
Abstract

To the Editor,
Dear Sir
A Letter to the Editor has expressed some concerns regarding our paper on risk factors for hip displacement in cerebral palsy. 1 First, we would like to thank the authors for their interest in the study. The criticism mainly concerns the interpretation of the statistical results. We agree with the fact that statistically non-significant results are not evidence that an association between a studied variable and the outcome does not exist, and we appreciate the papers of Altman and Bland 2 and Ranstam 3 explaining this matter.
The main findings of our study were that initial migration percentage (MP) and MP progression per year were the only independent predictors of clinically significant hip displacement, defined as final MP ≥ 40%, in children <5 years of age. Other variables (gender, patient age, cerebral palsy (CP) type, initial acetabular index, and initial head-shaft angle) were not independent risk factors. The authors found it difficult to deduce which subgroup was at higher odds. This is, however, obvious from the tables, since the numbers of patients in the different subgroups were specified. Perhaps, it would be clearer if the subgroup with the lowest risk of hip displacement had been marked “Ref” (Reference value), but this was considered unnecessary.
The authors pointed out that the confidence intervals of the non-significant associations were quite wide, which implied considerable statistical uncertainty with respect to the size of these associations. The statistical results would have been more reliable if the number of patients had been larger than the 107 children who were included in Tables. We therefore reanalysed the data with another procedure: stepwise backward logistic regression, with probability for stepwise removal of variables (p value > 0.05). All the eight variables in our article were initially tested (Table 1, Step 1).
Stepwise backward logistic regression: Step 1.
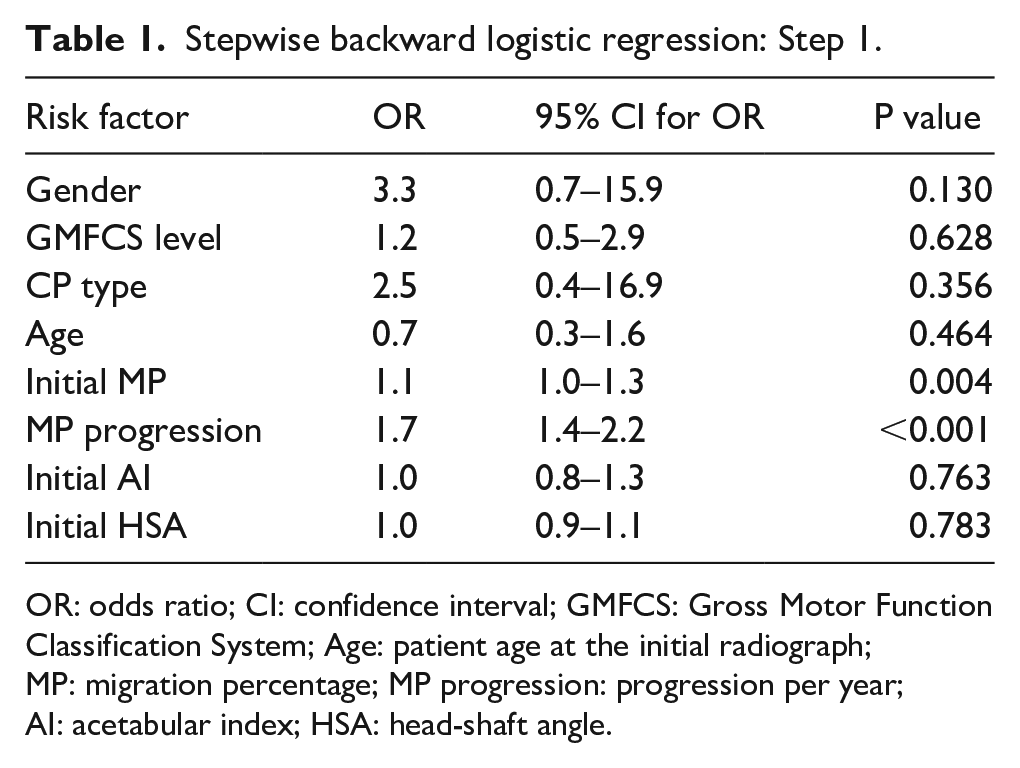
OR: odds ratio; CI: confidence interval; GMFCS: Gross Motor Function Classification System; Age: patient age at the initial radiograph; MP: migration percentage; MP progression: progression per year; AI: acetabular index; HSA: head-shaft angle.
“Initial HSA” had the highest p value and was omitted from the next step. In Step 2, “initial AI” had the highest p value and was therefore eliminated, as was “GMFCS level” in Step 3, “Age” in Step 4, “CP type” in Step 5, and “Gender” in Step 6. The two remaining variables (“Initial MP” and “MP progression”) were significant predictors in all the steps of the analysis and both had p values <0.001 in Step 7. This way of analyzing the data gave the same results as those we presented in Tables 1 and 2 of the original article. Thus, we maintain our conclusion that initial MP and MP progression per year were the only independent predictors of clinically significant hip displacement. However, we cannot, with absolute certainty, exclude that some of the other variables could be significantly associated with hip displacement if the number of patients had been larger and thus added strength to the study.
There is obviously no consensus regarding risk factors for hip displacement in CP, and the authors conclude their letter with this assertation: “This question remains open.” Thus, further research based on multivariable analysis is needed.
Footnotes
Acknowledgements
The authors would like to thank the statistician Are Hugo Pripp for help with the statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.