
Abstract
Purpose:
Pes planus (or flatfoot) is the most common deformity in children with cerebral palsy. There are several surgical interventions used to treat it: single calcaneal osteotomies, extra-articular arthrodesis, double calcaneal osteotomy, calcaneo-cuboid-cuneiform osteotomy, intra-articular arthrodesis, and arthroereisis. There is currently no evidence on optimal treatment for flatfoot in children with cerebral palsy. Our purpose is to systematically review studies reporting complications, recurrence rates, and radiological outcomes of the surgical management of flatfoot in children with cerebral palsy.
Methods:
Five databases were searched to identify studies published from inception until July 2021, with keywords relating to flatfoot, cerebral palsy, and surgical interventions. We included prospective, retrospective, and comparative study designs in the English language. Data was extracted and tabulated in duplicate into Excel, and analysis was conducted using Python SciPy.
Results:
In total, 1220 studies were identified of which 44 met the inclusion criteria, comprising 2234 feet in 1364 patients with a mean age of 10.3 years and mean follow-up of 55.9 months. Radiographic outcomes showed improvement with all procedures; complications and recurrence rates were too poorly reported to compare. Only 6 (14%) studies were assessed as a low risk of bias. There was substantial heterogeneity of outcome measures.
Conclusion:
There is a lack of high-quality, comparative studies assessing the radiological outcomes, complications, and recurrence rates of surgical alternatives to treat flatfoot in children with cerebral palsy. There is currently no clear evidence on optimal surgical treatment.
Level of evidence:
IIa based on Oxford Centre for Evidence-based Medicine.
Introduction
Pes planus (also known as flatfoot or pes planovalgus) is the most common foot deformity in children with cerebral palsy (CP). 1 The pathology develops due to the lateral displacement of the navicular, causing loss of the medial longitudinal arch, talar head uncovering, and talar prominence in the medial foot. 1 The condition can be categorized into flexible and stiff. 2 Flexible deformity involves preservation of the arch when sitting, extending the great toe or standing on tiptoes; stiff deformity involves a flat arch with limitation of motion during weight-bearing and non-weight-bearing, and is more difficult to treat. 3 Higher functioning, ambulatory patients (Gross Motor Function Classification System (GMFCS) I–III) usually present with flexible flatfoot, whereas stiff flatfoot is more common in adolescents with lower functional ability (GMFCS IV–V). 4 The deformity usually worsens during late childhood and can cause significant pain, pressure ulcers, and difficulty walking or wearing shoes.3,5 Surgical management is indicated when conservative measures have failed.
There are several surgical interventions used to treat pes planus but no guidelines on how to choose between them. Extra-articular arthrodesis (EAA) or single calcaneal osteotomies (SCO) are commonly used to treat children with milder, flexible deformities, and lower GMFCS levels. SCO includes calcaneal lateral column lengthening (LCL) and calcaneal slide (CS) with concomitant soft tissue procedures (peroneus brevis lengthening, tibialis posterior shortening, and talonavicular joint capsule reefing), and occasionally a medial cuneiform osteotomy. Double calcaneal osteotomy (DCO) and calcaneo-cuboid-cuneiform “triple C” osteotomies (TCO) have been used to treat moderate-to-severe deformities that would likely recur with SCO and EAA. 6 Intra-articular arthrodesis (IAA) is an invasive procedure that has been reserved for children with GMFCS IV or V and/or severe, stiff deformities.1,5 Subtalar arthroereisis (SA) is a non-fusion procedure that has recently received renewed interest in the literature as an alternative to SCO and EAA. 2
The purpose of this study is to systematically review the literature regarding the radiological outcomes, complications, and recurrence rates of current surgical management of flatfoot in children with CP.
Methods
This systematic review was reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA 2020) checklist and the AMSTAR 2 critical appraisal tool.7,8 The protocol was prospectively registered on PROSPERO CRD420201239285. 9 The authors declare no conflict of interest relevant to this work.
Search strategy
A literature search was conducted using the online Cochrane Library, EMBASE, MEDLINE, Web of Science, and PubMed databases, using the following terms: ((cerebral palsy)) AND (((pes planus) OR (flat foot) OR (pes planovalgus)) OR ((calcaneal) OR (calcaneus) OR (calcaneum) OR (slide) OR (double) OR (heel) AND (osteotomy) OR ((fusion) OR (arthrodesis) OR ((arthroereisis) OR ((Grice Green) OR (Grice-Green) OR ((lateral column lengthening) OR (MOSCA))). No limitations were placed on gender, date, or language. All results from inception until July 31, 2021 were included (Appendix 1).
Inclusion criteria
We included all prospective, retrospective, and comparative study designs (randomized controlled trials (RCTs), case studies, cohort studies, and case-controlled studies) reporting original/primary data on one or more of the outcomes of interest. A scoping review identified a significant lack of RCTs on this subject, thus including non-randomized studies was necessary for an all-encompassing review.
Exclusion criteria
We excluded duplicate articles, cost-effectiveness studies, and studies not reporting on primary data (such as review articles, editorials, discussions, commentaries, letters, and conference abstracts). We excluded studies not reporting data on radiographic outcomes, complications, and recurrence rates. Studies where data for pediatric patients with CP was not readily separable from other participants and where surgery was not the primary intervention were excluded on the grounds of not being relevant to the aims of the review.
Participants
Children with CP and symptomatic pes planus were included. Studies with a mean age of participants below 18 years of age were included. Children without CP treated for foot deformities other than pes planus were not included.
Intervention
The intervention was operative surgical management to treat symptomatic pes planus where conservative management had failed. The specific procedures identified by a scoping review included calcaneal LCL, EAA, CS, DCO, calcaneo-cuboid-cuneiform TCO, IAA, and SA. Data on variations of these procedures and any soft tissue procedures performed in conjunction was also extracted.
LCL is a procedure originally described by Evans that equalizes both columns in the foot via an osteotomy of the calcaneus bone approximately 1.5 cm proximal to the calcaneocuboid joint; as the lateral column is shorter in flatfoot, this equalization corrects forefoot abduction and restores the medial longitudinal arch. 10 Mosca popularized the procedure by adding the soft tissue procedures of peroneus brevis lengthening, tibialis posterior shortening, and talonavicular joint reefing, and a plantar closing-wedge osteotomy of the medial cuneiform. 11
EAA, originally used by Green and first reported by Grice in 1952, involves the extra-articular positioning of a structural autograft (either fibula or anterior tibia) between the talus and the calcaneus. 12
CS is the medial displacement of the posterior part of the calcaneus, thus creating a compensating deformity to improve the heel valgus and normal weight-bearing. 13 DCO is a combination of LCL and CS.
TCO is a versatile procedure that allows correction at the fore-, mid- and hindfoot by three osteotomies: a CS, an opening-wedge cuboid osteotomy, and a plantar flexion closing-wedge osteotomy of the medial cuneiform. 14
SA involves the insertion of an implant into the sinus tarsi or adjacent to it to prevent talonavicular impingement which consequently blocks and corrects excessive eversion movements of talus and calcaneus, and maintains the subtalar joint in a more neutral position. 2
Finally, IAA is a fusion of one or all of the joints of the hind- or midfoot, usually undertaken as a triple arthrodesis involving the talonavicular, subtalar, and calcaneocuboid joints. 15
Comparators
There is currently no gold standard for the surgical management of flatfoot in children with CP. We included papers that surgically managed flatfoot by LCL, CS, DCO, TCO, EAA, IAA, and SA using traditional or modified techniques. Non-surgical management of flatfoot was excluded.
Outcomes
Primary outcomes were radiographic angles, complications, and recurrence rates. The radiographic angles included were most commonly used to assess flatfoot: anterior–posterior talocalcaneal (AP TC), anterior–posterior talo-first metatarsal (AP T1MT), and talonavicular coverage (TNC) angles; and lateral talocalcaneal (Lat. TC), lateral talo-first metatarsal (Lat. T1MT), calcaneal-first metatarsal (C1MT), and calcaneal pitch (CP). 2 Gait analysis and clinical outcomes were not assessed, as gait analysis is infrequently reported in studies and there is no current standardized tool for assessing clinical outcomes for each surgical procedure.
Data extraction
Study selection was performed in duplicate (P.M., C.G., and P.M., M.M.), and data extraction was performed in duplicate (P.M., C.G., and P.M., M.M.). Discrepancies over the inclusion of any study or data extraction were resolved by consensus or arbitration by senior authors (T.L.L. and M.K.).
For every article, the following data was extracted based on a scoping literature review: Article demographic details (number of authors, title, year published, level of evidence (1–5), funding sources). Patient demographic details (number of patients, number of feet operated on, gender of patients, mean age, and age range of patients; GMFCS level of disability; mean follow-up (months/years) and range of follow-up). Surgery details: type of surgery, indication for surgery, and concurrent procedures. Radiographic outcomes: AP TC, AP T1MT, and TNC angles; and Lat. TC, Lat. T1MT, C1MT, and calcaneal pitch. Complications and recurrence rates
Gait analysis and pedobarographic outcomes were not tabulated or synthesized due to the heterogeneity of the reporting between the studies.
Assessment of methodological quality
The level of evidence and methodological quality of included studies was assessed using the MINORS criteria. 16 A MINORS score of 16/16 or 24/24 was deemed high quality (and low risk of bias), 10–15/16 or 15–23/24 was deemed moderate quality (and moderate risk of bias), and a score of < 10/16 or < 15 was deemed low quality (and at high risk of bias) based on previous studies that used these scores. The articles were independently assessed by three authors (P.M., C.G., and M.M.) with a senior author settling any disagreement (T.L.L.). P.M. recorded sources of funding for individual studies included in the review.
Statistical analysis
Where data was provided, weighted means of radiographic outcomes and recurrence rates of the surgical procedures were calculated. An independent t-test was used to compare the weighted means. All data analysis was conducted using Python SciPy. 17 Radiographic results were considered statistically significant when reported to have a p-value of less than 0.05.
Results
Literature search
The initial search yielded 1220 articles for review after duplicates were removed as shown in Figure 1. Review of titles and abstracts identified 80 articles for full-text screening, of which 44 met the inclusion criteria. The main reasons for excluding articles at this stage were “no reporting of outcomes” (n = 11, 31%) and “no separation of outcomes for patients with CP to patients with different etiology for pes planus (PP)” (n = 20, 56%).
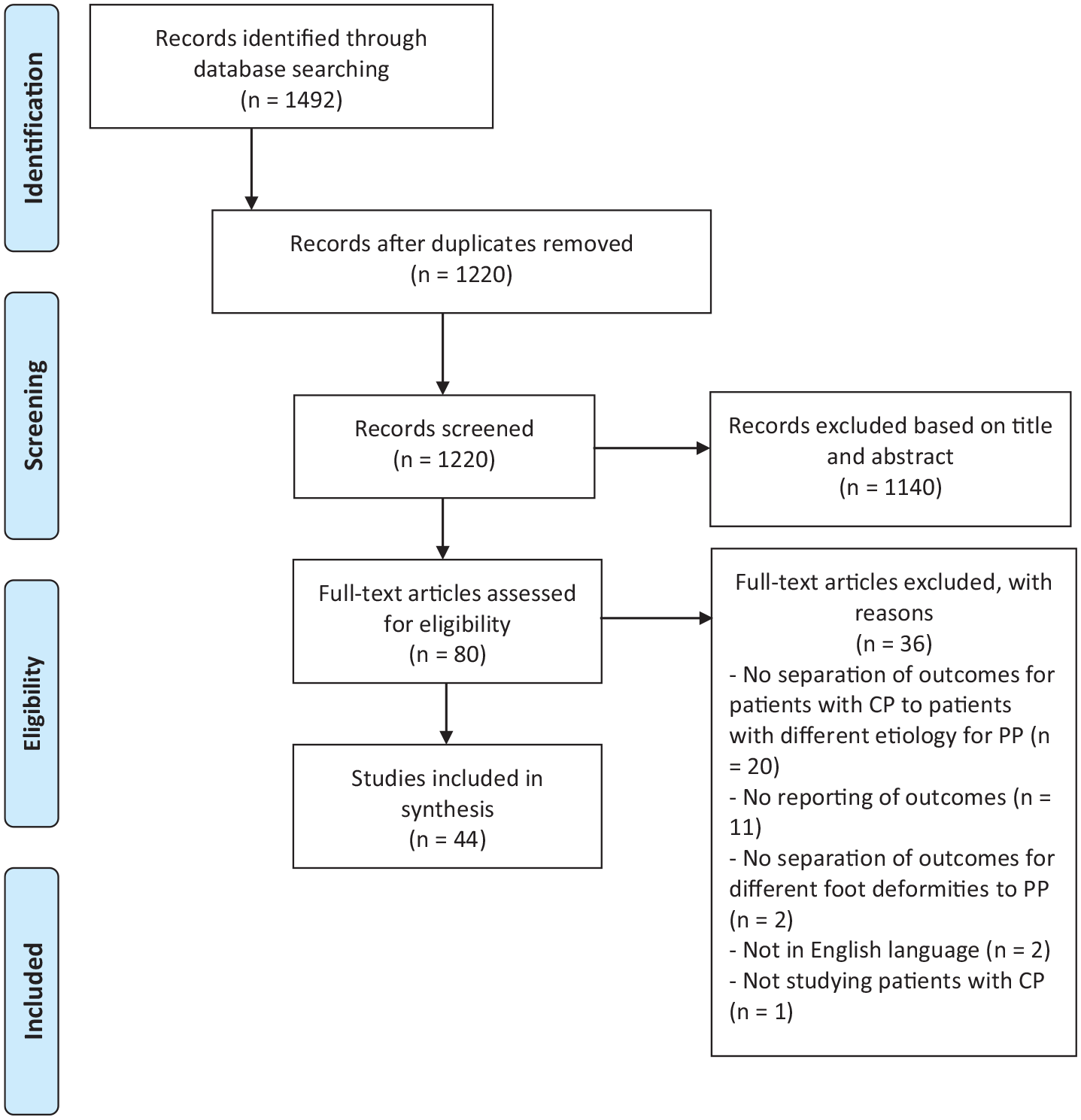
A prisma flow diagram for the systematic review detailing the database searches, the number of abstracts screened and the full texts reviewed. CP = cerebral palsy; PP = pes planus.
Study and patient characteristics
The search identified 10 comparative studies (23%): 8 of these were retrospective comparative studies (18%) and 1 was a prospective, randomized design (2%). Of the remaining studies, 7 were prospective case series (16%) and 27 were retrospective case series (63%). The study characteristics and outcomes of the papers included can be seen in Table 1 and summarized in Table 2.
Table of included studies.
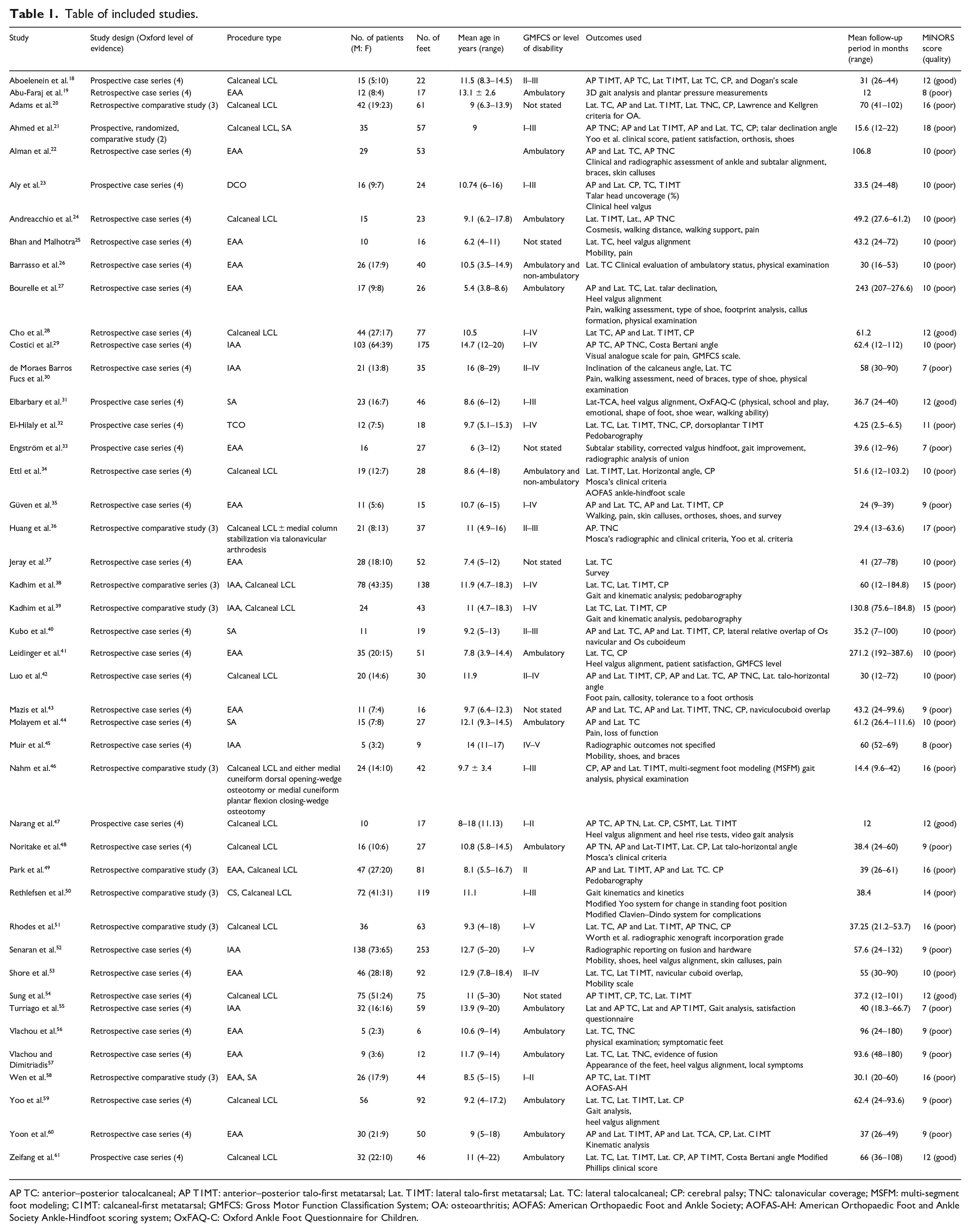
AP TC: anterior–posterior talocalcaneal; AP T1MT: anterior–posterior talo-first metatarsal; Lat. T1MT: lateral talo-first metatarsal; Lat. TC: lateral talocalcaneal; CP: cerebral palsy; TNC: talonavicular coverage; MSFM: multi-segment foot modeling; C1MT: calcaneal-first metatarsal; GMFCS: Gross Motor Function Classification System; OA: osteoarthritis; AOFAS: American Orthopaedic Foot and Ankle Society; AOFAS-AH: American Orthopaedic Foot and Ankle Society Ankle-Hindfoot scoring system; OxFAQ-C: Oxford Ankle Foot Questionnaire for Children.
Summart of included studies.
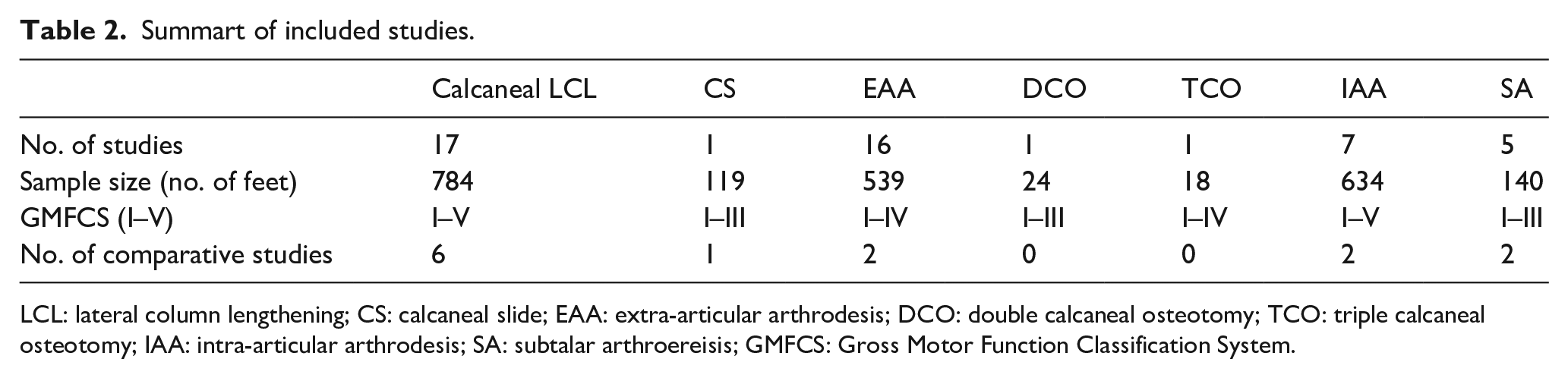
LCL: lateral column lengthening; CS: calcaneal slide; EAA: extra-articular arthrodesis; DCO: double calcaneal osteotomy; TCO: triple calcaneal osteotomy; IAA: intra-articular arthrodesis; SA: subtalar arthroereisis; GMFCS: Gross Motor Function Classification System.
The studies included 2234 feet in 1364 patients with a mean age of 10.3 years (ranging from 3 to 30 years) and a mean follow-up of 55.9 months (ranging from 4.3 to 217.2 months). Studies included patients with a GMFCS level of I–V, with both stiff and flexible flatfoot deformities. There was a significant focus on ambulatory patients with GMFCS level I–III and a flexible flatfoot deformity (n = 33, 75%).
Outcomes
A majority of the papers (75%, n = 33) reported on pre- and post-operative radiographic deformity correction outcomes. All of these papers clearly stated that the radiographs were weight-bearing. Overall, the radiographic angles showed significant improvement within normal range with the exception of the Lat. T1MT angle in LCL and the AP TC angle in IAA (Table 3).
Radiographic outcomes summarised using the weighted mean for each procedure.
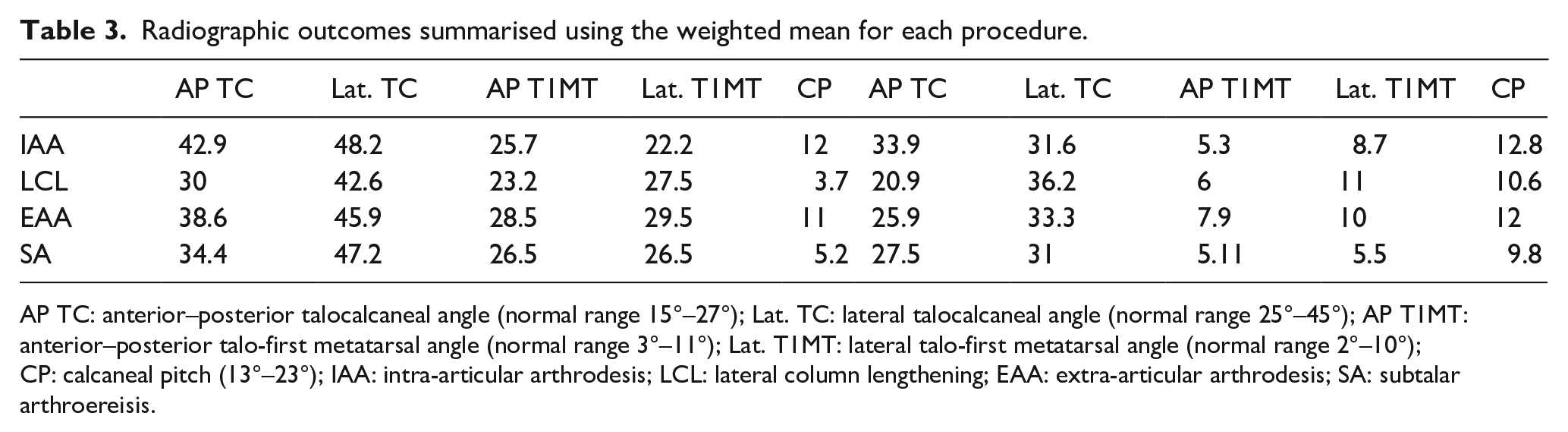
AP TC: anterior–posterior talocalcaneal angle (normal range 15°–27°); Lat. TC: lateral talocalcaneal angle (normal range 25°–45°); AP T1MT: anterior–posterior talo-first metatarsal angle (normal range 3°–11°); Lat. T1MT: lateral talo-first metatarsal angle (normal range 2°–10°); CP: calcaneal pitch (13°–23°); IAA: intra-articular arthrodesis; LCL: lateral column lengthening; EAA: extra-articular arthrodesis; SA: subtalar arthroereisis.
The clinical outcomes were measured differently in all papers (Table 1). Similarly, of the 11 studies (25%) that reported on gait analysis, kinematics, and pedobarography, the heterogeneity of the measurements meant that a comparison of the data between studies was not possible.19,32,38,39,46,47,49,50,55,59,60
Given the heterogeneity in outcome measures between the studies and their general poor quality, it was not possible to synthesize a meta-analysis. A formal narrative synthesis of the results is provided following the Synthesis Without Meta-analysis (SWiM) reporting guidelines. 62
Complications and recurrence
Data regarding complication and recurrence rates was poorly reported (Table 4). There was no clear correlation between complication rates and GMFCS level or the severity of the deformity. Recurrence rates were highest in relation to LCL and CS, and lowest in relation to DCO, TCO, and SA (Table 5).
Complications and recurrence rates.
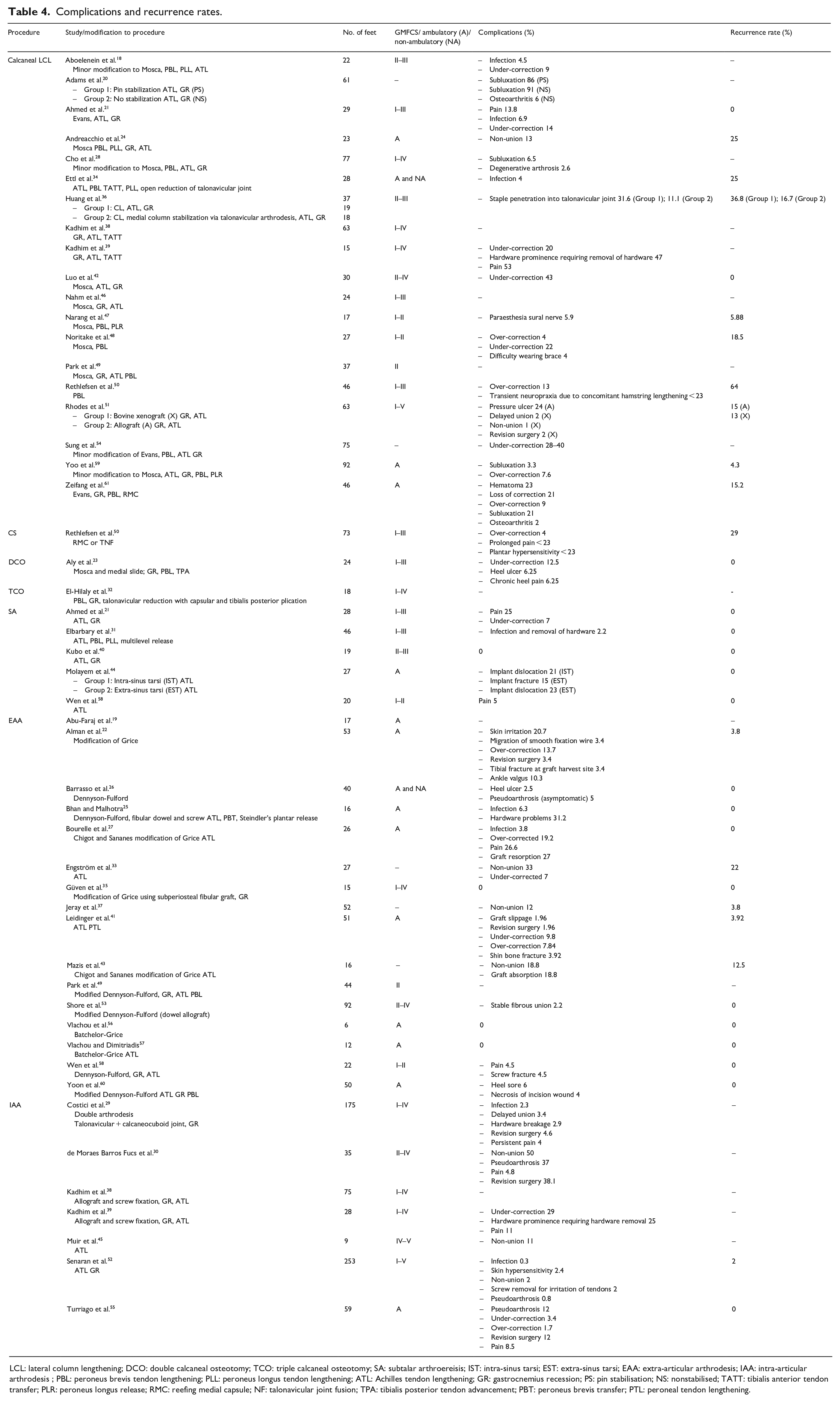
LCL: lateral column lengthening; DCO: double calcaneal osteotomy; TCO: triple calcaneal osteotomy; SA: subtalar arthroereisis; IST: intra-sinus tarsi; EST: extra-sinus tarsi; EAA: extra-articular arthrodesis; IAA: intra-articular arthrodesis ; PBL: peroneus brevis tendon lengthening; PLL: peroneus longus tendon lengthening; ATL: Achilles tendon lengthening; GR: gastrocnemius recession; PS: pin stabilisation; NS: nonstabilised; TATT: tibialis anterior tendon transfer; PLR: peroneus longus release; RMC: reefing medial capsule; NF: talonavicular joint fusion; TPA: tibialis posterior tendon advancement; PBT: peroneus brevis transfer; PTL: peroneal tendon lengthening.
Weighted mean of recurrence rates for each procedure where data was provided.

LCL: lateral column lengthening; CS: calcaneal slide; DCO: double calcaneal osteotomy; TCO: triple calcaneal osteotomy; SA: subtalar arthroereisis; EAA: extra-articular arthrodesis; IAA: intra-articular arthrodesis.
Quality of studies included
The quality of the studies included was assessed according to the MINORS criteria (Figures 2 and 3). In total, 38 studies (86%) were assessed as having a high risk of bias, and 6 (14%) studies as having a low risk of bias.
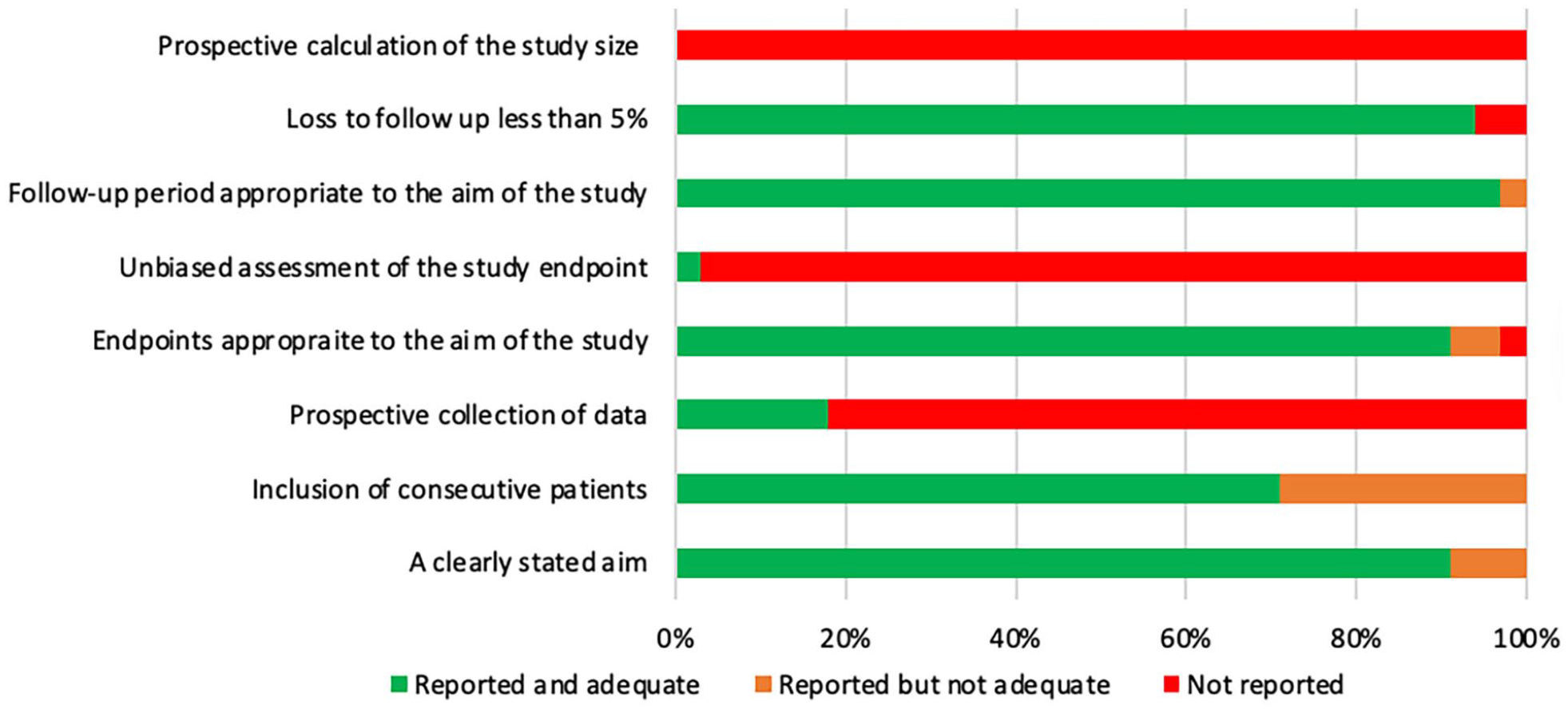
Bar chart demonstrating how non-comparative studies scored on MINORS.
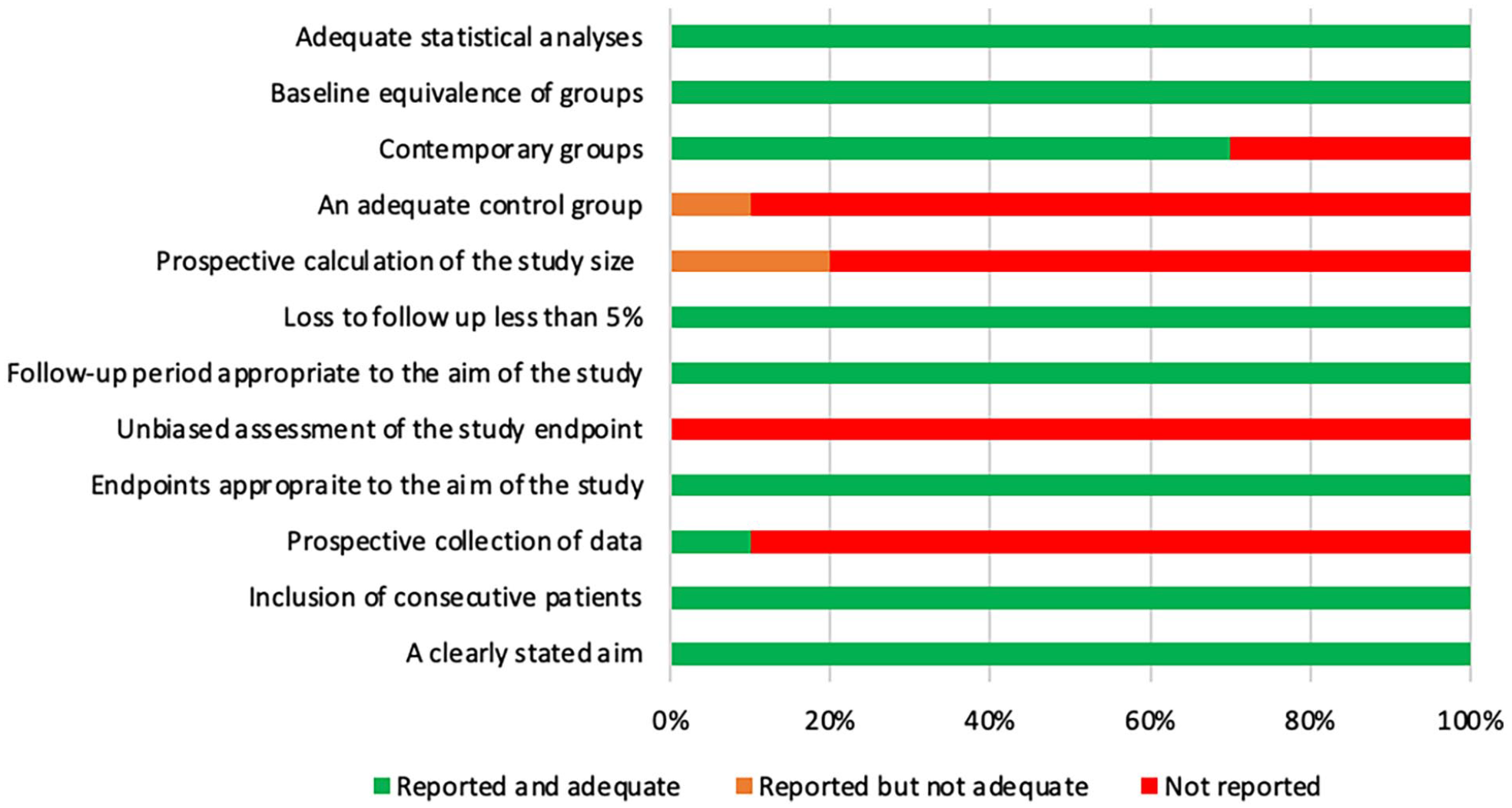
Bar chart demonstrating how comparative studies scored on MINORS.
Discussion
This is the first systematic review of surgical management of pes planus in children with CP, covering 2234 operations from 44 papers. Overall, we found that substantial deformity correction was achieved by each surgical intervention. Based on the evidence, however, it is not possible to show that one intervention is superior to others.
There is a significant lack of studies on CS, DCO, TCO, IAA, and SA (Table 2). Most of the patients included in the studies in this review had flexible deformity with lower GMFCS levels; there is limited data to allow a proper assessment of treatment for moderate–severe flatfoot deformities. Ideally, studies would separate management of stiff flatfoot in GMFCS levels IV and V from flexible flatfoot in GMFCS levels I–III as it constitutes a different deformity. Many of the papers used levels I–IV or I–V, or described the patients as “ambulant” or “non-ambulant” making it difficult to undertake subgroup analysis as the data was not always clearly separated.
The radiographic outcomes show significant improvement is achievable by all surgical interventions. Severe deformity in patients with higher GMFCS levels is difficult to treat even with an invasive procedure such as IAA, and achieving long-term correction with LCL, EAA, CS, or SA is unlikely unless there is concomitant joint fusion.34,36,50 Four of the papers offered useful parameters for when a modified or more invasive procedure than LCL or EAA should be used to treat pes planus to avoid recurrence, but these papers were limited by the bias in the studies.24,50,54,59 Some studies combined techniques, such as Nahm et al., 46 which are valid surgical options and would merit further research.
Our study has highlighted the need for a standardized method of measuring clinical outcomes. Four of the studies on LCL used either Mosca or Yoo’s clinical criteria, the latter of which was adopted by Ahmed et al., 21 to assess the results of SA.11,21,34,36,48 These criteria could be combined in future and validated to compare different procedures, but could be adapted to incorporate activity levels to assess function. There was a notable lack of patient-reported outcomes in the studies which are essential to assess the effect of treatment on the patient’s quality of life. For example, relief of pain post-procedure is an important treatment outcome that could not be assessed in our review because it was either not measured at all or not in a consistent way. Standardized methods of measuring gait analysis, kinematics, and pedobarography are also needed given a general consensus in the included studies on the limited ability of radiographic outcomes to fully reflect the clinical picture.19,32,38,39,46,47,49,50,55,59,60
The poor reporting of complications could be improved by the use of clearer definitions, for example, avoiding the interchangeable use of terms such as “non-union” and “pseudoarthrosis,” or “under-correction” and “recurrence.” The high recurrence rates seen in LCL and CS procedures compared to other procedures reflect the high risk of bias in the studies rather than the actual difference in recurrence rates, and other procedures reported significant complications such as hardware complications for SA. Any conclusions on the comparison between treatments in regard to recurrence rates and complications would be misleading given the small size of the studies, short follow-up and reporting bias which may have hidden recurrence rates and complications.
The strengths of this review are that it includes papers on multiple interventions with a large sample size and a long follow-up. The 44 studies reported on a homogeneous population with minimal loss to follow-up. The main limitation of this review is the quality of the included studies which were mostly graded as “poor” and thus had a high risk of bias. The robustness of our synthesized results is difficult to assess given that data was often missing from the studies, especially regarding complications of the procedures. Furthermore, the heterogenous complication results meant that any analysis between the procedures is difficult to undertake. The retrospective case series did not have comparator interventions, meaning a potential lack of systematic pre- and post-operative assessment, and a high risk of bias in the clinical and radiographic outcomes. P-values were often not provided by papers to demonstrate whether radiographic outcomes were statistically significant, and often not combined with clinical outcomes to make them useful. The prospective and comparative studies were weakened by small study sizes and short follow-up periods. Longer follow-up periods are needed to reliably assess whether there are any degenerative changes to adjacent joints that can occur after fusion. Degenerative changes after IAA were not reported in the six studies with a mean follow-up of 71.4 months, thus a longer follow-up may be needed to exclude this outcome.29,30,38,39,45,52,55
Conclusion
Pes planus is the most common foot condition for children with CP; a more robust evidence base is needed to provide guidance to surgeons on the optimal intervention for patients. Our review has highlighted the need for multi-center, large-scale, prospective, comparative studies, using standardized radiographic, clinical, and pedobarographic outcomes. Future studies should focus on interventions for patients with severe, stiff deformities, and higher GMFCS levels, and how the addition of fusion to procedures affects these patients in the long term.
Footnotes
Appendix 1
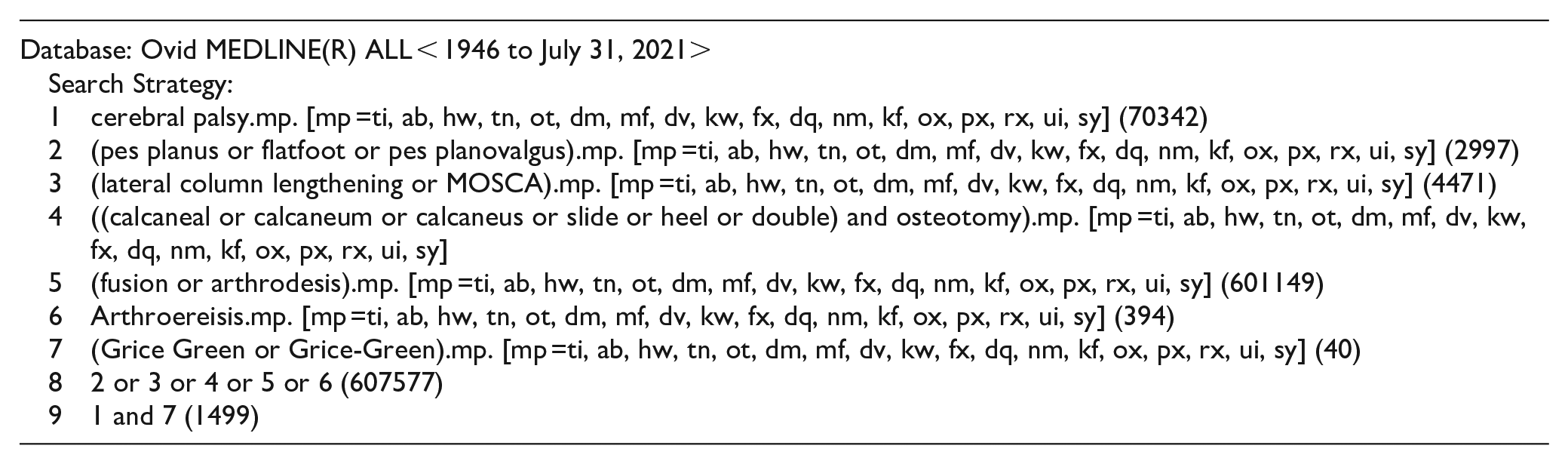
| Database: Ovid MEDLINE(R) ALL < 1946 to July 31, 2021> Search Strategy: 1 cerebral palsy.mp. [mp =ti, ab, hw, tn, ot, dm, mf, dv, kw, fx, dq, nm, kf, ox, px, rx, ui, sy] (70342) 2 (pes planus or flatfoot or pes planovalgus).mp. [mp =ti, ab, hw, tn, ot, dm, mf, dv, kw, fx, dq, nm, kf, ox, px, rx, ui, sy] (2997) 3 (lateral column lengthening or MOSCA).mp. [mp =ti, ab, hw, tn, ot, dm, mf, dv, kw, fx, dq, nm, kf, ox, px, rx, ui, sy] (4471) 4 ((calcaneal or calcaneum or calcaneus or slide or heel or double) and osteotomy).mp. [mp =ti, ab, hw, tn, ot, dm, mf, dv, kw, fx, dq, nm, kf, ox, px, rx, ui, sy] 5 (fusion or arthrodesis).mp. [mp =ti, ab, hw, tn, ot, dm, mf, dv, kw, fx, dq, nm, kf, ox, px, rx, ui, sy] (601149) 6 Arthroereisis.mp. [mp =ti, ab, hw, tn, ot, dm, mf, dv, kw, fx, dq, nm, kf, ox, px, rx, ui, sy] (394) 7 (Grice Green or Grice-Green).mp. [mp =ti, ab, hw, tn, ot, dm, mf, dv, kw, fx, dq, nm, kf, ox, px, rx, ui, sy] (40) 8 2 or 3 or 4 or 5 or 6 (607577) 9 1 and 7 (1499) |
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Compliance with ethical standards
The authors have no conflicts of interest to declare that are relevant to the content of this article. Ethical approval was not required.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The open access fee was supported by Lavender Medical ltd and Ames Medical, and this funding was secured after the completion of the study.