
Abstract
Background:
Pediatric Lisfranc injuries (PLI) are rare injuries that have few studies published about their occurrence and treatment in pediatric population. Due to this lack of information, the diagnostic criteria and surgical or non-surgical methods for treatment have not been clearly established within the pediatric orthopedic literature. The objective of this study was to review the published literature related to treatment options and develop a concise stepwise treatment algorithm for pediatric patients presenting with Lisfranc injuries.
Methods:
A systematic literature review was conducted using PubMed to find studies discussing the treatment of PLI with reported long-term outcomes. Data collection accounted for the mechanism of injury, diagnostic imaging modality used, injury type, fracture classification using the Myerson system, treatment method used, and postoperative complications.
Results:
An initial PubMed search revealed 290 articles, but only 10 studies fulfilled the criteria for in-depth review. A total of 114 patients were included in this review from the selected case reports and case series studies. Primary treatment methods were as follows: 44% (50/114) with open reduction internal fixation (ORIF) using Kirschner wires (K-wires) and/or screws, 3% (3/114) with closed reduction percutaneous fixation (CRPF), 4% (4/114) with suture-button constructs, 20% (23/114) with cast immobilization, and 29% (33/114) were described as not requiring reduction.
Conclusion:
There were two main limitations to this study. First, there are few published studies with longitudinal outcomes of PLI treatment. Second, some case series did not disclose which procedure a patient with post-treatment complications underwent. Therefore, an overall statistical analysis of success and failure rates with associated complications of each procedure could not be conducted. In conclusion, we found that a stepwise approach to evaluating conservative and surgical treatment options based on the presentation of the PLI should be utilized to optimize long-term outcomes.
Introduction
Pediatric Lisfranc injuries (PLIs) are an uncommon injury of the tarsometatarsal (TMT) joint complex that primarily affects the first and second metatarsals (MTs) and their connection to the medial and middle cuneiforms, but can also have effects across the entirety of the TMT joint. The instability of this joint complex can be attributed to the absence of a stabilizing ligament between the first and second MTs. The mechanism of injury for PLI is commonly caused by axial loading in a plantarflexed foot position due to disruption of the Lisfranc ligament’s connection between the proximal base of the second MT to the medial cuneiform.1–3 Due to the rarity of published literature on this injury in pediatric cases, evidence-based treatment guidelines for PLI are limited. This contrasts with adult Lisfranc injuries, which have standardized treatment protocols and less variability in their management due to the closure of physeal growth plates. This is an important area of concern when considering surgical versus non-surgical options for Salter-Harris type fractures because exposure of the physes or joint surface during operative management may induce premature physeal closure and/or fusion as a result.4,5 Furthermore, the intraarticular nature of PLI increases the risk of developing posttraumatic degenerative arthritic changes in the TMT joint complex. 6 Bone deformities of the midfoot region can develop during remodeling from physeal involvement which can create further complications for the patient.4,5 There are many treatment options with varying outcomes, but there is no consensus on the most optimal management protocol for this injury.1,4,5,7–14 Nonetheless, the majority of studies included in this systematic review have achieved successful postoperative outcomes using surgical intervention to achieve reduction and fixation in treating PLI.4,5,7–14 The purpose of this study is to define standardized diagnostic criteria and novel treatment guidelines based on the classification of injury to pair the best management protocols with optimal long-term outcomes for future patients receiving treatment for PLI.
Materials and methods
Search strategy
A systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) research methods and reporting guidelines. 15 A digital search of the online medical literature database, MEDLINE (PubMed) was done between January 4, 2021 and January 18, 2021. The search strategy included the following keyword terms: “pediatric” or “adolescent” or “child,” and “lisfranc” or “tarsometatarsal.” All potential studies were stored to Zotero, (www.zotero.org), an open-source software program used for bibliographic citation management, to facilitate evaluation of the studies used.
Study selection
The published literature selected for this study involves therapeutic measures for PLI. Studies involving adult-only cases were excluded. Studies that included a mixture of pediatric and adult cases, but that did not distinguish the data extracted from pediatric and adult patients were excluded. Case reports without appropriate postoperative follow up were excluded. Studies involving cadaveric specimens were excluded. Studies published in languages other than English were excluded.
Data extraction
Ten studies met the criteria for an in-depth review. These articles were examined for the number of patients/feet included in the study, diagnostic indicators for PLI including imaging, and physical exam findings, the number of patients undergoing either surgical or non-surgical therapy, instrumentation used (if applicable), and their respective outcomes. Each outcome was taken into consideration when determining the novel treatment guidelines. A PLI was determined resolved if there was complete resolution of pain and restored function of the foot. A PLI was determined to have a failure of resolution if there were post-treatment complications involving either pain, hardware failure (if applicable), or impaired function. Possible biases were considered when extracting data from case series studies and limitations were noted. Some case series studies did not differentiate which treatment option a patient had undergone even if they had a resultant complication. Thus, the sum of complications for each specific treatment option was unable to be obtained from the case series studies.
Results
Search results
There were 290 articles identified via PubMed search. Duplicate articles identified through other sources and articles written in languages other than English were excluded. The remaining total articles were screened based on their titles, leaving a total of 46 full-text articles to be assessed for eligibility using the previously defined criteria. Articles were excluded if they only included studies with adult patients, did not have postoperative follow-up, involved treatments for non-PLI, or included cadaveric studies. This left a total of 10 full text studies4,5,7–14 to be used in qualitative synthesis for this systematic review. Figure 1 details the search and selection process for narrowing the initial 290 searched articles to the 10 full-text studies used in this systematic review.
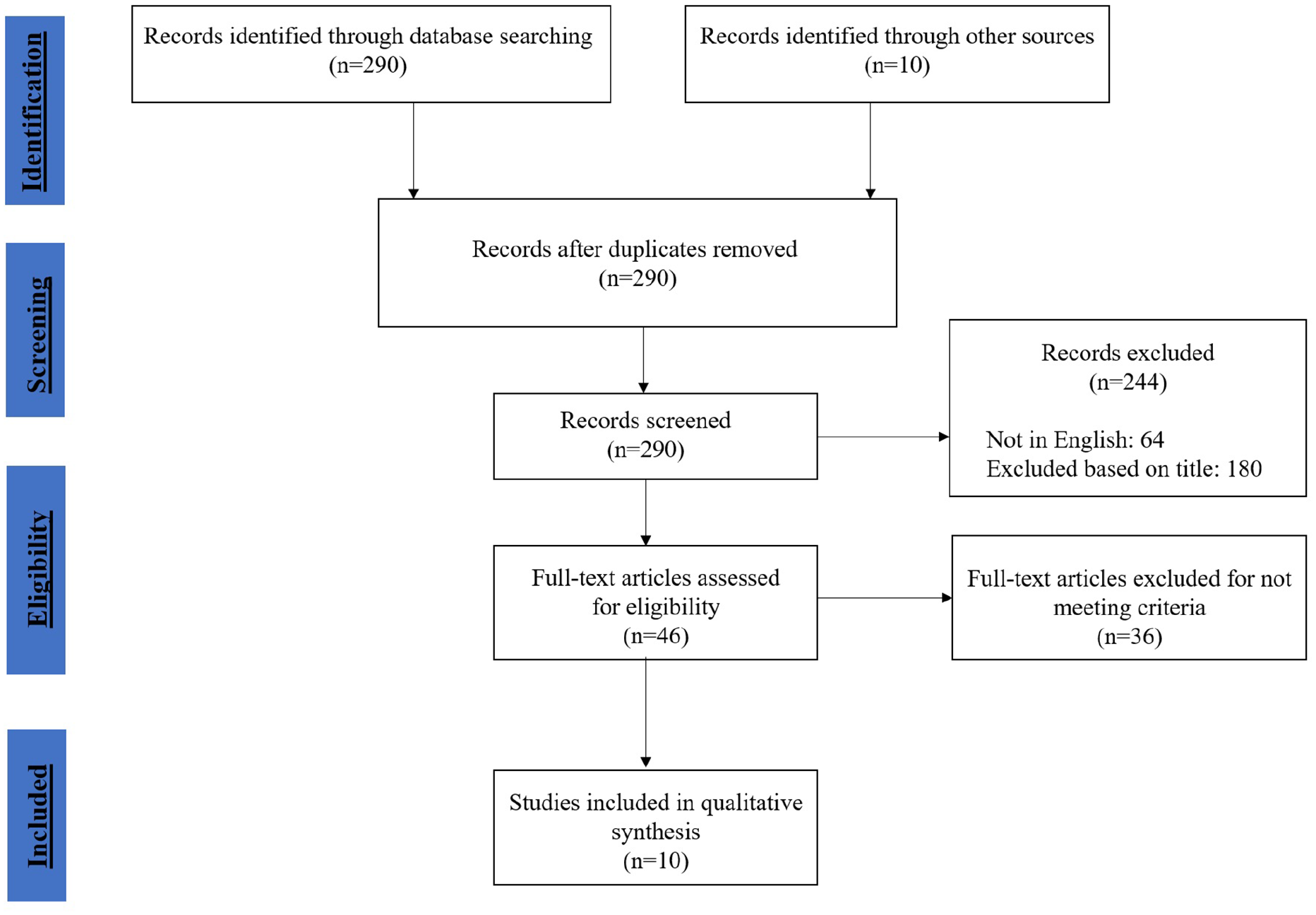
Flow chart of literature search identifying articles screened, assessed, included, and excluded.
Overview of literature
There were 5 feet from case reports and 109 feet from case series studies included that summated to a total amount of “114” feet included in the data from the 10 studies (Table 1). Primary treatment methods were as follows: 44% (50/114) with ORIF with K-wires and/or screws, 3% (3/114) with CRPF, 4% (4/114) with suture-button constructs, 20% (23/114) with cast immobilization, and 29% (33/114) were described as not requiring reduction. A summary of demographics, diagnostic imaging, imaging modality, mechanism of injury, treatment methods, and post-treatment complications are summarized for case reports in Table 1 and case series studies in Table 2 and 3.
Summary of diagnostic tools, therapies performed, and outcomes from single case report studies.
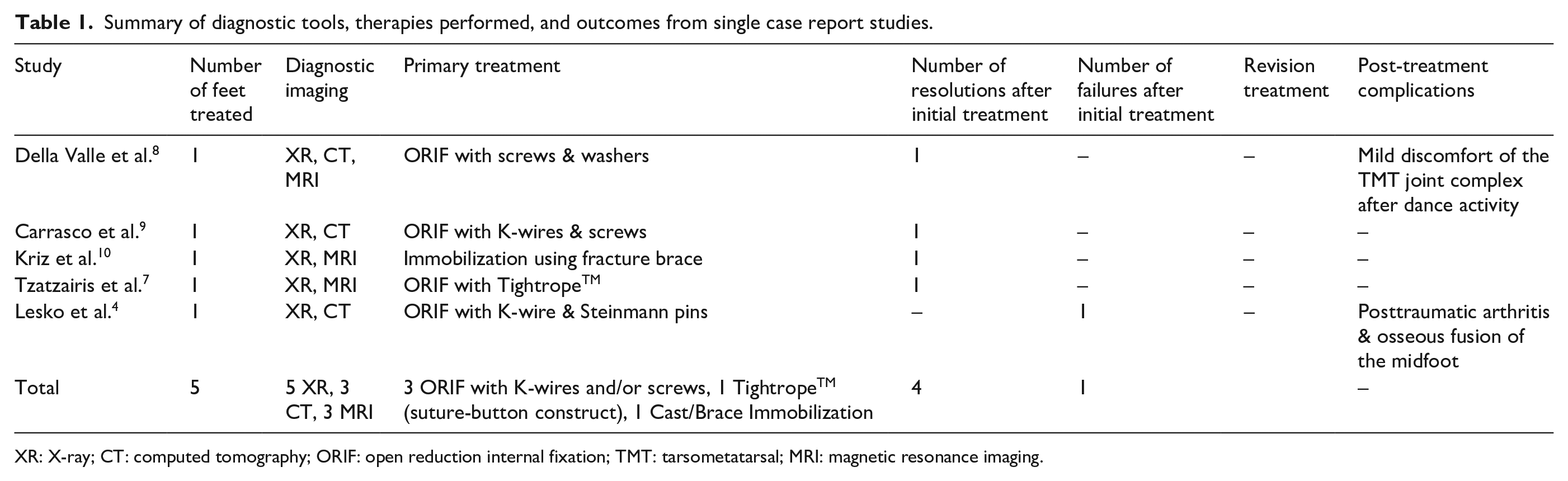
XR: X-ray; CT: computed tomography; ORIF: open reduction internal fixation; TMT: tarsometatarsal; MRI: magnetic resonance imaging.
Summary of diagnostic tools, therapies performed, and outcomes from case series studies.
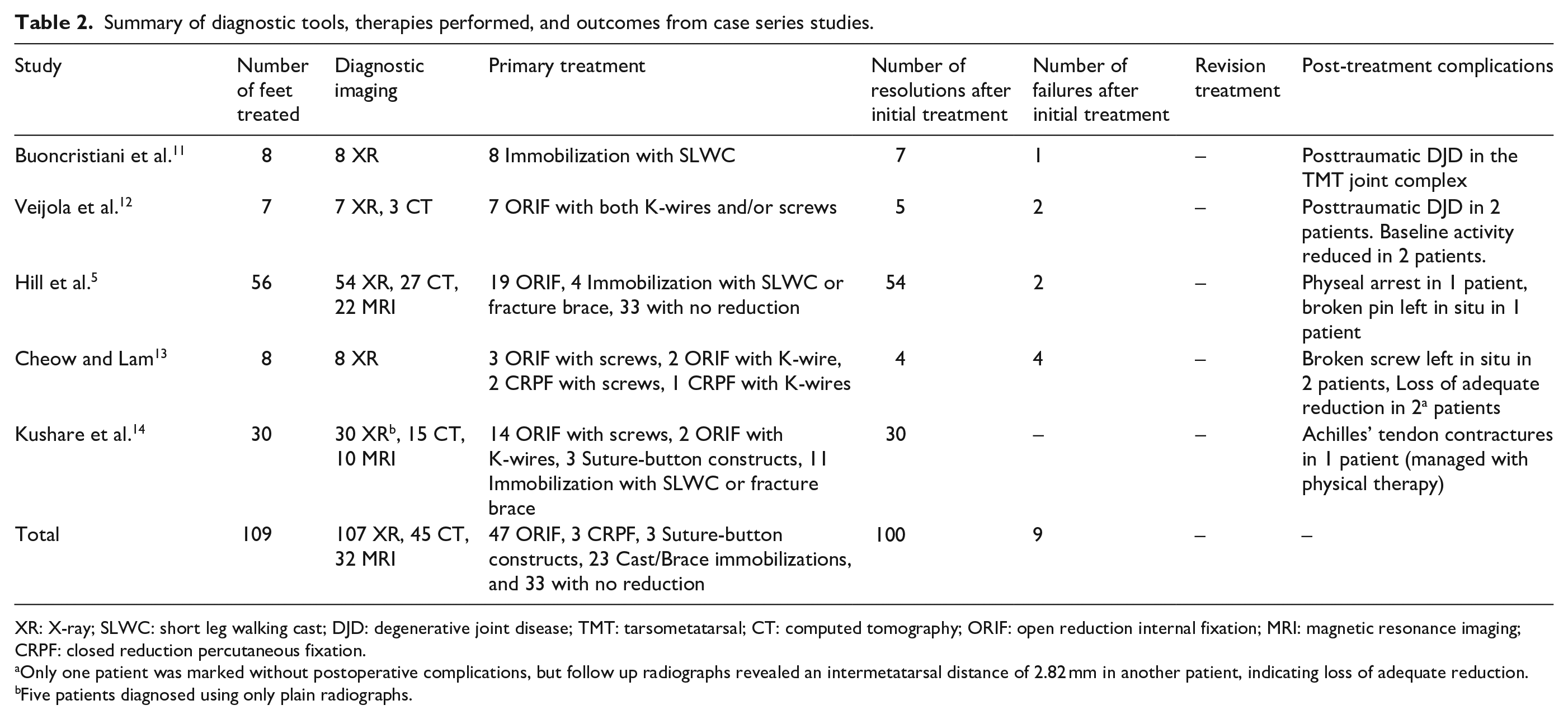
XR: X-ray; SLWC: short leg walking cast; DJD: degenerative joint disease; TMT: tarsometatarsal; CT: computed tomography; ORIF: open reduction internal fixation; MRI: magnetic resonance imaging; CRPF: closed reduction percutaneous fixation.
Only one patient was marked without postoperative complications, but follow up radiographs revealed an intermetatarsal distance of 2.82 mm in another patient, indicating loss of adequate reduction.
Five patients diagnosed using only plain radiographs.
Summary of age, sex, mechanism of injury, and imaging modality used from case series studies.
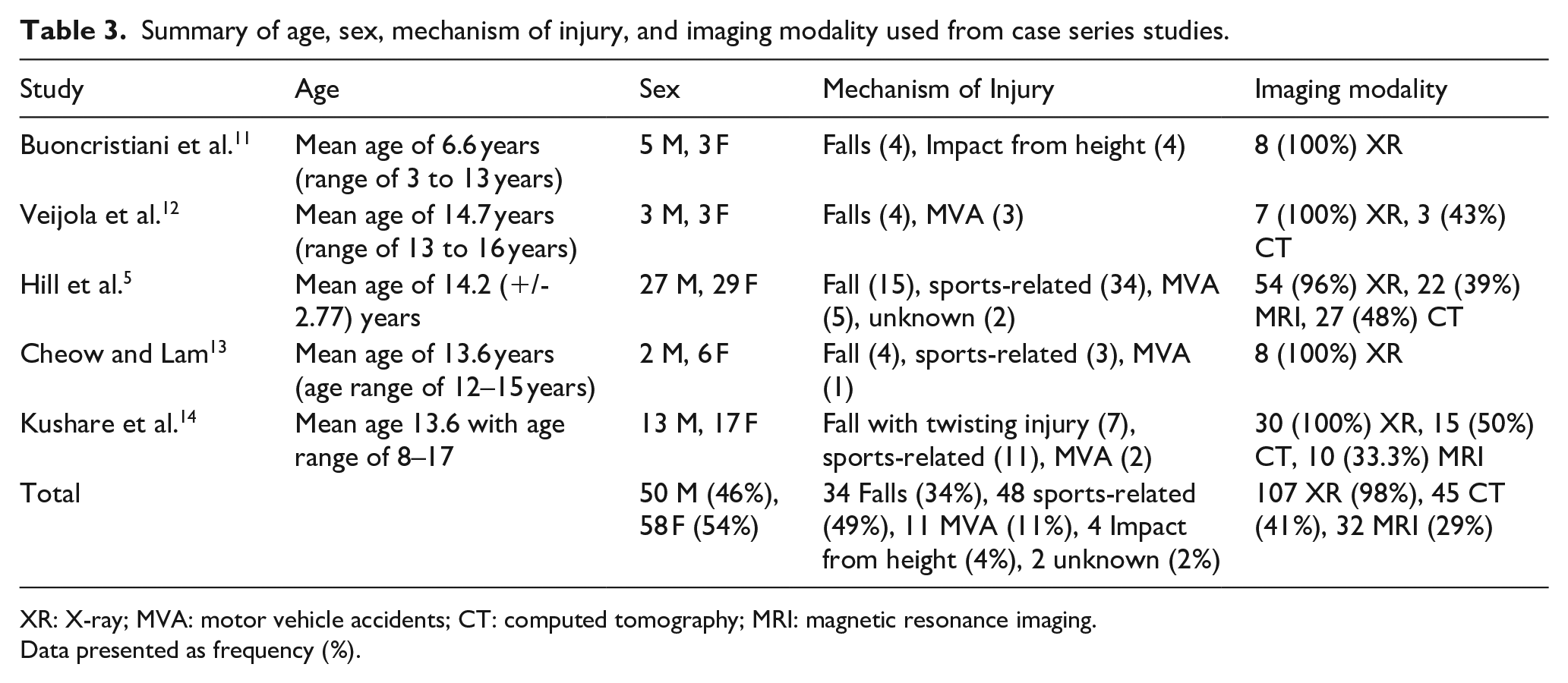
XR: X-ray; MVA: motor vehicle accidents; CT: computed tomography; MRI: magnetic resonance imaging.
Data presented as frequency (%).
Presentation
Buoncristiani et al. 11 conducted a retrospective review of five male and three female patients with a mean age of 6.6 years within an age range of 3 to 13 years old at the time of evaluation. Impact from a height accounted for four Lisfranc injuries and falls accounted for the other four injuries. All patients presented with tenderness over the TMT joint complex and midfoot edema; other symptoms included dorsal and plantar midfoot ecchymosis.
Veijola et al. 12 conducted a retrospective review of three male and three female patients with a mean age of 14.7 years within an age range of 13 to 16 years old at the time of evaluation; note, one patient had bilateral Lisfranc injures, totaling the amount of injured feet to seven. Impact from a height between 3 to 10 meters accounted for four Lisfranc injuries and the other three Lisfranc injuries were from motor vehicle accidents (MVA) involving motorcycles or scooters. Symptomatic presentation included edema, soreness, and erythema of the injured foot.
Hill et al. 5 conducted a retrospective review of 27 male and 29 female patients with an average age of 14.2 (+/- 2.77 years). Sports-related activities accounted for 34 Lisfranc injuries, falls accounted for 15 Lisfranc injuries, MVA accounted for five Lisfranc injuries, and unknown causes accounted for two Lisfranc injuries. Symptomatic presentation was not discussed.
Cheow and Lam 13 conducted a retrospective study of two male and six female patients with a mean age of 13.6 years within an age range of 12 to 15 years old. Impact from a height accounted for four Lisfranc injuries, sports-related activities accounted for three Lisfranc injuries, and MVA accounted for one Lisfranc injury. Symptomatic presentation included tenderness and edema in all injured feet.
Kushare et al. 14 conducted a retrospective study of 13 male and 17 female patients with an average age of 13.6 years within an age range of 8 to 17 years. Sports-related activities accounted for 11 Lisfranc injuries, falls with a twisting injury accounted for seven Lisfranc injuries, and MVA accounted for two Lisfranc injuries. Symptomatic presentation included midfoot edema, tenderness, and plantar ecchymosis.
Evaluation
Imaging
All patients reviewed by Buoncristiani et al. 11 had preoperative and postoperative anteroposterior, lateral, and oblique radiographs taken, but usage of advanced imaging was not discussed.
All patients reviewed by Veijola et al. 12 had radiographs taken which revealed Lisfranc dislocations in all patients. Computed tomography (CT) was utilized in three patients, but without specifying the impetus for doing so. Postoperative reductions in two of these patients were rated as excellent and one patient was rated as good. Evaluation for degenerative changes to the joint complex was only available for one of these three patients, which was recorded as none; postoperative reduction had been graded as excellent in this patient.
Imaging for the 56 patients reviewed by Hill et al. 5 was performed as follows: 54 (96%) patients were evaluated with radiographs, 22 (39%) patients with magnetic resonance imaging (MRIs), and 27 (48%) with CTs. Imaging was also used to evaluate for skeletal maturity to determine if open physes were present in addition to ligamentous and bony Lisfranc injuries. No further discussion was included on the usage of advanced imaging. It was not determined whether the use of MRI or CT were mutually exclusive.
All patients reviewed by Cheow and Lam 13 had preoperative and postoperative radiographs taken, but usage of advanced imaging was not discussed.
Imaging for the 30 patients reviewed by Kushare et al. 14 was performed as follows: 30 (100%) patients were evaluated with radiographs, 15 (50%) patients with CTs, and 10 (33%) patients with MRIs. Plain radiographs were solely used for the diagnosis of 5 (17%) of patients only and advanced imaging was utilized for the remaining 25 (83%) of patients as described. Of the 25 patients requiring advanced imaging, 23 (92%) of them were to confirm Lisfranc injuries due to suspicion evident on radiographs or for further evaluation of the injury, and 2 (8%) of them were required due to negative radiograph readings.
Injury types
Hill et al. 5 organized the Lisfranc injury types for their fracture patients into two categories: Ligamentous (sprains) and osseous (fractures). From the 39 fracture patients reviewed, 11 (28%) cases were reported to have ligamentous injuries and 28 (72%) were reported to have osseous injuries.
The cohort of patients reviewed by Kushare et al. 14 had 22 (73%) fracture (avulsion and dislocation) injury types and 8 (27%) ligamentous (sprain) injury types.
The other case series articles reviewed did not include statistical analyses that differentiated their patients from ligamentous and osseous injury types.
Myerson classification
Hill et al., 5 Cheow and Lam, 13 and Kushare et al. 14 used the Myerson fracture classification to differentiate the Lisfranc injury types; other case series articles reviewed did not differentiate the Lisfranc injury types in their studies. Myerson classification is divided into three types depending on the direction of displacement. 16 Type A is for complete incongruity of the TMT joint complex in the medial or lateral direction. Type B1 is for partial medial incongruity of the first ray in isolation. Type B2 is for partial incongruity of the lateral four metatarsals in any direction of displacement. Type C1 is for divergent displacement of the first metatarsal medially and the lateral four metatarsals in any direction with partial incongruity. Type C2 is for divergent displacement with complete incongruity.
Classification of the 39 fracture patients by Hill et al. 5 revealed statistically significant patterns of association between the skeletal maturity of patients and the type of fracture displacement. These associations may provide direction on whether to perform operative or conservative treatment. Open physes were present in 21 patients and 11 (52%) of them had Myerson B1 fractures. Only 7 (33%) of these patients with open physes underwent surgical treatment. Closed physes were present in 18 patients and 10 (56%) of them had Myerson B2 fractures. 12 (67%) of these patients with closed physes underwent surgical treatment. Both groups of patients with open and closed physes were primarily treated using ORIF, but significant differences were observed in the length of time it took to weight bear as tolerated. During follow-up examination, patients with closed physes were graduated from non-weight bearing status to weight bearing as tolerated after an average of 13 weeks while patients with open physes were graduated after an average of 8 weeks.
Classification of the eight patients by Cheow and Lam 13 revealed six patients with Myerson B2 fractures, one patient with Myerson B1 fracture, and one patient with Myerson A fracture. The presence of open or closed physes were not disclosed in the case results of this study.
From the 19 fracture patients reviewed by Kushare et al., 14 17 (89%) had Myerson B2 fractures, one patient had an A1 Myerson fracture and another one patient had a C1 Myerson fracture. The presence of open or closed physes were not disclosed in the case results of this study as well.
Treatment methods
Non-operative
All eight patients reviewed by Buoncristiani et al. 11 were treated non-operatively with a short leg walking cast (SLWC) and followed at three- and six-week intervals. Immobilization ranged from three to seven weeks and was discontinued after the patients had resolution of pain at the TMT joint complex and were able to ambulate without complications.
From the 56 patients reviewed by Hill et al., 5 37 (66%) were treated nonoperatively and either did not require reduction or underwent closed reduction with immobilization using a SLWC or a fracture brace.
From the 30 patients reviewed by Kushare et al., 14 11 cases underwent conservative management with eight (73%) using a SLWC and three (27%) using fracture braces.
Operative
All seven patients reviewed by Veijola et al. 12 underwent ORIF using both cannulated screws and K-wires.
From the 56 patients reviewed by Hill et al., 5 19 (34%) were treated operatively with all patients undergoing ORIF using screws; two patients required an external fixator plate placed prior to ORIF due to severe crush injuries.
From eight patients reviewed by Cheow and Lam, 13 five underwent ORIF with three cases using K-wires and two cases using screws. Three patients underwent closed reduction percutaneous fixation with two cases using screws and one case using K-wires.
From 30 patients reviewed by Kushare et al., 14 19 underwent operative management with 14 (76%) cases using ORIF using screws, 2 (10%) cases using ORIF with K-wires, and 3 (16%) cases using suture-button fixation.
Postoperative outcomes
From the eight patients reviewed by Buoncristiani et al., 11 cast immobilization ranged from three to seven weeks and was discontinued after the patients had pain resolution of the TMT joint complex and were able to ambulate without complications. Final radiographs were taken at their last follow-up, which averaged 32 months postoperatively.
Seven patients had complete resolution of their foot pain at rest and during physical activity. Radiographs confirmed a healed injury and showed maintenance of the TMT joint complex. These seven patients had a Midfoot Functional Rating (MFR) of 100.
One patient continued to midfoot pain and edema after 5min of physical activity that was absent at rest and had an MFR of 87; symptoms were tolerated well without the need for analgesic medications. Physical examination of this patient’s TMT joint complex was benign and tenderness was not reproduced with palpation or pronation-abduction stress. The radiograph revealed a healed medial cuneiform avulsion fracture, but with residual narrowing of joint space consistent with posttraumatic degenerative joint disease of the TMT joint complex.
From the six patients reviewed by Veijola et al., 12 each patient was immobilized for an average of five weeks (range four to five) and K-wire removal was performed at an average of five weeks (range three to seven) after the operation. Postoperative radiographs graded anatomic reduction as excellent in six feet and good in one foot, but radiographs performed during outpatient follow up ranging from 3 to 26 months after the injury revealed that two different feet with excellent grade postoperative anatomic reduction subsequently developed evidence of mild degenerative changes. With regards to functional outcomes, three patients reduced their baseline activity levels and two patients were unable to participate in the same activities as prior to their injury. Screw removal was only performed for two patients after 11 weeks and 16 weeks, postoperatively. The patient with screw removal at 11 weeks did not have available data regarding degenerative changes. The patient with screw removal at 16 weeks did not have any degenerative changes.
Patients reviewed by Hill et al. 5 did not have postoperative immobilization times disclosed in the study. Operative patients were followed for an average of 29 weeks (range 25.5 to 52.5) and had an average of 14.5 weeks before they were able to weight bear as tolerated. Nonoperative patients were followed for an average of 12 weeks (range 9 to 26) and had an average of 6.5 weeks before they were able to weight bear as tolerated. Only two patients incurred posttraumatic changes due to the severity of damage to their Lisfranc joint complex. One patient had a severely displaced Lisfranc equivalent to complete displacement of the first MT with Salter-Harris fracture present and subsequently developed physeal arrest at age 12. The other patient with a severely displaced Lisfranc joint complex had unresolved pain with weight-bearing due to a broken pin that remained in their cuboid.
Post-operative complications were observed in four patients reviewed by Cheow and Lam. 13 One patient underwent ORIF using K-wires. Hardware removal occurred at four weeks, with transition from nonweight-bearing to partial weight bearing at six weeks, and full weight bearing after three months. Radiographs after six months revealed loss of reduction with an intermetatarsal distance of 2.82 mm. Pain was present during sports activities, no gait abnormalities were noted, and AOFAS score 90 points. Another loss of reduction was noted in a patient who underwent CRPF using screws. The postoperative radiograph showed an intermetatarsal of 3.49 mm between the first and second MT, which was greater than the median distance of 1.0 mm for a child of this patient’s age (13 years old). 17 This patient also complained of mild left foot pain that was reproduced when walking for 45 min or more which restricted their ability to participate in recreational activities and wear heels. AOFAS score was 85; -10 for intermittent pain, -3 for limited recreational activities, -2 for limited footwear. Finally, two patients were found to have screw breakage, with one reporting midfoot pain while the other was asymptomatic. Screw breakage was associated with premature weight bearing on the injured foot prior to hardware removal in these two patients. A limiting factor of the Cheow and Lam 13 study is the lack of information detailing the time to partial weight bearing status and compliance with weight-bearing recommendations before hardware removal. The presence or absence of posttraumatic degenerative changes was also not discussed in the interpretations of radiographs taken at each patient’s follow-up examination.
With regards to complications discussed by Kushare et al., 14 postoperative immobilization and weight-bearing status were not delineated. Two cases failed conservative treatment due to unresolved pain and/or widening of the joint space with weight bearing and both subsequently underwent surgical management. Only one patient had a post-treatment complication due to an Achilles tendon contracture. There were no cases that reported broken hardware or implants left in situ. Hardware removal occurred on an average of 28.5 days (range of 6 to 65); patients with the suture-button fixation did not require additional surgery for hardware removal.7,14 Oxford Ankle Foot Questionnaire for Children (OxAFQ-C) and Visual Analog Scale (VAS) scores were available for both operative and conservative patient groups. Operative patients had an average OxAFQ-C score of 80.8 and VAS score of 1.04. Conservative patients had an average OxAFQ-C of 79.3 and VAS score of 1.67. There were no statistically significant differences in the outcomes between these two groups.
Discussion
Currently, there is no literature with an agreed upon consensus for the best method to treat PLI, due to a dearth of literature discussing the diagnosis, treatment options, and long-term outcomes. 1 This is in part due to the rarity of its presentation in orthopedic settings and difficulty of diagnosis, as it is often missed.1,5,14 Differing opinions on treatment management are employed at different orthopedic centers and may further contribute to the lack of consensus.5,11–14 However, synthesizing the information seen across the included studies has allowed us to generate a stepwise diagnostic and treatment algorithm for PLI that is outlined in Figure 2. Understanding the risks and benefits associated with initiating surgical intervention as the primary treatment modality should be carefully considered due to the increased risk for adverse long-term outcomes such as posttraumatic osteoarthritis associated with intraarticular Lisfranc injuries.4,18 Nonetheless, the primary aim of the treatment should be able to preserve the stability of the Lisfranc joint complex by maintaining anatomic reduction of less than 2.0 mm between the first and second metatarsal bases to optimize long-term functional outcomes.
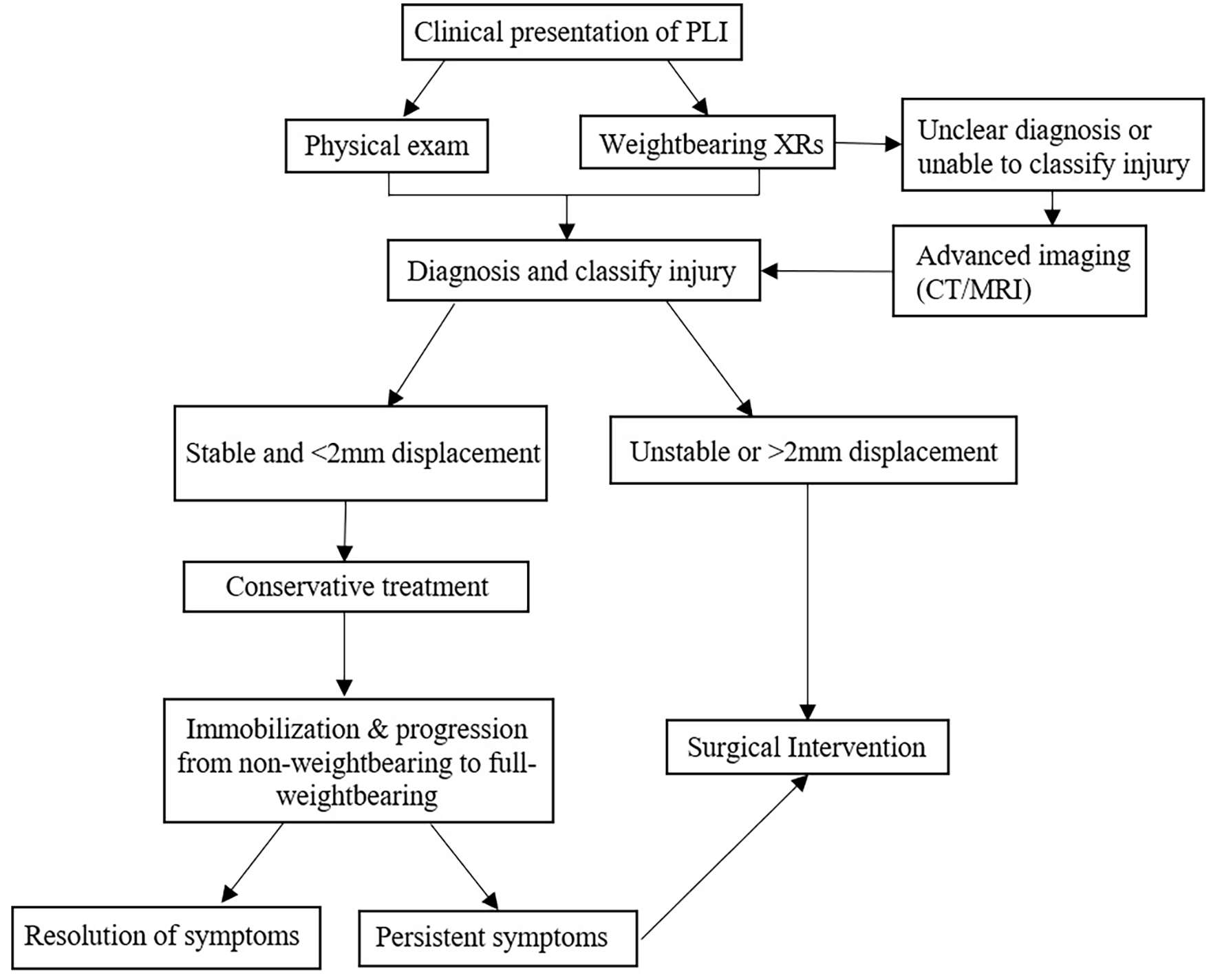
Stepwise diagnostic and treatment algorithm for PLI.
When including PLI as a possible differential diagnosis, physical exam findings and weight-bearing radiographs are helpful in aiding diagnosis. 19 PLI involving the TMT joint complex typically manifests with midfoot pain, swelling, decreased ability to weight bear, and plantar ecchymosis on physical exam.20,21 Initial weightbearing radiographs of both the injured and non-injured foot should be taken to have a baseline comparison. If weightbearing radiographs reveal that the distance between the proximal base of the first and second MTs or the distal base of the medial cuneiform and proximal base of second MT is greater than 2.0 mm, or that there is a loss of alignment between the second MT and the middle cuneiform, or that there is a fleck sign indicating avulsion within the Lisfranc joint complex—diastasis and/or instability of the Lisfranc joint complex may be present.1,14,17,22 If weight bearing radiographs are inconclusive, then advanced imaging is indicated as the next step of management using a CT or MRI scan. Operative treatment should be considered if there is greater than 2.0 mm displacement across the Lisfranc joint, evidence of soft tissue injury, or disruption of the joint complex is present on either weight-bearing radiographs or advanced imaging. With regards to advanced imaging, despite a systematic review of adult Lisfranc injuries demonstrating that CT scans may be able to detect more MT fractures and joint malalignments compared to an MRI, 23 the generalizability of this study to the pediatric population is limited due to radiation exposure.
Delay to diagnosis does occur. However, Kushare et al. 14 found that patients with subacute PLIs managed both conservatively and surgically, with average delay to treatment of four weeks, resulted in reasonable functional outcomes as measured by the OxAFQ-C and VAS score. Within the subacute group, there were no significant differences in outcomes, clinical presentation, or patient demographics compared to patients that presented with acute injuries.
With regards to management after diagnosis, conservative treatment using a short leg walking cast (SLWC) or walking boot is appropriate if the PLI reveals displacement of less than 2.0 mm and there is evidence of a stable Lisfranc joint complex. 19 Timeline for progression from non-weight bearing to partial weight bearing should range from six to eight weeks, with graduated partial to full weight bearing status ranging from eight to 12 weeks.5,13 Based on the literature review, only one postoperative complication was noted in a patient that underwent conservative management with an immobilization device (SLWC). 11 Of note, this patient was noted to have a fleck sign.
Surgical intervention should occur with evidence of instability or displacement greater than 2.0 mm with the goal of achieving and maintaining anatomic reduction across the Lisfranc joint complex to prevent the early onset of chronic pain and physical limitations due to degenerative joint disease.1,4,5,11,14 Surgeons should avoid large subperiosteal dissections to prevent physeal disruption, as this could potentially induce premature physeal closure, leading to posttraumatic osteoarthritis and impaired function.4,5,24,25
With regards to fixation, K wires and screw fixation are viable options. Recently, fixation using the suture-button technique has become more common and has been described in the adult and pediatric population.4,7,14,26 Tzatzairis et al. 7 and Kushare et al. 14 published a case report and case series study, respectively, documenting the successful treatment of a PLI using the suture button technique. The case series study by Kushare et al. 14 reported similar functional outcomes measured by the OxAFQ-C and VAS questionnaires for the three pediatric cases treated using suture buttons compared to the cases treated operatively using rigid fixation with K wires or screws. Documented advantages of using this technique may include earlier transition to full weight-bearing status at six weeks, compared to the recommended three months for rigid fixation, and lack of a second procedure for hardware removal.5,7,13,14 A cadaveric study using the suture-button technique also found evidence of similar stability as screw fixation when. 27 The suture button technique also has the added benefit of decreased risks that result from necessary secondary procedures such as hardware removal. However, additional studies will need to be conducted in PLIs to demonstrate their overall efficacy compared to other fixation techniques.
Limitations are present in this systematic literature review. This is a retrospective review of articles that comprise of non-randomized studies, differing postoperative follow-ups and management, and varying and small sample sizes. To determine the efficacy of each treatment modality available, higher-level studies with greater power and long-term follow up will be required.
Conclusion
Overall, based on our systematic literature review, we have created a stepwise treatment algorithm in hopes of aiding the diagnosis and treatment of pediatric Lisfranc injuries.
Footnotes
Author contributions
Samuel Paek was the primary author involved in collecting, analyzing, and organizing the data into the article. Dr. Michelle Mo interpreted the data and provided significant feedback that shaped the article. Dr. Grant Hogue conceived the study design and provided guidance throughout the project from beginning to completion. All authors were significantly involved in drafting and revising the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.