
Abstract
Purpose:
Developmental hip dysplasia is a prevalent pediatric musculoskeletal condition that lacks international standardized screening. We sought to characterize developmental hip dysplasia screening practices in countries with the top global health indices. We also explored diverse definitions in reported epidemiologic rates of this condition.
Methods:
We performed a scoping review of developmental hip dysplasia screening protocols utilizing countries ranked in the top 25 of the Bloomberg Global Health Index using a protocolized search strategy, progressing from academic to layperson sources. A reference was eligible for inclusion if it mentioned the countries’ screening program and developmental hip dysplasia was the pathology of concern. Incidence rates, when present, were also recorded. The United States Census Bureau’s International Database tool provided countries’ populations. We compiled the data and performed descriptive statistics and appropriate validation methods.
Results:
Twenty countries (80%) had searchable screening programs. Clinical screening with selective universal screening was the most commonly observed (n = 16). Four countries had universal ultrasound screening: Switzerland, Austria, Germany, and Slovenia. Five countries did not have searchable programs. No countries employed radiographic screening. Incidence rates were expressly stated in the literature for nine countries; however, the cohort of interest varied from developmental hip dysplasia versus severity of developmental hip dysplasia versus miscellaneous (e.g. requiring hospitalization).
Conclusion:
The findings of this investigation highlight international inconsistencies regarding developmental hip dysplasia screening and epidemiologic data. Screening variations exist despite consensus statements calling for uniformity. We agree with prior literature advocating for increasing consistency in developmental hip dysplasia management or, at a minimum, increasing transparency regarding how we manage these young patients.
Purpose
Developmental hip dysplasia (DDH) is a prevalent musculoskeletal condition impacting infants and young children globally. It is a frequent topic of debate among pediatric orthopedic surgeons for reasons such as how to define the spectrum of pathology and “best” screening practices.1,2 The lack of standardization on defining DDH leads to confusion in the literature. 3 For example, the often-cited DDH incidence of 1 per 1000 originally referred to dislocated hip unlikely to recover spontaneously and thus is a specific subtype of the spectrum of DDH rather than representing the frequency of the entire pathology.4,5
Managing this common condition without gold standard guidelines has not gone unnoticed by pediatric orthopedists. Numerous consensus statements and collaborative efforts have been published; however, controversies remain.1–3,6 Questions include selective versus universal screening?7,8 Clinical versus ultrasound? Neonatal age of screening?9,10 Which practitioners should perform the screening?11,12 Moreover, many other issues persist, such as standardization of training for ultrasound examination of infant hips.
Screening for DDH typically encompasses clinical examination and/or radiographic imaging.4,5 DDH diagnosis also represents an area of heterogeneity; standardized diagnostic criteria were proposed in a 2011 article after surveying members of the European Pediatric Orthopaedic Society. 3 The diagnostic criteria included clinical examination (e.g. positive Ortolani or Barlow test, asymmetric hip abduction), ultrasonography, patient characteristics (e.g. breech presentation), and history (first degree relative treated for hip dysplasia). 3 Treatment for DDH varies on the patient’s age at time of diagnosis and treating physician. 13 Young patients typically less than 6 months of age are treated with a dynamic splint (such as a Pavlik harness) or a static orthosis (e.g. a rigid abduction brace).13,14 Invasive treatment options (e.g. adductor tenotomy, closed vs open reduction, femoral or pelvic osteotomies) depend on the age at time of diagnosis, severity or persistence of dysplasia, treating physician, among other variables. 13
We sought to investigate the DDH screening practices in 25 counties with the top global health indices to characterize the global practice variations. In addition, we collected the reported frequencies of DDH diagnoses to explore diverse definitions in reported rates of this common condition.
Methods
We performed a scoping review of DDH screening protocols utilizing countries ranked in the top 25 of the Bloomberg Global Health Index. 15 We selected the Bloomberg Global Health Index due to its diverse factors contributing to the overall score, including environmental and population characteristics (tobacco use, obesity rates), life expectancy, mortality rates, and availability of clean water.15–17 The 2019 data were the most recently available when the search was conducted (see Table 1 for a list of countries).
Countries’ Screening Programs Organized By Global Health Index.
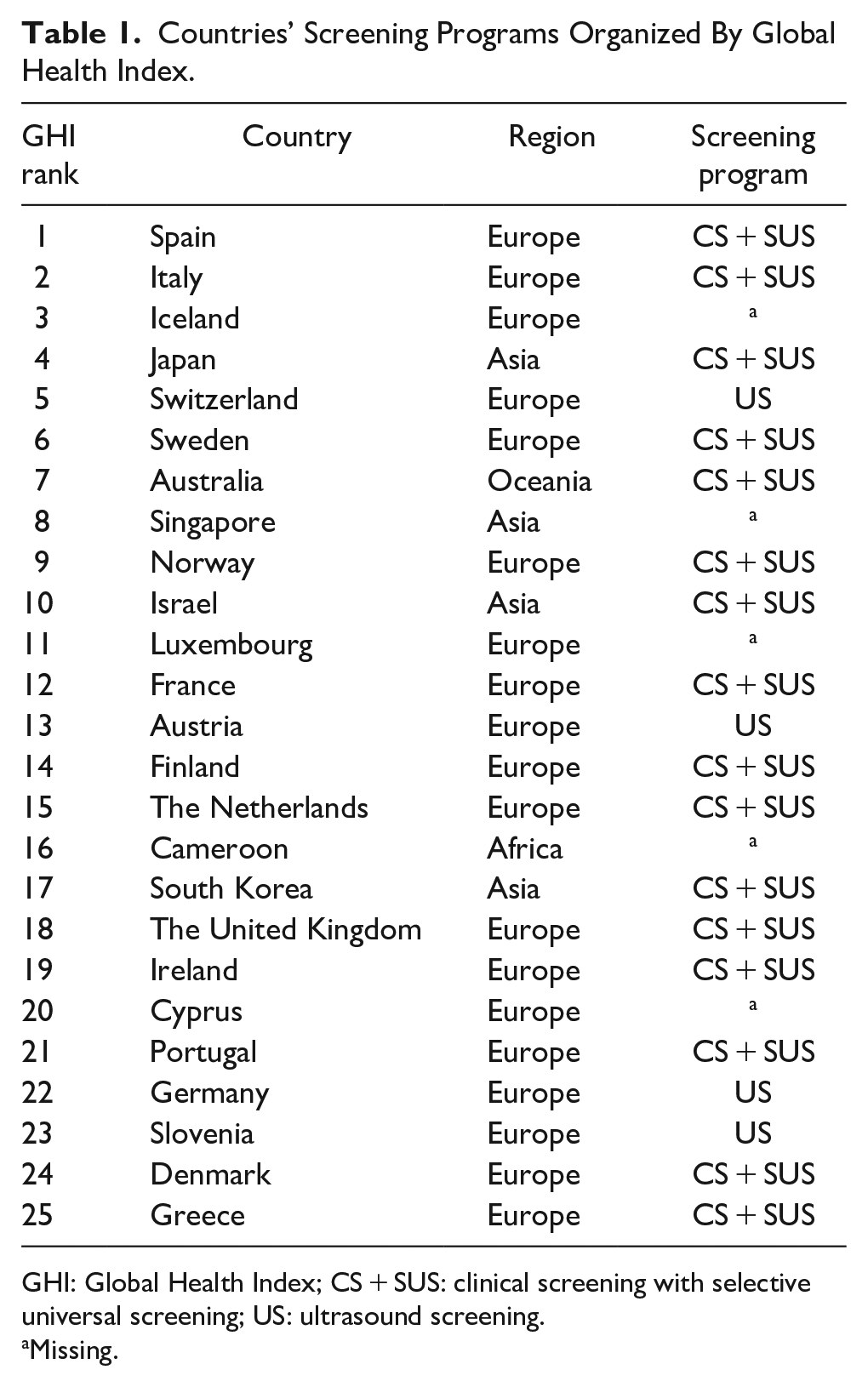
GHI: Global Health Index; CS + SUS: clinical screening with selective universal screening; US: ultrasound screening.
Missing.
We employed the following definitions for consistency:
DDH: the spectrum of developmental (meaning not neuromuscular, syndromic, or teratologic) pediatric hip pathologies, which includes acetabular dysplasia, hip subluxation, and hip dislocation.
Simple dysplasia: shallow acetabula without subluxation or dislocation of the femoral head.
Hip subluxation: superior or lateral migration of the femoral head in relation to the acetabulum, whereas a portion of the femoral head is in contact with the acetabulum.
Hip dislocation: superior or lateral migration of the femoral head in relation to the acetabulum, in which the femoral head is no longer in contact with the acetabulum
Clinical screening: a detailed physical examination, including the Ortolani and Barlow maneuvers, performed to detect hip instability/subluxation/dislocation.13,18
Ultrasound screening (US): ultrasonography detailing the anatomic relationship of the femoral head to the acetabulum (e.g. the alpha and beta angles).1,10 Specifying the ultrasonography classification method (such as the Graf method vs others) was outside the study scope.
Radiographic screening: standardized anteroposterior radiographs to evaluate bony anatomy (such as acetabular morphology) and the relation between the acetabulum and femoral head. 19
Universal screening: screening program applied to all infants regardless of risk factors.
Selective screening: screening is only applied to infants with identified risk factors.
A protocolized search strategy was used to conduct the investigation, beginning with academic and progressing to layperson data sources (see Figure 1).
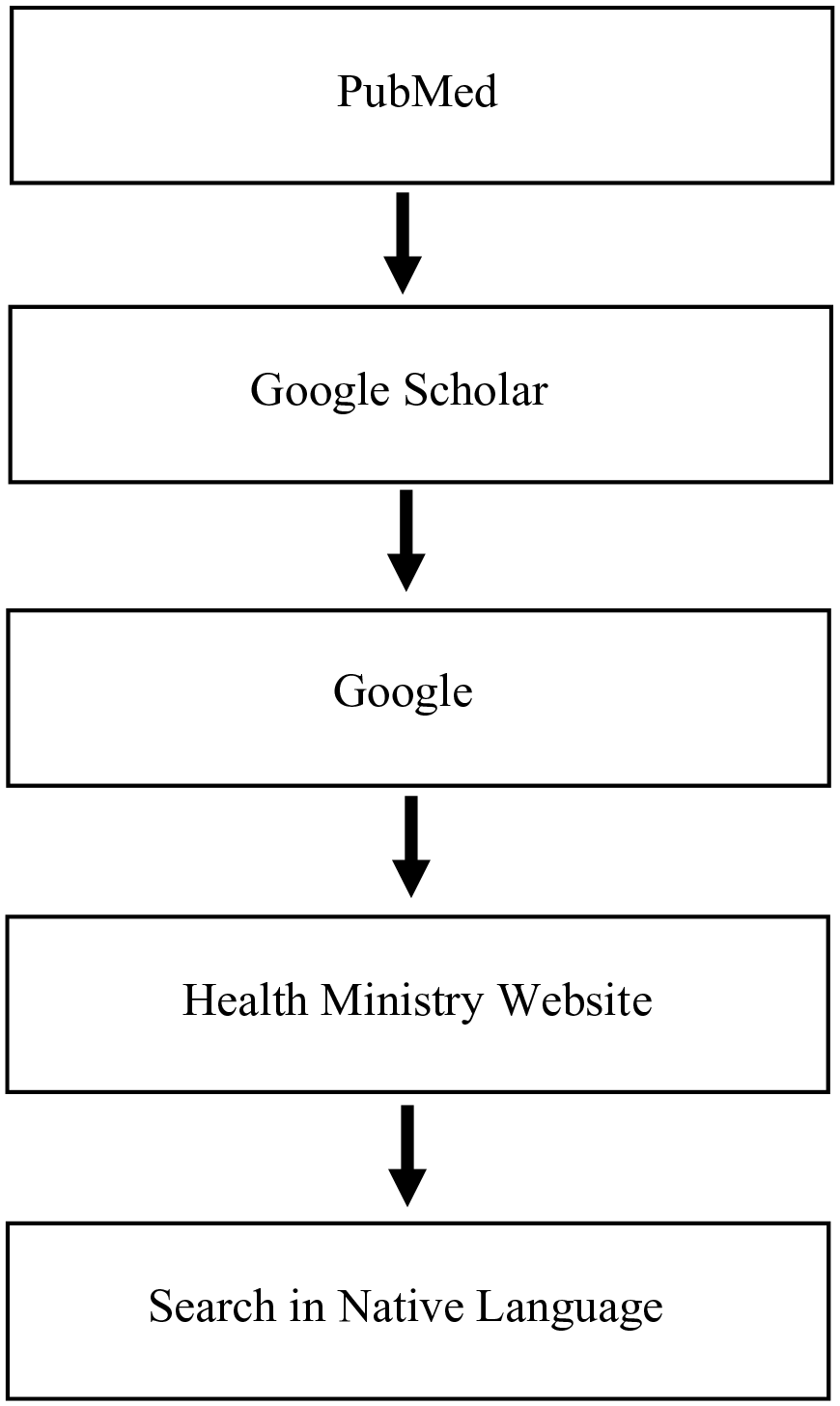
Search Strategy.
The search terms used for PubMed, Google Scholar, and Google were a combination of (country name), DDH, hip dysplasia, guideline, protocol, or program. Numerous search attempts were performed in PubMed before using Google Scholar or Google. A source was eligible for inclusion if it mentioned the country’s screening program (clinical or imaging-based) and DDH was the pathology of concern. We excluded literature if it failed to indicate the country’s screening practice or if the pathology included non-developmental (i.e. teratologic or neuromuscular) hip conditions. The remaining countries’ government health ministries were queried if these searches yielded no results. The final search attempt was to translate “hip dysplasia” into a countries primary language and then search: (country name) (translation of hip dysplasia). The primary search goal was to identify a screening program, with a secondary goal of identifying two references per country. Congenital dislocation of the hip (CDH) was not included in the search strategy, as DDH has replaced this term globally. 20
Countries’ populations were recorded using the United States Census Bureau’s International Database tool (2023), which also contains information on sex frequency by age. 21 Population and sex data were included to speak to the potential magnitude of DDH diagnoses in a nation compared to the incidence reported in the literature. With the available incidence rates, a calculation of (countries’ overall population × percentage females 0–4 years old × incidence) provided a crude estimation of the number of affected females with DDH for various countries.
After the initial data were compiled, the identified literature was explored for the reported frequency of DDH per country. Special attention was made to record how the authors defined DDH, meaning hip dysplasia versus dislocation versus other. Data were compiled, and Microsoft Excel was used for descriptive statistics. Unpaired T-tests comparing countries’ populations were performed using STATA/1C 14.0 (Stata Statistical Software: Release 14; StataCorp LP, 2015, College Station, Texas, USA).
Results
Twenty-five countries were determined using the Bloomberg Global Health Indices; published screening programs were identified in 20 countries (80%). The five countries without searchable screening programs were Iceland, Singapore, Luxembourg, Cameroon, and Cyprus (Table 1). The populations of the unidentified countries were 10-fold smaller than those with searchable screening programs (7.7 million ± 12.7 vs 75 ± 14.1, p = 0.30). Most searchable countries were European (n = 16), with three Asian countries and one in Oceania, similar to the non-searchable countries (three European, one Asian, one African).
Clinical screening with selective universal screening (CS + SUS) was the most commonly observed recommendation. Four countries had universal US: Switzerland, Austria, Germany, and Slovenia. No countries employed radiographic screening. Geographically, these four countries are considered Central European. 22 A population difference of roughly 60 million was apparent in clinical versus US countries (CS: 88 million (SD = 155), US: 26 million (SD = 39), p = 0.44).
Incidence rates were expressly stated in the literature for nine countries (see Table 2). The cohort of interest varied widely for these data. Four references stated rates for DDH. These values ranged from 0.759 per 1000 patients with DDH (Japan 23 ) to 10.83 per 1000 (Crete, Greece 26 ). Other studies published rates referring to the severity of the DDH, such as specifying dislocation (as opposed to subluxation 32 ) or the Graf classification IIIA or IV. 9 Additional cohorts of interest included babies treated in an abduction brace, premature infants, and requiring hospitalization.28–30
Published DDH Incidence By Country.
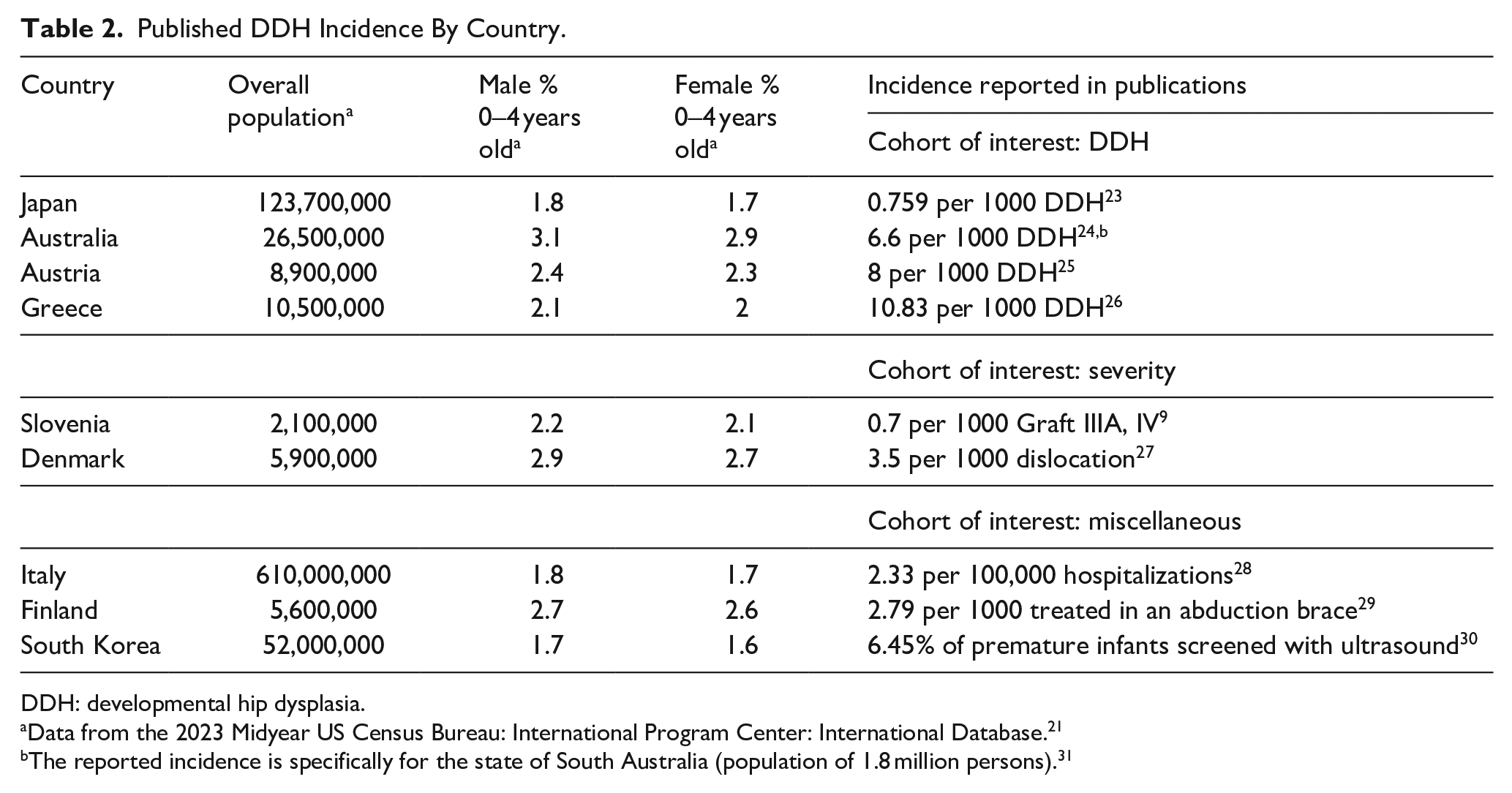
DDH: developmental hip dysplasia.
Data from the 2023 Midyear US Census Bureau: International Program Center: International Database. 21
The reported incidence is specifically for the state of South Australia (population of 1.8 million persons). 31
Conclusion
The findings of this investigation highlight the international inconsistencies regarding DDH screening and epidemiologic data. These results support previously published literature on variations in DDH screening, diagnosis, and management.1–3,6 Our results thus add to the literature on inconsistent approaches to DDH screening despite the various reports calling for consensus.2,6
More than a decade has passed since two international events meant to unify DDH management: the 2008 creation of the International Hip Dysplasia Institute and a 2011 study in Clinical Research and Relation Research publishing consensus criteria for DDH diagnostic criteria by the European Paediatric Orthopedic Society members.3,31 We theorized that the time lapse between these events and conducting this scoping review would lead to fewer variations in DDH management, in which we focused on screening programs. These results illuminated the persistent variability in DDH practices, disproving the thought that time would lead to a more standardized approach to this common pathology. Among European countries included in our investigation, no consensus was observed in screening practices, as evidenced by the mix of clinical versus US and several countries whose screening was not searchable.
The secondary aim of the investigation was to explore differences in how researchers reported frequencies of DDH in the literature, which was demonstrated in our findings. Existing literature commonly utilizes the historical incidence of one to two per 1000 babies with DDH.3,33,34 However, our findings demonstrate discrepancies in how the rates are defined and a wide range of data. Epidemiological data were determined for 9 of the 25 countries included in the study. The traditional definition (rate per 1000 patients with DDH) was used in four publications, two publications focused on DDH severity, and three definitions were miscellaneous.9,23–30 Inconsistent publishing of epidemiologic rates is problematic for researching DDH, as data cannot be compared across studies. This was true in our investigation, where variations in incidence rates limited our ability to calculate and meaningfully compare crude estimates of DDH across countries included in the study. It is curious and disappointing that the heterogeneity persists over two decades after a 1999 article in Pediatrics sought to establish a definition of incidence reporting to compare worldwide incidence rates. 5
The reasons DDH management remains non-standardized are multifactorial, for reasons such as population size and definition of incidence rates differences as illustrated by our findings, distribution of healthcare resources and infrastructure, and differing opinions on clinical exam findings suggestive of DDH.11,20,35 One country’s journey toward developing a newborn screening program highlighted several difficulties in reviewing the available literature. Singapore is one of the countries that did not have a searchable screening program. Several recent publications comment on individual, institutional progress toward a formal screening process; however, that does not appear nationally.10,11,36 Reasons for difficulties encompassed the gap between neonatology clinical screening and orthopedic referral, concerns a typical hip at the time of neonatal screen later develops dysplasia, variations in patient population characteristics, and ongoing debates about the timing of a screening ultrasound.10,11 The recent literature in Singapore provided an interesting look into the controversies present in a well-developed nation (ranked eighth in the global health index), which lacks a DDH screening program despite pediatric orthopedists and neonatologists’ recommendations.10,11,16,36
Our study has limitations and some study design flaws. Despite the rigorous and tiered search strategy, no screening program was identified in five countries, representing possible exclusion bias. Two citations per country were discovered in 8 of the 20 countries with searchable programs (40%), although 5 of those 8 countries had a third citation. The lack of multiple citations per country could not be avoided due to the study design; however, authors felt more citations may increase the data’s rigor. We cannot postulate a rationale for why certain countries are more represented in the literature than others. The difficulties in determining academic literature containing screening programs were further highlighted by three countries whose screening programs could only be found within a single publication. 1 The sole publication does not include a cited source for the data. We elected to record the screening programs documented in the common publication. However, we acknowledge the selection bias which may have occurred secondary to this decision. The employed search strategy may represent another area of criticism because a layperson Google search was included. It was necessary to have the tiered search to have a wide breadth of data for analysis on a topic with limited available citations. Finally, searching for screening strategies in countries’ native language could be perceived as a weakness in study design, albeit it was successful in identify an additional citation. 27
A scoping review was selected as the study design instead of a systematic review to focus on the counties being investigated. In addition, we aimed to synthesize the available evidence, understanding that appraising bias would be exceptionally difficult. 37 We further sought to characterize concepts leading to the lack of standardization in DDH, for example, reported incidence, which was also better suited for a scoping review. Although the timing of screening (such as hours or weeks of gestational age) is another controversial topic, we did not include this in the investigation’s scope.
DDH is a common pathology with international implications for patient care. Despite decades of calls for consensus by pediatric orthopedists and neonatologists, our findings support the existing literature on the global inconsistencies in DDH care, extending from screening protocols to reporting epidemiological data. We agree with the prior literature advocating for increasing consistency in DDH management or, at a minimum, increasing searchable transparency regarding how we manage these young patients. The inconsistencies underscored by this investigation may serve as a call for creating a consensus between international pediatric orthopedic societies, such as the Pediatric Orthopedic Society of North America and European Pediatric Orthopedic Society.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241229978 – Supplemental material for Globally inconsistent: Countries with top health indices erratic developmental hip dysplasia screening protocols
Supplemental material, sj-pdf-1-cho-10.1177_18632521241229978 for Globally inconsistent: Countries with top health indices erratic developmental hip dysplasia screening protocols by Natalie L Zusman, Pablo G Castañeda and Rachel Y Goldstein in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Dr P.C. assisted in study design and critically reviewed and revised the manuscript. Dr N.L.Z. conceptualized and designed the study, carried out data analyses, wrote the manuscript, and compiled revisions to prepare final manuscript. Dr R.Y.G. assisted in study design and critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
Institutional review board approval was not sought for this study, as there were no human or animal participants, no health protected information obtained, and no reviewing of medical records. All data are publicly available on the Internet and pertain to national (not individual) level data.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.