
Abstract
Substantial advances in the treatment of early onset scoliosis (EOS) over the past two to three decades have resulted in significant improvements in health-related quality of life of affected children. In addition to classifications that address the marked heterogeneity of this patient population, increasing understanding of the natural history of the disease, and new implants and treatment techniques have resulted in innovations unlike any other area of pediatric orthopedics. The growing understanding of the interaction between spinal and thoracic growth, as well as dependent lung maturation, has had a lasting impact on the treatment strategy of this potentially life-threatening disease. The previous treatment approach with early corrective fusion gave way to a growth-friendly concept. Despite the steady development of new growth-friendly surgical treatment options, whose efficacy still needs to be validated, as well as a revival of conservative growth control with serial casts and/or braces, the psychosocial burden of the long lasting and complication-prone treatments remains high. As a consequence, EOS still represents one of the greatest pediatric orthopedic challenges.
Introduction
Early onset scoliosis (EOS) refers to a deformity of the spine (scoliosis and/or kyphosis), with or without involvement of the thorax, diagnosed before the age of 10. 1 In 2014, the Classification of Early Onset Scoliosis (C-EOS) has been introduced to encounter the heterogeneity of the affected patient population. 2 The C-EOS uses a continuous age prefix and four deformity characteristics: etiology, major curve magnitude, annual progression rate (APR), and kyphosis. In terms of etiology, a distinction is made between neuromuscular, congenital, syndromic, and idiopathic EOS. Validation of the C-EOS showed substantial to excellent interobserver and intraobserver reliability. 3 The natural history varies with the underlying disease and may be associated with increased mortality.4,5 At the same time, the principle of early definitive spinal fusion, which was still practiced until the beginning of the new millennium, has taught us not only revision rates of up to 39% but also the disastrous influence of a short (thoracic) spine on pulmonary function. 6 Children who underwent spondylodesis before the age of 9 showed a forced vital capacity <50% with associated restrictive ventilatory dysfunction when the length of the thoracic spine was significantly shortened (T1-T12 distance < 18 cm). 7 The interdependence of spinal and thoracic growth and lung maturation has been substantiated by the achievements of Dr Robert Campbell Jr. and his description of Thoracic Insufficiency Syndrome (TIS) as the inability of the thorax to provide normal respiration and lung development. 8 As a consequence, the conservative and surgical treatment of EOS must, in addition to controlling the deformity, primarily focus on maintaining, or ideally stimulating, the growth of the spine and thorax in order to achieve the targeted minimum T1-T12 distance of 18–22 cm, as a prerequisite for normal lung function. The development of new and the optimisation of existing treatment methods have recently been influenced by the consideration of aspects such as health-related quality of life (HrQoL) and psycho-social burdens for the affected children and their relatives. Additional comorbidities increase the already high-risk profile and require, in addition to early multidisciplinary management, treatment approaches with as few complications as possible and a minimum number of necessary (surgical and anesthetic) interventions.
In addition to a consequent use of the C-EOS, the validated Early Onset Scoliosis Questionnaire (EOSQ-24) should consistently be used to provide optimal and reproducible configuration of treatment management, outcome analysis, communication, and research. The EOSQ-24 consists of 24 items pertaining to the patient’s Health-related Quality of Life (HrQoL) during the past 4 weeks. 9 The 24 questions cover the following 11 areas: General Health, Pain/Discomfort, Pulmonary Function, Transfer, Physical Function, Daily Living, Fatigue/Energy Level, Emotion, Parental Impact, Financial Impact, and Satisfaction. The EOSQ-24 has been proven as a valid, reliable, and responsive instrument that is able to serve as a patient-reported outcome measure for EOS patients. 9 The questionnaire has meanwhile been validated in nine languages and can be found, for example, via the Pediatric Spine Foundation homepage (https://pediatricspinefoundation.org/). The efforts achieved to increase quality in treatment and research can be further improved by national and international multicenter studies with a relevant increase in patient numbers. 10
However, despite the aforementioned comprehensive and systematic approach to classification, treatment options, and outcome evaluation, there is still little consistent expert consensus on the optimal choice and design of adequate treatment for EOS. 11 In 2020, Hughes et al. 12 constructed a six-case survey that was sent to 20 EOS world thought-leaders with an average clinical experience of 24 years. The response rate was 100% with no consensus on any case.
Diagnosis
Medical history and physical examination
A comprehensive past and current medical history represents the fundament in the evaluation of a patient with EOS.13,14 The personal history begins with pregnancy and birth and includes further health, motor and neurological development, as well as previous surgical procedures or hospitalizations, neuromuscular or syndromic conditions, and respiratory infections. Family and social history can provide additional information about possible hereditary problems or environmental influences related to EOS. The disease-specific history should include age of onset, history of progression, and previous nonoperative and operative treatment. Current medications and known allergies should be documented. Additional neurological, urological, cardiological, neurosurgical, and endocrinological conditions should also be inquired. In the clinical examination, the overall health and nutritional status of the child must be considered, always including documentation of body height and weight, and dietry regimen. In ambulatory patients, a primarily dynamic assessment with observation of gait pattern and assessment of motor skills, such as toe-walking or bipedal and unipedal hopping, is very informative and allows the child to build confidence. In addition to a thorough general clinical examination, spine-specific assessment includes the evaluation of spine, chestwall, and rib deformities, as well as inspection for dimpling, sinus tracts, or other cutaneous signs of spinal dysraphism.
Radiographic evaluation
A posteroanterior and lateral full spine radiograph, preferably with a low-dose EOS imaging system and whenever possible in standing position, is the first line of diagnostic imaging. In addition to objectifying the spinal deformity and potential failure of segmentation and/or formation, abnormalities of the rib cage and ribs can be assessed and statements about skeletal maturity can be made based on the radiographic aspect of the different growth zones.
There is still no clear consensus regarding the routine performance of magnetic resonance imaging (MRI) in patients with EOS. In a global cohort of 836 patients, the overall prevalence of abnormal MRI findings was 24%. 15 In addition to the routine performance of an MRI prior to any planned spine intervention, we accordingly consider an MRI to be generally indicated also in case of an observational approach. However, in the absence of anamnestic and clinical neurological abnormalities, we try to postpone the MRI until it can be performed without the need for anesthesia.
An additional computed tomography (CT) scan is helpful to further investigate bony abnormalities and three-dimensional (3D) reconstructions or even CT-based 3D-printed models of the affected part of the spine can comprehensively illustrate the underlying bony pathology and can also be extremely valuable for planning a surgical intervention.
Conservative treatment
Although there have been no relevant innovations in the field of conservative treatment approaches for EOS in recent years, serial casting and/or the use of braces have revived increased attention due to the high complication rate and the associated need for unplanned re-operations (UPROR) in surgical growth-friendly techniques. This trend is also reflected in a consensus study on the evaluation and evolution of the preferred treatment options for EOS among a selection of renowned pediatric spine surgeons over the last 10 years.16,17 In 2020, 11 pediatric spinal surgeons with a mean number of 32 years in practice were invited to re-evaluate 315 idiopathic and neuromuscular EOS cases after a 10-year interval. Preferences for conservative management have increased, especially in younger children, and casting was preferred over bracing in infantile cases. 16
The methods used for bracing largely correspond to the principles of elongation, derotation, and flexion, based on the techniques of Mehta and Cotrel (traction and apical derotation) or Risser (traction and apical lateral translation), each described in the 1970s.18,19 While a sustainable correction or at least control of the deformity seems possible with noncongenital EOS in case of early treatment,19,20 conservative measures are often used to gain time until surgical intervention becomes necessary (“buy time strategy”) with some studies showing an average time gain of 2–3 years.21 –24
Despite the assumed non-invasive approach and the associated lower risk profile of conservative methods, possible effects on health-related quality of life (HrQoL) must be taken into account. 25 While patients with non-idiopathic EOS showed a decrease in the sub-domains “transfer” and “emotions” in the EOSQ-24, patients with idiopathic EOS experienced a deterioration in almost all sub-domains during and partly also after plaster or brace treatment. In addition, repetitive cast changes at 2- to 4-month intervals are traditionally associated with a high exposure to general anesthesia, which can lead to lasting negative effects on learning and behavioral functions, especially in children under 3 years of age. 26 However, a study investigating the radiological and clinical outcomes of serial body casting with and without general anesthesia in infantile idiopathic scoliosis (IIS) has shown that the hurdle of repetitive general anesthesia could be omitted in a selected population. 27 The study included 121 children who underwent serial casting for IIS. In 29 patients serial casting was performed awake, diverting the children’s attention with electronic devices. Although, these patients were older (median 3.4 vs 2.4 years), had a lower body mass index, and more severe curve magnitudes, they presented similar radiographic outcomes with regard to major curve correction, as well as gain in thoracic and total spine height, when compared to those who were casted under general anesthesia. This again is in contrast with the findings by Canavese et al. 28 who reported a better initial deformity correction in patients with juvenile scoliosis who were casted under general anesthesia, especially in combination with neuromuscular-blocking drugs. Further studies are necessary to address this relevant aspect more reliably.
Operative treatment
Surgical treatment of spinal deformities dates back more than 100 years. After the original goal of preventing further worsening of scoliosis and lowering mortality by aiming for uninstrumented bony fusion, the possibility of—at least partial—correction of a deformity by instrumented spondylodesis emerged with spinal implants introduced by pioneers such as Harrington, Luque, Cotrel, and Dubousset from the 1960s onwards. 29 Although primarily designed for adolescent and adult patients, these techniques were increasingly used for EOS that could no longer be controlled conservatively. After the initial use of periodically lengthened unilateral Harrington rods, or Luque trolley systems for passive growth control, a “claw foundation” with anchorage of a growing rod proximal and distal to the deformity, sometimes combined with apical fusion, has been described in the early 1990s. 30 Based on this, the use of dual growing rods with spine-based fixation above and below the deformity became the gold standard in the surgical treatment of progressive EOS. 31 In 2014, the different techniques for surgical growth-friendly management were divided into 3 groups, distinguishing between distraction- and compression-based systems, and growth-guiding techniques, which is still valid in principle. 32 However, with the introduction of motorized magnetically controlled growing rods (MCGRs), the heterogeneity in the choice of growth-friendly implants for the index surgery has decreased massively with a marked predominance of MCGR. 33 Recently, efforts have also been made to systematically characterize an older, heterogeneous EOS patient population, the so-called “tweeners,” who qualify for either growth-friendly treatment options or definitive fusion due to their age and skeletal maturity. 34
Vertical expandable prosthetic titanium rib (VEPTR®)
The main indication for VEPTR, originally provided by the inventor, Dr Campbell Jr, is the presence of TIS in skeletally immature patients. From an anatomical perspective, in addition to missing or fused ribs, a hypoplastic thorax, or EOS of congenital or neurogenic etiology without rib anomalies are also indications for VEPTR treatment (Figure 1). 35 Although often clinically evident, changes in lung function in VEPTR-treated patients are difficult to objectify with standard pulmonary function tests, and newer techniques based on dynamic magnetic resonance imaging may provide valuable evidence. 36
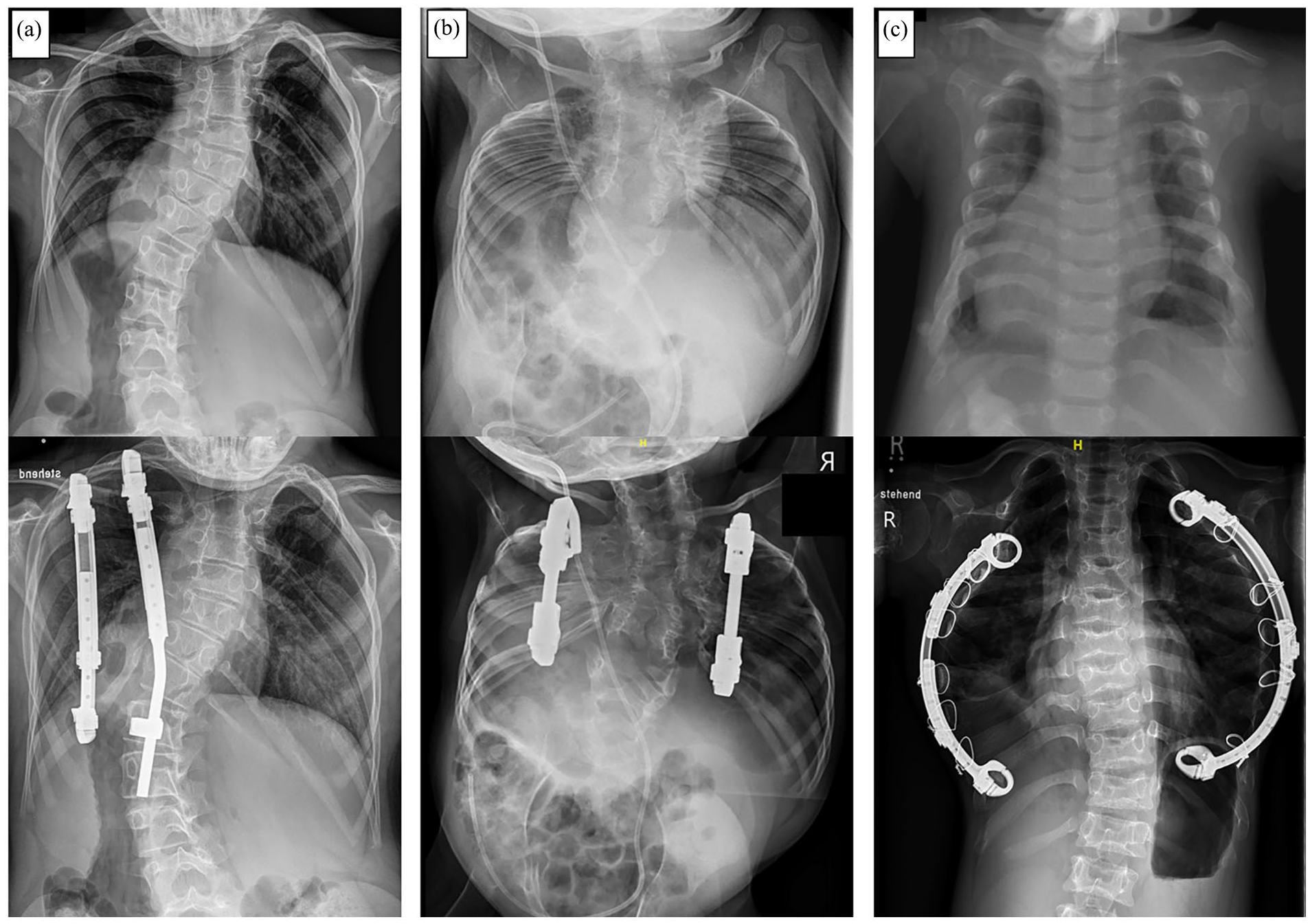
Common indications for the use of Vertical Expandable Prosthetic Titanium Rib (VEPTR) as a distraction-based growth-friendly technique in case of thoracic insufficiency syndrome (TIS): (a) Congenital early onset scoliosis (EOS) in combination with fused ribs. (b) Volume-depletion deformity (VDD) type IIIa in a patient with Jarcho-Levin syndrome with a foreshortened thorax. (c) VDD type IIIb in a patient with Jeune syndrome and a transverse constricted thorax.
The potential to improve lung function while indirectly controlling the spinal deformity has continuously expanded the range of indications for VEPTR, not least due to frequent reports of complications with traditional growing rods (TGR). However, the initial enthusiasm for spine-sparing deformity correction has gradually faded with an increasing number of reported complications, including the evidence of extraspinal ossifications along the implants and across ribs. 37 The avoidance of repetitive surgical implant lengthening with the availability of motorized distraction-based implants has further reduced the use of VEPTR.
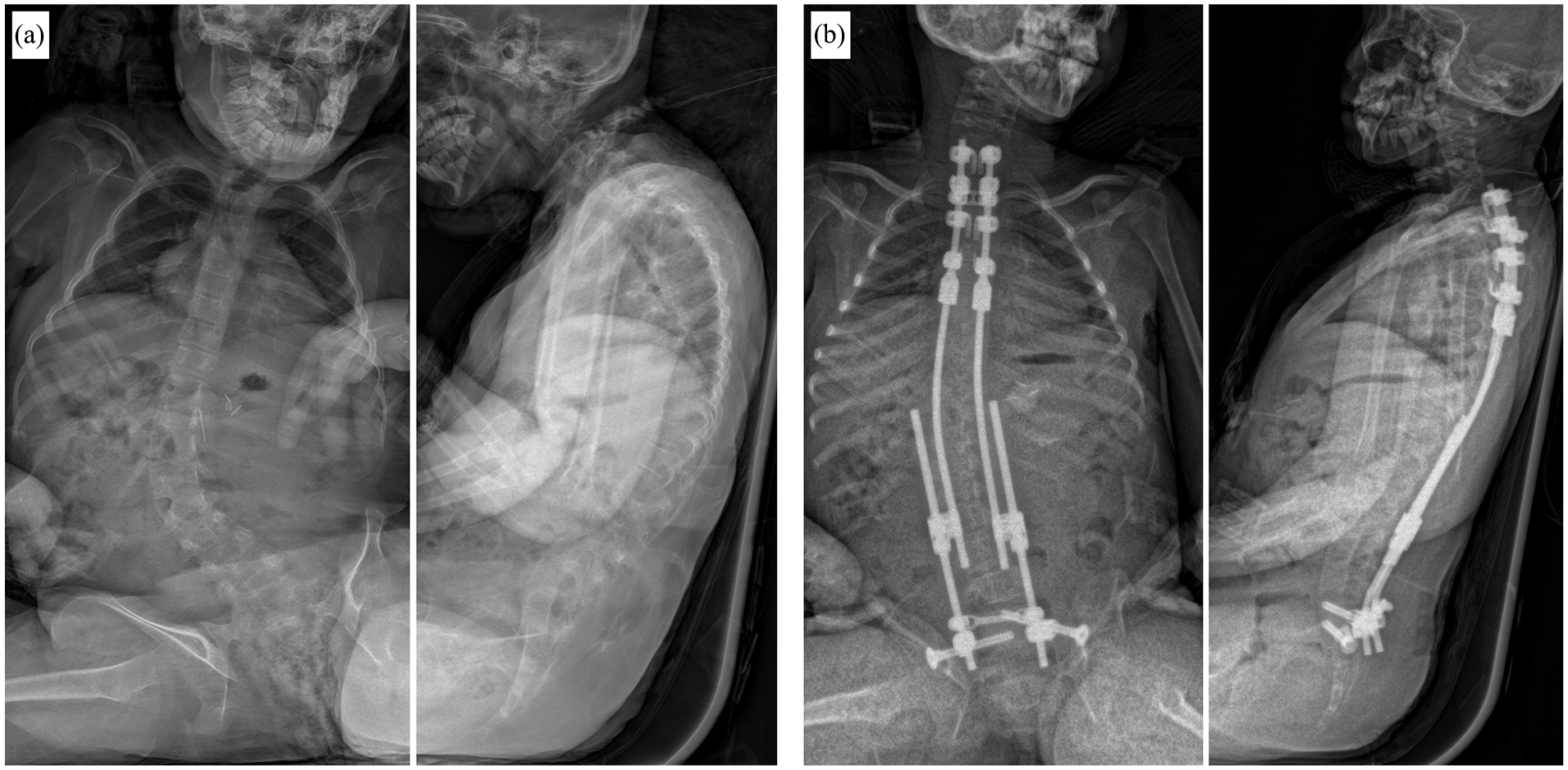
As with other distraction-based systems, VEPTR primarily follows a delaying fusion strategy, and the limited data and heterogeneity of the treated population limit the decision-making process for so-called “graduates” of growth-sparing surgery. In many cases, the decision on when to stop lengthening is less surgeon driven than more determined by curve progression, lack of further distraction, or complications. 38 Previous evidence of outcomes after final fusion with modest correction and high complication and reoperation rates, both in VEPTR patients and with other growth-friendly systems, prompted to rethink the original idea of controlling the deformity during growth and aiming for significant correction with conversion to final fusion (Figure 2).39 –41
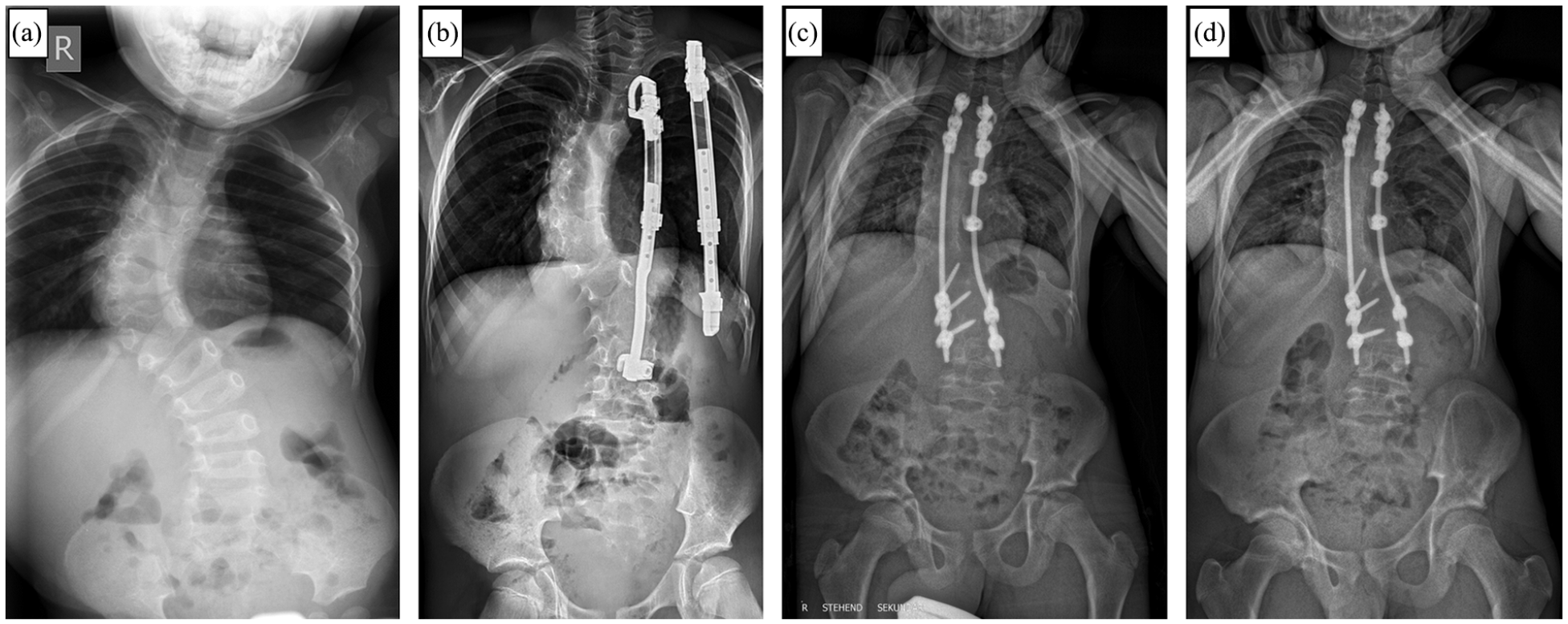
Course of a patient with congenital scoliosis and concave fused ribs before (a) and during (b) Vertical Expandable Prosthetic Titanium Rib (VEPTR) treatment. After frustrating lengthening attempts due to spontaneous stiffening of the spine and thorax over time, final fusion surgery had to be performed before reaching skeletal maturity (c). (d) Follow-up x-ray 3 years after conversion to final fusion.
Due to the more restrained use of VEPTR in recent years, there are only few valid data regarding patient-reported outcome. The complication-prone course and the necessity for repetitive surgical lengthening with encumbering cosmetic consequences explain the poor evaluations in regard to “pain”, “self-image”, and “function” (Figure 3). 42
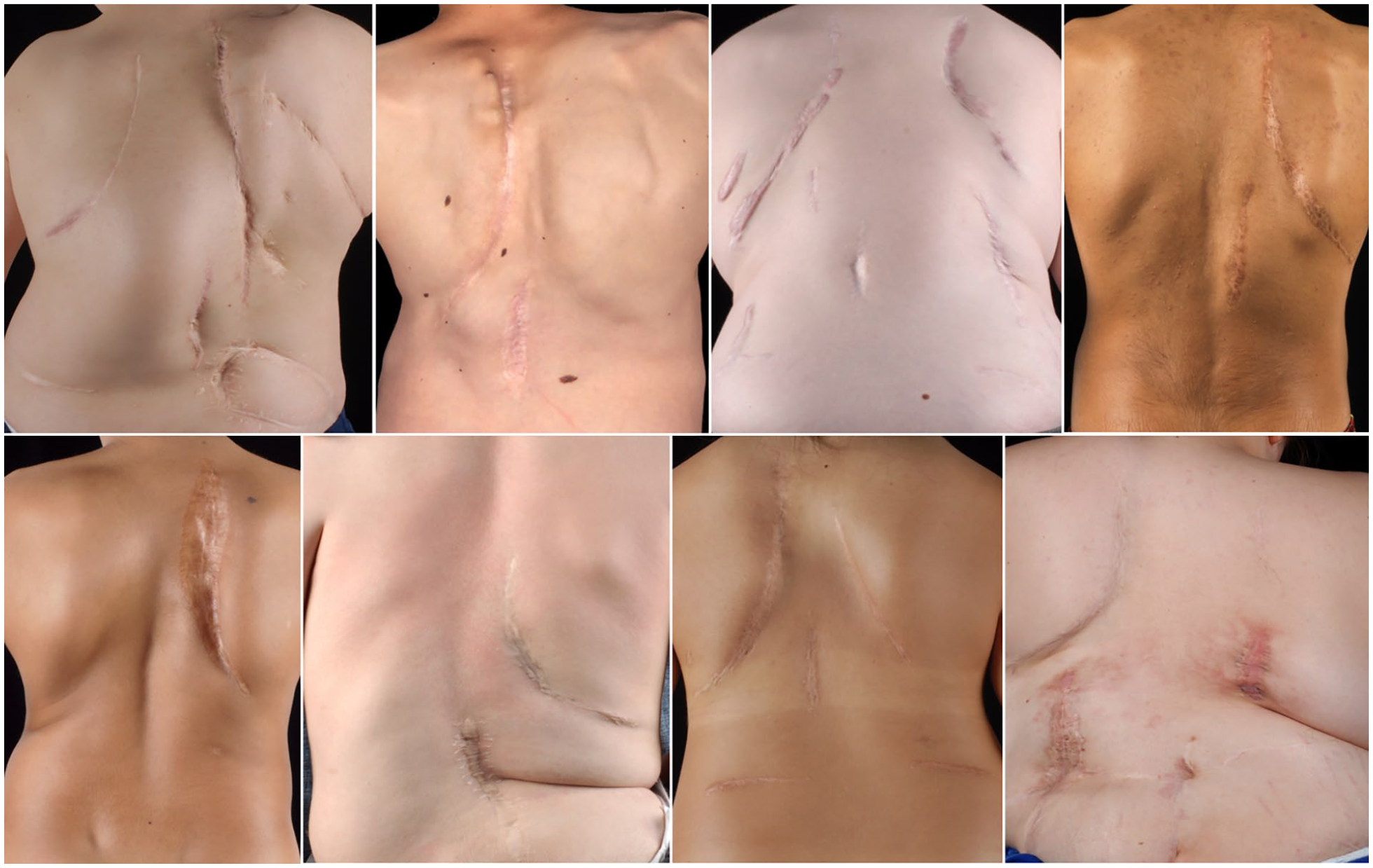
Clinical pictures of different patients treated with Vertical Expandable Prosthetic Titanium Rib (VEPTR) System. Tipically, a parascapular approach is used for the proximal rib anchors. Depending on the location of the distal foundation, the incision is either performed in the midline (for rib-to-spine constructs) or above the iliac crest (for rib-to-pelvis constructs). Due to the need for repetitive surgical implant lengthening, the scars tend to become broad and hypertrophic.
Growing rods
Progressive EOS in patients without thoracic or rib abnormalities and a normally segmented spine are the classic indications for Growing Rods (Figure 4). In the era of MCGR, the use of TGR has been significantly reduced. However, TGRs can still play a relevant role in patients of short stature with stiff, hyperkyphotic curves. 43 Dual rods are superior to single rods in terms of complications. 31 The extent to which this is true in regard of correction and control of deformity, as well as gain in length is controversial.31,44
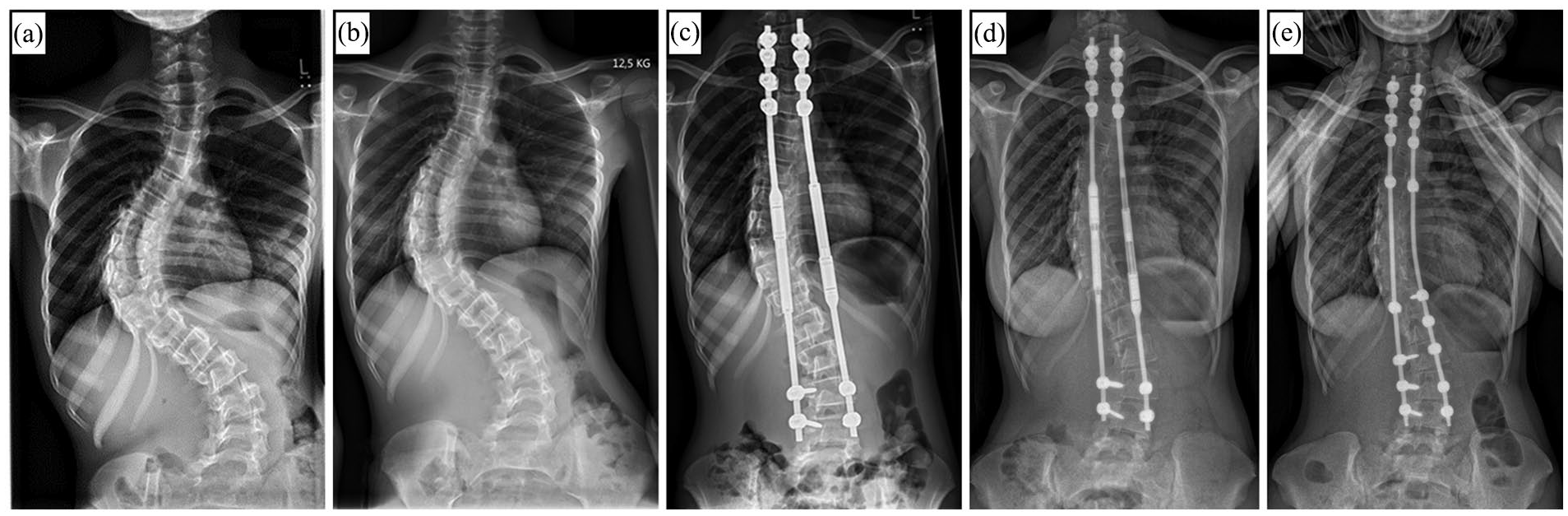
X-rays of a 9-year-old female patient with syndromic early onset scoliosis (EOS) before treatement (a), after 2 weeks of preoperative halo gravity traction (b), and after index surgery with magnetically controlled growing rods (MCGR) (c). (d) Radiograph 4 years after index surgery showing convex-sided failure to lengthen. (e) 2 years after conversion to definitive instrumented spinal fusion.
MCGRs do not require open lengthening, which, in addition to a reduction in peri- and intraoperative complications, has a particular effect on the psychosocial burden of patients and their relatives. 45 Accordingly, MCGRs are now used in >80% of index operations in EOS. 46 However, the initial enthusiasm gave way to the humiliating results of progressive complication rates with increasing follow-up,47,48 and it can be assumed that this number will soon decline. Based on an expert consensus, inadequate skin and soft tissue cover, a stiff spinal curve, a sagittal curve apex above T3, hyperkyphosis, or patients requiring repetitive MRI for their care were recently defined as contraindications for the use of MCGR. 49 Whereas in parallel, a syndromic EOS patient without prior surgical treatment and the possibility of using a 90-mm actuator was declared an ideal candidate for MCGR. 50 The supposed cost savings of MCGR over TGR has also recently been questioned due to frequent reports of early implant failure 51 and by the latest Field Safety Notice (FSN) in December 2021 in Europe, urgently recommending to change or remove the implant(s) after implantation time of no more than 2 years (MAGEC and Precice systems CE Marks FAQs_7December2021_Final (nuvasive.com)).
The predominance of a motorized implants in the treatment of EOS has clearly underlined the claim for non-invasive surgical growth management. Hopefully, further optimisation of existing, or development of new motorized implants can address this need and broaden the options for the treating physicians.
Guided growth
The high costs and the associated limited global availability of motorized implants, as well as the high complication and reoperation rates of all classic distraction-based techniques, have again paved the way for « guided growth » implants. Traditional systems, such as the Shilla technique or Luque Trolley, have not been able to sustainably be established. In addition to the lack of growth stimulation and the presumably lower correction rate, reports of premature autofusion with the Luque trolley or a significant risk of crankshaft phenomenon with the Shilla system have led to a hesitant use of these techniques.52,53 New techniques are currently being validated. Like growing rods, these systems are based on a bipolar spine-based anchorage proximal and distal to the deformity. While the Spring Distraction System (SDS) shall be validated for all EOS aetiologies, the One-Way Self-Expanding Rod (OWSER) system is now mainly recommended for the treatment of neuromuscular EOS (Figure 5).54,55 The available short-term results are encouraging but must stand the test of time.56,57
One-Way Self-Expanding Rod (OWSER) technique as a growth guiding concept in neuromuscular Early Onset Scoliosis (EOS): (a) Preoperative anteroposterior (ap) an lateral x-ray of a 9-year-old female patient with progressive neuromuscular EOS. (b) Postoperative ap and lateral x-ray after instrumentation with the OWSER system.
With the persistent challenges of surgical growth guidance associated with current techniques, discussion has recently been raised regarding the optimal treatment of an older, biologically more advanced population of patients with EOS, the so-called “tweeners,” in whom in addition to growth-friendly approaches primary final fusion may be considered. Based on a three-round survey, consensus (≥70% agreement) was reached among experts in regard of chronological age (8–10 years in girls; 9–11 years in boys), as well as inclusion of Sanders stage (<4). Patients with Sanders stage ≥4, closed triradiate cartilage, and postmenarchal should no longer be included in the tweener group and should preferably undergo corrective spondylodesis (Figure 6). 34
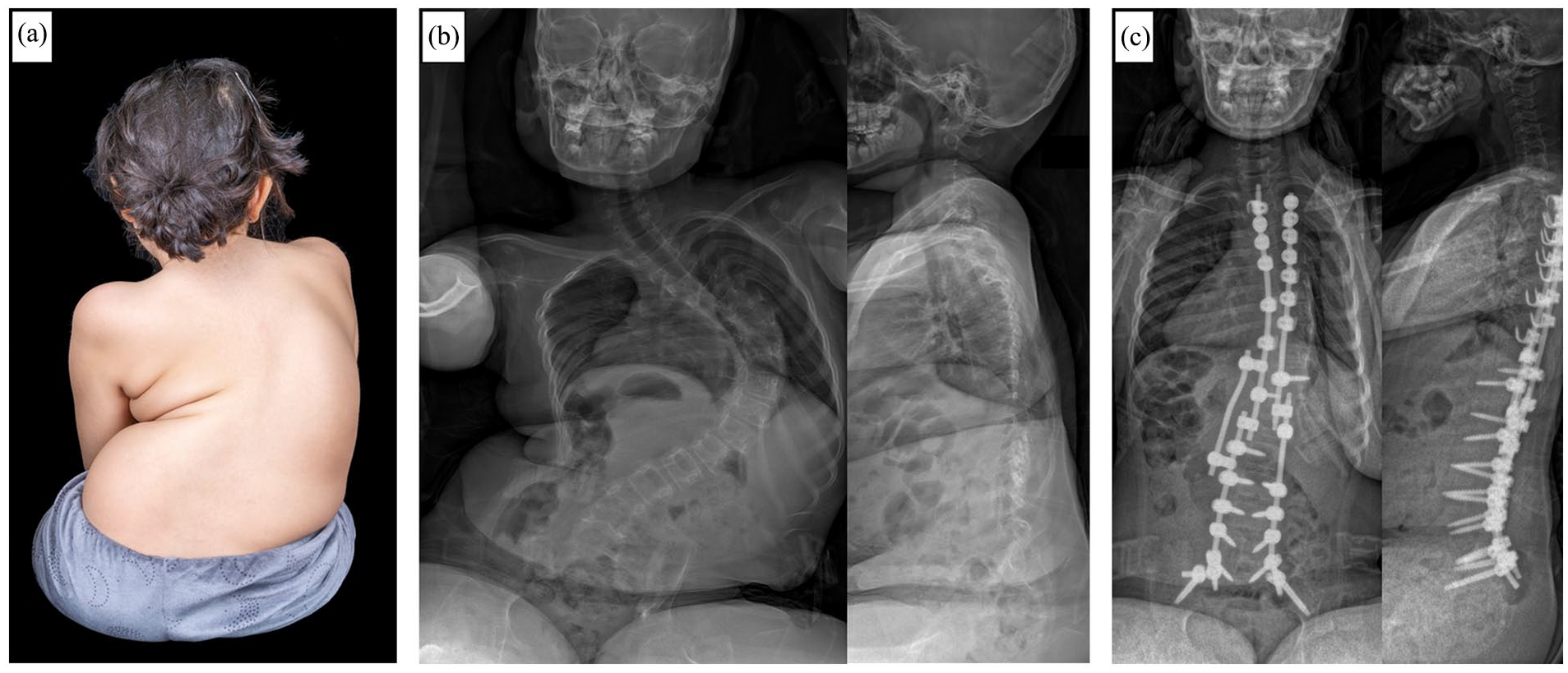
(a) Clinical photograph of a 9-year-old non-ambulant female patient with cerebral palsy with rapidly progressive neuromuscular early onset scoliosis. Posteroanterior and lateral radiographs preoperative (b) and after posterior instrumented spinal fusion surgery without previous growth-friendly surgery (c).
Similar criteria are found in the anterior convex growth-guiding system approaches that have been highly controversial in recent years. Modern anterior vertebral body tethering techniques are primarily dedicated to be used in skeletally immature patients with adolescent idiopathic scoliosis. 58 Recently, however, there has been an expansion of the range of indications in non-idiopathic and even EOS, particularly in the previously defined tweener category.59,60 The limited available results with short follow-up periods do not yet allow an adequate assessment, and the patients treated with this technique did not really comply with the EOS definition in terms of age.
The extensive enthusiasm for growth-friendly surgery leads to certain approaches receiving little or no attention in many publications. Congenital EOS, for example, can often be sustainably treated by a single surgical procedure at an early age to prevent long-term and stressful treatments, as well as functional restrictions and growth deficit. This is especially true for congenital EOS in which no additional rib fusions are present or in which only single or few segments of the spine are affected. Surgical options range from convex-side growth inhibition using pedicle screw epiphyseodesis, to partial or total (hemi-)vertebra resection (Figure 7). 61
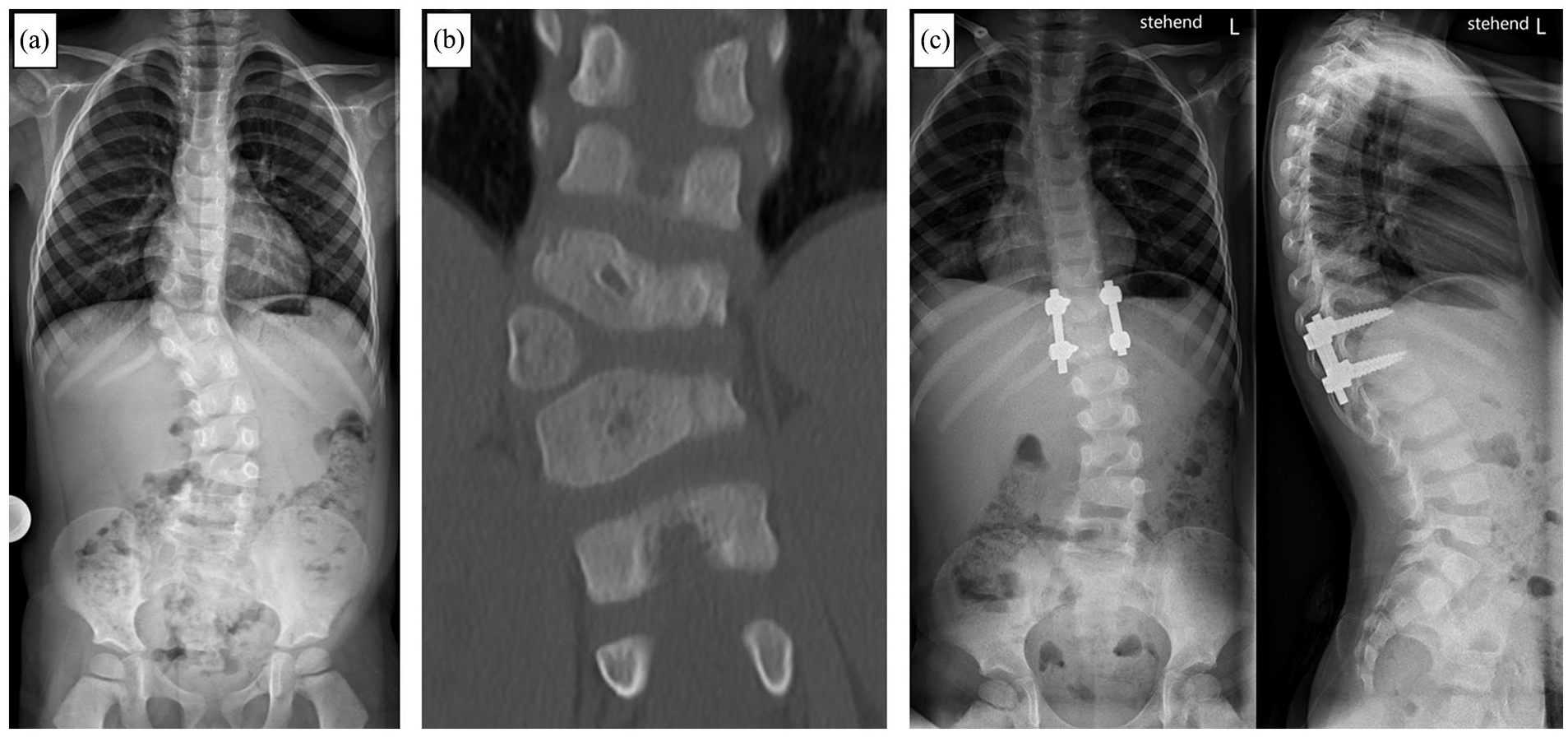
A 4-year-old male patient with congenital early onset scoliosis (EOS). Anteroposterior (ap) x-ray (a) and computed tomography (b) showing a fully segmented accessory hemi-vertebra T11/T12. (c) ap and lateral xray after hemi-vertebra resection an instrumented monosegmental spinal fusion of the adjacent segments.
Current challenges and future perspectives
Recent years have taught us that there is no cookbook approach in the treatment of EOS. A multidisciplinary team represents the basis for an optimized individual strategy, in which the principles of indication of the available growth-friendly options, as well as recent pharmacological and medical advances must be considered. With the fading enthusiasm for motorized implants as a comprehensive problem solver, a more differentiated approach will be necessary again in the future. Fundamental problems, such as progressive stiffening of the spine, diminished gains in length, and a kyphosing effect remain unavoidable with rod-based systems.37,51,62 –64 In addition, there are implant-specific problems, such as metallosis in MCGR, whose long-term consequences we do not yet know. 65 The different growth-friendly strategies can be used selectively based on the EOS etiology, for example modern growth guiding techniques such as the one-way self-expanding rod system (OWSER) in neuromuscular EOS, or they can be predetermined by anatomical features, for example as hybrid constructs (Figure 8). In addition, there is a distinct trend back to a time-buying non-operative initial treatment approach, opposed to early definitive fusion in older EOS patients. 16
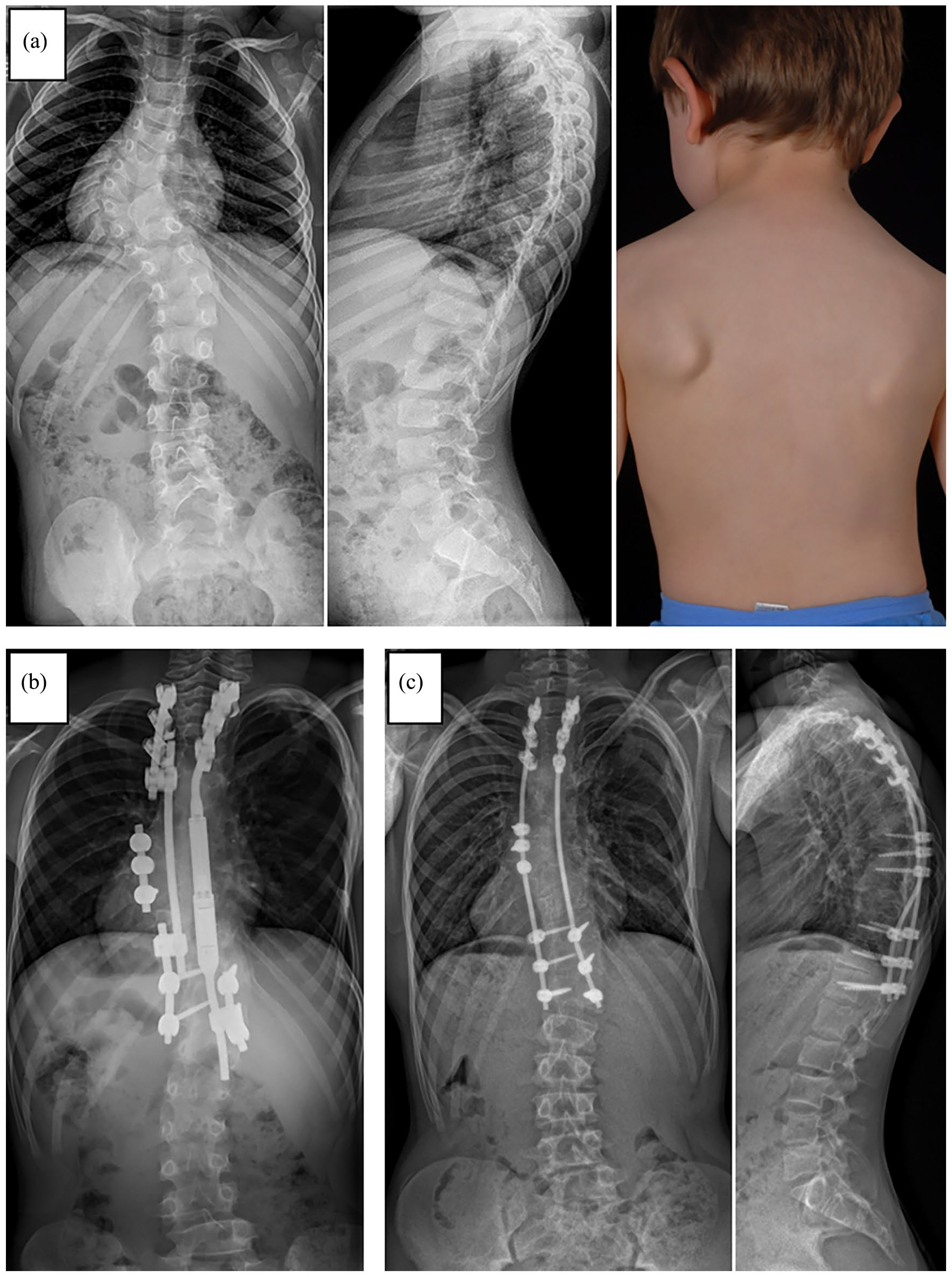
(a) X-ray and clinical photograph of a 6-year-old male patient with congenital early onset scoliosis (EOS). (b) X-ray after growth-friendly surgery with a hybrid construct including a magnetically controlled growing rod (MAGEC®) on the concave side in combination with apical fusion and a passively sliding construct on the convex side. (c) Posteroanterior and lateral x-ray after conversion to final instrumented spinal fusion. Due to spontaneous bony fusion between the proximal and distal foundation no additional anchors were used (apart from the initial convex-sided apical fusion screws).
The heterogeneity of patients included under the umbrella of EOS and the overall low incidence mandate a systematic approach with multicenter research projects and a global exchange among experts. In addition, healthcare and industry partners must prioritize their ethical obligations to fund research and empower the development of improved treatment options.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241228141 – Supplemental material for Diagnostic and therapeutic strategies in early onset scoliosis: A current concept review
Supplemental material, sj-pdf-1-cho-10.1177_18632521241228141 for Diagnostic and therapeutic strategies in early onset scoliosis: A current concept review by Daniel Studer and Carol Claudius Hasler in Journal of Children’s Orthopaedics
Footnotes
Author contributions
D.S.: Conceptualization and drafting of the manuscript.
C.C.H.: Critical revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Approval not needed because of the article type. This article does not contain any studies with human or animal participants. Written informed consent was obtained from the individuals for the publication of any potentially identifiable images in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.