
Abstract
Purpose:
To evaluate the residual acetabular dysplasia in Graf type II hips after Pavlik harness treatment with a radiographic follow-up at 2 years of age.
Methods:
We retrospectively reviewed the developmental dysplasia of the hip patients who were treated with the Pavlik harness between March 2018 and February 2022. Patients with Graf type II hip dysplasia who had at least one radiographic follow-up after 2 years of age were included. The following information, sex, laterality, affected side, age at harness initiation, treatment duration, α angle, and the morphology of bony roof, was collected and studied. We evaluated the radiographic acetabular index at the last follow-up and defined the value of greater than 2 standard deviations as residual acetabular dysplasia.
Results:
A total of 33 patients (53 hips) met the criteria. The mean initial α angle was 53.4°; the mean age at Pavlik harness initiation was 10.9 weeks. The mean treatment duration was 10 weeks. The mean α angle at the last ultrasound follow-up was 64.9°. The mean age of the last radiographic follow-up was 2.6 years, and 26 hips had a residual acetabular dysplasia with acetabular indexes greater than 2 standard deviations above the mean. The morphology of the acetabular bony rim (odds ratio = 4.333, P = 0.029) and age of initial treatment <12 weeks (odds ratio = 7.113, P = 0.014) were seen as significant predictors for a higher acetabular index more than 2 years of age.
Conclusions:
A notable incidence of residual acetabular dysplasia after Pavlik harness treatment in Graf type II hips, wherein the acetabular bony roof with a blunt rim at the end of treatment and initial age after 12 weeks were independent predictors associated with residual acetabular dysplasia.
Levels of evidence:
Therapeutic studies, IV.
Introduction
Developmental dysplasia of the hip (DDH) is one of the most common congenital musculoskeletal disorders in children. It encompasses a spectrum of pathologic hip disorders from mild acetabular insufficiency to frank dislocation. Earlier detection and treatment of DDH are more effective because the anatomical structural abnormalities secondary to the dislocated femoral head can be reversed after reduction. Treatment before 7 weeks is preferable than later.1,2 Ultrasound (US) monitoring Pavlik harness (PH) treatment for DDH is the first choice for patients aged <6 months, and the success rate was reported to be between 58% and 100%.2 –4 However, parents may not be assured of normal development of the hip joint after achieving ultrasonographic normalization at the end of the treatment, because radiographic residual dysplasia was reported in the clinical follow-up.2,5 –12 In a recent literature meta-analysis of 17 studies, radiographic evidence of residual acetabular dysplasia (RAD) following successful treatment was found in 9.49% hips; 4.14% of these cases required additional surgery. 13 The severity of the dislocation, age at initiation, and sides of involvement may be related to the residual dysplasia.
In Graf type II hips, which are defined as a centered joint with a deficient bony acetabular roof, the optimal treatment strategy and the outcome after PH treatment are less discussed. 14 In this study, we retrospectively studied our patients with Graf type II dysplasia hips. We tried to answer the following questions: (1) What are the potential risk factors of RAD after treatment of the PH in Graf type II hips? (2) Does sonographic mild stable hip dysplasia have a lower rate of RAD?
Patients and methods
After institutional review board approval was obtained, we retrospectively reviewed the medical records of patients with DDH who were treated with PH between March 2018 and February 2022. All patients were clinically evaluated by senior orthopedic physicians, and US examination was performed with a GE LOGIQ E9 machine by trained radiologists according to Graf’s method with a 7.5 MHz short-focus linear-ray transducer.
Our treatment protocol for the dysplastic hip is similar to the expert-based consensus. 15 Patients with Graf type IIa-, IIb, and IIc are routinely treated with the PH. While Graf type IIa + hips are reassessed within 2 weeks, the harness will be applied if there is no improvement. The harness is worn for 22 h/day and is allowed removal when changing the diaper or during bathing. The repeated US evaluation is scheduled 2 weeks after treatment, then every 4 weeks. The treatment would be discontinued when the α angle is greater than 60°, and the minimum duration is 6 weeks. Patients are required at least one radiographic follow-up when they can stand, commonly at 12 months of age.
The inclusion criteria were patients with Graf type II hip dysplasia who were treated with the PH in our outpatient clinic, initial treatment age under 6 months of age, the α angles greater than 60° at the end of treatment and having at least one radiographic follow-up after the age of 2 years. Patients with neurotologic or teratologic problems were excluded. Patients treated or have the pelvic radiography in other institutions were excluded as well. We studied the following demographic information: sex, bilaterality, affected side, age at harness initiation, and treatment duration. Ultrasonographic parameters included the initial α angle, the final α angle, and the morphology of the bony acetabular roof at the end of the treatment. According to the Graf method, the bony rim of the roof was classified as sharp angular or blunt. 14
The acetabular index (AI) was measured on the pelvic radiograph at the last follow-up according to Kim et al. 16 The lateral end of the acetabular sourcil was used as a measurement point, and the sourcil orientation was divided into upward and horizontal or downward. The AI was evaluated according to Tönnis criteria depending on age, sex, and side. 17 The AI value of greater than 2 standard deviations (SDs) was defined as RAD.
Statistical analysis
All statistical analyses were performed using SPSS V24.0 software. (IBM Corporation, Armonk, NY). P < 0.05 was considered to indicate statistically significant differences. The parametric Kolmogorov–Smirnov test was used to verify the normal distribution of the continuous variables. Descriptive statistics were calculated for demographic information, and continuous variables were presented as the mean ± standard deviation and ranges. RAD was chosen as a dependent variable. The independent sample t-test and Mann–Whitney U-test were performed to check for significant differences between RAD and non-RAD for continuous and categorical variables, respectively. Binary logistic regression analysis was used to identify significant independent risk factors for RAD after PH treatment. All significant variables (P < 0.05) were entered into the model. Spearman’s rho or Kendall’s tau correlation analysis was used to assess the relationship between the RAD and acetabular sourcil.
Results
Demographic and clinical characteristics of the study population
A total of 8693 infants were screened with US during the study period. A total of 98 infants (156 hips) had stable acetabular dysplasia (Graf type II). Only 33 patients (53 hips) had a radiographic pelvis after the age of 2 years, and their data were collected and analyzed. A total of 21 patients were screened for gluteal fold asymmetry in the community health center, and the rest were transferred from other hospitals for abnormal US scan results. There were significantly female patients in this study (31 (94%) female and 2 (6%) male). The mean age at PH initiation was 10.9 (5.3–20.7) weeks. A total of 20 (61%) patients had bilateral hip involvement (40 hips), and 13 (39%) patients had unilateral hip involvement (10 in the left and 3 in the right, P = 0.691, chi-square). Two infants had torticollis, and two were born in the 36th week of gestation or early. The mean initial α angle was 53.4°; the Graf grade was IIa in 31 hips, IIb in 13 hips, and IIc in 9 hips. The mean PH treatment duration was 10 (6–16) weeks. The mean α angle at the end of treatment was 64.9° (Table 1). No late hip dislocation or avascular necrosis of femoral head was observed during the follow-up. Two patients underwent Salter osteotomy at 3.5 years because of RAD.
Patient demographics and clinical characteristics.
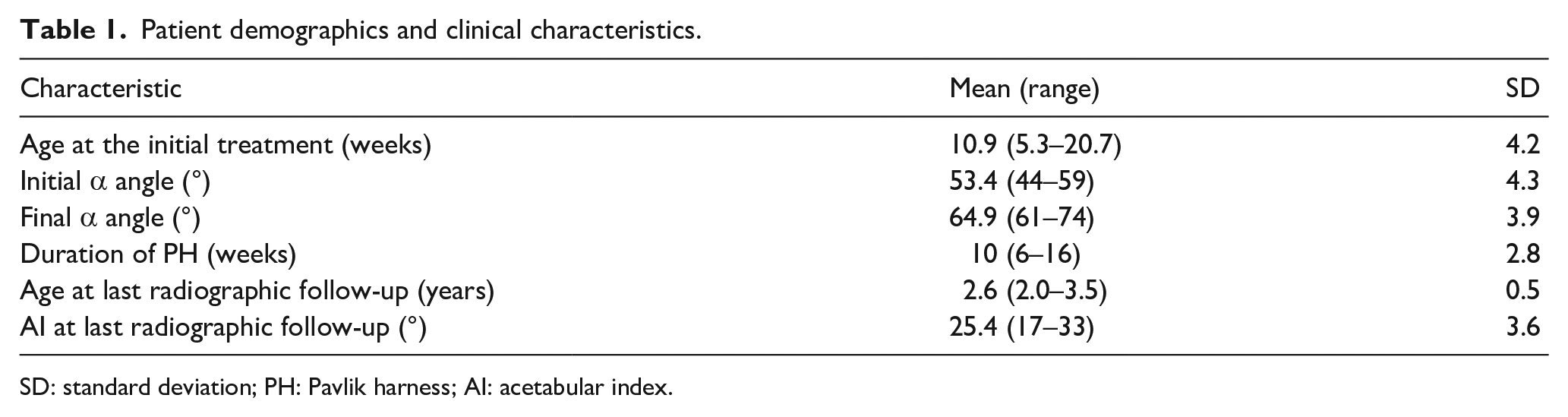
SD: standard deviation; PH: Pavlik harness; AI: acetabular index.
The mean age of the last radiographic follow-up was 2.6 years. An upward sourcil was found in 29 hips, and the mean AI was 25.4°. Twelve hips had AIs under the mean value, 15 hips had AIs >1 SD above the mean, 26 hips had a dysplastic hip with AIs >2 SDs above the mean, and there was a significant relationship between the upward sourcil and RAD (Spearman’s rho = 0.404, P = 0.003). We also found a weak relationship between the ultrasonographic morphology of the bony acetabular roof and the radiographic sourcil orientation (Spearman’s rho = 0.286, P = 0.038).
The cutoff α angle value of 55° at the initial US scan was evaluated, and we found that there was a significant negative relationship between an α angle of greater than 55° and RAD (Spearman’s rho = −0.317, P = 0.021). When comparing the mean age at the initial treatment, hips with α angle greater than 55° were 12.4 weeks, and that of hips with α angle less than 55° were 9.7 weeks (P = 0.023).
There was a significant difference between the duration of treatment and the initial treatment age of 12 weeks (P = 0.008) (Figure 1). In addition, when the initial α angle was classified into three groups (Figure 2), we found a significant relationship between the duration of treatment and the initial α angle (Spearman’s rho = −0.447, P = 0.001).
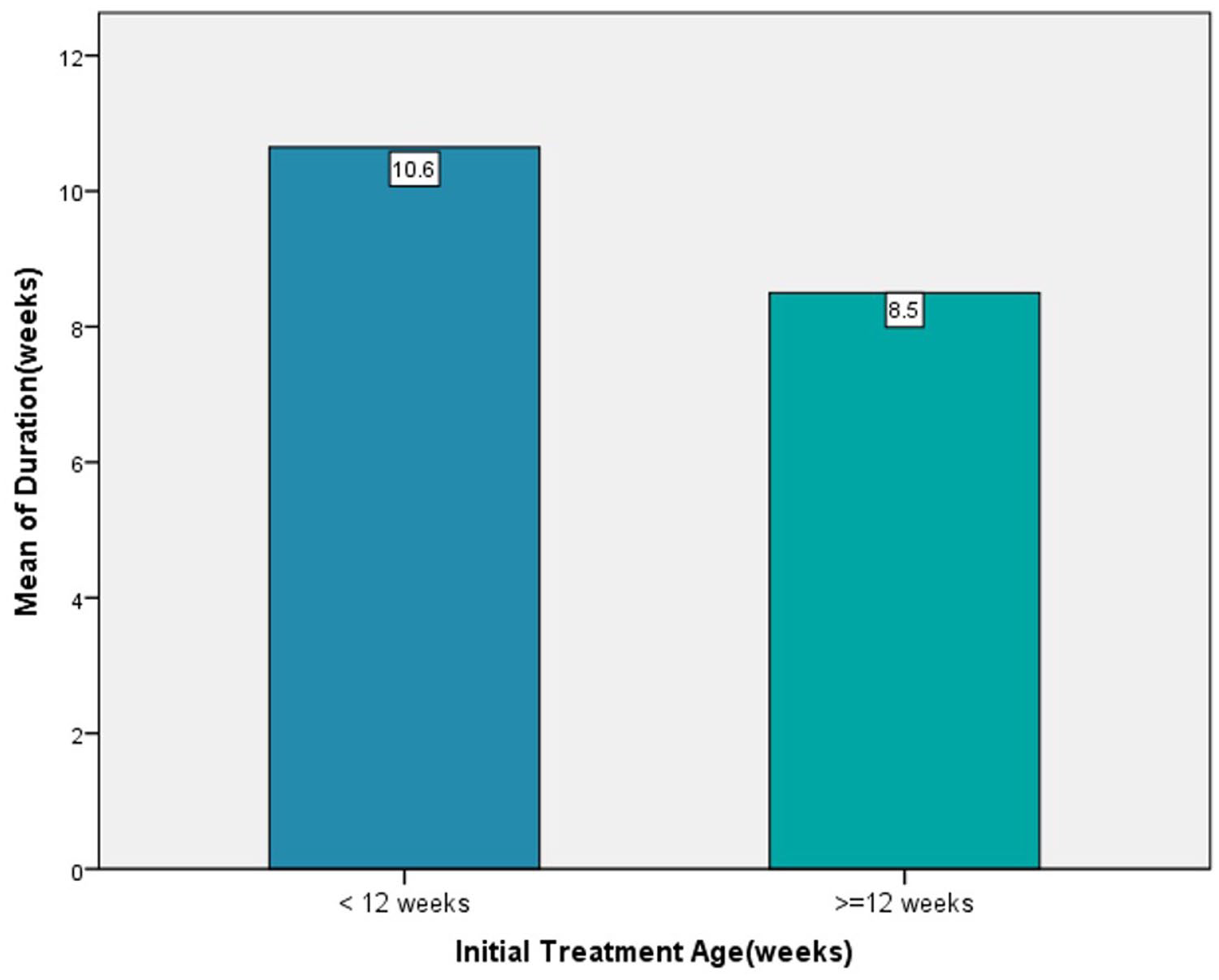
Mean duration of PH treatment was 10.6 weeks in infants <12 weeks and 8.5 weeks in infants ≥12 weeks of age. There was a significant difference between the duration of treatment and the initial treatment age of 12 weeks (P = 0.008). PH: Pavlik harness.
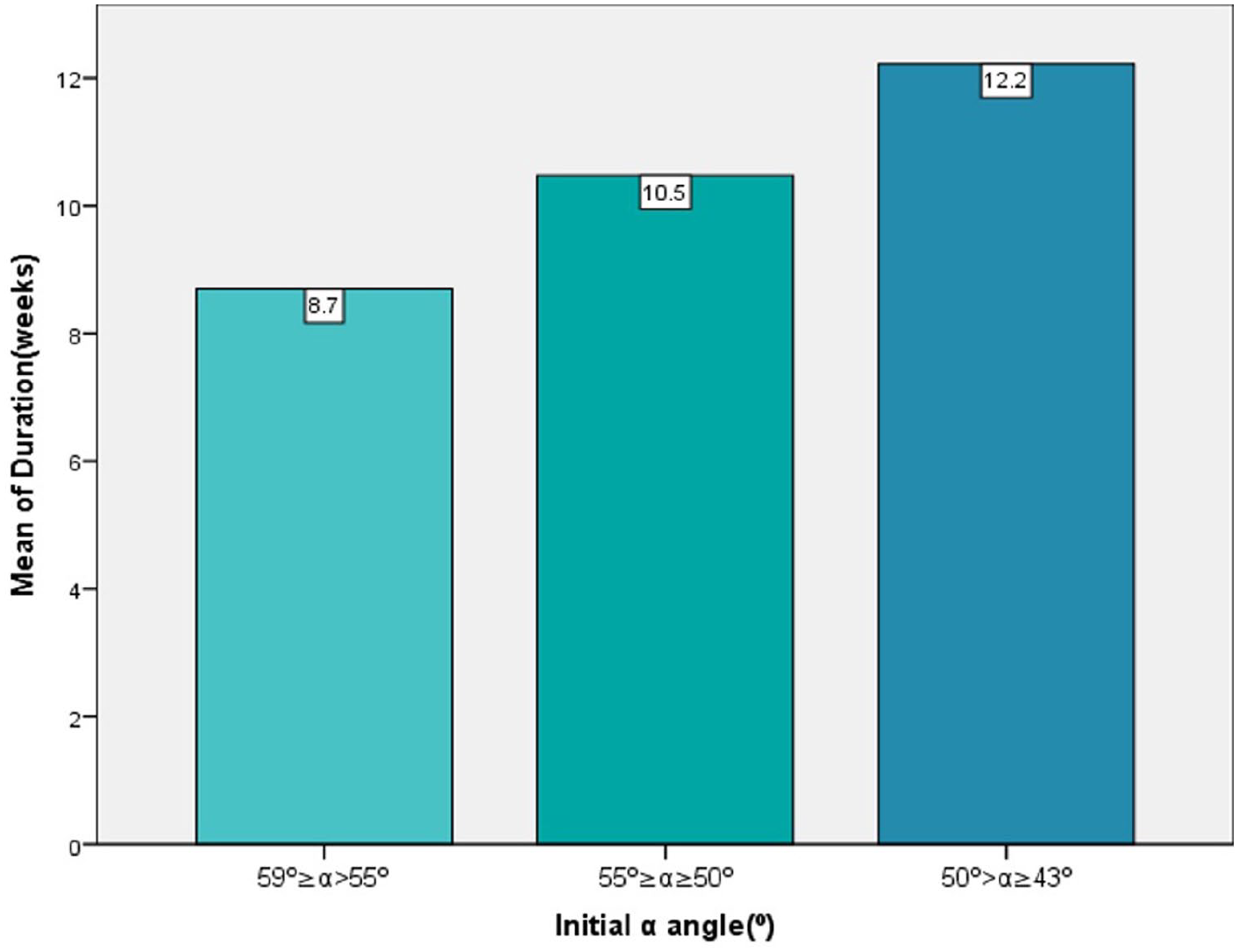
We divided initial α angle into three groups: 59° ≥ α > 55°, 55° ≥ α ≥ 50°, and 50° > α ≥ 43°. The mean treatment duration for the three groups was 8.7 weeks, 10.5 weeks, and 12.2 weeks, respectively. The initial α angle is negatively correlated with the duration of treatment (P = 0.001).
There were significant differences in age at the initial treatment mean (P = 0.005), initial α angle (P = 0.008), and the morphology of acetabular bony rim at the last US scan (P = 0.010) (Table 2). The initial treatment age of 12 weeks and α angle of 55° were further analyzed as potential risk factors (Table 3). When all these three factors were entered into the regression model as independent variables, only the morphology of the acetabular bony rim and age of initial treatment <12 weeks were seen as significant predictors for a higher AI more than 2 years of age (Table 4).
Comparison of continuous variables between groups of normal hip and residual dysplasia hip.
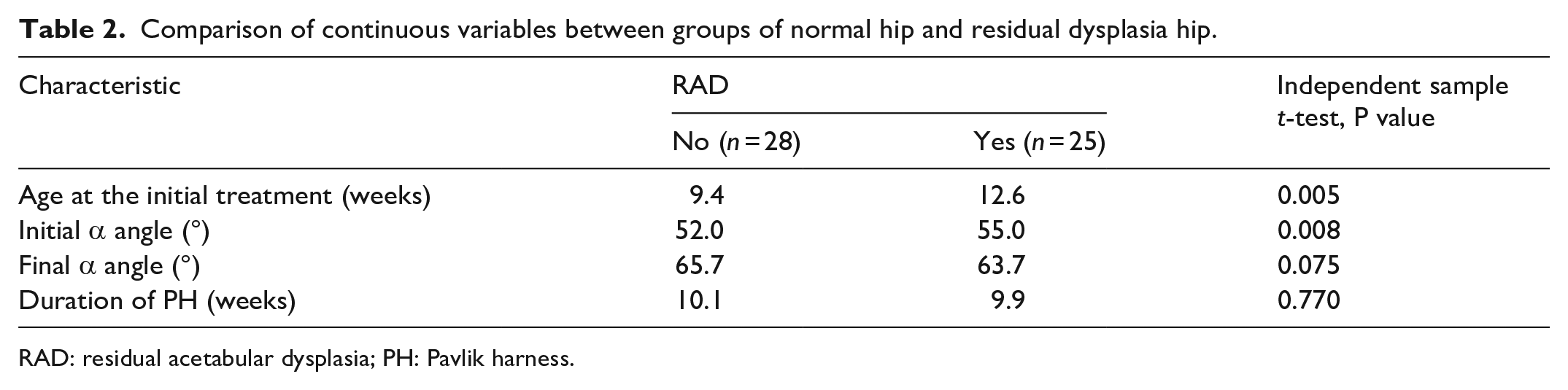
RAD: residual acetabular dysplasia; PH: Pavlik harness.
Comparison of categorical variables between groups of normal hip and residual dysplasia hip.
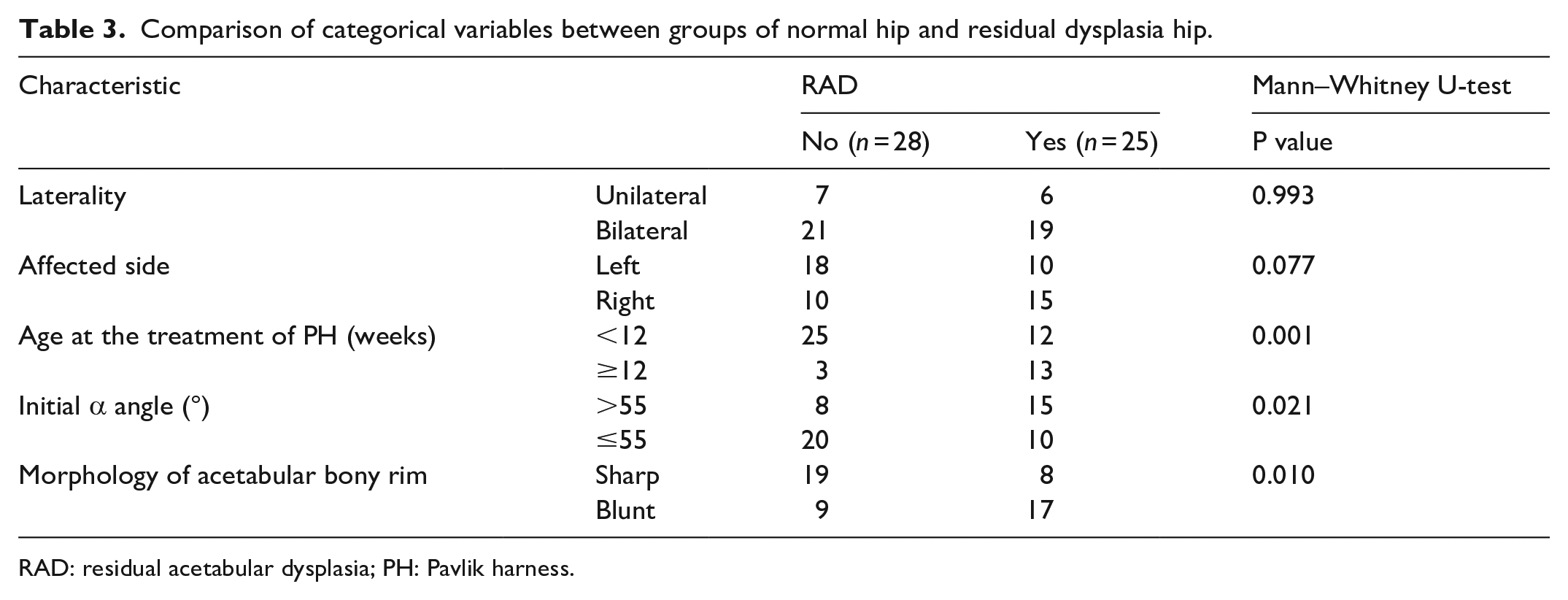
RAD: residual acetabular dysplasia; PH: Pavlik harness.
Multivariate analysis for independent risk factors associated with RAD.

CI: confidence interval; PH: Pavlik harness; OR: odds ratio.
Discussion
Residual hip dysplasia after the treatment of PH has been reported by many authors.7,12,13,18,19 Several potential risk factors were associated with residual hip dysplasia. The severity of dislocation was reported as one of the predictors in patients treated with PH. In a mid-term study of PH treatment in infants, Alexiev et al. 7 demonstrated that dynamic coverage index <22% and α angle less than 43° on the initial US predicted late dysplasia. Similar results were reported by Novais et al. 12 who identified the Graf type IV hip as a significant factor predictive of high AI at 12 months.
The above studies focused on a total spectrum of DDH from hip dysplasia to dislocation. Graf type II hips are defined as stable dysplasia hips with an α angle ranging between 43° and 59° without hip dislocation. In this study, we found that although all hips achieved an α angle greater than 60° at the end of treatment, 49% hips showed high AIs >2 SDs above the mean (according to Tönnis criteria) at the last pelvic radiographs. Initial age at treatment was a potential predictor of RAD, and initial treatment after 12 weeks of age had a higher rate of RAD (P = 0.001). The duration of the PH may be related to this phenomenon. In a retrospective study of 343 hips, Bialik et al. 20 reported that the PH treatment started before 13 weeks of age tended to have a shorter duration in type IIa, IIc, and III hips. We usually prescribe a 6-week treatment duration for mild dysplasia hip no matter how old the infant is. However, the duration of older infants (age ≥ 12 weeks) was shorter than younger infants (age < 12 weeks) in this study (Figure 1). We attributed it to older infants’ intolerance of the PH. The application of the PH is more challenging in older infants who are more active and can more easily overpower the harness. The longer treatment duration may lead to a sleeping problem or skin affection and challenge parental compliance, which would affect the treatment results. 21 However, whether prolonging the duration for patients older than 12 weeks reduces the occurrence of RAD remains unclear due to the lack of control.
There is little consensus about the duration of PH use (the timing and method of cessation). According to an expert-based consensus, the duration was variable according to the severity of DDH, usually a minimum of 6 weeks for dysplasia hip and 8 weeks for dislocatable or dislocated hip. 15 Van der Sluijus et al. 22 and Gornitzky et al. 23 suggested prolonged treatment for more severe hip dysplasia, as it was beneficial to the developing acetabulum and stabilization of the hip, especially for Graf type III hips. Other researchers have recommended age-dependent treatment protocols and suggest a prolonged treatment for older infants.24,25 Ömeroglu proposed a maximum duration of 8 weeks of the PH for stable dysplasia hips (Graf IIa, IIb, or IIc); if there was no improvement or worsening within 8 weeks, the treatment was considered as the failure. 26 The mean duration was 10 weeks in this study. There was a weakly negative relationship to the initial α angle (Figure 2); the smaller the angle, the longer the duration. However, it was not significantly associated with RAD.
The blunt bony rim indicates a pathological lateral epiphysis of the acetabulum, which may result from abnormal blood vascular supplement. Alexiev et al. 7 found that the hyaline cartilage becomes fibrous and deformed resulting in a pathological cartilaginous roof echogenicity, which was the most specific predictor of residual dysplasia of hip. In this study, the blunt bony rim at the end of treatment is a significant independent factor associated with RAD (Figure 3). Although all hips achieved an α angle greater than 60°at the end of the treatment, 26 hips had blunt bony rims, 17 hips (65%) were identified to have RAD at the last follow-up, and all of them occurred in female patients. In addition, the sonographic blunt bony rim may develop to an upward sourcil on the pelvic radiography (Figure 4). A short, interrupted, upward sourcil indicated an uneven distribution of pressure forces on the weight-bearing surface and was related to acetabular dysplasia. 27 Why a stable dysplasia hip, which obtained early ultrasonographic normality after treatment of the PH, became late dysplasia is still unclear. Histological analysis showed that the acetabular cartilage in dysplastic hips was thicker than that of normal hips. 28 This phenomenon was also observed by US and magnetic resonance imaging.29,30 Several genetic factors have been identified as being associated with the development of DDH, which may intervene the cartilage development. 31 In addition, capsule laxity is also considered as a primary cause of postnatal subluxation and dislocation. 32 In agreement with this point, we speculated that gene-related acetabular cartilage dysplasia combined the capsular laxity might lead to mild lateral displacement of the femoral head after infants begin to stand. The abnormal loading can cause a lateral interrupted sourcil on the radiograph, which is more common in female patients.
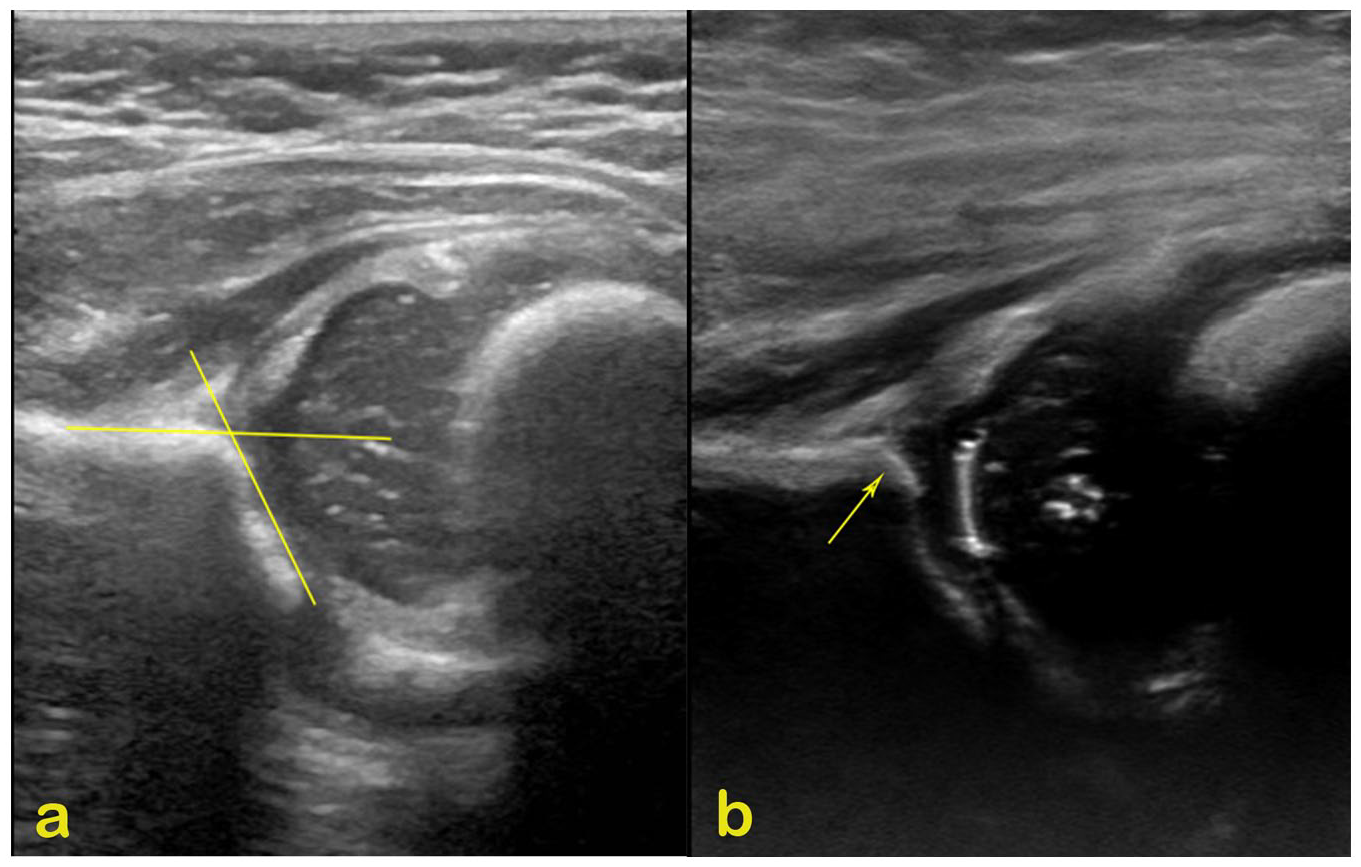
(a) Coronal plane US of the left side hip appearance before Pavlik harness in a 12-week-old girl, α angle of 58°, was measured according to the technique of Graf; (b) repeat US after 6 weeks of treatment, α angle of 66°, while the acetabular bony rim is still blunt. US: ultrasound scan.
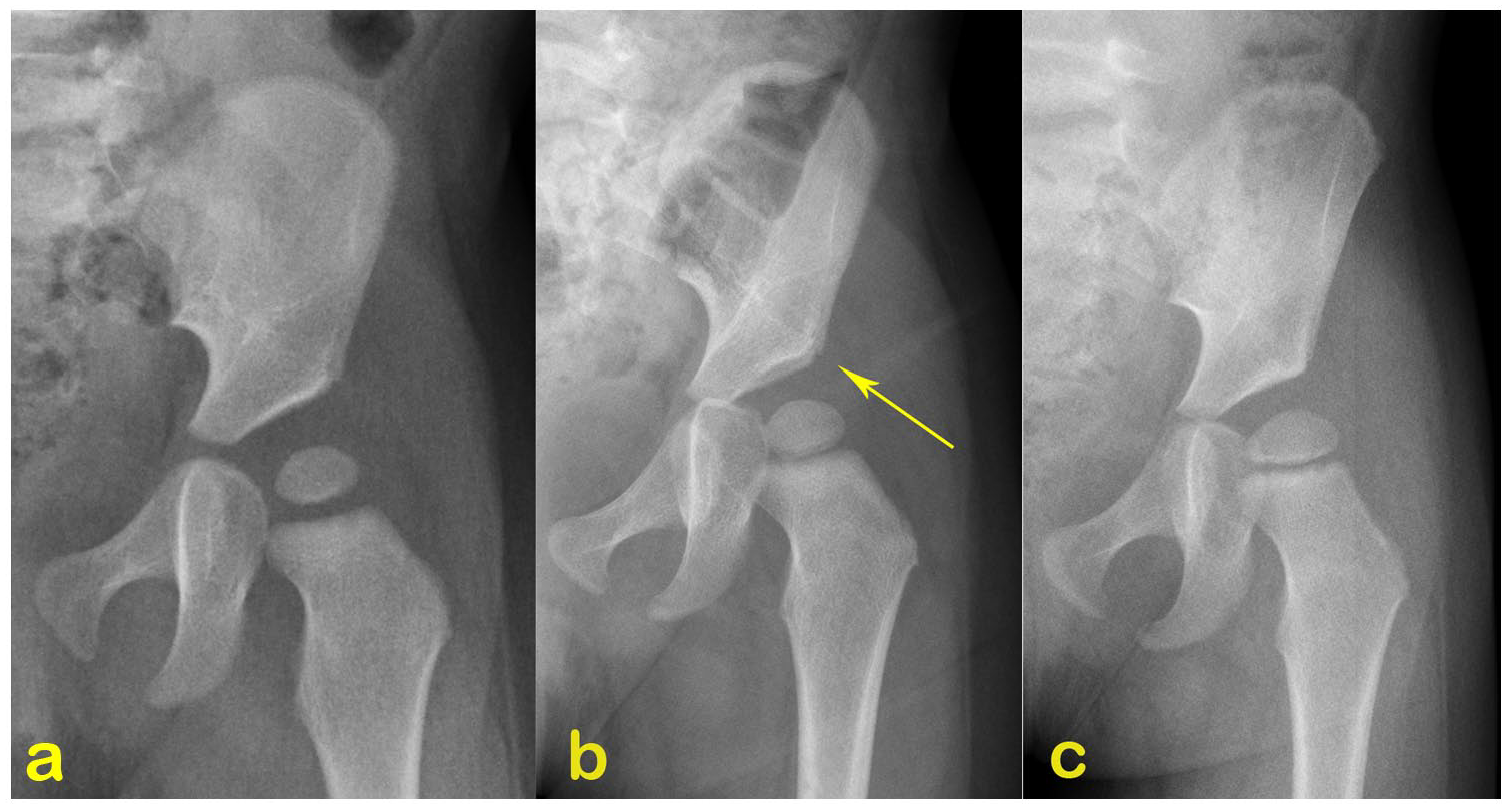
Serial radiographic follow-up of the girl. (a) At the age of 12 months, the lateral end of the sourcil is upward and did not extend to the lateral bony margin of the acetabular roof, acetabular index of 32°; (b) radiograph at the age of 18 months and acetabular index of 30°. Mild acetabular dysplasia is observed according to Tönnis criteria; (c) acetabular dysplasia developed by the age of 30 months, with an acetabular index of 30° greater than 2 SDs above the mean. SD: standard deviation.
When discussing the second question, we found our result was contrary to the hypothesis. Although the initial α did not show a statistically significant to the RAD in the regression model, we found a significant difference when comparing the mean value of the initial α angle between RAD hips and non-RAD hips (P = 0.007). An initial α angle greater than 55° showed a significant negative relationship with RAD. In other words, a type II dysplasia hip with a relatively larger α angle might have an unfavorable outcome compared with one with a smaller α angle. Meanwhile, the mean treatment age was relatively older in patients with an initial α angle greater than 55°. The wait-and-see regime, which leads to treatment delay, can explain such results. A study by Sakkers and Pollet 33 found that normal development without treatment in the first 6 months for Graf type IIa to IIc was between 80% and 97% from clustered data. Those mild dysplasia hips are expected to normalize spontaneously without treatment. Some parents were reluctant to start the treatment until there were no improvements after repeat US. However, Ömeroğlu et al. 34 studied the natural history of 285 type IIa hips and found that although about 80% of type IIa hips showed spontaneous normalization at 6–7 weeks of age, 15.6% hips deteriorated to type IIa- and suggested immediate treatment for female type IIa- hips because of the potential risk of RAD. Bilgili et al. 35 reported a natural course of type IIa hips; in contrast to our results, they proposed that an α angle less than 55° on the initial US was an independent predictor for worsening. Our study included the whole type II hips, which might lead to such difference. We believed that type II hips with an α angle greater than 55° should be considered more, especially in infants close to 12 weeks of age. Further control studies in a larger population are warranted.
The incidence of residual hip dysplasia was reported between 4% and 33% at approximately 12 months of age in infants who achieved normalization of hips upon US imaging (Graf type I hip), after PH treatment.6,8,12,19 Good interobserver agreement was demonstrated on the α angle and the standard plane.36,37 However, is an α angle greater than 60° with a blunt bony rim after PH treatment considered a normal hip? Vasilescu et al. 38 proposed that as 2° of interobserver variation was allowed according to Graf’s method, type I hips with α angles of 60° and 61° could become type II if another examiner performs the US (α angle: 58° or 59°). They found that such borderline hips carry the risk of deteriorating to IIb or worse. In some studies, the treatment goal was defined as an α angle more than 64°.18,39 Some authors argued rounding or blunt acetabular rim might affect the measurement of the α angle and influence the treatment strategy.40 –42 Hareendranathan et al. 42 proposed a contour-based α angle and a rounding index to improve the reliability and accuracy of DDH diagnosis, and they found that the apex point moved 8 mm leading to a 10° change of α angle. Thus, we would prefer to choose a larger α angle to define normal hips after PH treatment. However, whether 64° is the optimal cutoff value warrants further study.
Besides the intrinsic biases of the retrospective research, our study has some limitations. One is the short follow-up period; it is unclear whether the hip dysplasia will persist or resolve spontaneously with growth. Cashman et al. 43 proposed that most patients with late dysplasia could be identified by 18 months from the development of the AI; they also suggested further evaluating the center-edge angle at 5 years of age. A long-term radiographic follow-up until skeletal maturity is warranted. Second, the limited number of patients may reduce the statistical power of this study. Although the parents were informed of the radiographic follow-up at least once at 12 months old, most did not understand why residual hip dysplasia could occur after US normalization and refused further radiographic evaluation. The COVID-19 pandemic made follow-up difficult for patients in other provinces, which is one of the reasons for loss of follow-up. Finally, because of the lack of control groups, we could not further identify the difference between the use of PH and the natural history of type II hips.
Conclusion
Despite the above limitations, we found a notable incidence of RAD in type II hips after PH treatment, wherein the blunt bony rim at the last US examination and initial age after 12 weeks were independent predictors associated with RAD. Although we cannot precisely predict which hip will persist in dysplasia, our results provided information that initiation treatment before 12 weeks has better results. Based on the results of this study, long-term radiographic follow-up evaluation is necessary for hips with an α angle greater than 60°, but with a blunt bony rim at the end of the treatment. Graf type II hip with an α angle greater than 55° needs more consideration as the high rate of RAD, especially in infants close to 12 weeks of age.
Footnotes
Authors contribution
All authors contributed to the study conception and design. Writing original draft preparation: (Yuchan Li, Zhigang Wang). Writing review and response to the reviewers, revised the article and final approval of the version: (Yuchan Li, Zhigang Wang). Data collection and analysis were performed by (Yunlan Xu, Mingyuan Miao, Jing Shi). All authors commented on previous versions of the article. All authors read and approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study received ethical approval from the Shanghai Children’s Medical Center Ethics Committee (Approval #SCMCIRB-K2018048-1) on 20 October 2018. This is an institutional review board (IRB)-approved retrospective study; all patient information was deidentified; and patient consent was not required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.