
Abstract
Purpose:
Congenital femoral deficiency is characterized by limb length discrepancy and genu valgum. Lengthening of the femur along its anatomic axis increases valgus alignment by medial knee translation. Pairing limb lengthening with simultaneous medial distal femoral hemiepiphysiodesis can simultaneously correct two limb deformities.
Methods:
All skeletally immature patients with congenital femoral deficiency who underwent antegrade femoral lengthening and concomitant guided growth over a 4-year period were reviewed. Length and alignment data were quantified during lengthening, consolidation, and for 1 year after guided growth implants were removed or the patient reached skeletal maturity. Digital simulation was performed for all lengthenings to assess the mechanical alignment that would have been achieved had lengthening been performed without medial distal femoral hemiepiphysiodesis.
Results:
Nine patients (five males, four females, mean age = 12.3 ± 1.9 years) underwent 10 antegrade intramedullary femoral lengthenings with simultaneous medial distal femoral hemiepiphysiodesis. All had improvement in valgus alignment (average improvement in mechanical axis deviation was 18 ± 11 mm, average change in limb alignment was 6 ± 5°). In simulated lengthenings without guided growth, all limbs would have experienced increased lateral mechanical axis deviation of 5 ± 3 mm. The hemiepiphysiodesis implant and lengthening device were explanted simultaneously in 7 of 10 lengthenings.
Conclusion:
Simultaneous medial distal femoral hemiepiphysiodesis with antegrade femoral lengthening for ongenital femoral deficiency can minimize the number of surgical episodes for the skeletally immature patient. The lengthening device and guided growth construct can be removed simultaneously in a majority of cases, saving children one or two additional surgical treatments.
Introduction
Congenital femoral deficiency (CFD) occurs in 1 in 200,000 live births 1 and results in a limb length discrepancy (LLD) emanating largely from the femur. Shortening usually coexists with lateral femoral condyle hypoplasia and genu valgum. Distraction osteogenesis has been used for decades to correct LLDs in congenital limb deficiencies.2,3 External fixation has the potential to lengthen and correct deformities that occur during the lengthening process, 4 but this approach has a unique complication profile and steep learning curve. 5 Motorized internal nails have been used to perform distraction osteogenesis in recent years and minimize select complications (i.e. pin site infections, pain, scarring) while improving the patient experience during lengthening.6,7
Implanted motorized lengthening devices lengthen the femur along the anatomic axis, which will medialize the distal femoral segment and therefore lateralize the weight-bearing line (i.e. increase knee valgus). Techniques to mitigate knee valgus during lengthening of a congenitally short femur include performing a distal femoral corrective osteotomy or combining the treatment with medial distal femoral hemiepiphysiodesis (MDFH) if the patient is skeletally immature. At our institution, LLD in CFD has been routinely treated with combined use of an antegrade lengthening device with MDFH of the distal femur when pre-operative valgus is present, or when such a lengthening will incite or worsen such a deformity. The purpose of this study is to evaluate the effect of these paired procedures.
Our primary question was to quantify the extent to which combining these procedures affected the total number of surgical interventions needed to achieve both lengthening and deformity correction. Our secondary questions were to compare the mechanical alignment that would have occurred had MDFH not been performed and to assess whether patients undergoing the paired procedures experienced additional complications or surgeries related to the guided growth beyond planned implant removal.
Patients and methods
Study design
We retrospectively reviewed a consecutive series of skeletally immature patients with CFD undergoing concomitant antegrade, motorized intramedullary femoral lengthening with MDFH in a single surgical event, between 2016 and 2020. Children were excluded from the study for any of the following reasons: (1) they did not have a diagnosis of CFD, (2) lengthening and guided growth procedures were not performed simultaneously, or (3) if any additional femoral and/or tibial procedure(s) was/were performed that could contribute to changes in the mechanical axis or deformity of the operatively treated limb. For the children meeting inclusion and exclusion criteria, demographic, surgical, and radiographic data were extracted from the medical record. The total number of operations required for placement and removal of all implants was also recorded. This study was approved by our Institutional Review Board with a waiver for informed consent.
Surgical procedure
All children in the study underwent antegrade, motorized, internal femoral lengthening with either a FITBONE®, (ORTHOFIX, Bussolengo, Italy) nail, or a PRECICE® antegrade trochanteric entry nail (NuVasive®, San Diego, CA, USA), along with application of a single medial distal femoral guided growth plate (ORTHOFIX®).
Length and deformity assessment were performed using full-length standing radiographs obtained within 3 months pre-operatively, at the onset of consolidation of the lengthening site (i.e. post-lengthening), and every 3 months thereafter. Guided growth implants were removed when a neutral mechanical axis was achieved on patients with <2 years of skeletal growth remaining, and slight overcorrection was the target for patients with more than 2 years of skeletal growth (goal 2–4° varus).
Radiographic measurements
LLD, mechanical axis deviation (MAD), coronal plane femoral-tibial angle (FTA), mechanical lateral distal femoral angle (mLDFA), medial proximal tibial angle (MPTA), and length achieved were measured on digital radiographs according to standard deformity analyses. The three time points were the immediate pre-operative alignment, the post-lengthening alignment (the end of the lengthening process and onset of regenerate consolidation), and the “final measurements”—meaning those obtained at the time of guided growth plate removal. A fourth measurement was obtained 1 year after guided growth implant removal or skeletal maturity. For each radiographic measurement, the rate of change per month was calculated by dividing the magnitude of coronal plane correction by the duration of MDFH treatment. By convention, valgus was denoted positive and varus negative.
Digital simulation of limb deformity without MDFH
Each lengthening plus MDFH was compared to its simulated counterpart without MDFH with surgical planning software (Bone Ninja 5.0.3, Apple iPad, Cupertino, CA, USA). This was accomplished in the following fashion: pre-operative radiographs were templated to achieve the identical magnitude of femoral lengthening along an intramedullary implant within the anatomic axis of the femur. MAD, FTA, mLDFA, and MPTA were obtained at the final alignment of this “simulated lengthening.” This approach provided data on femoral segment and overall limb alignment that would have occurred if hemiepiphysiodesis had not been performed at the time of lengthening.
Statistical analyses
For the purposes of data analysis, positive values for MAD and FTA denote lateral/valgus measurements, and negative values denote medial/varus measurements. Rates of changes in MAD, FTA, and LDFA were calculated for the lengthening and consolidation phases of treatment. Descriptive statistics were used for all parameters.
Results
Nine children undergoing a total of 10 lengthening procedures were eligible for analyses. Demographics are shown in Table 1, denoting five male and four female patients and a mean age of 12.3 ± 1.9 years at the time of surgery. The mean amount of days of lengthening was 62 ± 18 days, and the mean total duration of treatment with guided growth was 310 ± 119 days. Prior to surgery, the mean pre-operative MAD was 12 mm, FTA 4°, LDFA 86°, MPTA 89°, and LLD 60 mm. The mean post-lengthening MAD was 8 mm, FTA −1.9°, LDFA 89°, MPTA 89°, and lengthening achieved was 43 mm. At the time of guided growth implant removal, the final MAD was −9 mm, FTA −3°, LDFA 91°, and MPTA 88°. At final follow-up radiographs, mean MAD was 1 mm (range = −6 to 11 mm).
Lengthening characteristics in 10 antegrade femoral lengthenings with simultaneous medial distal femur hemiepiphysiodesis.
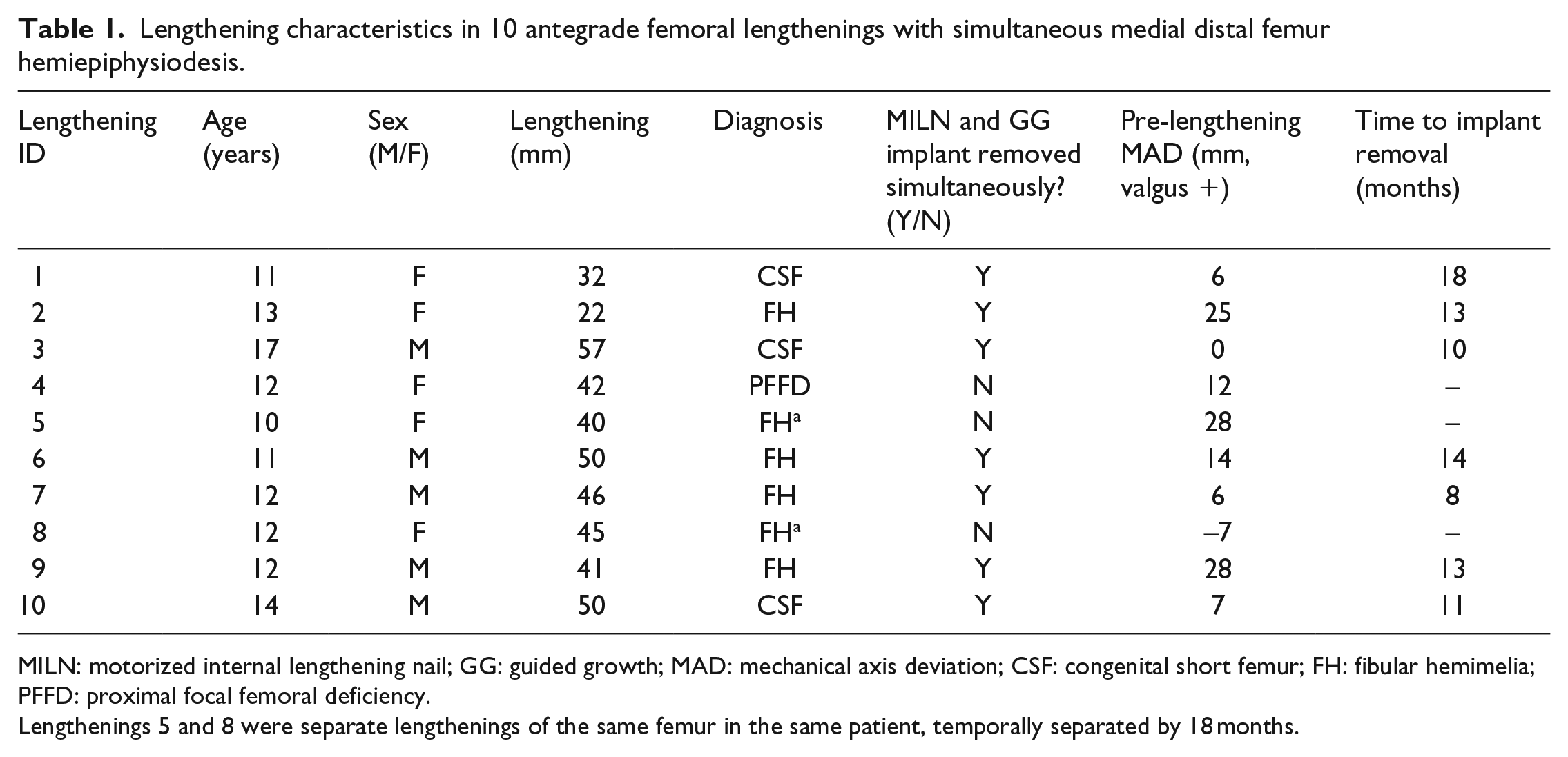
MILN: motorized internal lengthening nail; GG: guided growth; MAD: mechanical axis deviation; CSF: congenital short femur; FH: fibular hemimelia; PFFD: proximal focal femoral deficiency.
Lengthenings 5 and 8 were separate lengthenings of the same femur in the same patient, temporally separated by 18 months.
There were improvements in MAD (mean = 12 ± 12 mm pre- to −6 ± 8 mm post), FTA (mean = 5 ± 4° pre to −2 ± 4° post), and LDFA (mean = 84 ± 3° pre to 89 ± 3° post) in all patients by the time of guided growth implant removal. No appreciable changes occurred in MPTA. This result is expected based on the exclusion of individuals with procedures performed on the tibial segment, allowing for an internal control for measurement error.
The mean rate of deformity correction during lengthening was 0.1 mm/month for MAD, 0.1°/month for FTA, and 0.5°/month for mLDFA. After lengthening was completed, the rate of change of each parameter was MAD 2 mm/month, FTA 0.1°/month, and LDFA 0.5°/month. No patients went on to require distal femoral osteotomy for residual coronal plane deformity after guided growth.
The motorized nail and guided growth implant were removed concomitantly in 7 of 10 lengthenings, all between 8 and 18 months after index surgery (Figure 1). There were no complications referable to MDFH in any patient. One patient who underwent two motorized lengthenings 2 years apart (lengthenings 5 and 8, Table 1) had the MDFH implant placed at the time of a first motorized lengthening, but valgus remained at the time of motorized nail removal. The MDFH implant remained, and this was removed in an entirely separate procedure (after a second lengthening but not simultaneous with second nail removal).
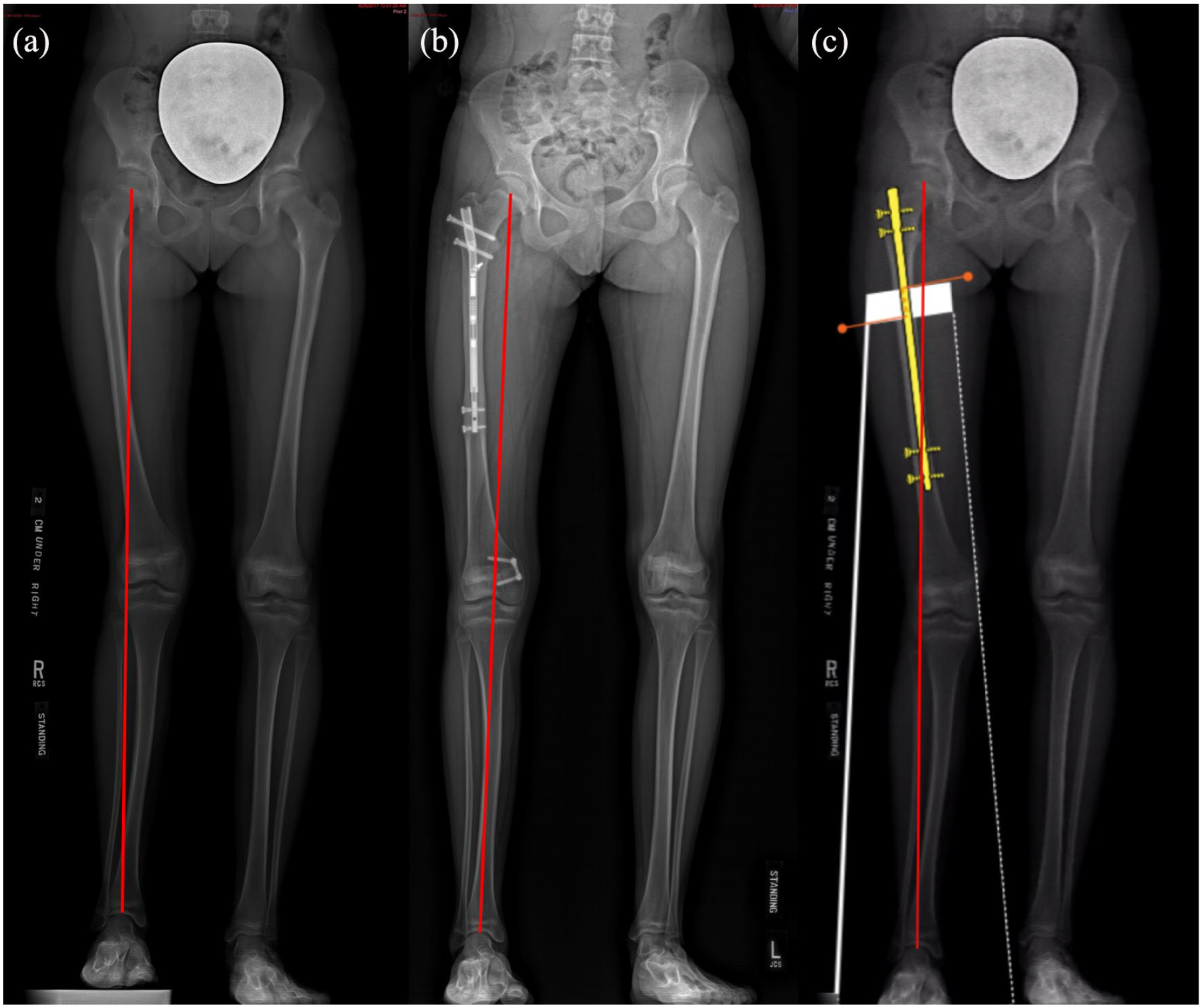
A 13-year-old female (lengthening ID 2) underwent a 2.2-cm right femoral lengthening with a motorized internal lengthening nail. Pre-operatively, the mechanical axis was deviated 25 mm into the lateral compartment (a). After 13 months, lengthening site had completely consolidated and MDFH had corrected the mechanical axis to neutral alignment (b). Had surgical lengthening been performed identically but without MDFH, the MAD would have worsened to 28 mm of lateral deviation (c). Both the lengthening and device and guided growth implant were removed simultaneously.
Simulated data for lengthening without MDFH revealed that all MAD and FTA measurements would have worsened (i.e. more valgus would have occurred) if lengthening had been performed in isolation (Figure 2). The addition of medial distal femur hemiepiphysiodesis resulted in a final limb alignment of mean −2 ± 4°, range −5 to 6° (Table 2). Up to 5° of “rebound” valgus, alignment was observed in most patients in the 1 year following guided growth implant removal (Table 3).
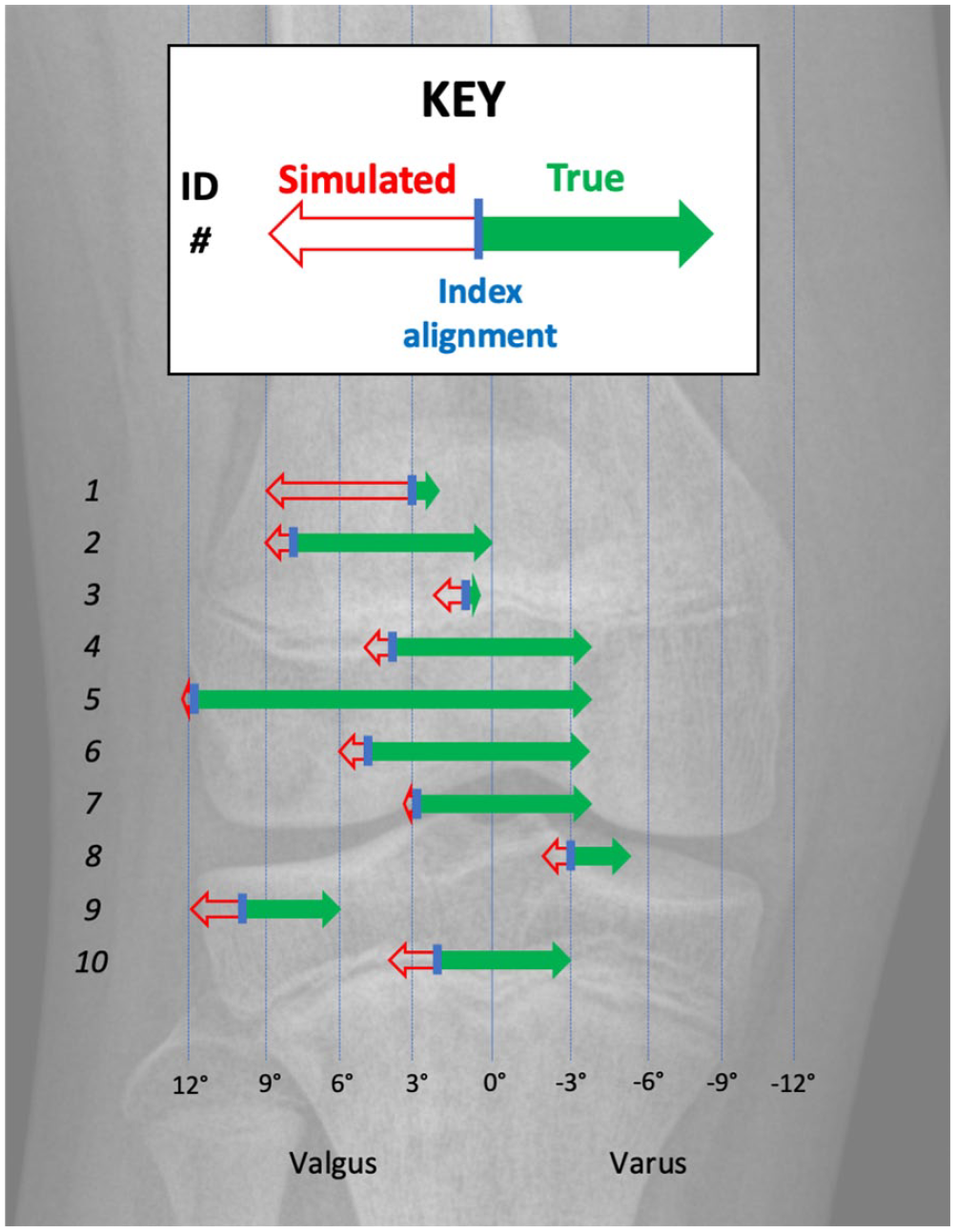
Graphical representation of the alteration in the weight-bearing line (mechanical axis). Italicized numbers at left denote the lengthening ID, consistent with Tables 1 and 2. Alignment before treatment is denoted by the small blue vertical line. The digitally simulated lengthening without MDFH is denoted by a red arrow pointing to the final simulated mechanical axis. The real-world alignment achieved by pairing MDFH with lengthening is denoted by the green arrow, which points to the final mechanical axis at the time of guided growth implant removal. Note that the tibiofemoral joint pictured is a visual representation of the quantitative data, utilizing the radiographs of a healthy 12-year-old child’s knee (average age at surgery in this series). Note that lengthenings 4, 5, and 8 were the three patients who had continued guided growth after lengthening nail removal.
Details of achieved and simulated mechanical alignment of operatively treated limbs.
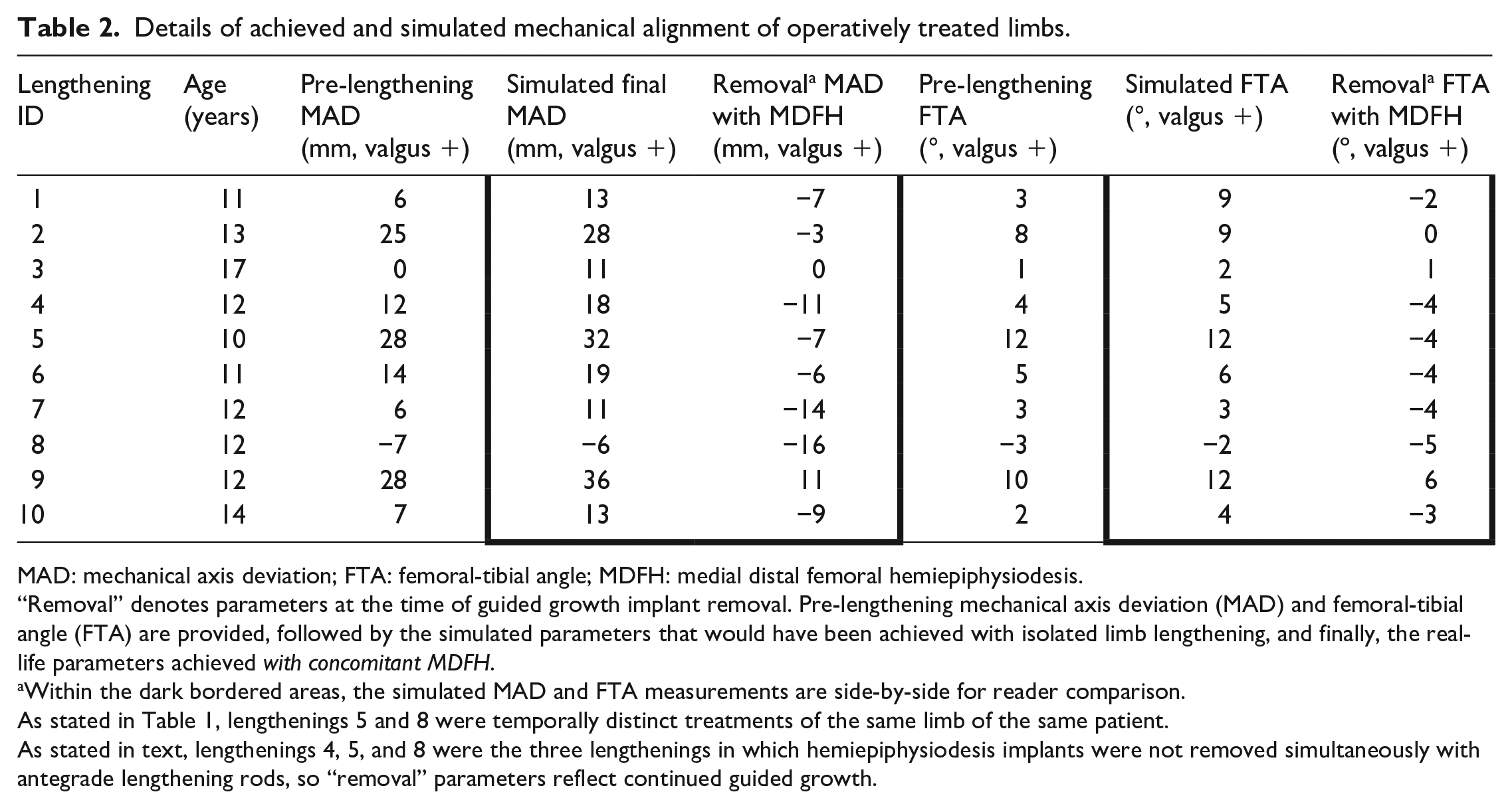
MAD: mechanical axis deviation; FTA: femoral-tibial angle; MDFH: medial distal femoral hemiepiphysiodesis.
“Removal” denotes parameters at the time of guided growth implant removal. Pre-lengthening mechanical axis deviation (MAD) and femoral-tibial angle (FTA) are provided, followed by the simulated parameters that would have been achieved with isolated limb lengthening, and finally, the real-life parameters achieved with concomitant MDFH.
Within the dark bordered areas, the simulated MAD and FTA measurements are side-by-side for reader comparison.
As stated in Table 1, lengthenings 5 and 8 were temporally distinct treatments of the same limb of the same patient.
As stated in text, lengthenings 4, 5, and 8 were the three lengthenings in which hemiepiphysiodesis implants were not removed simultaneously with antegrade lengthening rods, so “removal” parameters reflect continued guided growth.
Coronal alignment parameters at the time of guided growth implant removal and 1 year later (or skeletal maturity).
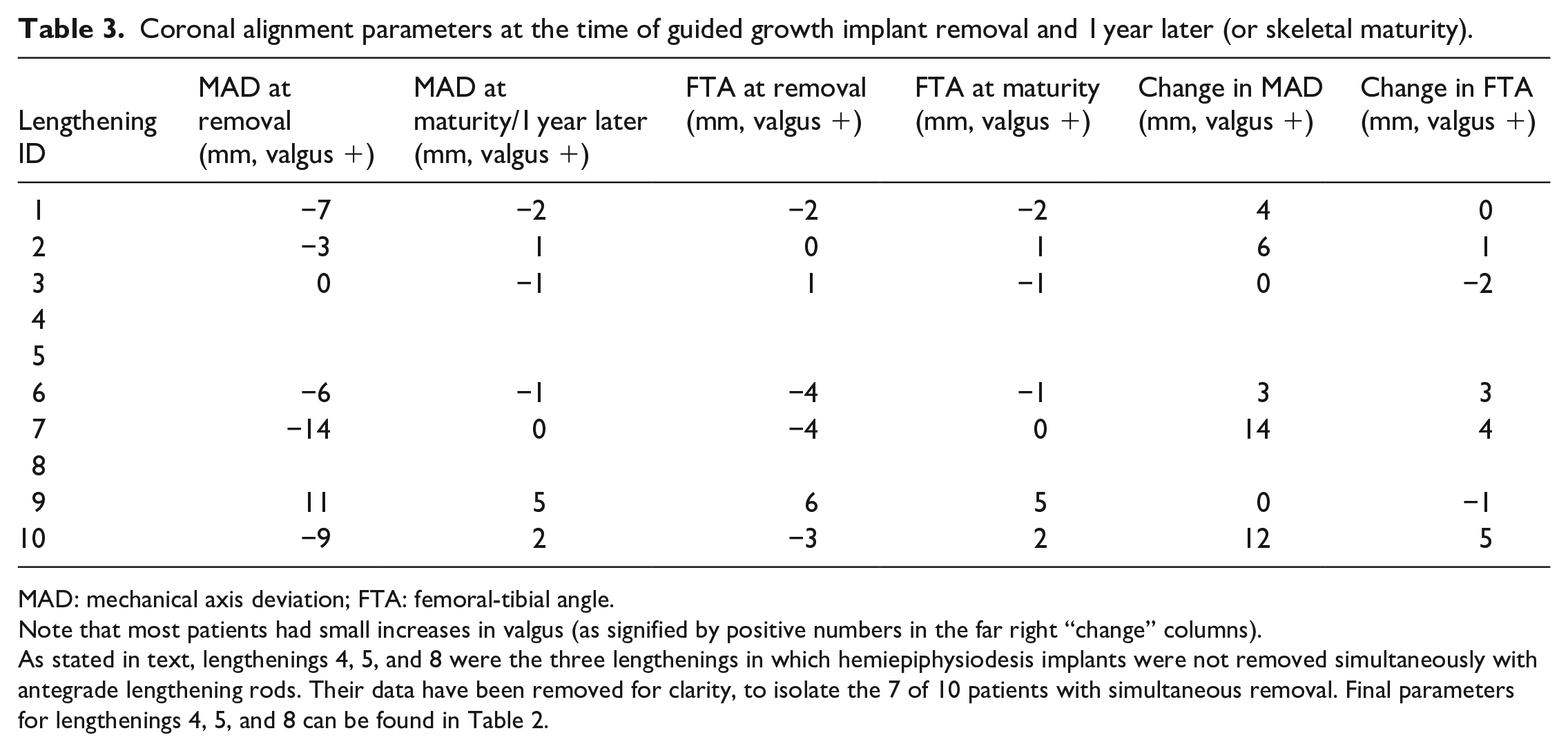
MAD: mechanical axis deviation; FTA: femoral-tibial angle.
Note that most patients had small increases in valgus (as signified by positive numbers in the far right “change” columns).
As stated in text, lengthenings 4, 5, and 8 were the three lengthenings in which hemiepiphysiodesis implants were not removed simultaneously with antegrade lengthening rods. Their data have been removed for clarity, to isolate the 7 of 10 patients with simultaneous removal. Final parameters for lengthenings 4, 5, and 8 can be found in Table 2.
Discussion
Children with CFD often have LLD accompanied by ipsilateral genu valgum and lateral femoral condyle hypoplasia. In the past, lengthening would have been performed with an external fixator and the pre-operative valgus (or any deformity acquired during lengthening) could have been corrected during or at the terminus of lengthening with a number of adjunctive techniques.4,8–11 Valgus correction is a target of orthopedic treatment because of its hypothesized role in abnormal joint stresses and degenerative changes, 12 particularly in the setting of congenital limb deficiencies wherein knee joints are often cruciate deficient and clinically unstable. Recurrence of coronal deformities has been observed in children with CFD undergoing either lengthening or guided growth treatment. 13 In addition to these alignment considerations, surgical lengthening of congenital limb deficiencies has a high learning curve with potentially devastating complications if over lengthening (>15% of starting length) is performed.14,15
Trochanteric entry nailing of the femur has been suggested to be safe procedure in older children, 16 and motorized lengthening nails with this entry point have been used without reports of avascular necrosis in children as young as age 9 years. 17 The technique is employed at a bone age of minimum 10 years at the authors’ institution in select cases. If trochanteric nailing is performed on a skeletally immature patient with pre-lengthening valgus, guided growth presents an opportunity to improve mechanical alignment with small surgical risk. The alternative is to perform a procedure with larger blood loss, operative time, and recovery (namely, separate osteotomy with internal fixation). Once patients are skeletally mature, retrograde lengthening and deformity correction can be performed at the same anatomic site. 18
Radler et al. 17 reported on use of the PRECICE® magnetic lengthening nail in children, concluding that it was safe and effective in this age group. Among 47 lengthenings performed in skeletally immature patients, guided growth was paired with the lengthening in 14 cases, although no further granular detail was provided. The authors suggested that hemiepiphysiodesis was often employed for limb malalignment antecedent to or during the lengthening. Jardaly and Gilbert 19 recently reported on seven patients (average age of 13.6 years) on whom antegrade lengthening was performed with concomitant distal femoral osteotomy with successful length and alignment correction. Laufer et al. 20 reported on tibial and femoral stapling for hemiepiphysiodesis either concurrent with or separate from femoral lengthening in children. They reported that 53% of patients with pre-lengthening valgus had good realignment at maturity, and that larger discrepancies and more severe angular deformities were less likely to both be corrected accurately.
In the present series, 70% of patients were spared one or two additional surgeries by pairing the hemiepiphysiodesis and lengthening procedures. Stated differently, 70% of patients achieved both length and deformity correction with only a single episode of orthopedic implantation and removal. The valgus deformities in these patients were all mild to moderate before lengthening (≤12°) and simulation suggested all deformities would have worsened without MDFH. Even two older children in this series, chronologically aged 14 and 17 years, were able to garner mechanical axis improvement from the hemiepiphysiodesis. This technique avoids damage to the physis with retrograde nailing and decreases the possibility of miscalculation of final LLD, a potential outcome of antegrade nailing with distal osteotomies.
Radler et al. 13 reported on recurrence of varus or valgus malalignment in children with CFD undergoing lengthening or hemiepiphysiodesis. They concluded that more severe subtypes of fibular hemimelia with more ankle involvement appeared more prone to recurrent valgus, occurring in approximately half of cases. As a result, they recommended overcorrection when employing guided growth treatment. This has also been the experience of the senior author, who (when possible) tends to perform surgical lengthening and paired MDFH for congenital discrepancies in the adolescent years, both to achieve slight coronal overcorrection (2–4°) and leave less growth remaining for recurrence.
In the seven patients who had simultaneous removal of all implants, “rebound” into genu valgus was seen in the following year, consistent with other reports. This was unpredictable but up to 5° of additional valgus did develop after guided growth treatment ended, even in individuals near skeletal maturity (Figure 3). This would give credence to the expert opinion that small overcorrection into varus may be desirable if significant growth remains.
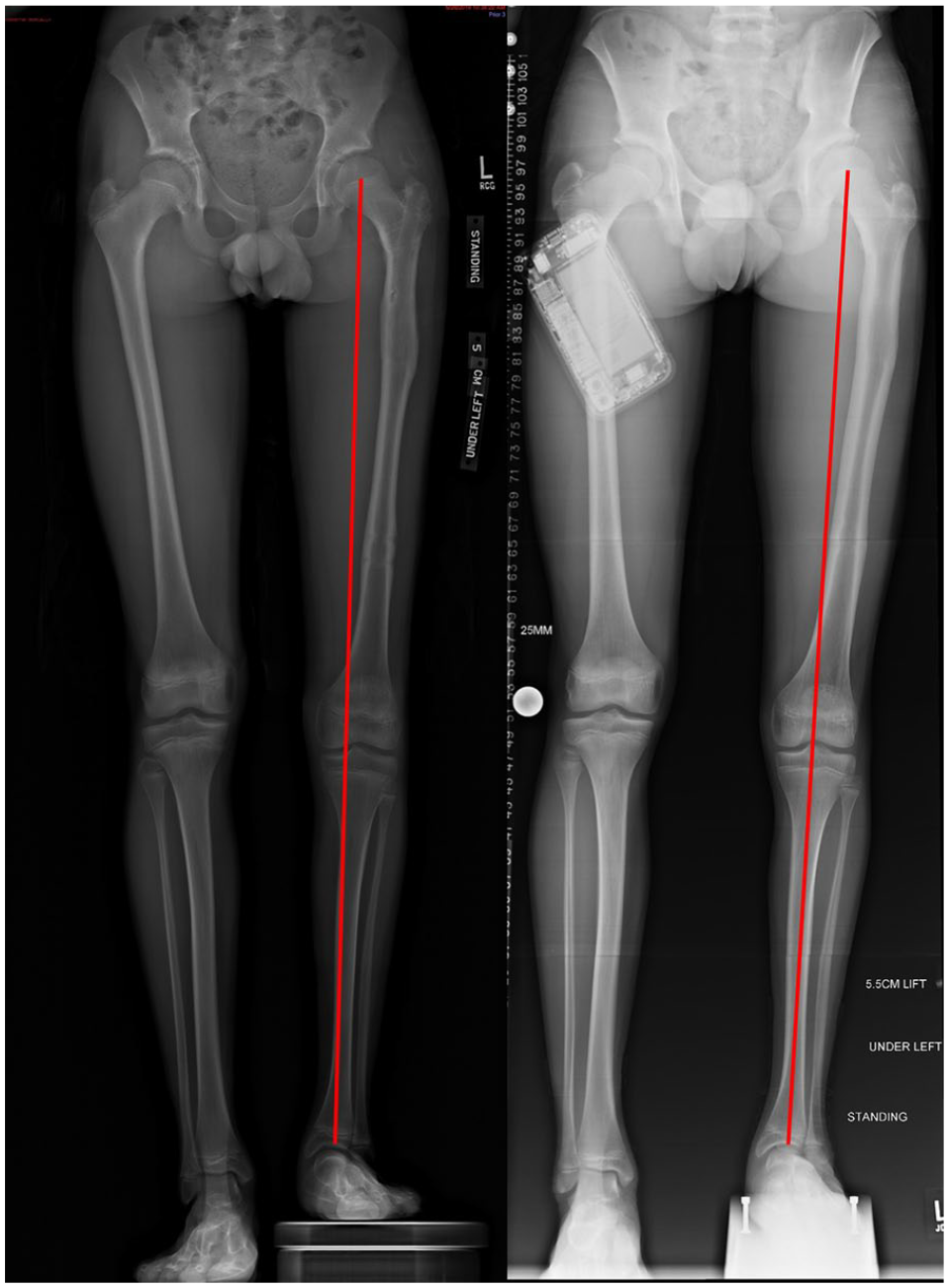
Representation of recurrent valgus alignment after antegrade femoral lengthening and simultaneous MDFH. This 13-year-old boy underwent left motorized femoral lengthening and MDFH, with implants removed simultaneously. At left, immediately after implant removal, there is mild varus alignment (14 mm of MAD into the medial compartment or 4° varus). One year later, at right, the mechanical axis is neutral (0 mm MAD, neutral coronal alignment), suggesting “rebound” valgus. Also notable are characteristic morphologic features of patients with fibular hemimelia, including a ball-and-socket ankle deformity.
This series is limited by observational, retrospective data and the use of simulated comparison groups to establish a counterfactual treatment effect (i.e. femoral lengthening without MDFH). Congenital short femurs were studied because of the proclivity of these limbs to experience recurrent valgus, but in principle, any immature femur with growth remaining would be amenable to this combined treatment. The simulation of lengthening without MDFH assumes that deformities are not introduced during lengthening, which is consistent with our experience with routine antegrade intramedullary lengthening of pediatric femora, even for congenital discrepancies. In addition, trochanteric nailing of the skeletally immature femur could induce coxa valga from trochanteric inhibition (not observed herein) or asymmetrical loading of the distal femoral physis. 21 We excluded patients who underwent other procedures on the femur or tibia which would have affected overall alignment.
This study suggests that the data obtained herein are a mathematical “proof of concept”: the increase in valgus during antegrade femoral lengthening is simply a feature of the osteology of the human femur and is accentuated by the pathoanatomy of CFD. If children are sufficiently immature, MDFH will generally be able to accomplish deformity correction. The burden of additional surgery can be lessened in many patients with congenital limb discrepancies because length and MAD can often be corrected simultaneously.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241229619 – Supplemental material for Antegrade femoral lengthening and simultaneous hemiepiphysiodesis for congenital femoral deficiency
Supplemental material, sj-pdf-1-cho-10.1177_18632521241229619 for Antegrade femoral lengthening and simultaneous hemiepiphysiodesis for congenital femoral deficiency by Andrew G Georgiadis, Patrick D Albright, Aaron J Huser, Susan A Novotny and Mark T Dahl in Journal of Children’s Orthopaedics
Footnotes
Author contributions
A.J.H., A.G.G., and M.T.D. contributed to conception and design. A.G.G. and M.T.D. contributed to analysis and interpretation. A.J.H., A.G.G., and S.A.N. contributed to data collection. A.G.G., M.T.D., and S.A.N. contributed to writing the article. A.G.G., M.T.D., S.A.N., and A.J.H. contributed to critical revision of the article. A.G.G. and M.T.D. contributed to final approval of the article. A.G.G. and P.D.A. contributed to statistical analysis. A.G.G. and M.T.D. contributed to overall responsibility.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.T.D. is a paid consultant for NuVasive and Stryker Trauma.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by generous donors to Gillette Children’s Hospital.
Ethical approval
This study was approved by The University of Minnesota Institutional Review Board, ID 1406M51162 on 10 January 2023.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.