
Abstract
Background:
To investigate the clinical characteristics and surgical efficacy of localized tenosynovial giant cell tumors in children.
Methods:
The clinical data, surgery, and follow-up results of 17 children with localized tenosynovial giant cell tumors who visited our hospital from 2011 to 2021 were collected for statistical analysis.
Results:
The median patient age was 7 years and 8 months, and the ratio of males to females was 1.43 (10/7). The predilection of disease was similar in hands and feet, and the common presenting symptom was mass. One patient experienced recurrence after surgery, and one child had postoperative functional limitations.
Conclusion:
Extremities are common sites of localized tenosynovial giant cell tumors in children. Complete surgical resection helps reduce the recurrence rate.
Level of evidence:
Level III
Introduction
Tenosynovial giant cell tumor (TGCT) is a type of fibrous tissue tumor that originates from synovium or tendon sheath tissue. Currently, it is classified as localized, diffuse, or malignant, with localized cases being the most common. 1 While there are many studies reporting research findings on localized tenosynovial giant cell tumors (L-TGCTs) in adults, research on L-TGCTs in children is limited due to their relatively rare occurrence, presenting challenges for diagnosis and treatment. Therefore, we retrospectively analyzed the clinical data, surgery, and follow-up results of 17 children treated for L-TGCTs at our hospital over the past 10 years to investigate the clinical characteristics and treatment outcomes of L-TGCTs in children.
Patients and methods
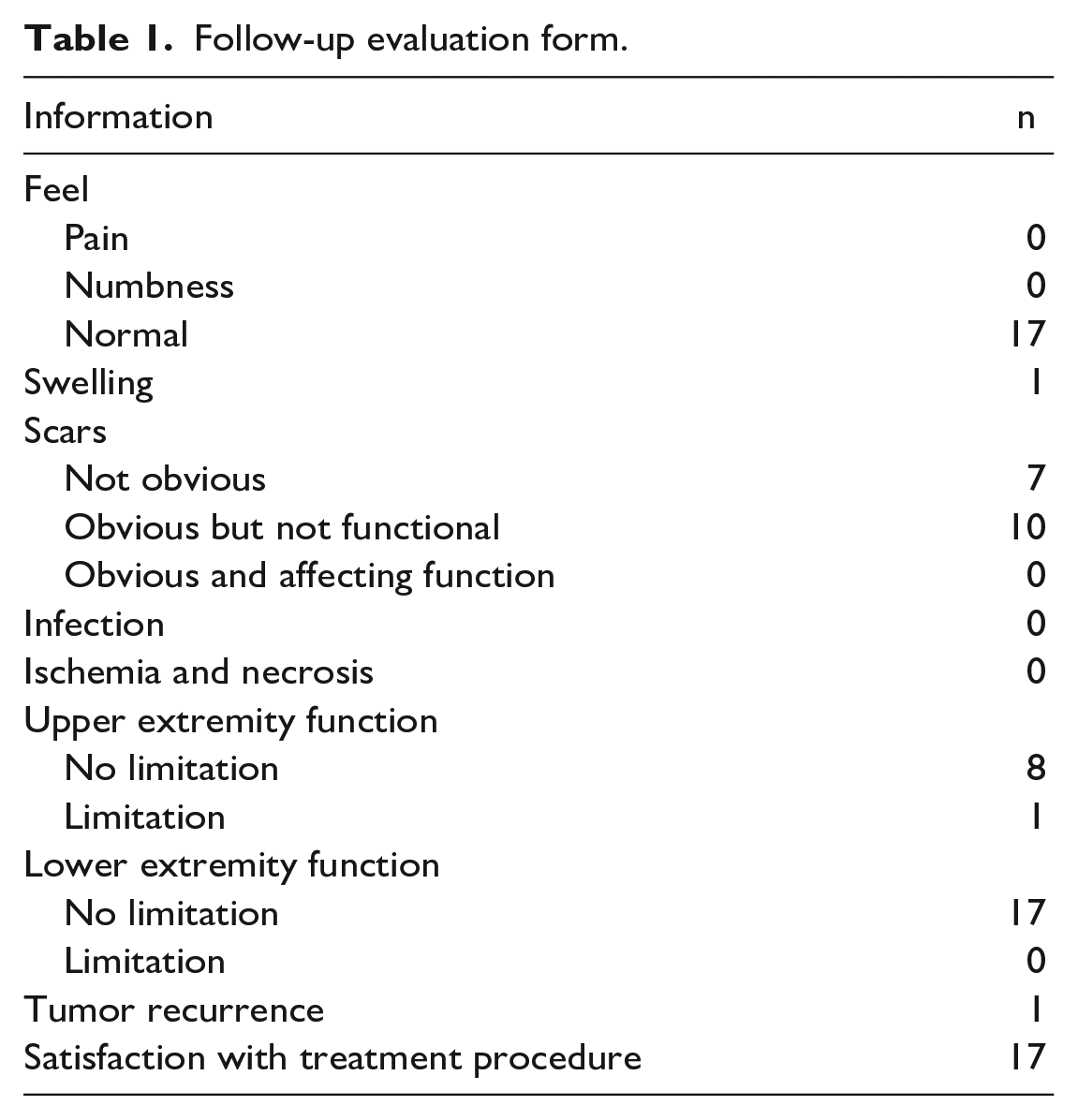
Data from children with L-TGCT who were hospitalized in our hospital from August 2011 to August 2021 were collected. The inclusion criteria were as follows: (1) under 18 years old; (2) complete clinical data, surgery, and postoperative follow-up; (3) pathological diagnosis was L-TGCT; and (4) no other malignant tumors. We collected the patients’ age, sex, symptoms at presentation, duration, location, local physical examination findings, ultrasonic and radiological features, details of surgery, pathological findings, postoperative complications, and functional recovery. The patients were followed up by telephone or outpatient review; follow-up evaluation included whether there was tumor recurrence, changes in function, and parents’ satisfaction with the treatment (Table 1). The last follow-up was on 31 December 2022.
Follow-up evaluation form.
Results
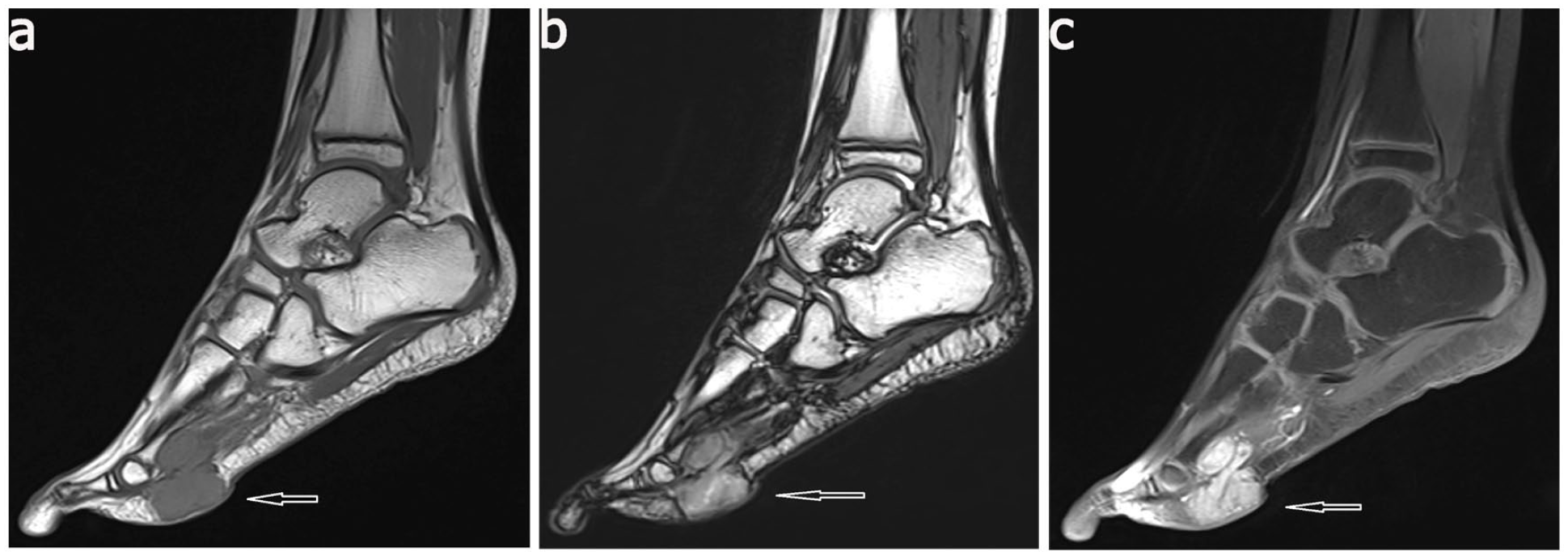
There were 17 patients in this group, 10 boys and 7 girls. The median patient age was 7 years and 8 months (range, 3 years and 9 months to 11 years). The median duration of the disease was approximately 9 months (range, 2 weeks to 2 years). One child had a history of trauma 2 years ago. One child had a previous history of seizures, and the remaining patients were in good health. One child underwent tumor resection at another hospital 2 years ago and experienced recurrence shortly after surgery. All patients presented with masses, 11 of lesions had gradual enlargement (Figure 1(a)). Physical examination showed that two children had two masses, one child had three masses, and all the other children had only one mass. The mass was slightly hard or tough in texture, and most of them were not tender (four cases, mildly tender), and there were two cases of functional limitation (one case had mild limitation on the extension of the second toe of the right foot, and one case had limitation on the flexion and extension of the great toe of the right foot). The tumors were in the hands and feet of eight children each and in the thigh in one child (Table 2).
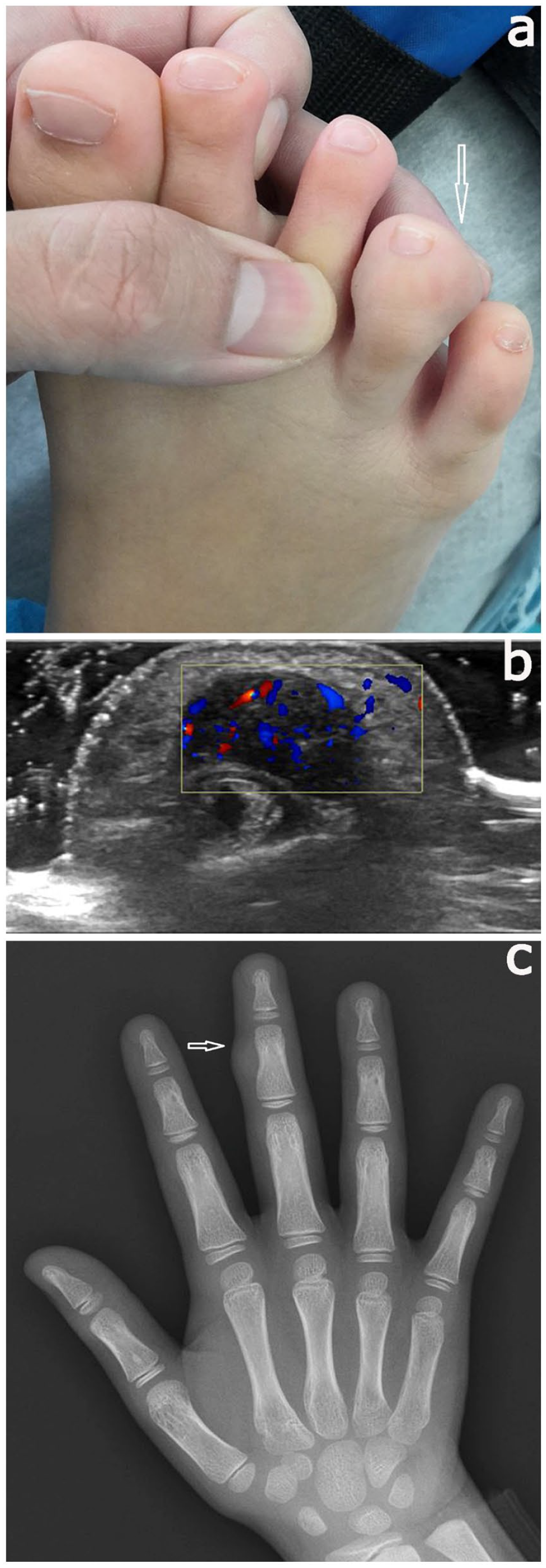
(a) Local appearance photograph of patient number 12, (b) ultrasonography of patient number 9, and (c) plain radiography of patient number 3.
The characteristics of patients with L-TGCT.
L-TGCTs: localized tenosynovial giant cell tumors.
2 weeks.
20 days.
Second surgery.
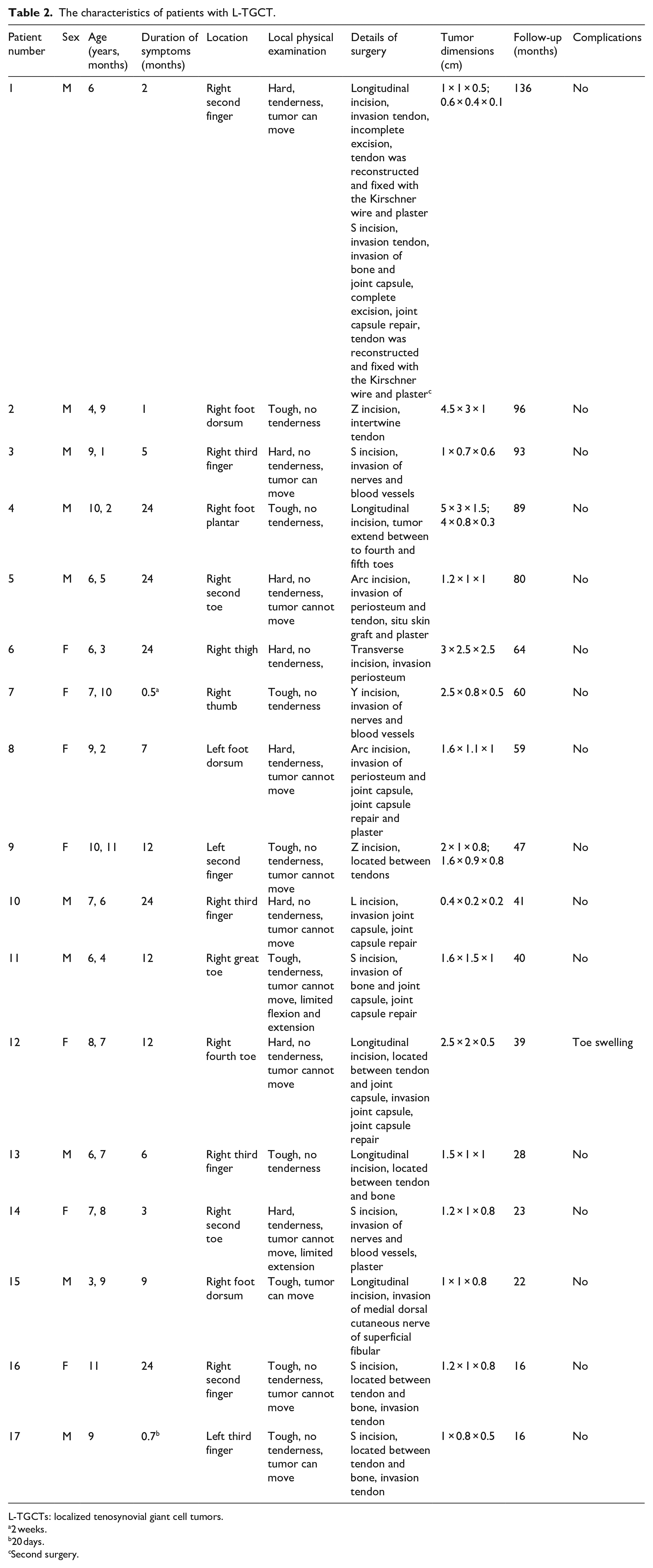
All patients underwent ultrasonography, which mainly showed hypoechoic masses; 4 cases showed cystic masses, inhomogeneous internal echoes in 15 cases, and blood flow signals in 11 cases (Figure 1(b)). Ultrasonography showed that the tumors were adjacent to or intertwined with important structures in seven patients (tumors of five patients intertwined with tendons (one of which intertwined with a blood vessel), one patient’s tumor was adjacent to the blood vessel, and one patient’s tumor was intertwined with more than three-quarters of the phalanx). All ultrasonography showed no liquid area or echo of calcification in the mass. Preoperative plain radiography was performed in 10 patients, and the most common showed soft tissue swelling or mass shadow (Figure 1(c)). Five children showed cortical compression or irregular bone morphology (one of them had destructive changes in bone), and two cases showed no abnormality and no bone structure was destroyed. Only three patients (2 feet, one thigh) underwent magnetic resonance imaging (MRI) before surgery. MRI showed equal signal on T1-weighted images and slightly longer signal on T2-weighted images, and the lesion was significantly enhanced after enhancement with well-defined borders and no significant abnormalities signal in adjacent bone (Figure 2).
Magnetic resonance imaging of right plantar mass in patient number 4: (a) T1-weighted images, (b) T2-weighted images, and (c) T1-weighted enhanced images.
No patients received other treatments (chemotherapy or radiation) postoperatively. The median operation times were 1 h and 15 min, and a tourniquet was used in 16 children during the operation. Intraoperative exploration showed that the tumor was solid yellow or dark brown, with a complete capsule in seven patients; tendon tissue was involved in four patients, blood vessels or nerves were involved in four patients, a joint capsule was involved in four patients, the periosteum was involved in three patients, and bone tissue (intact bone cortex, bone tissue compression, and deformation) was involved in one patient (Figure 3(a)). Tumors were completely resected in 16 children. In one child, the tumor was not completely removed during the first operation to prevent ischemic necrosis of the finger due to the tumor involving more than three-quarters of the finger diameter. One patient underwent tendon reconstruction, and four patients underwent partial periosteal resection. There were four cases of joint capsule repair, one case of internal fixation with the Kirschner wire, one case of in situ skin grafting, and four cases of plaster use.
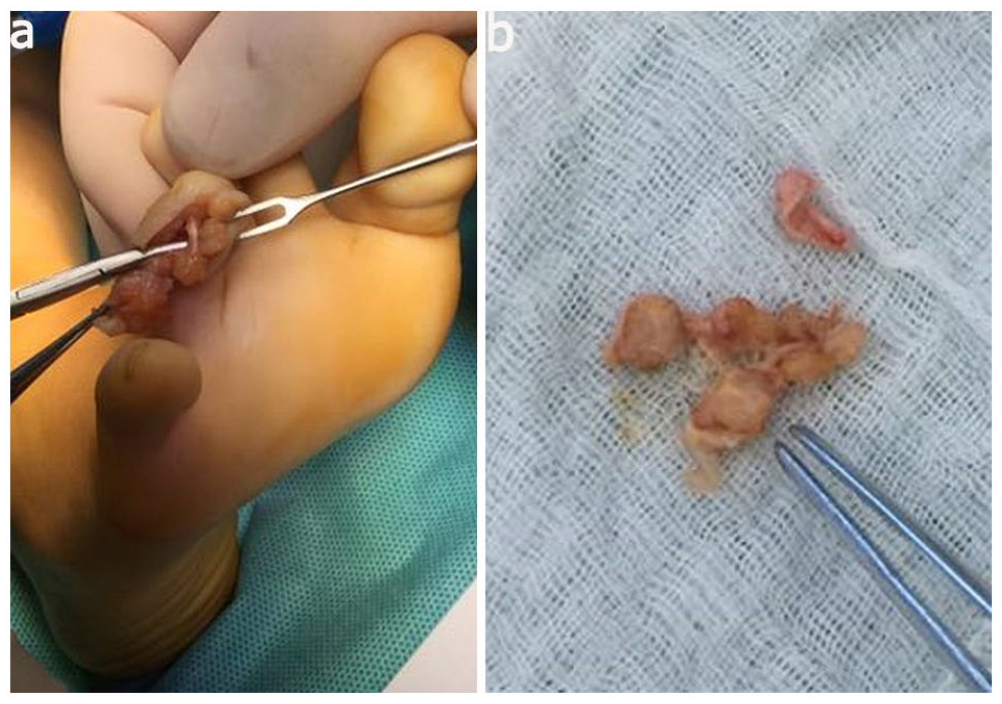
(a) Intraoperative picture of right fourth toe tumor in patient number 12 and (b) gross appearance in patient number 12.
The median follow-up time for all patients was 47 months (range, 16 months to 136 months), and the patients without serious postoperative complications (such as ischemia and necrosis and infection) and swelling in the affected toe were treated with drugs in one patient who recovered well. One patient had recurrence approximately 3 years after surgery and underwent reoperation with no recurrence to date (see Table 2 for the second surgical procedure). One child had postoperative functional limitation (slightly limited flexion of the distal interphalangeal joint of the second finger of the right hand). The parents of 10 patients considered the surgical scars to be obvious but to have no effect on function.
Discussion
The study found that L-TGCTs in children tend to occur in the extremities and require a pathological diagnosis. Complete resection is an effective way to reduce recurrence. TGCTs are mesenchymal tumors that originate from synovium, tendon sheath, or bursa and can be categorized into localized, diffuse, and malignant types based on location, growth pattern, and biological behavior. The disease has had various names in the past, such as fibrous xanthoma and pigmented villonodular synovitis, 2 but is now known as TGCT according to the World Health Organization classification of bone and soft tissue tumors in the 2020 edition. The most common type is localized and tends to occur in adults aged 30–50 years with a female predominance. 3 However, there are relatively few articles about L-TGCTs in children.4,5 The age range in this study was 3 years and 9 months to 11 years old, with a median age of 7 years and 8 months. More boys than girls were affected, and L-TGCTs were found to be equally likely to occur in the hands and feet of children, which differs from adult cases where they are more common in the fingers. 3 This finding is similar to Gholve et al.’s 5 study.
At present, the specific etiology of the disease is unclear and may be related to trauma, metabolic abnormalities, or related factors.6,7 In this study, one child had a history of trauma, but whether there is an association warrants further study. Previous studies have found that TGCT is a type of tumor associated with the overexpression of colony-stimulating factor-1 (CSF-1); 8 it is most commonly caused by the t(1;2) translocation, which fuses the CSF-1 gene on chromosome 1 with the type VI collagen promoter gene on chromosome 2 (resulting in the VI collagen α3-CSF-1 fusion gene). 9 Several novel fusion genes involving CSF-1 have recently been identified, 10 and these studies provide potential ideas for treatment of the disease. The overexpression of CSF-1 can promote proliferation and accumulation of cells in the synovial membrane and even affect bone tissue. 2 Pexidartinib can selectively inhibit the internal tandem repeats of CSF-1, c-KIT proto-oncogene receptor tyrosine kinase, and Fms-like tyrosine kinase-3 genes, thereby suppressing proliferation of tumor cells. 11 Currently, the US Food and Drug Administration has approved pexidartinib for patients with TGCTs who have severe functional limitations and who likely would not achieve improvement with surgery; 12 related research in children is being conducted a phase II clinical study (NCT04703322). However, other drugs are also being assessed in a phase III clinical study, such as the efficacy study of emactuzumab for localized or diffuse TGCT that cannot be surgically removed (NCT05417789). The most common reason for children to present to the clinic was the discovery of a mass, with a relatively long disease duration that slowly increases with age and rarely affects function. Ultrasound is the preferred evaluation tool, which can assess the relationship between the mass and surrounding tendons and vessels. In this study, ultrasonography showed that the tumor was consistent with intraoperative exploration results of adjacent or surrounding soft tissue. Typical ultrasonography showed a hypoechoic mass with ill-defined borders, an irregular shape, nonuniform internal echoes, and punctate blood flow signals within the mass.13,14 However, sometimes ultrasonography may be misjudged as other lesions. For instance, ganglion cysts have a positive light transmission test, clear boundary, and no obvious blood flow signal in the mass. 15 Haemangiomas are located superficially and may have skin color changes and abundant blood flow signals in the mass. 16
In addition to ultrasonography, radiographs are sometimes performed. Radiographs mainly evaluate whether the tumor originates from bone tissue, whether the tumor invades the bone tissue, and to distinguish it from other diseases. For example, the extremity masses found in children need to be differentiated from osteochondroma. Radiographs of osteochondroma showed a bony protrusion, continuous bone cortex and diaphysis, and a bone marrow cavity communicating with the bone marrow cavity, with no periosteal reaction. 17 MRI has a high value in differentiating the location, size, shape, signal characteristics, and relationship with soft tissue and has important application value in the localization, characterization, and staging of soft tissue tumors. 18 However, the application of MRI is limited by factors such as costs and durations and sometimes requires sedation or anesthesia. Therefore, only three children in this study underwent MRI, but the results were similar to those of Wang et al. 19 Nevertheless, T2-weighted image signals may differ due to the different contents of hemosiderin and collagen fibers in the lesions. The patients who underwent MRI also had a differentiating diffuse tenosynovial giant cell tumor (D-TGCT), and whether the surrounding bone tissue was involved assessed, which is helpful for the surgical plan. For example, typical manifestations of D-TGCT by gradient-echo sequence MRI are irregular synovial thickening (>5 mm), which is generally described as “frond-like” with villous or nodular morphology, joint effusion, and extra-articular invasion, among others. 20
L-TGCTs in children are solid, tough, and nodular or lobular with a yellowish-brown gross appearance (Figure 3(b)). Microscopy shows multinucleated giant cells, monocytes, and collagen fibers (Figure 4), and immunohistochemical staining detects the expression of different antibodies, such as CD68, CD163, and CD45.21,22 In this study, CD68 positivity was the most common finding. L-TGCTs should be pathologically differentiated from D-TGCTs, malignant tenosynovial giant cell tumors (M-TGCTs), and tenosynovial fibromas. D-TGCTs are relatively large (>5 cm) and have a villous pattern if occurring in the joint but a multinodular pattern if occurring outside the joint. Osteoclast-like giant cells are uncommon, and slit-like spaces are more common. M-TGCTs are rare and exhibit atypical mitosis, necrosis, abnormal nuclei, and myxoid changes. 1 Tenosynovial fibroma is similar to L-TGCT in its predilection location and histological morphology, but it occurs more commonly in young people, with fibrous nodules and spindle cells with scattered fissure-like vascular lacunae seen on microscopic examination. 23
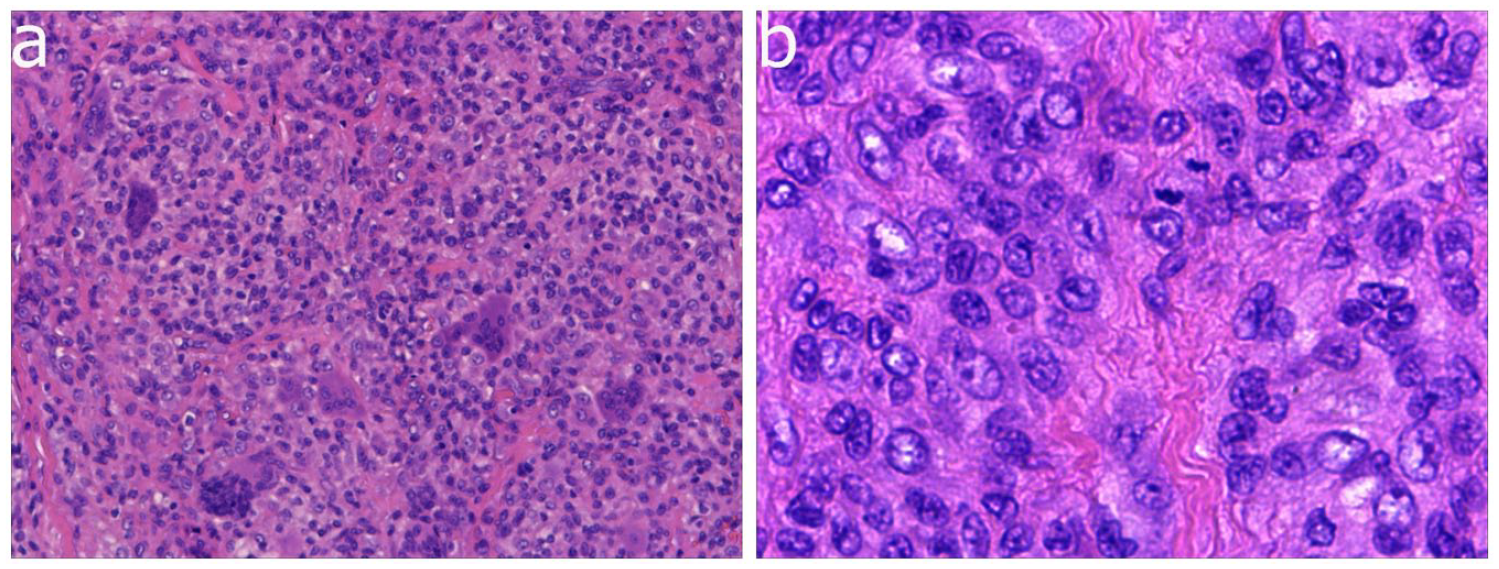
(a) Microscopic pictures of the tumor in patient number 17 (200×) and (b) microscopic pictures of the tumor in patient number 17 (400×).
Currently, surgical resection remains the primary treatment for L-TGCT in children. However, there is a certain probability of recurrence, and complete resection of the tumor is essential to reduce postoperative recurrence.24,25 Some tumors may be located between tendons or invade tendons and vessels, making complete surgical resection challenging. Staged surgical resection can be attempted to reduce postoperative complications. Magnification loupes can be utilized during the operation to improve complete surgical resection of tumors hidden in some tendons, especially since children’s extremities are relatively small compared to adults.5,24 Controversies remain about the treatment for tumors involving bone tissue.26 –28 Scholars believe that bone involvement may not require specific treatment as it could be due to changes caused by compression of the tumor. 26 However, some reports recommend treatments such as simple curettage and curettage plus bone grafting for damaged bone tissue resulting from tumor erosion. 28 In this study, only partial periosteal resection was performed for patients whose tumor involved the bone tissue but no bone destruction. Satellite lesions are a factor affecting postoperative recurrence, 29 and our center has attempted to use iodine tincture and other methods to reduce satellite lesions to reduce recurrence. However, further study is needed as damage to the soft tissues may occur with these methods.
The study was a single-center retrospective case study with a low level of evidence, a single treatment plan, and a lack of comparative studies of children treated non-operatively, which is a direction for future research. In addition, for the tumor involved bone tissue, the treatment plan needs to be further clarified by higher level of research.
Conclusion
L-TGCTs in children are still more common in the extremities. Lesions commonly present as a slowly enlarging mass. Ultrasonography, radiography, or MRI is good options for diagnosing, differentiating other diseases, and planning surgical plans. Intraoperative complete tumor resection through careful manipulation is the most effective treatment to reduce recurrence.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231186795 – Supplemental material for Localized tenosynovial giant cell tumor in children
Supplemental material, sj-pdf-1-cho-10.1177_18632521231186795 for Localized tenosynovial giant cell tumor in children by Xifeng Du, Anning Xia, Junying Sun and Yinting Ye in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
This study is very grateful to Jingming Han and Xianping Jiang and for their help in the collection of data.
Author contributions
A.X. is responsible for designing and revising papers. X.D. is mainly responsible for collecting data, statistical analysis, and writing papers. J.S. help collect data and statistical data. Y.Y. is mainly responsible for data verification and statistical results.
Consent for publication
All authors agreed to publication of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
The study was approved by the Ethics Committee of Shezhen Children’s Hospital. This study has been agreed by the all patients of parents. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Guangdong High-level Hospital Construction Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.