
Abstract
Purpose:
Up to 4% of patients who undergo cross pinning of a pediatric supracondylar humerus fracture sustain an iatrogenic ulnar nerve palsy (IUNP). This study aims to summarize the evidence regarding the management of IUNP in this setting, and to identify if early intervention (early wire removal or exploration) leads to faster and/or more complete recovery of the ulnar nerve.
Methods:
A formal systematic review was undertaken, with databases searched including Ovid Medline, Embase and Cochrane central. This was performed in accordance with JBI methodology and PRISMA guidelines.
Results:
In all, 26 articles were included in final evaluation, reporting a total of 179 IUNP. In all, 153 cases (85%) were managed expectantly, reporting full recovery at final follow-up (average 4.5 months) in 140 cases (91%). There were 26 cases of IUNP which were managed with early wire removal and/or exploration, of which 22 had full recovery (85%). There were 17 cases of 179 (9%) which did not have full recovery.
Conclusion:
The majority of IUNP are managed expectantly, with approximately 90% achieving full recovery at final follow-up. The literature does not support early wire removal and/or exploration, possibly because the damage to the nerve is done at the time of wire placement.
Keywords
Introduction
Pediatric supracondylar humerus fractures (SCHF) account for approximately 75% of all pediatric elbow fractures. 1 There is debate in the literature regarding crossed versus lateral wires only for fracture fixation; lateral wires are not as stable but avoid the morbidity of an ulnar nerve injury.2,3
Iatrogenic ulnar nerve injuries with crossed Kirshner-wires (k-wires) occur in approximately 4% of cases treated with k-wire fixation. 1 This is decreased to 0.4%–1.8% if a mini-open approach is used for the medial wire.2,4 There is no consensus how to treat these iatrogenic nerve palsies. Some authors advocate treatment of the fracture without early intervention;5,6 others advocate for early wire removal or repositioning7,8 and/or early exploration of the ulnar nerve.9,10
This systematic review aims to summarize the evidence regarding the timing of wire removal and/or surgical intervention for iatrogenic ulnar nerve palsies. Does early intervention lead to a faster and/or more complete recovery of the ulnar nerve when compared with expectant management?
Methods
The review has been registered with the International Prospective Register of Systematic Reviews (PROSPERO, CRD42021281131) and written using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Supplemental Appendix 1). 11 Using the Joanna Briggs Institute (JBI) guidelines, 12 a search was performed on Ovid MEDLINE to identify keywords and terms. Databases searched included Ovid MEDLINE, The Cochrane Central Register of Controlled Trials and The Cochrane Database of Systematic Review and Embase, with the key words and terms (Supplemental Appendix 2). Studies from bibliographies were then considered.
The inclusion criteria included papers published in the English language after the year 1950-, with patients aged 2–12 years old with an ulnar nerve palsy attributed to medial wire insertion to treat supracondylar fracture of the humerus, with documented follow-up of management and function after the nerve palsy.
Exclusion criteria included children with supracondylar humerus fractures with an ulnar nerve palsy not attributed to the medial wire (e.g., if the nerve palsy was present preoperatively, or there was a postoperative ulnar nerve palsy without a medial wire), and patients who did not have documented management, follow-up or assessment of function after their iatrogenic nerve palsy.
Experimental, quasi-experimental and analytical observation study designs from after 1950 were included. Our systematic review investigated clinical management and outcome of iatrogenic ulnar nerve palsy after a smooth medial wire to treat pediatric supracondylar humerus fractures with either:
No treatment of the nerve palsy (wires were removed at the usual time) OR
Treatment of the nerve palsy by early wire removal +/- exploration of the nerve (the exposure).
The primary measure of outcome was clinical nerve function at final follow-up. Secondary outcomes included time to full recovery, need for secondary surgery, and findings at exploration.
Data extraction was performed by four independent investigators (GD, YH, MK and JS). Any discrepancies were discussed and resolved with the senior investigator (CG). Each eligible article was critically appraised for bias by two independent investigators (MK and JS) using the Joanna Briggs Institute Critical Appraisal Checklist for the specific study type (Supplemental Appendices 3–6). 12 Cohort studies with complete follow-up were scored out of 11, case reports out of 8, and case series out of 10. Cohort studies without confounding factors OR incomplete follow-up were scored out of 10, and cohort studies without confounding factors AND without incomplete follow-up were scored out of 9.
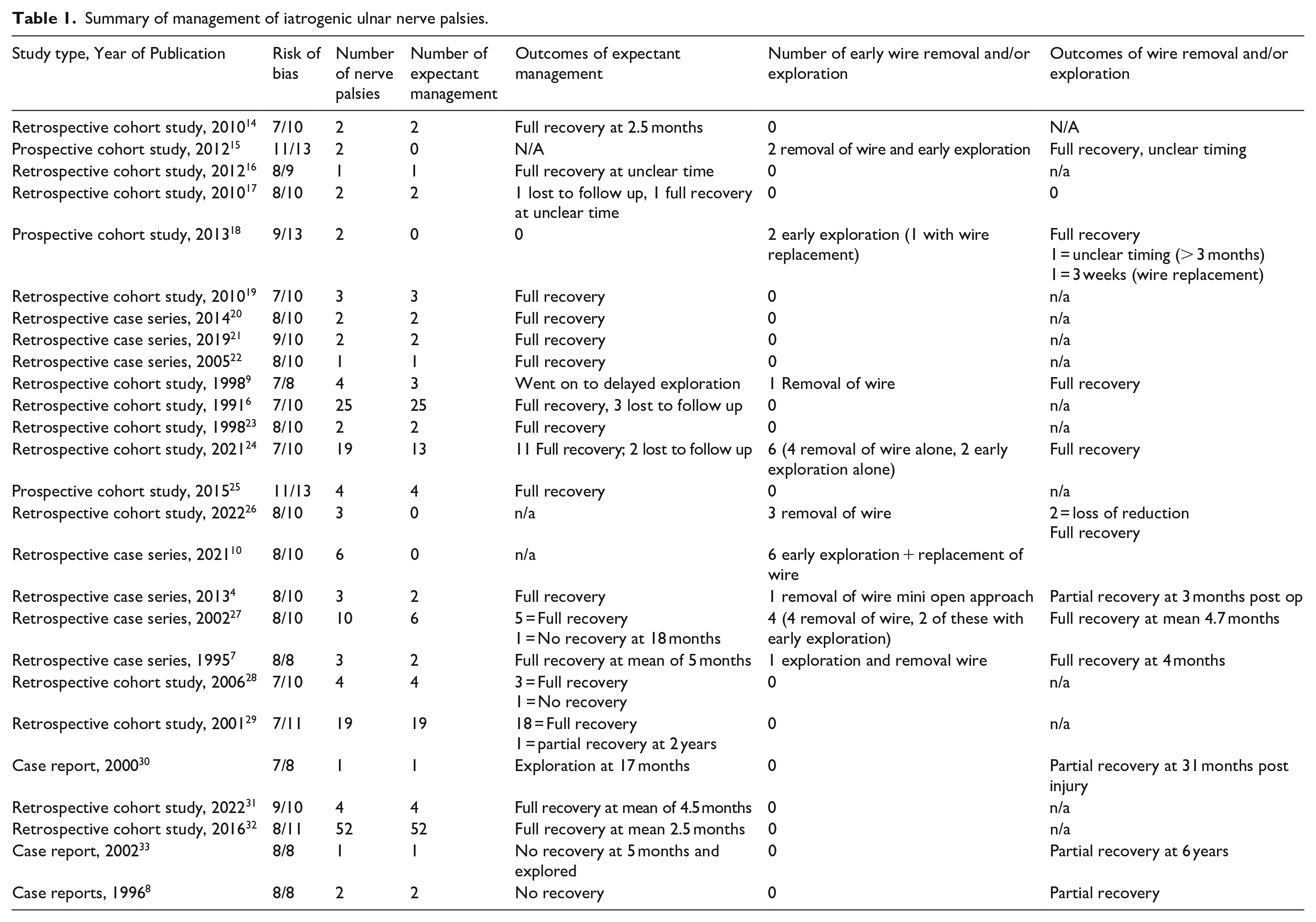
Meta-analysis was not possible due to the heterogeneity of the data. Qualitative data were reported according to JBI, with thematic and tabular synthesis. 12 Patients managed with expectant treatment of the iatrogenic ulnar nerve palsy (wire was removed at the usual time of 3–6 weeks) were compared with patients managed with treatment of the iatrogenic ulnar nerve palsy with early wire removal +/- exploration of the nerve (Table 1).
Summary of management of iatrogenic ulnar nerve palsies.
Results
Twenty-six articles were included (Figure 1). Sixteen articles with Level III evidence, seven articles with Level IV evidence and three articles with Level V evidence were included, using Merlin’s hierarchy of evidence. 13
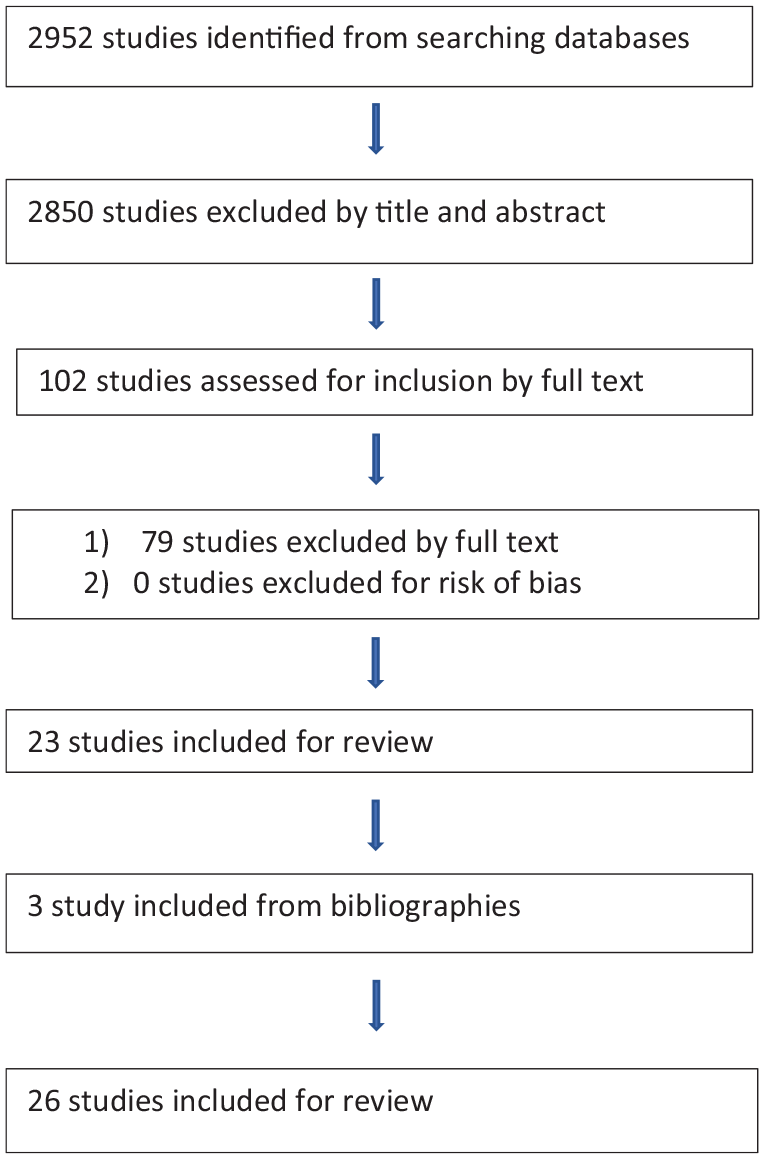
PRISMA diagram detailing the inclusion and exclusion of articles.
Number of iatrogenic ulnar nerve palsies and management
A total of 179 iatrogenic ulnar nerve palsies were reported in our literature review (Table 1). Four (2.2%) occurred using a mini open approach, and 175 occurred using a percutaneous approach. A total of 153 (85.5%) nerves were managed expectantly, without any early intervention. Ten (5.6%) nerves were managed with early wire removal alone, whereas 13 (6.1%) were managed with early wire removal/replacement and ulnar nerve exploration. Three (2.8%) were managed with ulnar nerve exploration only. The outcomes of each intervention will be discussed below.
Expectant management
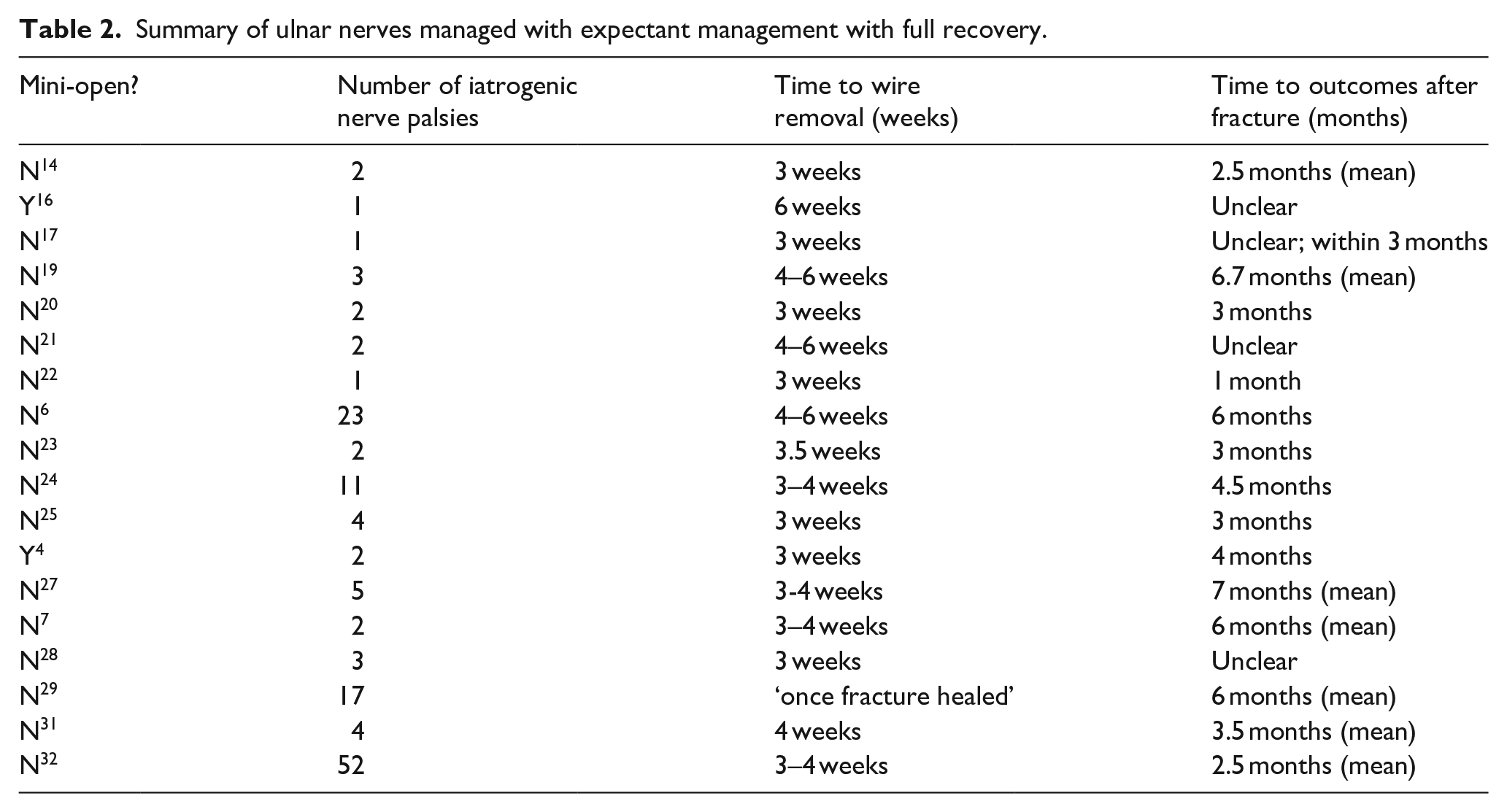
A total of 140 (91% of expectant management group) ulnar nerves had full recovery with expectant management, with an average time to wire removal of 3.5 weeks (Table 2). Four papers did not report the timing of recovery. Most papers report full recovery “at final follow up,” meaning the nerves may have recovered prior to final follow-up. The data suggest an average time to full recovery in this group of 4.5 months.
Summary of ulnar nerves managed with expectant management with full recovery.
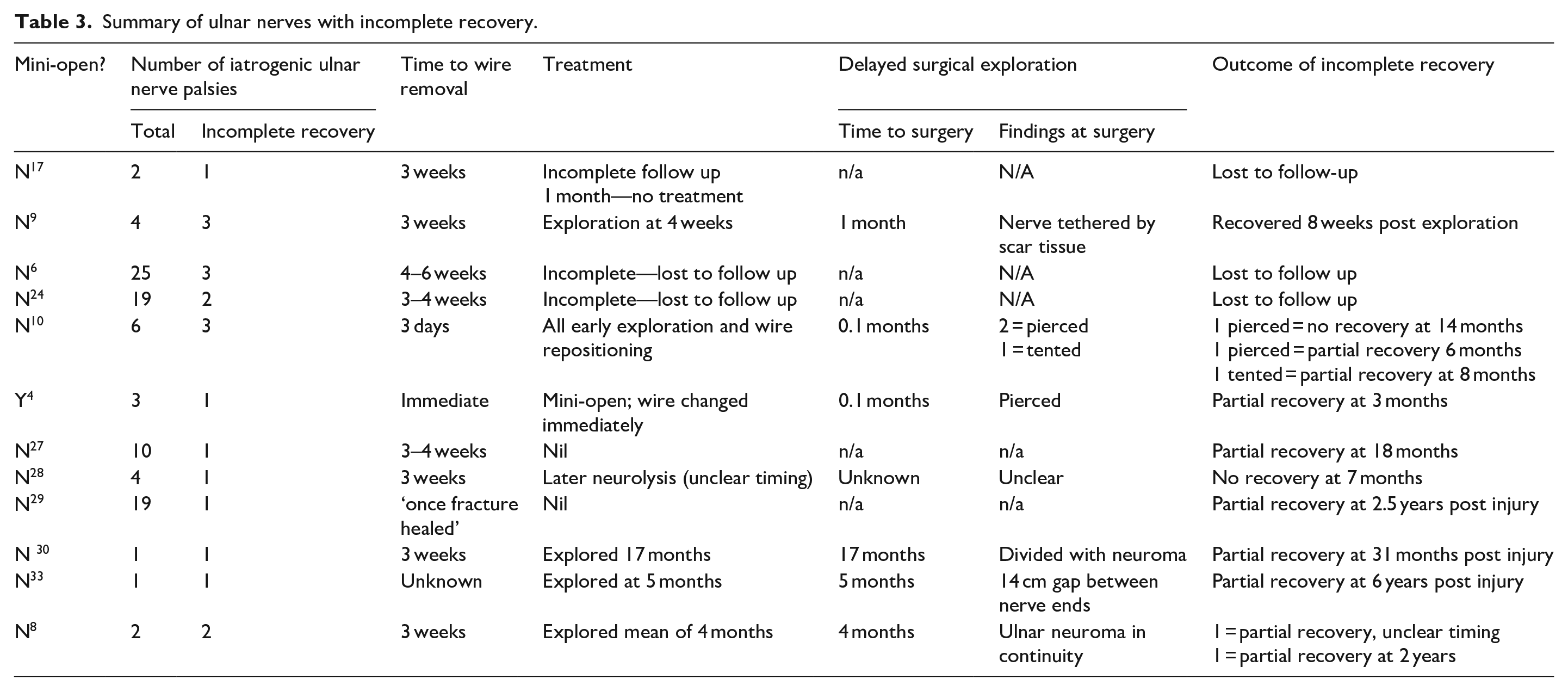
In comparison, 13 (8.5% of expectant management group) ulnar nerves did not have documented full recovery (Table 3). Of the nerves without full recovery, only one had had a mini-open approach, compared with 19 that had had a percutaneous pinning.
Summary of ulnar nerves with incomplete recovery.
Early intervention (exposure)
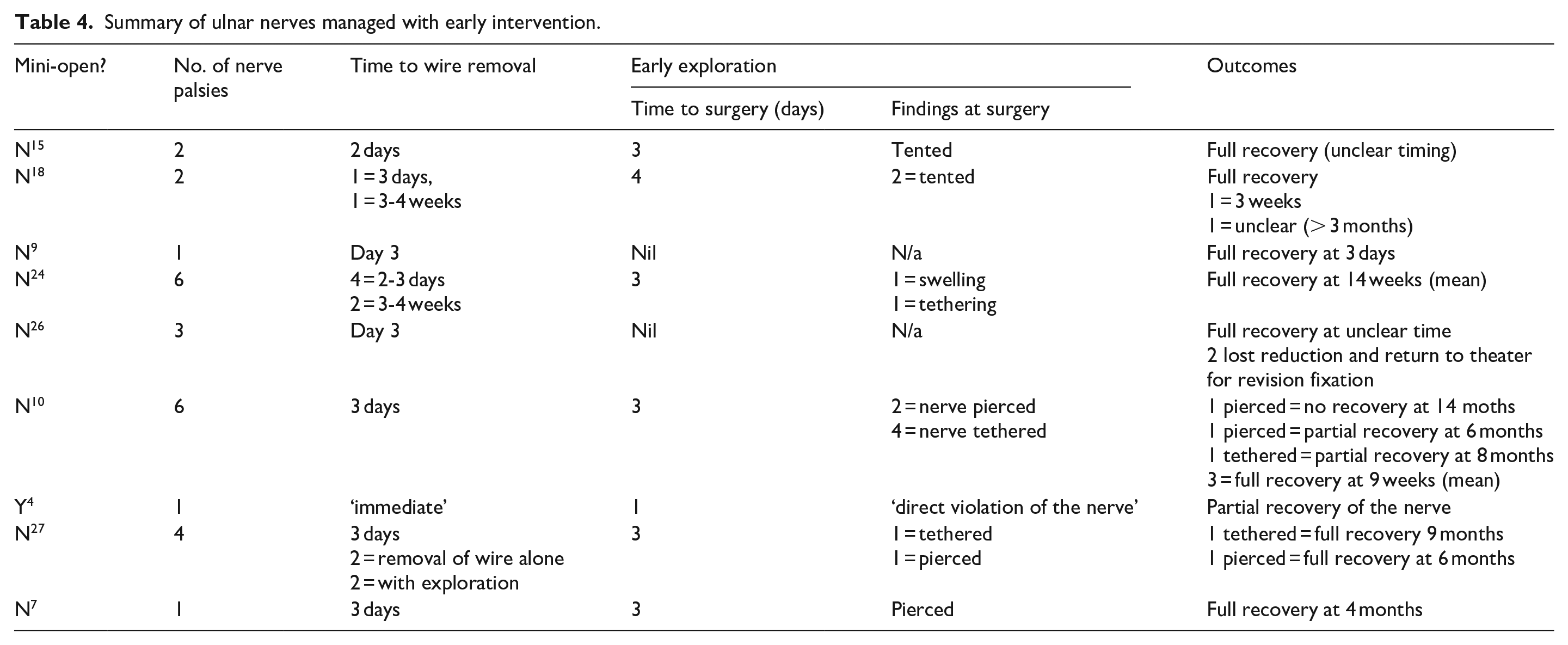
In all, 26 (14.5%) iatrogenic ulnar nerve palsies were managed with either early wire removal alone (10 nerves), early exploration with wire removal or replacement (13 nerves) or early exploration alone (3 nerves) (Table 1). Four (15.4% of the exposure group) did not have documented full recovery (Table 3). Of the explored nerves, there were no divided nerves requiring repair or grafting. Of the 10 patients managed with early wire removal alone, 2 were reported to have loss of reduction and a return to theater for revision 26 (Table 4).
Summary of ulnar nerves managed with early intervention.
Discussion
There is a paucity of robust data in the literature regarding management of this complication to guide clinicians in decision making. This is problematic from both clinical and medicolegal perspectives. Two of the largest series29,32 suggest that an expectant approach in managing iatrogenic ulnar nerve injuries is safe. In the papers in which there was early exploration of the nerve, no reason was given as to why some nerves were managed with early exploration versus expectant management (Tables 1 and 4).
Unfortunately, this is not the same experience shared by others. Although most authors managed their iatrogenic ulnar nerve palsies expectantly, this was often because the complication was not picked up until the wires were removed at the 3- to 6-week mark. Excluding those who were lost to follow up, 7 (4.6% of expectant management) ulnar nerve palsies did not fully recover at final follow-up. Of those who had early intervention, 4 (15.4% of the exposure group) did not fully recover at final follow-up. These data came from 2 papers,4,10 and due to the very low numbers and heterogeneity of the data, no statistics could be applied.
In the papers in which there was early exploration of the nerve, no reason was given as to why some nerves were managed with early exploration versus expectant management (Tables 1 and 4). Diagnosis of the ulnar nerve palsy was clinical in all papers. Description of the ulnar nerve palsy was rarely delineated in the literature; few authors described if the clinical signs were sensory alone or both motor and sensory, complete or partial. “Full recovery” was also rarely defined and was diagnosed clinically.
Current literature does not support early wire removal and/or exploration, which may be because the damage to the nerve is done at the time of wire placement. Due to the lack of centers reporting their management and outcomes, it is recommended that clinicians proceed with caution in their practice on a case by case basis until further research is reported.
It would be useful for other centers to publish their results in management of iatrogenic ulnar nerve palsies to further guide clinicians. A prosective randomized or quasi-randomized controlled trial could also be considered. This paper represents the largest pooled research of iatrogenic ulnar nerve palsy and can summarize several important points:
It may be safe to manage iatrogenic ulnar nerve palsies with expectant management as early intervention may not improve outcomes.
Approximately 90% of iatrogenic ulnar nerve palsies managed expectantly will return to full function.
Even if an ulnar nerve palsy is “recovering,” it is important to follow the patient to full recovery, as a small percentage do not fully recover.
Future studies in this field would benefit clinicians in their discussion with patients and their families as to how to treat iatrogenic ulnar nerve palsies. In these future studies, results that need to be reported should include: (a) A clear distinction between acute iatrogenic ulnar nerve injury (motor and sensory loss) and iatrogenic ulnar nerve impingement or irritation (sensory change) because of their very different clinical consequences.
4
(b) Timing to detection and management of the ulnar nerve palsy including time to removal of the medial wire and/or exploration. (c) Findings at surgical exploration. (d) Other complications such as loss of reduction. (e) Detailed clinical recovery at final follow-up.
Supplemental Material
sj-docx-1-cho-10.1177_18632521221124632 – Supplemental material for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review
Supplemental material, sj-docx-1-cho-10.1177_18632521221124632 for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review by Christy Graff, George Dennis Dounas, Jonghoo Sung, Medhir Kumawat, Yue Huang and Maya Todd in Journal of Children’s Orthopaedics
Supplemental Material
sj-docx-2-cho-10.1177_18632521221124632 – Supplemental material for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review
Supplemental material, sj-docx-2-cho-10.1177_18632521221124632 for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review by Christy Graff, George Dennis Dounas, Jonghoo Sung, Medhir Kumawat, Yue Huang and Maya Todd in Journal of Children’s Orthopaedics
Supplemental Material
sj-docx-3-cho-10.1177_18632521221124632 – Supplemental material for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review
Supplemental material, sj-docx-3-cho-10.1177_18632521221124632 for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review by Christy Graff, George Dennis Dounas, Jonghoo Sung, Medhir Kumawat, Yue Huang and Maya Todd in Journal of Children’s Orthopaedics
Supplemental Material
sj-docx-4-cho-10.1177_18632521221124632 – Supplemental material for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review
Supplemental material, sj-docx-4-cho-10.1177_18632521221124632 for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review by Christy Graff, George Dennis Dounas, Jonghoo Sung, Medhir Kumawat, Yue Huang and Maya Todd in Journal of Children’s Orthopaedics
Supplemental Material
sj-docx-5-cho-10.1177_18632521221124632 – Supplemental material for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review
Supplemental material, sj-docx-5-cho-10.1177_18632521221124632 for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review by Christy Graff, George Dennis Dounas, Jonghoo Sung, Medhir Kumawat, Yue Huang and Maya Todd in Journal of Children’s Orthopaedics
Supplemental Material
sj-docx-6-cho-10.1177_18632521221124632 – Supplemental material for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review
Supplemental material, sj-docx-6-cho-10.1177_18632521221124632 for Management of iatrogenic ulnar nerve palsies after cross pinning of pediatric supracondylar humerus fractures: A systematic review by Christy Graff, George Dennis Dounas, Jonghoo Sung, Medhir Kumawat, Yue Huang and Maya Todd in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Compliance with ethical standards
Approval not needed due to study type. There are no human participants in this article and informed consent is not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.