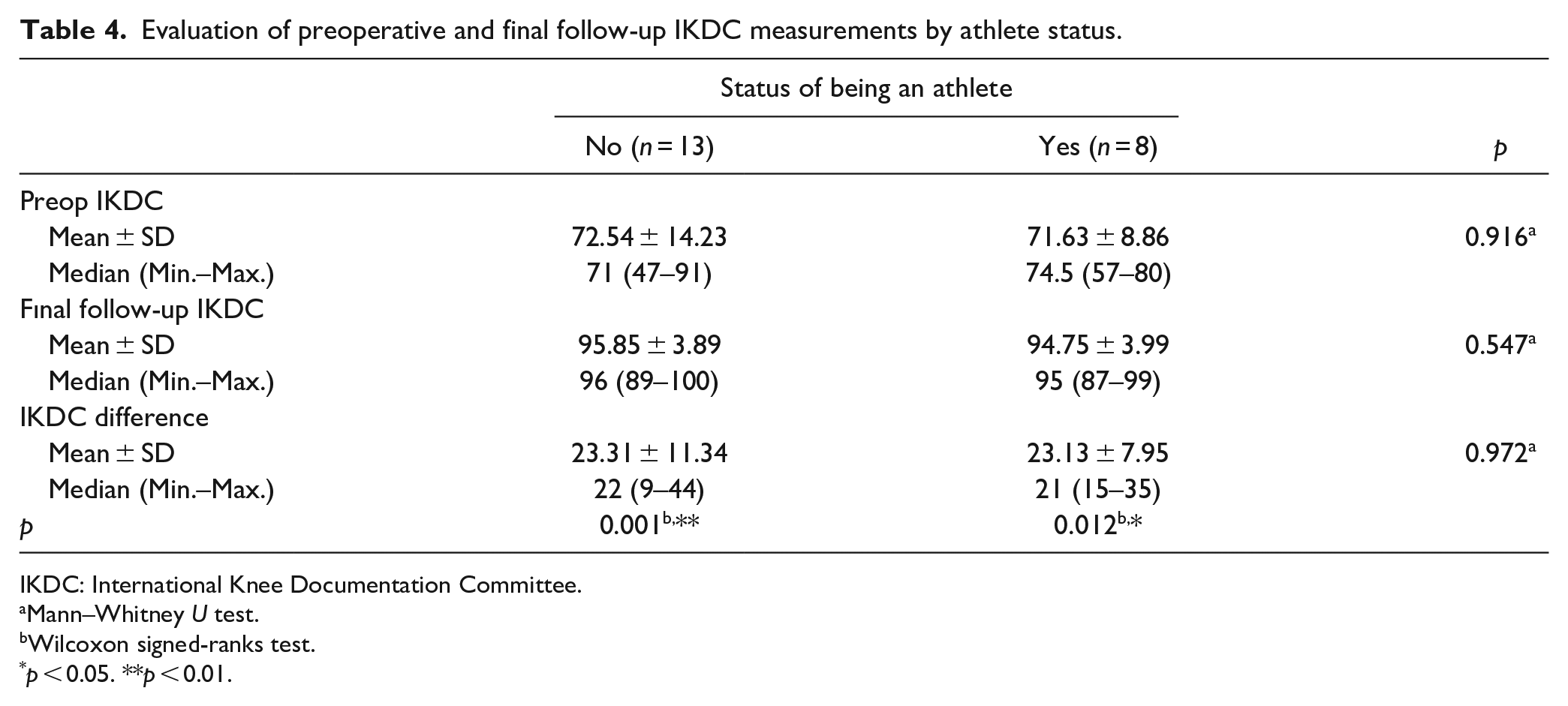
IKDC: International Knee Documentation Committee.
Mann–Whitney U test.
Wilcoxon signed-ranks test.
p < 0.05. **p < 0.01.
The follow-up period of the athletes ranged from 14 to 39 months, with an average of 24 ± 9 months. The duration of the patients’ return to sports ranged from 2 to 6 months, with an average of 4 ± 1 months. The functional results of the subjects included in the study at the last follow-up with HSS Pedi-FABS ranged between 13 and 21, with an average of 16 ± 3. It was observed that 62.5% (n = 5) of the cases had split intervention to the pes anserinus tendon, and 37.5% (n = 3) tenoplasty (Table 5).
Distribution of athletes.
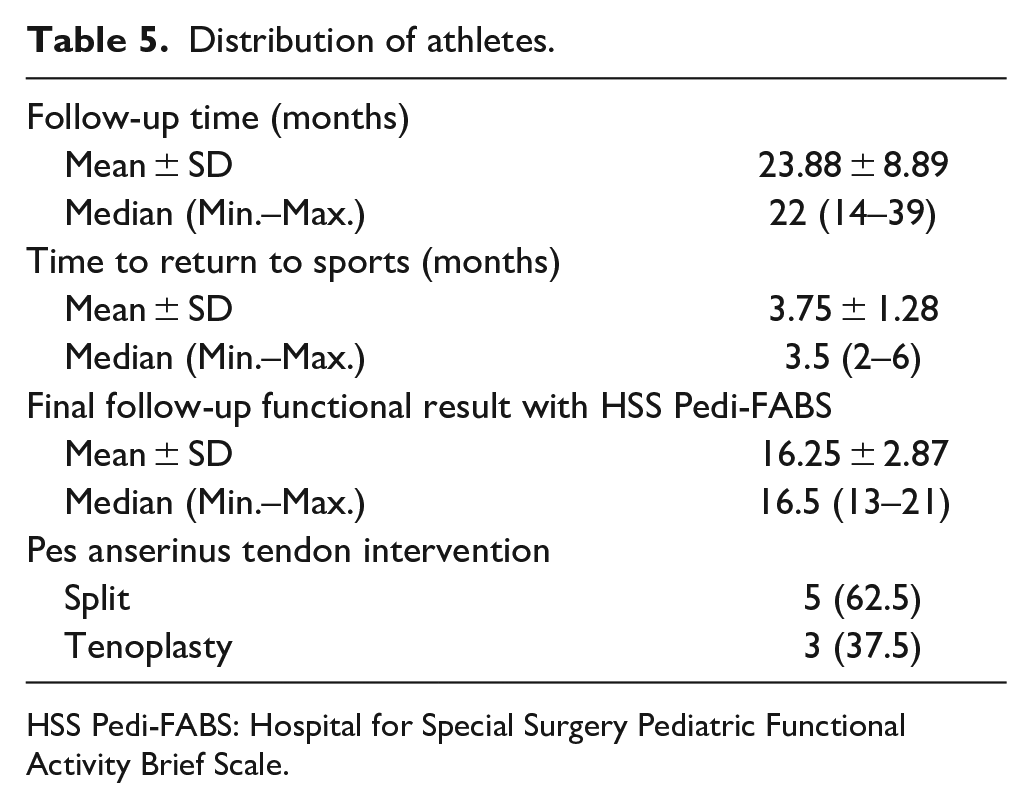
HSS Pedi-FABS: Hospital for Special Surgery Pediatric Functional Activity Brief Scale.
Discussion
Osteochondromas may cause pain depending on their localization and size. It may cause mechanical effects such as limitation of joint movement and tenosynovitis due to irritation in the surrounding tendons and ligaments. Although most of the osteochondromas are solitary (85%), they are asymptomatic. 1 Generally, symptomatic patients are in the young age group, and 75%–80% of them are diagnosed before the age of 20.1 –3 Our study included symptomatic osteochondromas, and we observed that a higher rate of patients with MPTO were symptomatic and resulted in surgical treatment. However, when we evaluated the preoperative pain and functional scoring of the patients with the IKDC score, it was seen that the symptoms were independent of the size and total volume of the lesion in all three planes. In addition, we thought that the lesion might worsen functional results by causing more tendon irritation in people who do active sports. However, in our evaluation of the IKDC score, we observed that the symptoms affected the patients with similar severity regardless of being an athlete.
The diagnosis of pes anserinus syndrome should be considered in patients with pain in the inferomedial region of the knee joint.7,8,16 It has been shown that the incidence of pes anserinus syndrome is high in elderly overweight women, especially in patients with gonarthrosis and accompanying pes planus.7,17 Medial compartment arthrosis, medial meniscus lesions, medial collateral ligament damage, lumbar radiculopathy, foreign body irritation, and infections are considered in the differential diagnosis of pes anserinus syndrome. 17 In addition, MPTOs should be kept in mind in the differential diagnosis of pes anserinus syndrome. In addition, in our evaluations with the IKDC score, we reported that MPTOs seriously affect knee functions and that high functional results were obtained (95.8 ± 3.8, 94.7 ± 3.9) due to the elimination of pes anserinus irritation after surgical treatment.
Consistent with previous studies, solitary lesions constituted the majority (83%) of patients with MPTO.18,19 In case series involving only osteochondromas that cause pes anserinus syndrome, it has been shown that pain is the first symptom in most of the cases.10 –12 The first complaint of all patients in our current study was pain, which is consistent with previous studies. Since the lower extremity bones are exposed to more weight than the upper extremity at the osteooligamentous junctions, there is a high probability that lower extremity osteochondromas will have a symptomatic course due to increased mechanical irritation.18,20 Murphey et al. They reported that MHE, sessile and larger volume osteochondromas may cause more angular deformity in the extremities. In our study, patients diagnosed with MHE were excluded because it would limit the reliability of the study. Three patients had sessile lesion type, but no extremity deformity was observed. Although the sizes of the lesions were very different, angular deformity was not observed in any of the patients.
Bottner et al. performed excision in 86 of 92 symptomatic osteochondromas in their study and reported local recurrence in only 1 patient (2%) in the pediatric population and in a total of 5 patients (6%) in their 3- to 8-year follow-up. 21 No recurrence was observed in any of the patients in our current study. This can be explained by the fact that our study was in the pediatric age group and the mean follow-up period was 19 months. Wirganowicz and Watts performed 285 osteochondroma excisions in a total of 80 patients in the patient population under the age of 21 and reported complications in 10 patients (12.5%). 19 In our study, complications were observed in 2 patients (10%), including postoperative paresthesia in 1 patient due to perop irritation of the saphenous nerve and postoperative seroma in 1 patient. During the follow-up period, the complaints of the patient with paresthesia improved in the postoperative 3rd month, and the discharge of the patient with seroma improved in the 2nd postoperative week. No other major or minor complications were observed.
Wu et al. studied 264 patients with osteochondroma who underwent excision around the knee in the pediatric age group and reported postoperative functional scoring measures; however, the response rate was limited. 22 Apart from this, although there is no other functional outcome study on osteochondromas in the literature, our study is the first to evaluate preoperative functional scores. In our study, we evaluated the functional results of the patients with both preoperative and postoperative IKDC scores. In addition, we evaluated the functional scores of the patients according to the size of the tumor, the type of intraoperative tendon intervention, and whether the patients were not athletes, and we found that there was no significant difference between the groups. Wu et al. In the same study, they evaluated the postoperative functional results of patients who were athletes with Pedi-FABS scoring and reported it as 17 ± 8. In our current study, we observed that the patients had excellent Pedi-FABS scores (16 ± 3) at the last postoperative follow-up.
The present study has inherent methodological limitations due to its retrospective nature. However, the study may have a bias arising from additional factors such as tertiary health care that accepts patients locally, and the high rate of athletes. In addition, the study does not provide information about the natural course of surgical treatment of osteochondromas. Specifically, it aimed to evaluate lesions associated with the pes anserinus tendons. An important point is that the mean follow-up period of the patients is limited to 19 months.
Conclusion
Although MPTOs cause pes anserinus tendinitis, regardless of their size, and significantly reduce the quality of life, excellent results can be achieved with surgical treatment. There was no difference between partial or complete intervention of the pes anserinus tendon during surgery, therefore, we recommend that the pes anserinus tendon be completely cut and then repaired if it will facilitate the surgery.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241276323 – Supplemental material for Solitary medial proximal tibial osteochondromas cause pes anserinus syndrome in adolescents
Supplemental material, sj-pdf-1-cho-10.1177_18632521241276323 for Solitary medial proximal tibial osteochondromas cause pes anserinus syndrome in adolescents by Fevzi Saglam and Muhammed Fatih Serttas in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Data availability statement
All data generated or analyzed during this study are included in this published article (and its Supplemental Material files).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Sakarya University Faculty of Medicine (no: E-71522473-050.01.04-224775) on February 27, 2023, with an exemption from informed consent. No specific consent is needed for statistical analyses of aggregated de-identified data. For this study, the raw data were first extracted from HIS, and patients’ identities, including names, screening IDs, patient IDs, and mobile phone numbers, were de-identified.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.