
Abstract
Purpose:
The aim of this study was to evaluate the long-term outcomes of the bone transport technique in the management of post-infectious segmental femoral bone defects in children in a low-income country.
Methods:
Eleven children were included in this case series. All had a femoral defect secondary to osteomyelitis managed with the internal bone transport technique using an external fixator alone. Bone and functional results were evaluated and complications recorded after a minimum follow-up period of 10 years (range: 10–16).
Results:
The mean age of the patients was 7.8 years, and the average size of the bone defect was 10.8 cm. At the latest follow-up, bone results were excellent in three, good in five, and fair in three, while the functional results were excellent in three, good in four, fair in three, and poor in one. Limb length discrepancy was observed in 10 cases while hip and/or knee joint disorder was recorded in six cases. At the last follow-up, only one patient had a recurrence of infection.
Conclusion:
The bone transport technique has proven to be a valid option for eradicating infection and filling large bone defects in children. However, it is a technically difficult and lengthy procedure that is prone to unique complications.
Level of Evidence:
IV-Case series
Keywords
Introduction
Segmental bone defects represent one of the most challenging complications of pediatric osteomyelitis.1,2 In low-income countries, such bone defects typically develop as a sequela of mismanaged or undertreated acute bone infections.3,4 The systemic upset resulting from osteoarticular infections such as fevers, pain, and myalgia may be falsely attributed to malaria or infection at alternate sites. Moreover, local practitioners or child caretakers may ineffectively self-manage with over-the-counter antibiotics. As a result, there is significant delay in presentation to healthcare facilities in order to seek treatment. Infection in the bone is often only revealed by the swelling or bursting of an abscess. 3
The severe clinical and radiologic features (Figures 1(a), 2(a) and 3(a)) of osteomyelitis in cases of delayed presentation to our facility often require complex surgery, ranging from partial to full diaphysectomy. The management of the large bone defects that inevitably follow these surgeries is technically difficult, time-consuming, and costly. The most appropriate management depends on several patient factors, such as the size and site of the defect, the status of the soft tissues, the child’s age, and their family’s socioeconomic status. In resource-limited settings specifically, two important factors to consider are the surgeons’ skill and the facility in which they operate.5,6
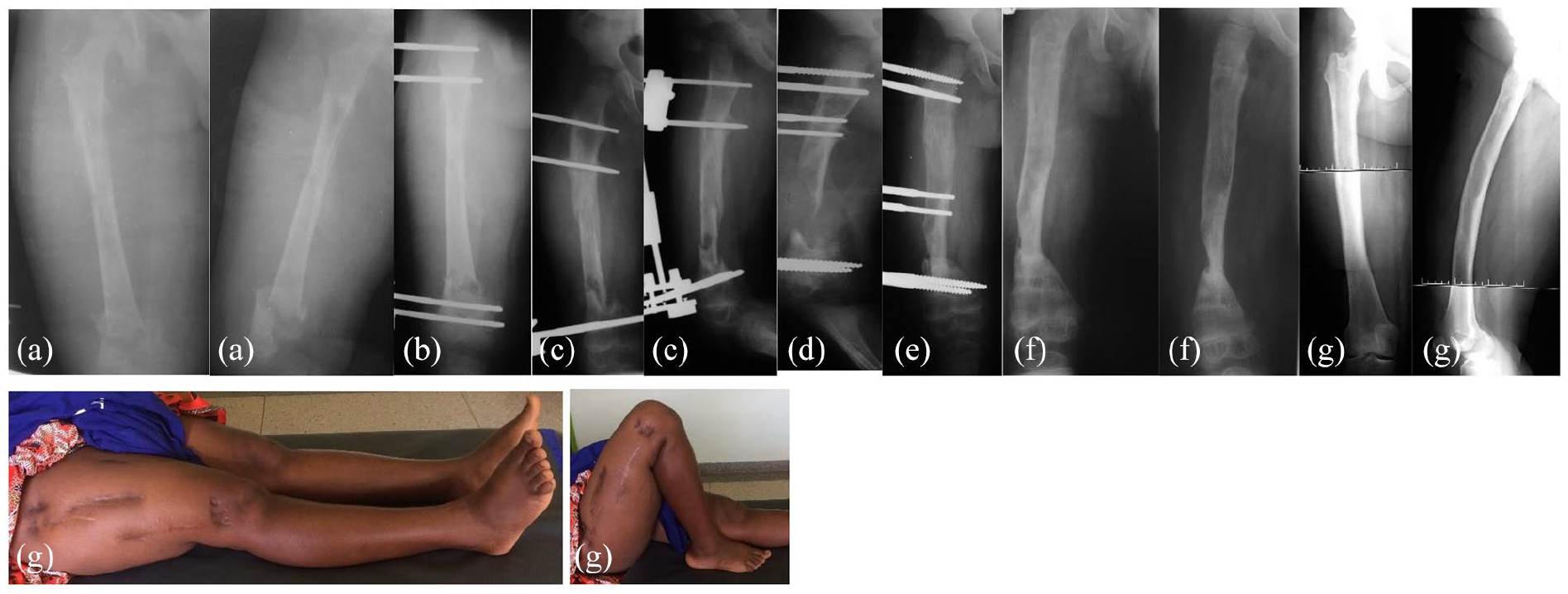
Radiographic sequence of case 1. (a) Radiograph at presentation showing sequestration of the femoral diaphysis, with pathological fracture and enlarged shadow of the soft tissues, mirroring a concurrent severe pyomyositis (600 ml of pus were drained). (b) External fixator was applied to allow proper demarcation of the sequestrum and to restore child mobility. (c) Seven months later, the diaphysis showing restoration in the proximal third, with healing of the fracture, and clear demarcation of the sequestered fragment. (d) Radiograph following sequestrectomy, proximal osteotomy, and application of Orthofix pediatric rail. (e) Five months later, after completion of transport and limb lengthening. (f) Radiographic control taken 2 months after removal of the fixator, showing good axis and sound union at the docking point. The little girl was lost to follow-up at this stage. (g) Clinical and radiographic pictures taken 16 years later showing an excellent bone and functional results.
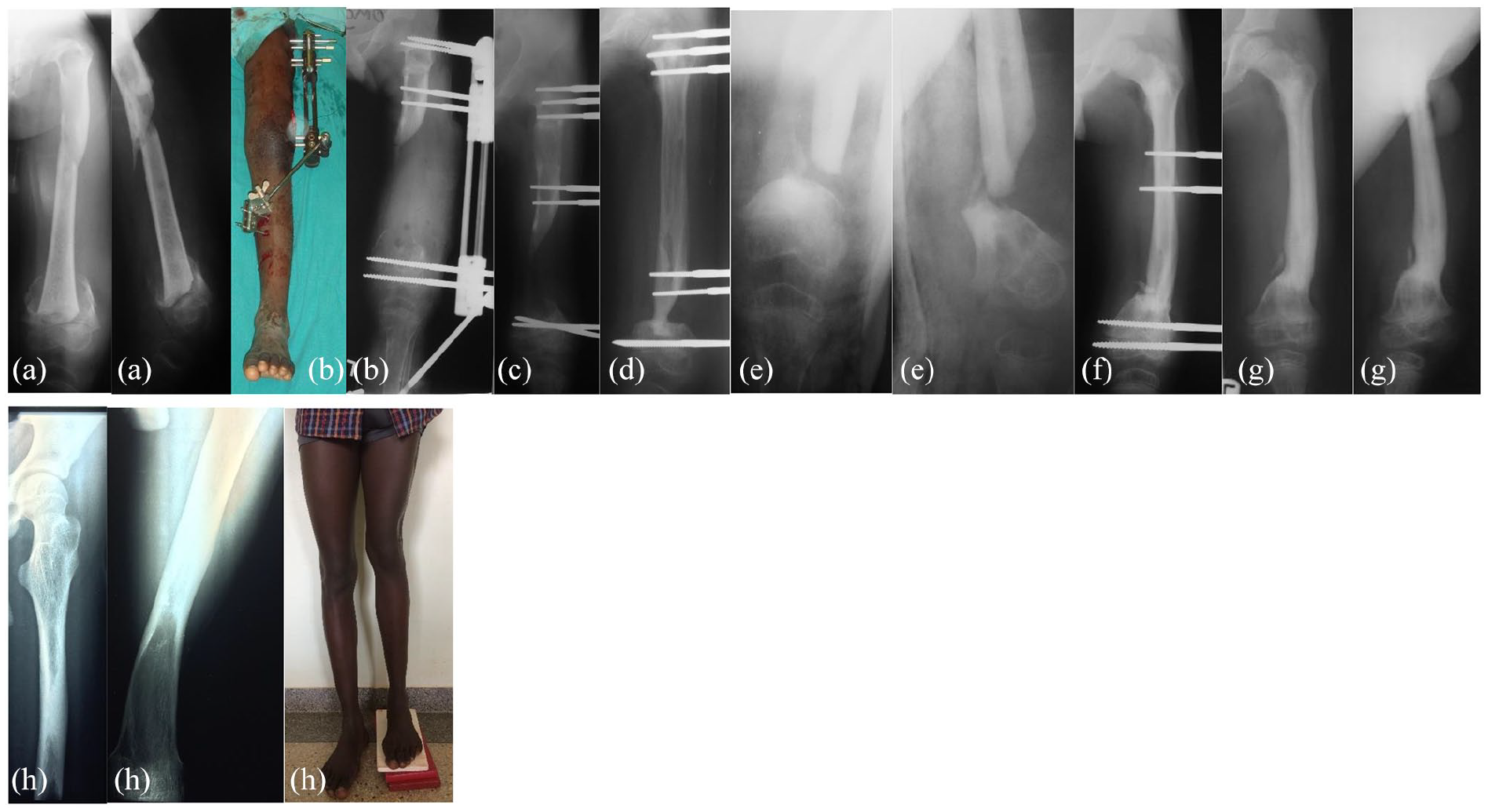
Radiographic sequence of case 4. (a) Radiographs taken at presentation, with sequestrum clearly demarcated and pathological fracture, without surrounding involucrum. Varus deformity of the femoral neck is observed, result of an early pan-diaphysitis partially healed. (b) Radiograph following sequestrectomy, proximal osteotomy, and implant of pediatric rail. To note the fixator extension to the tibia in order to correct a knee flexion contracture. (c) Two months from the index procedure, after screws replacement. (d) Seven and half months from the index procedure, showing a good femoral axis and a docking point lacking congruency and sufficient contact area. (e) Four months later, the child presented with a septic non-union at the docking point, with a bone fragment looking sequestered. A huge thigh abscess was also present. (f) Site debridement and external fixation were used. (g) Seven months after this last procedure, with sound union was achieved, an additional surgery was done to remove a medially located sequestrum embedded in the soft tissues. The boy was lost to the follow-up at this stage. (h) Clinical and radiographic controls 13 years from presentation, showing a slight valgus deformity of the knee and a limb length discrepancy of 5 cm. Excellent functional results, despite the discrepancy.
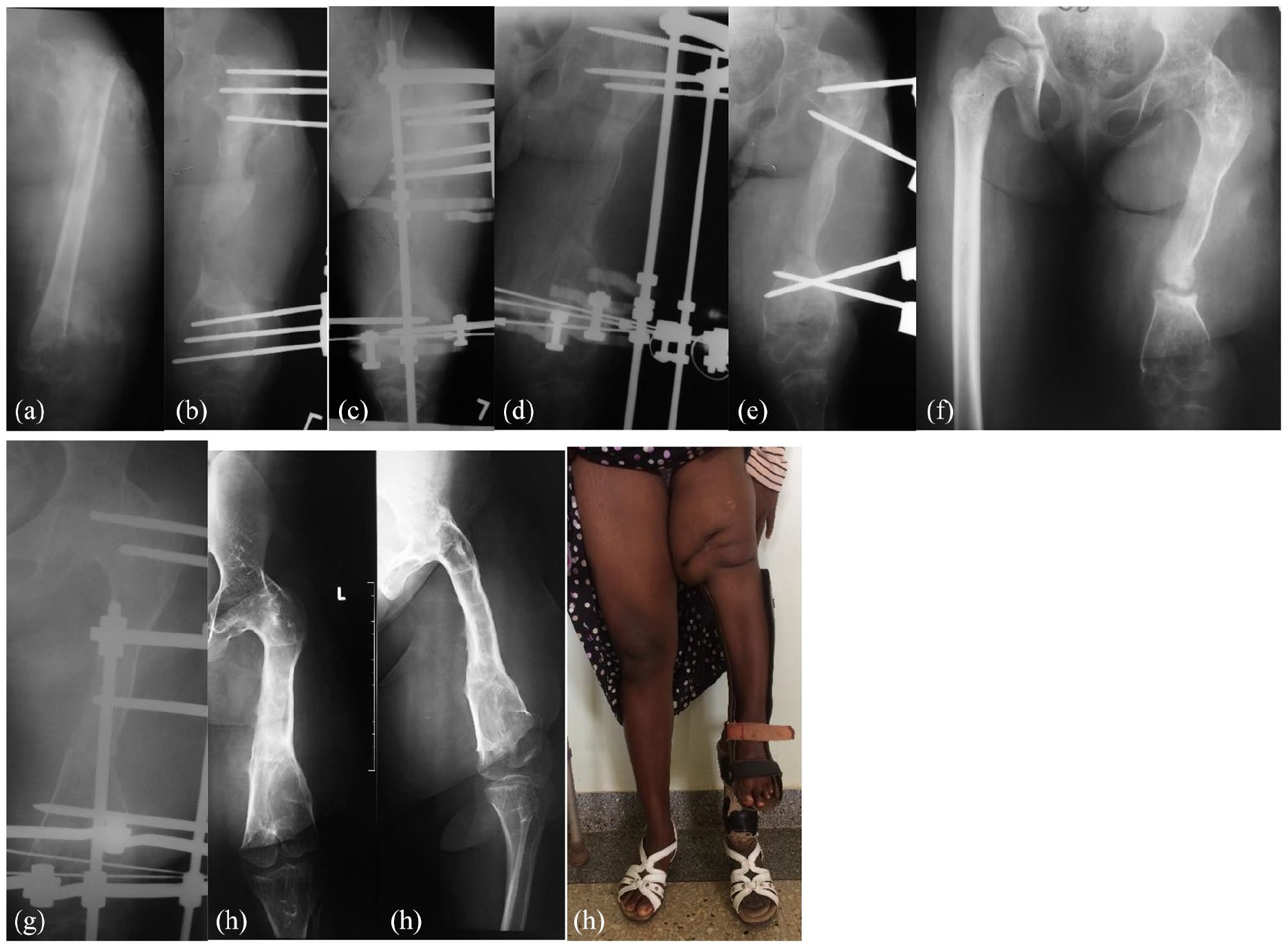
Radiographic sequence of case 2. (a) Radiograph at presentation, showing sequestration of the entire diaphysis, septic arthritis of both hip and knee joints, and inadequate involucrum formation. Apparently, the infection started 8 months prior to admission. (b) Radiograph showing stabilization of the femur after extensive debridement and sequestrectomy. External fixator was applied to see if a better involucrum would form. (c) Two months later, a ring fixator was applied and a proximal osteotomy performed. (d) Despite removal of the transport ring and compression, non-union at the docking point was observed 8 months after distraction started. (e) Persistence of non-union despite fixator change. (f) Five years later, the girl presented with non-union and significant leg discrepancy. Site re-freshening and a new implant of external fixator led to sound union of the docking point. (g) Clinical and radiographic control 15 years from the presentation. (h) Severe limb shortening is seen, with fusion of the hip joint and ankylosis of the knee. A poor functional result was obtained.
There are limited techniques available to bridge femoral defects in children, particularly those exceeding 5 cm in length. Conventional bone grafting has been used, especially to fill small defects, while vascularized fibula flap (VFF) and distraction osteogenesis represent valid options for larger defects.2,7–10
Distraction osteogenesis, a term coined by Ilizarov, 11 has been extensively used in reconstructive surgery. Through the assembly and adjustments of an adequate frame, it can address the bone defects resulting from infection, trauma, and tumors as well as the associated limb length discrepancies (LLD), joint contractures, and angular deformities.1,2,12,13 The bone transport procedure (BT) is the application of Ilizarov’s method in filling intercalary defects of different etiology through the transport of a bone segment across the gap while new bone forms at the trailing end.1,2,12,13
Research is sparse on post-osteomyelitis femoral reconstruction using bone transport in the pediatric age group.7,8 To our knowledge, no literature to date reports on the topic within low-income countries or sub-Saharan Africa. Systematic reviews have shown distraction osteogenesis to be a good choice for treatment of infected non-unions 14 and long bone defects of the lower limbs. 15 However, these reviews only included adult cases and were not based in low-income settings. In addition, heterogeneous etiologies of bone defects were included, such as tumors, trauma, and infection. This case series was undertaken in order to evaluate the long-term outcomes of post-osteomyelitis bone transport in a pediatric group over a minimum follow-up period of 10 years.
Materials and method
Pediatric surgical records were screened including all bone transport procedures performed between 2004 and 2010 by two orthopedic consultants (Antonio Loro and Fulvio Franceschi), one of whom had been trained on Ilizarov fixation. Only those bone transports performed for post-osteomyelitis femoral defects were included; post-traumatic or post-surgical bone transports were excluded in order to keep the diagnostic group homogeneous. Operations occurred across two hospitals in Uganda: Children’s Orthopaedic Rehabilitation Unit (CORU) Mengo Hospital from 2004 to 2009 and Comprehensive Rehabilitation Services in Uganda (CoRSU) Hospital from 2009 onward.
Fifteen cases of bone transport for femoral bone defects in children were found and eleven of these included. Four cases were excluded due to loss of follow-up: two cases due to civil unrest in the country of origin and two cases were not contactable due to outdated details.
Clinical notes, radiographs, and operation notes were reviewed and data collected regarding the demographics, operation characteristics, and post-operative difficulties. As suggested by Paley, 16 difficulties were subdivided into problems, obstacles, and complications. A problem is a difficulty which is resolved by non-operative means, while an obstacle requires further surgical input. A complication is a difficulty which remains unresolved at the end of the treatment and is further subdivided into minor (nuisance problems that leave no significant residua on the patient) or major (more serious problems). 16 All cases were contacted and assessed by our study team in the second half of 2020. At this visit, the bone health and functional outcomes were assessed according to the criteria proposed by Paley and Maar. 17 According to these criteria, bone results are based on bone union, infection relapse, limb deformity, LLD and cross-sectional area of union of the regenerated bone and docking site. Functional results are assessed based on pain, need for walking aids or braces, hip/knee deformity or contracture, loss or ROM when compared with pre-operative range and ability to return to activities of daily living or work. 17 Where possible, patients were interviewed by a social worker to evaluate personal, financial, and social outcomes of both the infection and the procedure.
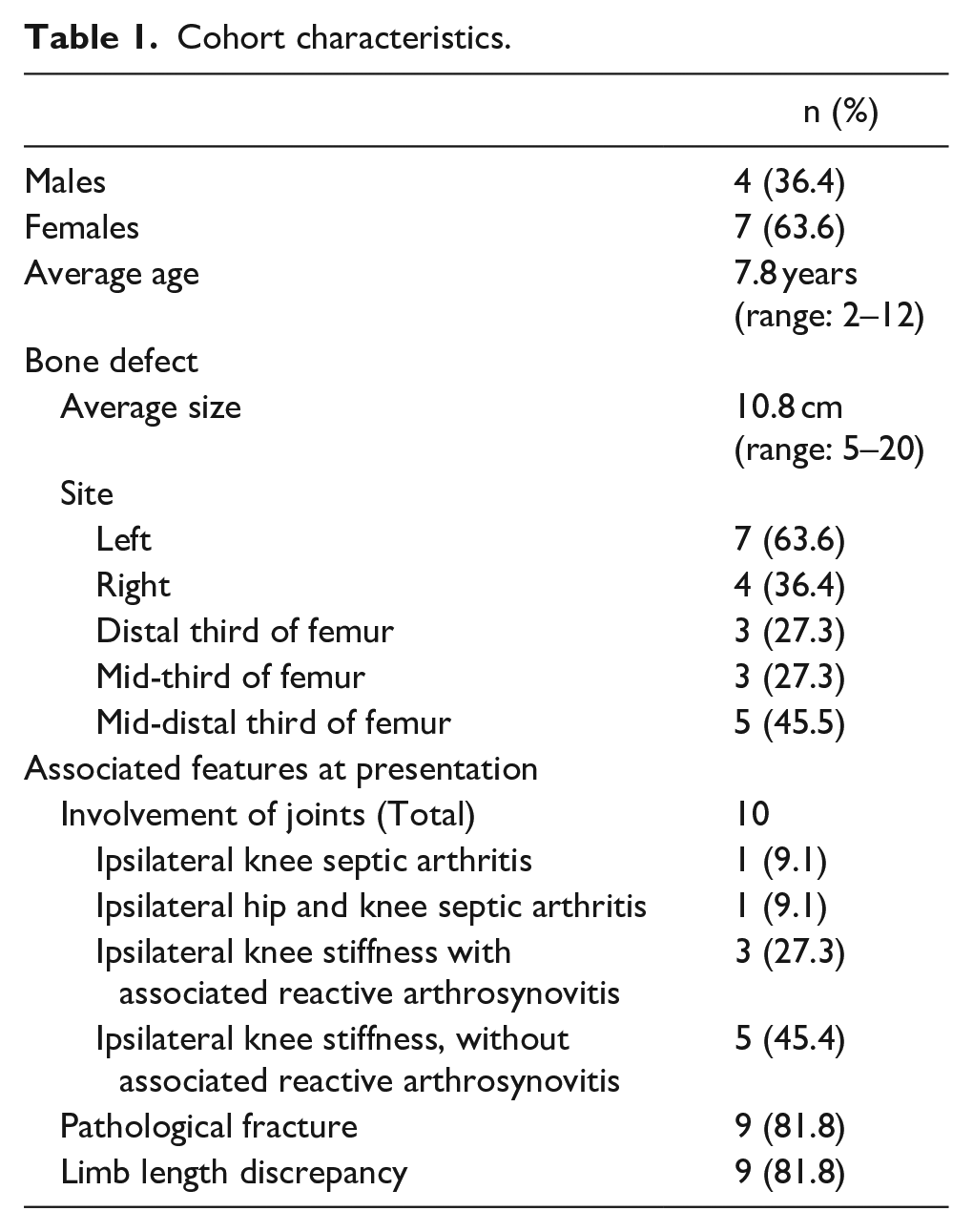
Patient characteristics
Patient characteristics and associated features at presentation are outlined in Table 1. All cases had open growth plates at presentation. All cases (n = 11) presented with active infection, of which the onset was reported between 4 and 11 months prior. Prior to referral to our facility, all cases received empirical antibiotics. Previous surgical procedures were also reported, including incision and drainage of thigh abscesses and incomplete debridement, although documentation provided was very poor.
Cohort characteristics.
A total of 64 operations were performed, with each child undergoing an average of 6 (see supplemental file). Initially, 20 operations were performed in order to optimize patients prior to bone transport. The 11 bone transport procedures were performed at an average of 6 months from initial presentation to our facility (range: 1–16 months). The external fixator stayed in situ for an average of 290 days (range: 150–550 days). Thirty-three additional operations were carried out to manage post-operative obstacles or complications; three cases had no need for further surgeries after the bone transport procedure.
Management protocol
The management protocol was dictated by the clinical and radiological features at presentation, involving either a one- or two-stage approach. A one-stage protocol was adopted in three cases; this involved radical debridement, implant assembly, and osteotomy in the same surgical session, as exemplified in Figure 2. 18 A two-stage protocol was followed in the remaining eight cases, 19 exemplified by the case in Figure 1. The first stage involves a preliminary debridement prior to reconstruction. In the presence of incomplete demarcation of the sequestrum, the affected bone was stabilized with external fixation in order to bide time for proper demarcation and/or resizing of the sequestered fragment, or for a better involucrum formation (Figure 1(b)). Radical debridement, implant assembly, and osteotomy were then performed after 2–3 months of observation.
The construct and the osteotomy were done concurrently in all except one case. The osteotomy was done according to the De Bastiani method 20 under direct vision and was assessed for completeness intraoperatively.
Hybrid ring fixators were used in five cases while monolateral fixators were used in the remaining patients. The ring fixator was chosen in cases where the residual distal bone segment was short and osteoporotic, or when joint contractures were present. Half-rings with Schanz half-pins were used in the proximal femur. All half-pins and wires were inserted without fluoroscopy. External fixators were removed based on two radiological findings: bony union at the docking site and consolidation of the regenerate in at least three cortices out of four. Fixators and pins were removed in a single setting.
An additional ring or clamp was positioned in the upper third of the tibia to correct a concurrent knee flexion contracture (Figure 2(b)) in two cases, since the correction was not achievable by physiotherapy alone, and to stabilize a fracture of the upper tibial metaphysis in one. All cases were treated with a single-level transport. In three cases, the technique of compression-distraction was adopted. This technique includes debridement of the defect, followed by acute compression of the bone ends; the contact may be obtained in full or in part. The external fixator has two aims: to facilitate compression and union of the debrided site, and to lengthen the bone through a metaphyseal osteotomy, performed distally or proximally to the site.
Distraction started after a latency period of 5–7 days at a rate of 1 mm/day in a single step. The direction of the transport was proximal-to-distal in all cases but one, according to the amount of distal bone available. The limb was lengthened as much as allowed by the pain, the onset of joint contracture and radiographic findings on the quality of the regenerate. Intramedullary guide wire was not utilized in our series.
Post-operative care
Radiographs were taken on days 1 and 15 after the index surgery to monitor the opening of the osteotomy site. Radiographic monitoring was taken every 4 weeks thereafter where possible.
Weight-bearing was allowed as tolerated alongside the procedures. Daily physiotherapy was started 2 or 3 days post-operatively, and early mobilization was strongly encouraged. All cases were monitored in a rehabilitation center until completion of the transport.
Results
Outcomes
Cases were followed up for an average of 12.2 years (range: 10–16 years). At the final review, all 11 femora were soundly united radiologically. The bone and functional outcomes were graded according to the criteria set by Paley and Maar, 17 as shown in Table 2.
Long-term bone and functional outcomes, at least 10 years after bone transport procedure, as per criteria by Paley and Maar. 17
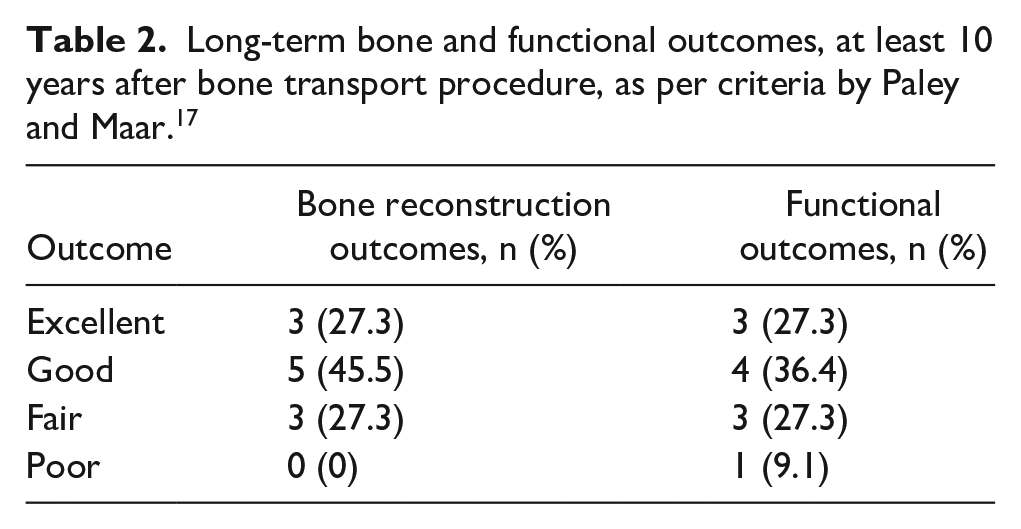
Cases that were unable to achieve excellent outcomes were primarily limited by limb angulation and joint range of motion. Three angular deformities of the distal femur were noted (less than 10 degrees valgus in two cases, a procurvatum and rotational deformity in the third case). Fused knee alone was noted in 1 patient (case 5) and fused hip and knee in another (case 2); both of these cases initially presented with associated septic arthritis. Of the three children who initially presented with a stiff knee and disorder of the ipsilateral hip joint, one fully recovered (case 4), one had severe reduction of knee range of motion and a coxa profunda (case 3), and the third developed a flexion and extension gap of the knee joint but had a full recovery of the hip disorder (case 11). Out of the five cases with an isolated stiff knee at presentation but without associated arthritis, three had significant and one moderate improvement in the range of motion, while no difference was recorded in the remaining one. Due to poor follow-up of the aforementioned cases in this paragraph, timing and other factors that might have influenced the improvement or worsening of the original disorders are not known and could therefore not be further analyzed.
At the last follow-up, LLD was recorded in 10 cases. Eight patients had a difference ranging from 2 to 6 cm, one had a 9 cm difference, and the remaining one had a 25 cm discrepancy. The latter case required an orthoprosthesis and stick to mobilize (Figure 3(f)). Occasional discomfort and pain were reported by nine patients, mainly when walking for prolonged periods. No cases opted to use a shoe lift and none required regular analgesia.
Social worker interview was performed in 9 out of 11 patients at the 10-year follow-up. At this visit, seven were full-time students, two were full-time mothers, and two were full-time employees. All cases emphasized that they experienced social stigma due to the frame but none required removal. All children were able to attend school at the completion of treatment. The entire process was financially draining for all cases.
Problems, obstacles, and complications
A total of 40 difficulties were observed, as outlined in Table 3: 5 problems, 10 obstacles, and 25 true complications. No major intraoperative difficulties were recorded.
Problems, obstacles, and complications during and after the completion of bone transport process, as per criteria by Paley. 16
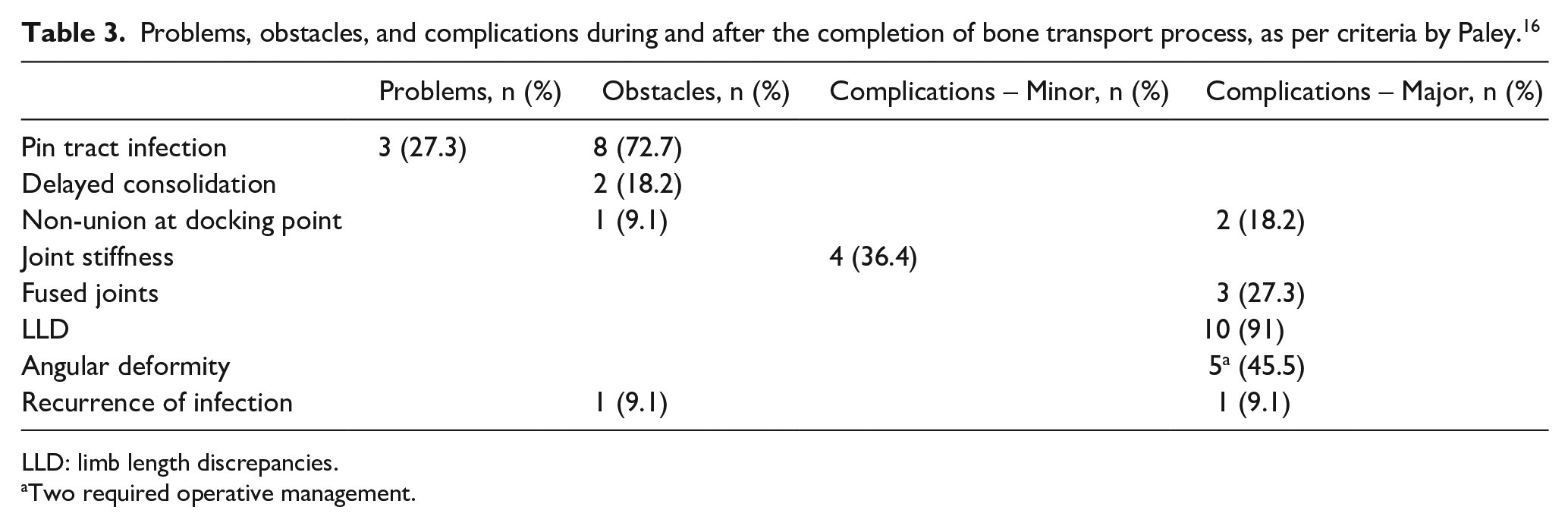
LLD: limb length discrepancies.
Two required operative management.
Pin tract infection was the commonest post-operative difficulty (n = 11), and conservative management was successful in three cases. The remaining eight cases required operative treatment: six cases required wires and half-pin extraction and replacement, one case required wire replacement in association with sequestrectomy, and one case required a debridement to remove a sequestrum in the soft tissues (Figure 2(g)).
Two cases of delayed consolidation of the regenerate were observed. Initially, both cases were on treatment with a rail and after docking, a slow maturation of the regenerate was observed on plain radiographs. The rail was replaced by a monolateral fixator with newly placed screws spanning over the docking site, giving more stability. Sound consolidation was then obtained in both cases.
Three cases developed non-union at the docking point. The first case (case 5) occurred at the end of the bone transport process and was addressed surgically. A fibula graft was placed in the site after re-freshening. This did not integrate and the ring fixator had to be kept in place for 11 months. The site was further protected with a long leg cast for almost 5 months after fixator removal, and union was eventually achieved. In the following 3 years, the same child required two osteotomies to correct knee angular deformities and limb shortening. In the second case (case 2), a non-union at the docking point occurred a few days after fixator removal. At this point, the child was unfortunately lost to follow-up for 5 years for unknown reasons. Successful union was eventually achieved 11 months after site re-freshening and implantation of a ring fixator. The third case (case 4) experienced a septic non-union 4 months after fixator removal (Figure 2(e)). Debridement and external fixation were performed, and union was achieved in 3 months.
Recurrence of the infection was observed in two cases. In the first case, the infection resolved after further debridement. In the second case, two additional operations of debridement and sequestrectomy were performed; however, an intermittent sinus remained present at 10-year follow-up.
Two children underwent successful surgical correction for angular deformities, between 3 and 3½ years after fixator removal.
Discussion
Post-osteomyelitis femoral defects in children are challenging for the treating physicians, particularly when exceeding 5 cm and combined with LLD, joint disorders, or angular deformities. The difficulties in management are augmented in low-income countries in which adequate facilities and surgical skills are few in number and difficult to access both logistically and economically.4,21 We opted for BT as it may address all of the clinical requirements of complex cases. The improvements in clinical and radiological features within our series show excellent BT results in the long term, achieving sound bone reconstruction, resolution of infection, and functional improvement of joints that initially appeared unsalvageable.
As in other similar series, functional results in our study are slightly poorer than bone results.7,22,23 Function is only partly dependent on the bone’s status and is affected by the damage inflicted to surrounding soft tissues by the infection and by the surgical procedures. In our series, sequelae of previous surgical treatments or mismanagement likely increased the difficulty in restoring limb function.
The long procedure time is one of the major disadvantages of the bone transport technique. To minimize procedure time, we used compression-distraction in three cases. To reduce the fixator time and associated costs, double-level transport and transport over an intramedullary (IM) nail have been suggested.8,24 The small size of the residual bone segments in children restricts the adequate placement of pins required for double-level transport. IM nailing was not utilized in our setting to avoid recurrence of infection by using hardware in previously infected sites.
Difficulties are frequent and intrinsic to the technique; additional surgeries are likely needed to manage them.1,12,22,23 Children were admitted to our rehabilitation center until procedure completion so that staff could swiftly identify and manage these difficulties. As in other series, the commonest difficulty related to the distraction process was pin tract infection, considered an inevitable complication of external fixation by some authors.8,22,23,25
This series involved three cases of non-union at the docking site requiring further complex management. According to Ilizarov, 11 primary union can be achieved by prolonged compression in a stable frame and in children this may be obtained without grafting of the site. As in Zhang et al.’s 8 and Barbarossa et al.’s 23 series, pre-grafting of the docking site was not performed in our cases but may have lowered the risk of non-union. Delayed consolidation of the regenerate is a further complication as observed in two of our cases.22,23 Ilizarov 11 recommends a stable frame, a low energy osteotomy, proper latency time before distraction, and correct distraction rhythm-rate to minimize this risk. Poor bone quality in our cases, mostly osteoporotic, often made it challenging to obtain sound stabilization. A rate of 1 mm/day in a single daily adjustment was used in our cohort in attempt to increase compliance. It was primarily the case’s parents trained to perform the adjustment and they were not reliably able to adhere to more than one daily procedure.
Involvement of the adjacent joints is not uncommon in long-standing infections (Figure 3(a)). Temporary or permanent reduction of joint motion may be the inevitable sequela of the disease itself or may complicate the procedure. In presence of knee joint contracture, without radiological features suggestive of established arthritis, an extension of the frame to the upper third of the leg can lead to gradual extension of the joint (Figure 2(a)). The child is thus able to bear weight during the long treatment process, lowering the risk of muscular atrophy, osteoporosis, and loss of joint motion. Standing and walking exercises with involvement of the physiotherapists were started as early as possible. However, fusion of the joints and bone growth disturbances may be inevitable and the end results independent from the bone transport procedure itself.
Equalization of LLD was achieved by transport or lengthening in most of our patients after the index procedure. However, due to damaged growth plates, further limb discrepancy developed during the remaining growth period. In some cases, overcorrection was obtained to compensate for the expected reduced growth of the affected limb. All cases declined femoral lengthening when offered, as this was not seen as a priority.
Alternative techniques to BT are available for managing post-osteomyelitis femoral defects in children, each associated with specific complications and barriers in low-income countries. Spontaneous regeneration of the femoral diaphysis has been reported in young children in which the periosteal membrane is preserved,26,27 but this has never been observed in extensive femoral gaps within our institution. Conventional bone grafting may be used to bridge small defects using iliac crest, proximal tibia, or fibula strut as sources.9,28,29 However, filling large defects requires long immobilization and significant bone harvesting which may not be possible in young children. In addition, bone resorption and graft fracture pose serious complications of this procedure. VFF requires expertise in microsurgery and technical equipment, both sparse in low-income countries. 10 The graft needs prolonged immobilization with an external fixator or hip spica, and hypertrophy of the graft usually requires several months. It is further complicated by the mismatch between fibula and femur size increasing with age. Neither VFF nor conventional bone grafting can address associated limb deformities or leg length discrepancies.
In very complex cases within failing health facilities, amputation might be indicated. Amputation remains a very delicate issue in this cultural context and is not widely accepted by the population. 30 The very mention of amputation can lead to patients requesting discharge from a center. Furthermore, there are very few prosthetic workshops in East Africa that can provide quality artificial limbs. Regular prosthetic adjustments and their associated travel requirements are a financially draining commitment until a child’s growth ceases. The ortho-plastic team in our center is fortunately able to carry out challenging and costly reconstruction procedures, even in catastrophic cases, and so amputation was never advised to any of our patients.
The financial implications of the BT procedure become most relevant when it is considered that osteomyelitis has higher incidence and more severe complications in children from low-income countries. 14 Procedures in our institution were heavily subsidized by the hospital and outside sponsors. The majority of Ugandan families would have unlikely been able to afford these costly procedures without such financial sponsorship; the 2020 gross domestic product per capita in Uganda was US$822. 31 It is important to note that in our center, no child was excluded, and no bone transport process terminated early due to economic grounds. Our hospital administration, social workers, and clinical psychologists were essential in counseling, evaluating the family’s situation, and looking for outside sponsors.
Follow-up
Follow-up in low-income countries proves difficult due to logistic and financial reasons.21,32 As a result, all cases in this series were admitted to rehabilitation centers connected to our hospital until bone transport and associated rehabilitation processes had been completed. Unfortunately, after discharge, most children were lost to follow-up for a period of years. Once bone reconstruction was achieved and the infection eradicated, out-patient appointments were deemed an unnecessary expense from the families’ perspective. Furthermore, children were referred to our center from all over Uganda and neighboring countries, complicating follow-up arrangements. Contact was further prevented owing to logistical reasons such as lack of postal addresses, telephone, or Internet access. It is likely that complications could have been limited and outcomes improved if follow-up was more strictly adhered to.
Conclusion
Our study has shown that bone transport is a valid procedure for reconstruction of post-osteomyelitis large skeletal defects in children. It displays in both good bone and functional outcomes in the long term, particularly if strict supervision is applied during the process. It is a lengthy and demanding process, prone to complications and associated with a significant financial burden. Prospective studies with larger samples are needed to further evaluate outcomes of this procedure for this specific patient cohort.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521221106389 – Supplemental material for Bone transport in the management of post-osteomyelitis femoral defects in children: A case series with a minimum of 10-year follow-up in Uganda
Supplemental material, sj-pdf-1-cho-10.1177_18632521221106389 for Bone transport in the management of post-osteomyelitis femoral defects in children: A case series with a minimum of 10-year follow-up in Uganda by Antonio Loro, Francesca Loro, Fulvio Franceschi and Niall Brown in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
Special thanks to Mrs Nafuna Sylvia and Miss Nakayiga Catherine, social workers at our hospital, for their wonderful effort in tracking the patients.
Author contributions
Antonio Loro was responsible for idea of the study, its methodology, data gathering, and manuscript writing. Francesca Loro and Niall Brown were responsible for data analysis and writing of the original manuscript. Fulvio Franceschi was responsible for the idea of the study, its methodology, and manuscript editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Surgeries performed at CORU Mengo Hospital were fully sponsored by Christian Blind Mission (CBM) and other charities. Surgeries performed at CoRSU Hospital were only partially sponsored by CBM, with partial contribution from the patient or other sponsors. No funding was received for this project.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.