
Abstract
Screen time has been implicated in young children’s behaviour, but less is known about the behaviours that predict screen time and caregivers’ views about children’s screen time. Caregivers of 3- to 5-year-old Australian children completed questionnaires on their child’s screen time, behavioural and social development, sleep-related behaviours, and their own perceptions about screen time. The lower children’s personal-social development the more caregivers disagreed about setting limits, which in turn was related to longer screen times. Children’s greater externalising behaviours were associated with caregivers’ belief that setting limits causes conflicts. Children’s greater difficulties with sleep were also associated with caregivers’ belief that limits cause conflicts, which was associated with greater screen time. Therefore, more challenging behaviours are linked with caregivers’ more permissive views of screen time and with difficulties setting limits. Strategies for managing behaviours and conflicts surrounding screen time could help in regulating children’s time spent on screens.
Screen time is a regular part of young children’s lives (McArthur et al., 2022). The World Health Organization (2019) recommend no more than 1 hour of screen time per day for preschoolers, but only 25%–35% of young children meet this guideline (Hinkley et al., 2020; McArthur, Tough, & Madigan, 2022, Volkova et al., 2022). The guidelines have been questioned as lacking a strong evidence base (Stiglic & Viner, 2019), so further research on screen time is required. The early years are important for multiple developmental domains, and early behavioural tendencies are foundational for behaviours throughout childhood (Fernald & Weisleder, 2015; Hart & Risley, 1995). Children’s screen time is associated with greater behavioural difficulties (Tandon et al., 2021), negative affect (Brauchli et al., 2024), and sleep problems (Janssen et al., 2020), particularly when used to manage emotions or during bedtime (Selak et al., 2025). However, the findings vary (e.g., Liu et al., 2022), and few studies focus on preschoolers. Caregivers’ perceptions of screen time also vary (e.g., Minges et al., 2015). As young children’s time is governed by their caregivers, understanding the links between caregivers’ perceptions about screen time and children’s behaviours is vital (e.g., Coyne et al., 2021).
Screen Time and Internalising and Externalising Behaviours
Preschoolers’ screen time has been associated with poorer behavioural regulation (Lawrence et al., 2020). Behaviour regulation problems include internalising behaviours, such as anxiety, loneliness, and sadness; and externalising behaviours such as impulsivity, aggression, attention difficulties and hyperactivity; and both are associated with greater risk for later psychopathology and maladaptive behaviours (Patwardhan et al., 2021). Greater screen time is associated with greater levels of hyperactivity, impulsivity, conduct problems, and anxiety (Zoromba et al., 2023), and an increased risk of clinically significant externalising behaviours (Xie et al., 2020). Risks for emotional and behavioural problems are more likely when screen time exceeds 2 hours per day (Kwon et al., 2024; McArthur, Tough, & Madigan, 2022; Wu et al., 2017). A review by Liu et al. (2022) found bidirectional relationships — screen time predicted internalising and externalising behaviours, and internalising and externalising behaviours predicted screen time, but the findings were less consistent with externalising behaviours. Neville et al. (2021) found that higher levels of internalising and externalising behaviours among 3-year-old children predicted greater screen time at age 5, and screen time predicted later internalising, but not externalising behaviours.
Screen Time and Social Development. Greater screen time is also linked with poorer social and emotional development in preschoolers (Cost et al., 2023; Guerrero et al., 2019). Aishworiya et al. (2022) found that greater screen time at 12 and 36 months predicted poorer social development and behaviours at 4.5 years, but early social behaviours did not predict later screen times. Screen-based activities could reduce opportunities to interact with others (Duch et al., 2013). Some find that the relationship is mediated by parent-infant playtime (Wan et al., 2021) and greater parental interactions (Ma et al., 2024), suggesting the importance of caregivers’ involvement.
Screen Time and Sleep-related Behaviours. The WHO (2019) recommend 10-13 hours of sleep per day for preschoolers, and adequate sleep is critical for neuro-cognitive and behavioural development (Mukherjee et al., 2015; Touchette et al., 2007). Around 43% of children use screen devices around bedtime (Rhodes, 2017), which contributes to longer screen engagement (Paudel et al., 2024). Longer screen time is associated with shorter sleep, poorer sleep quality, and delayed sleep in preschoolers (Axelsson et al., 2022; Janssen et al., 2020), which is concerning as poor sleep can mediate the relationship between screen time and behaviour (Kahn et al., 2021; Zhou et al., 2024).
Caregivers’ Perceptions of Screen Time
Caregivers’ Rules. Caregivers’ views on screen time vary with three quarters believing that their child’s screen time is acceptable (Carson et al., 2013), 85% reporting setting limits (O’Connor & Fotakopoulou, 2016), and 68% supporting a 2-h daily limit (Schoeppe et al., 2016). Many caregivers (25%–62%) also state concerns that screen time is detrimental to behavioural and social development (O’Connor & Fotakopoulou, 2016; Rideout, 2021). In a qualitative review, Minges et al. (2015) found that most caregivers acknowledge the importance of screen time limits, its potential effects on their child’s sleep, but that screen time facilitated family interactions. Caregivers are influential as children’s screen times are longer when caregivers hold positive beliefs (Napier, 2014; Veldman et al., 2023) or more relaxed rules about screen time (Pedersen et al., 2022). Engagement times are reportedly shorter if caregivers apply rules to their children’s screen time (Fitzpatrick et al., 2023; Sanders et al., 2016). However, a recent review (Veldman et al., 2023) revealed that relationships between children’s screen times and caregivers’ rules were inconsistent.
Calming Strategy. Caregivers also view screen time as a household peacekeeping tool (Napier, 2014), a way to occupy their children (O’Connor & Fotakopoulou, 2016), and an opportunity for their child to relax (Carson et al., 2013). Elias and Sulkin (2019) found that 68% of caregivers use screen time to calm their children, a view linked with greater screen time. This approach is more likely among caregivers of young children with greater social-emotional difficulties, negative affect, and responsivity; and among caregivers who perceive behaviour management as difficult (Coyne et al., 2021; Radesky et al., 2016).
Limit Setting. Caregivers also view screen time as a source of family contention (Rhodes, 2017), and experience difficulties with setting limits, particularly with increasing child age (Jago et al., 2018). Caregivers’ frequent use of screen time to regulate children’s emotions is linked with increased emotional reactivity in children when screen time is restricted (Coyne et al., 2021).
Current Study. Further investigating caregivers’ perceptions could provide insight into whether caregivers use screen time in response to children’s behaviours. Greater clarity is also needed regarding relationships between screen time and behaviour. Given previous findings (Liu et al., 2022), we predicted that poorer behavioural and social development would be associated with longer screen times. We also predicted that children’s poorer behavioural and social development, and difficulties surrounding sleep would be associated with caregivers’ more relaxed rules and positive views of screen time (e.g., Coyne et al., 2021; Elias & Sulkin, 2019), and that these views would be associated with children’s greater screen times (e.g., Pedersen et al., 2022).
Method
Participants
A power analysis (G*Power, Faul et al., 2007) indicated that a hierarchical multiple regression with 6 predictors required 85 participants (medium effect size f2 = .15, power = 0.80, alpha = .05). For path analyses, post-hoc power was calculated (medium-to-large effect size f2 = .20, alpha = .05, 12 paths, N = 91, power = 0.77). Caregivers of Australian children were recruited using social media (N = 106, mothers = 104; fathers = 2; Mage = 36.58 years, SD = 4.83). The children’s mean age was 4 years, 3 months, 10 days (SD = 9 months, 14 days; range: 2 years, 10 months, 27 days to 5 years, 11 months, 5 days). This age range aligned with the preschool ages of the Ages and Stages Questionnaire-3 (ASQ-3). Seven children who exceeded the 5.5-year age-limit for the ASQ-3 were excluded from analyses involving personal-social scores. Caregivers’ ethnicities were: Australian (76%), European (8%), Asian (8%), Australian-European (4%), Australian-Asian (1%), New Zealander (2%), and North American (1%). All caregivers lived with their child 7 days per week.
Materials
Caregivers completed the questionnaires online (Qualtrics, 2021) between 16 September 2021 and 21 February 2022. Data are available on the Open Science Framework (https://osf.io/5ec4h/). This study was approved by the Human Research Ethics Committee (H-2021-0216) at the University of Newcastle, Australia. Caregivers provided informed consent. Questionnaires could be completed in more than one sitting (median completion time: 48.48 mins). Caregivers received an AUD$20 book voucher upon completion, mentioned after recruitment during informed consent to avoid incentivising participants.
Sociodemographic Questions. These included the child’s date of birth, sibling count, health history, and any developmental or learning difficulties; caregivers’ ethnicity, age, education level, years in education, and occupation.
Screen Time. Adapted from SCREENS-Q (Klakk et al., 2020; Pedersen et al., 2022), caregivers reported their child’s typical engagement durations on a given day on weekdays and weekends for three content types: entertainment, relaxing/calming, and educational/learning (see Axelsson et al., 2022 for details). As all children engaged with entertainment content, and fewer with relaxing and educational (see Axelsson et al., 2022), entertainment durations were the focus.
Caregiver Screen Time Perceptions. Also from SCREENS-Q (Klakk et al., 2020), caregivers agreed or disagreed with the following rule: ‘There are fixed boundaries for how much time the child may use screen media’ (hereon ‘time limit rule’). Agree was coded as 1 and disagree as 2, making higher scores more permissive. Test-retest reliability for rule-related items is moderate-to-substantial (kappa: 0.71–0.79). Caregivers also rated behaviour-relevant statements on four-point scales from strongly agree (1) to strongly disagree (4): ‘The use of screen media often helps the child calm down’ (hereon ‘helps calm child’); and ‘It often causes conflict if I try to limit the child’s screen media use’ (hereon ‘limits cause conflicts’). Lower scores reflect more positive views. Test-retest reliability for caregiver perception-related items is fair to almost perfect (kappa: 0.37–0.85).
Child Behavior Checklist (CBCL) 1.5–5 (Achenbach & Rescorla, 2000). Caregivers rated 99 statements on their child’s behaviour on a 3-point scale: not true, somewhat/sometimes true, very true/often true. Internalizing scores are derived by summing the Emotionally Reactive, Anxious/Depressed, Somatic Complaints, and Withdrawn subscale scores. Externalizing scores are derived by summing Attention Problems and Aggressive Behavior subscale scores. The CBCL has very good internal consistency (rs>.86), moderate-to-good test-retest scores (r = .68–.85), and moderate cross-informant agreement (r = .61). Subscale T-scores are classified as normal (28–59), borderline (60–63), and within clinical ranges (64–100).
Ages and Stages Questionnaire-3 (ASQ-3; Squires et al., 2009). We focussed on the personal-social domain, which includes six questions about self- and other-directed behaviours such as self-care and turn-taking. Questions are answered on a three-point scale (yes = 10, sometimes = 5, not yet = 0). Scores indicate whether development is on schedule (>∼45), whether further monitoring (∼35–40), or assessment is required (∼0–30). The ASQ-3 has moderate-to-excellent internal consistency (Cronbach’s α = .51–.87), very good test-retest reliability (ICCs = .75–.82), moderate inter-rater reliability (ICCs = .43–.69), and high concurrent validity (Rubio-Codina et al., 2016; Squires et al., 2009).
Children’s Sleep Wake Scale (CSWS; LeBourgeois & Harsh, 2016): Caregivers rate 25 items, on a 6-point scale, the frequency of children’s behaviours surrounding bedtimes, falling asleep, maintaining sleep, and getting out of bed. Scores distinguish ‘good sleepers’ (>5), children with problematic sleep behaviours (<5), and children with sleep onset issues (<4). The CSWS has moderate-to-strong test-retest reliability (r = .67–.84), moderate-to-strong correlations with caregiver diaries (r = .58–.72), and weak-to-moderate correlations with actigraphy-measured sleep quality (r = .38–.61).
Attention Check Questions. These were integrated into dense sections of the questionnaire (e.g., “I am living in the southern hemisphere (yes, no)”).
Analyses
Path analyses were performed using jamovi 2.2.5 software (2020) to determine how much children’s behaviours (exogenous variables) related to caregivers’ perceptions about screen time and how much perceptions related to children’s screen times (endogenous variables). Child age and caregiver years in education were included as both typically correlate with screen times (Reus & Mosley, 2018). Path analyses were performed separately for each caregiver perception as this led to acceptable model fit. A hierarchical multiple regression analysed direct relationships between children’s behaviours and screen time.
Results
Children’s Behaviours and Screen Time
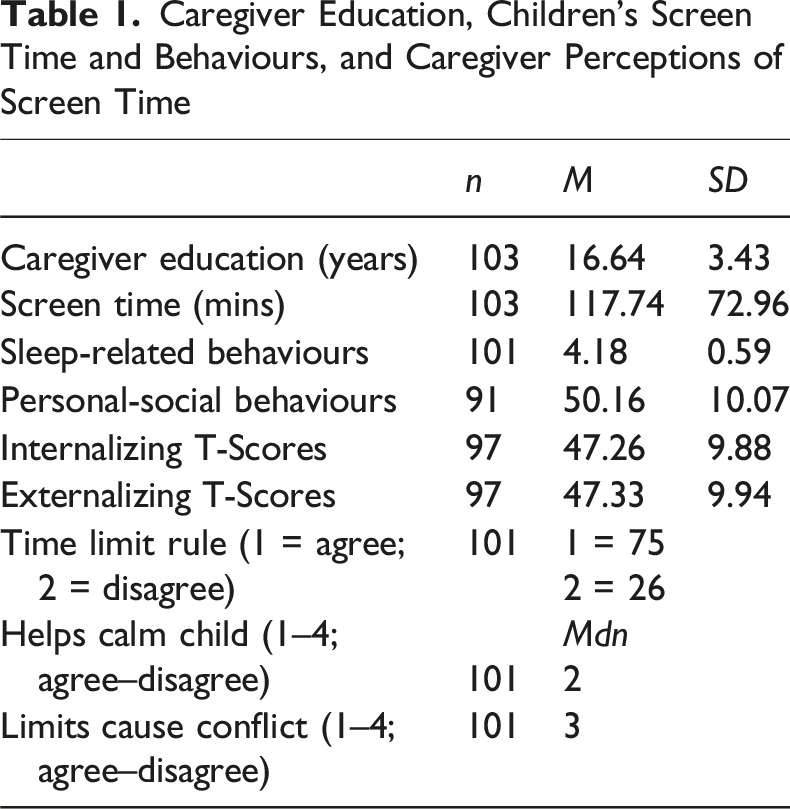
Caregiver Education, Children’s Screen Time and Behaviours, and Caregiver Perceptions of Screen Time
Screen Time and Relationships With Child Behaviours
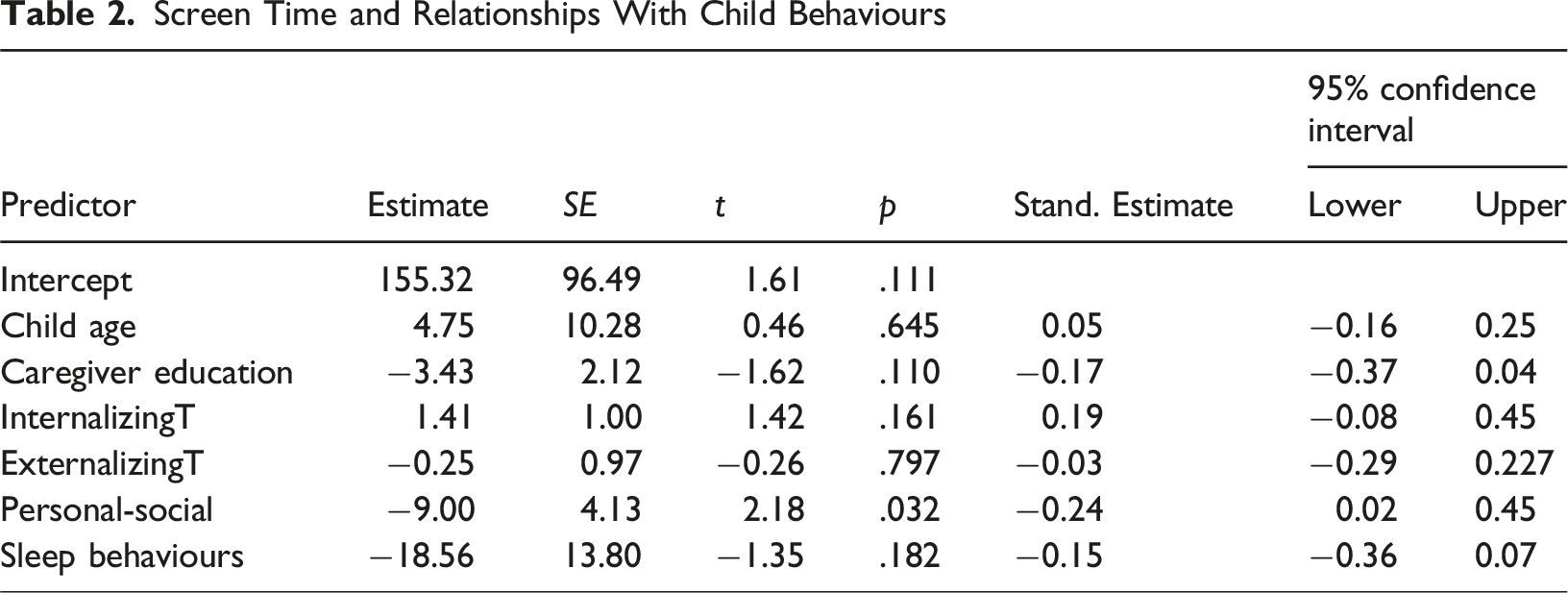
Screen Time and Relationships With Children’s Behaviours.
Children’s Behaviours, Caregivers’ Perceptions About Screen Time, and Screen Time
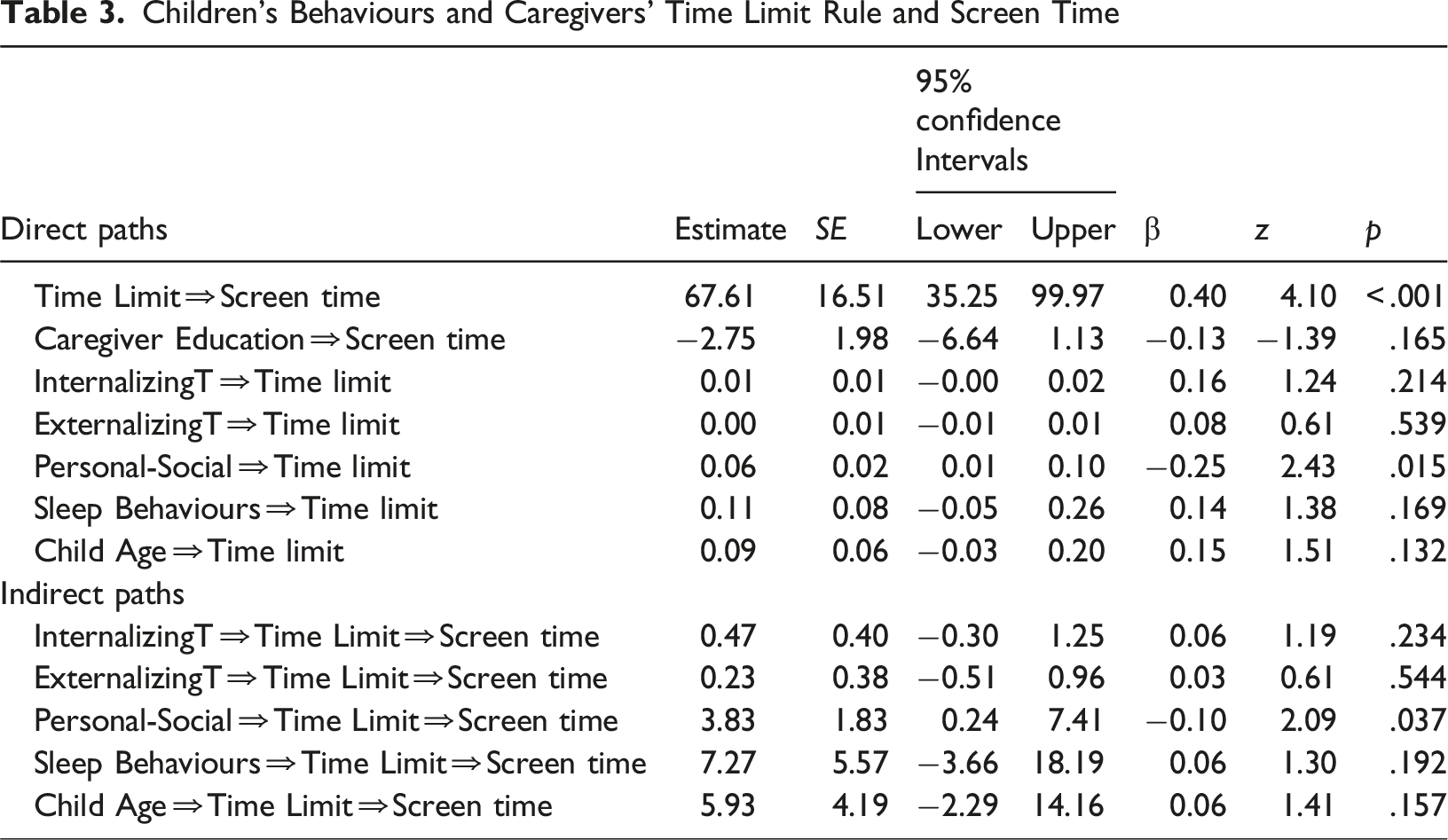
Children’s Behaviours and Caregivers’ Time Limit Rule and Screen Time
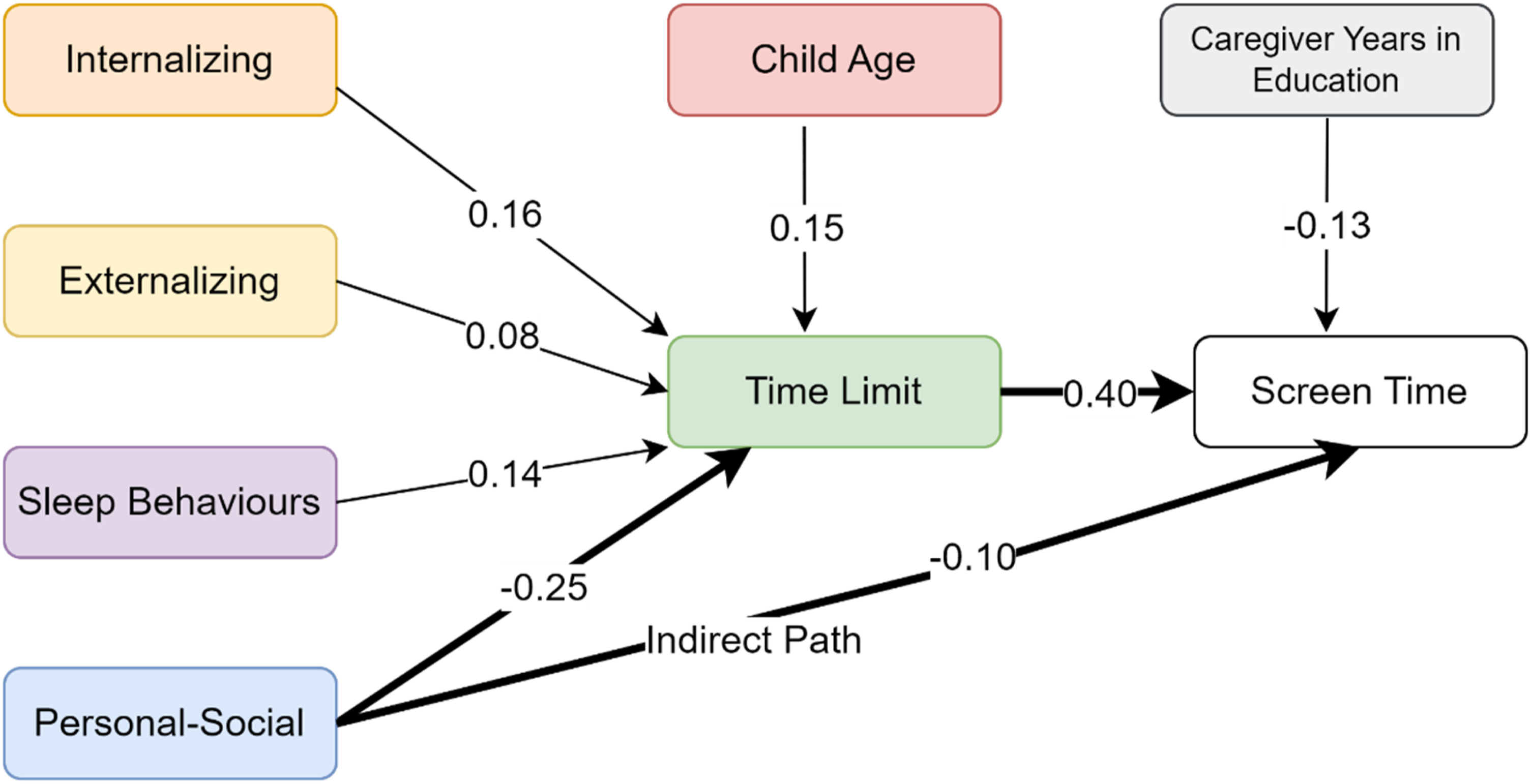
Path Plot of Relationships Between Children’s Behaviours and Caregivers’ Time Limit Rule and Screen Time
Caregivers’ Time Limit Rule and Relationships With Children’s Behaviours and Screen Tim.
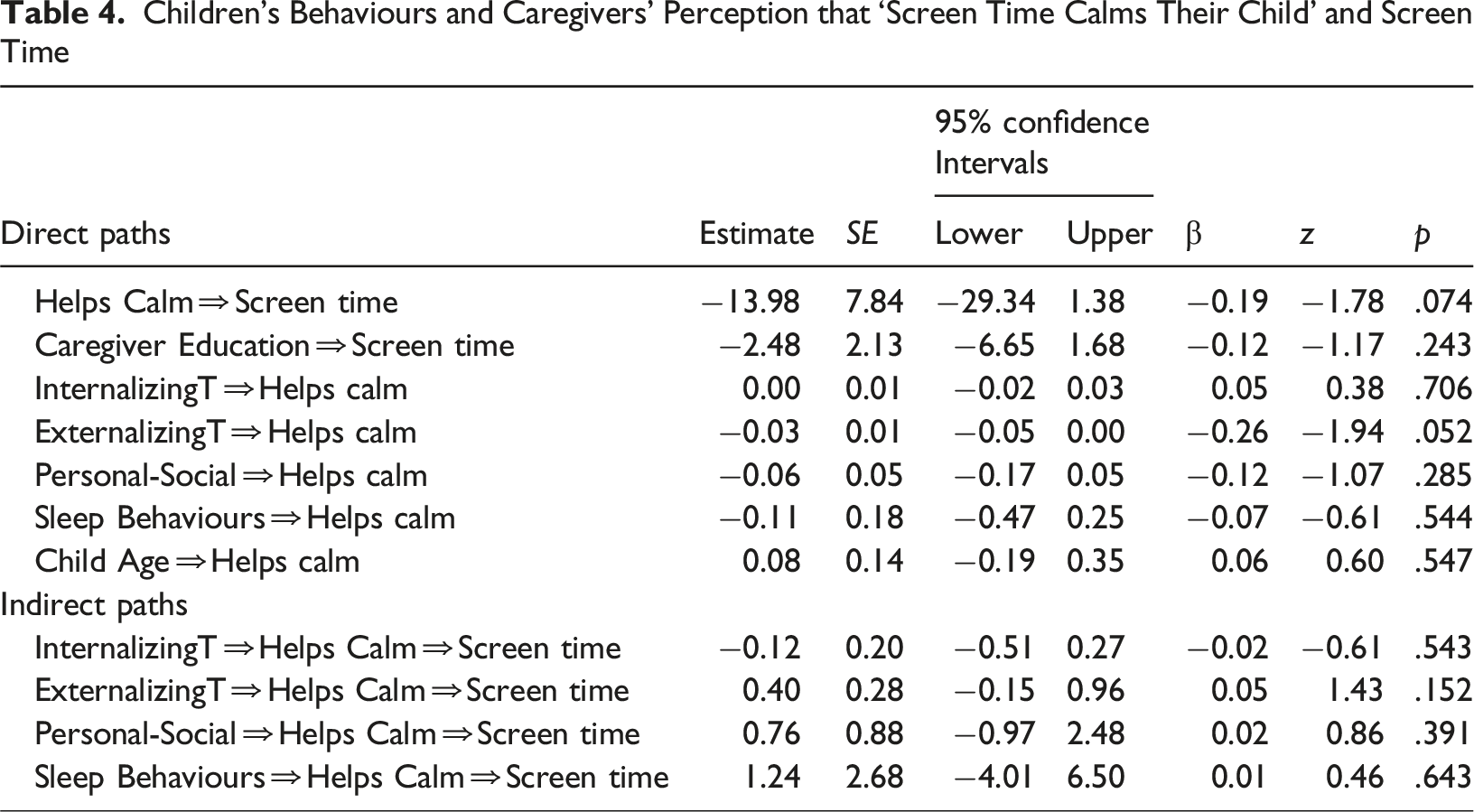
Children’s Behaviours and Caregivers’ Perception that ‘Screen Time Calms Their Child’ and Screen Time
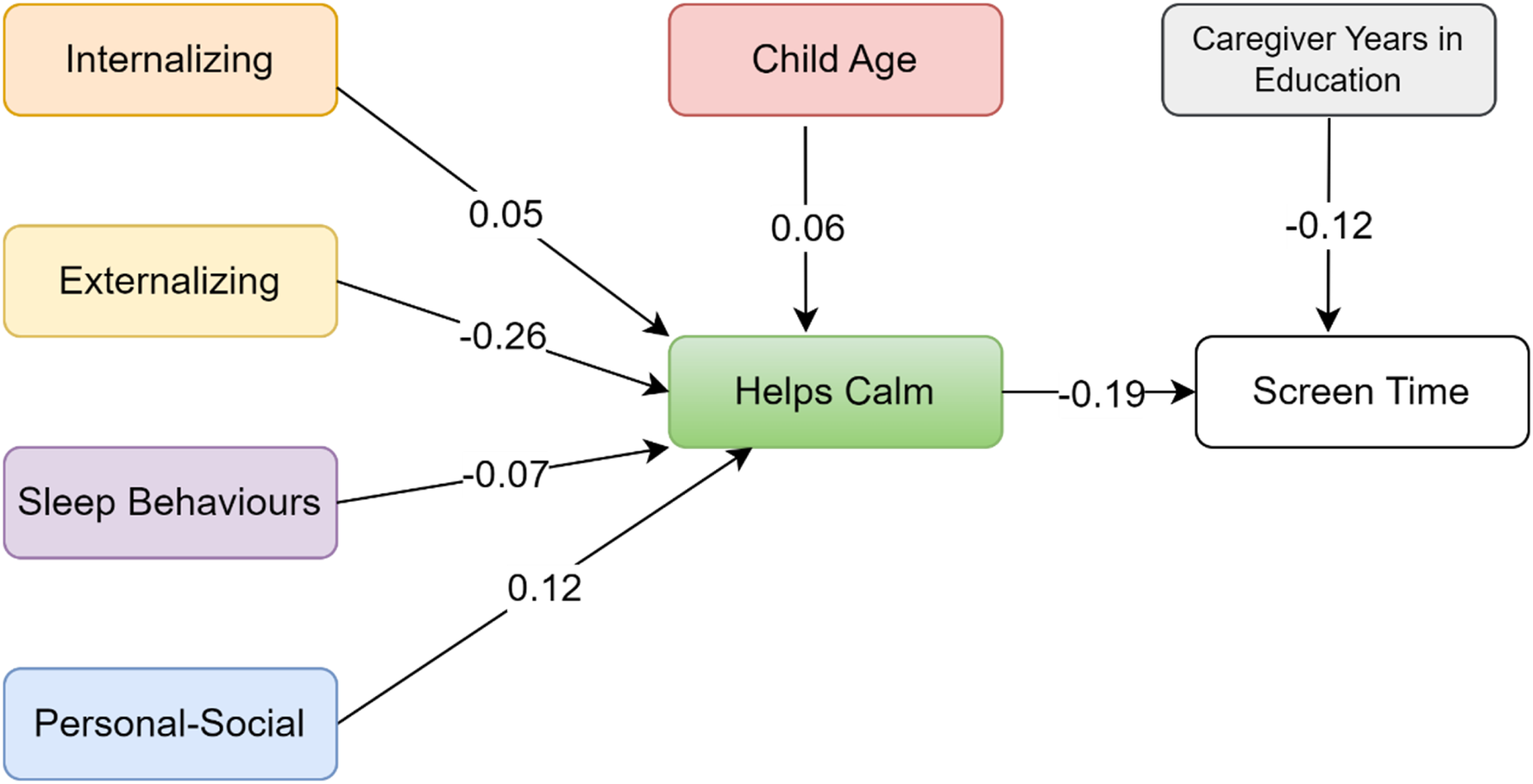
Path Plot of Relationships Between Children’s Behaviours and Caregivers’ Perception that ‘Screen Time Calms Their Child’ and Screen Time
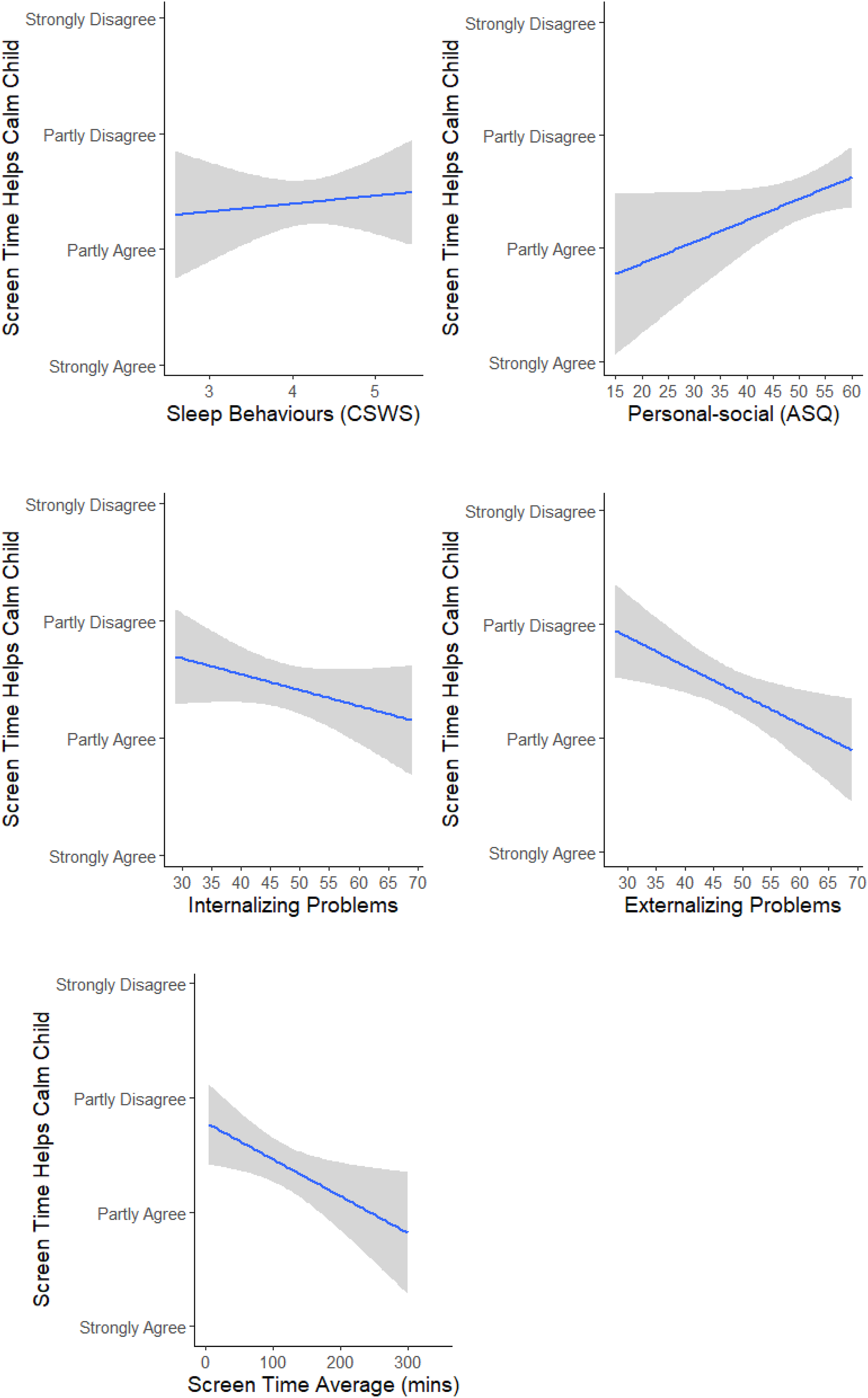
Caregiver Perception ‘Screen Time Calms Their Child’ and Relationships With Children’s Behaviours and Screen Time.
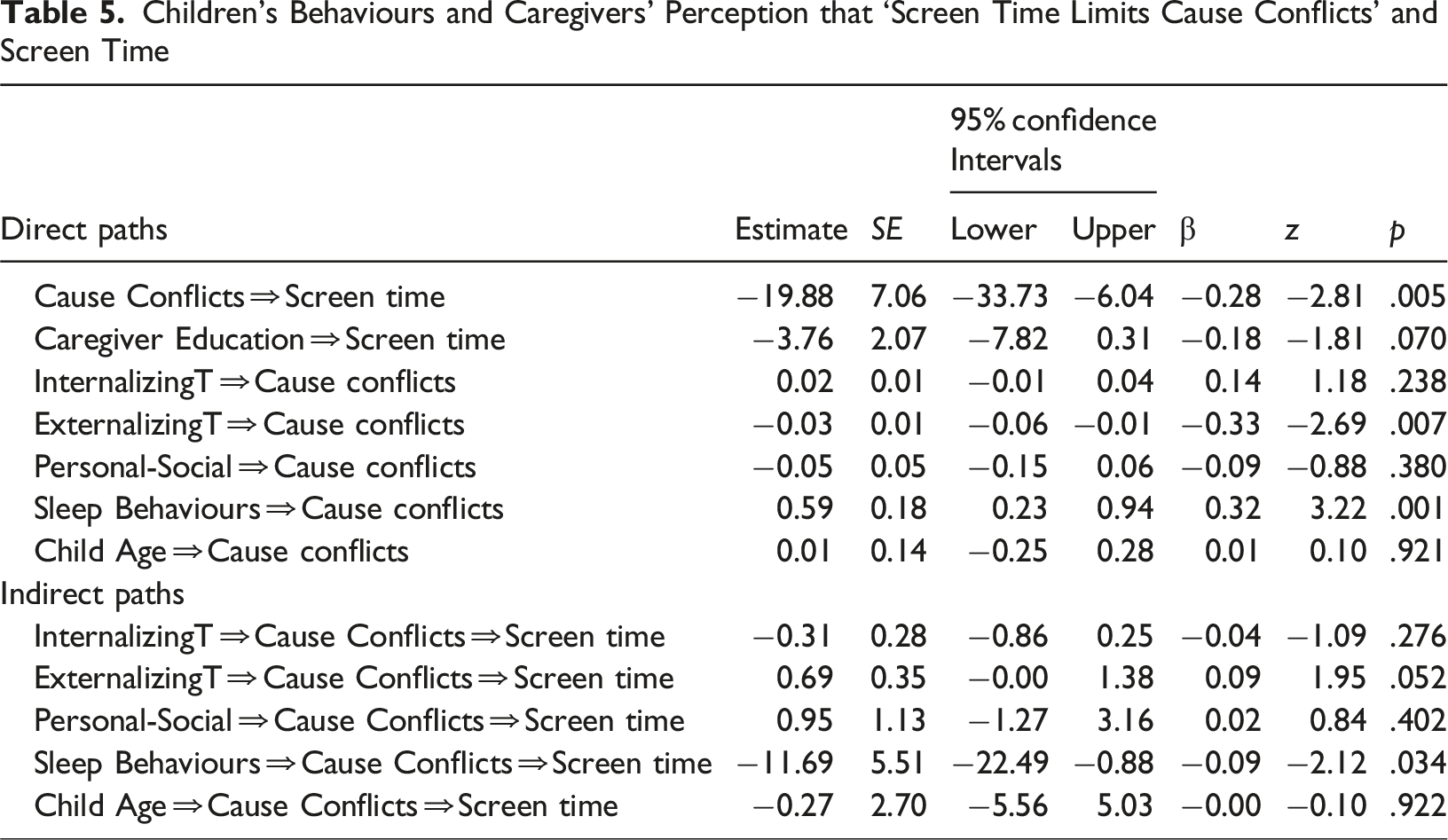
Children’s Behaviours and Caregivers’ Perception that ‘Screen Time Limits Cause Conflicts’ and Screen Time
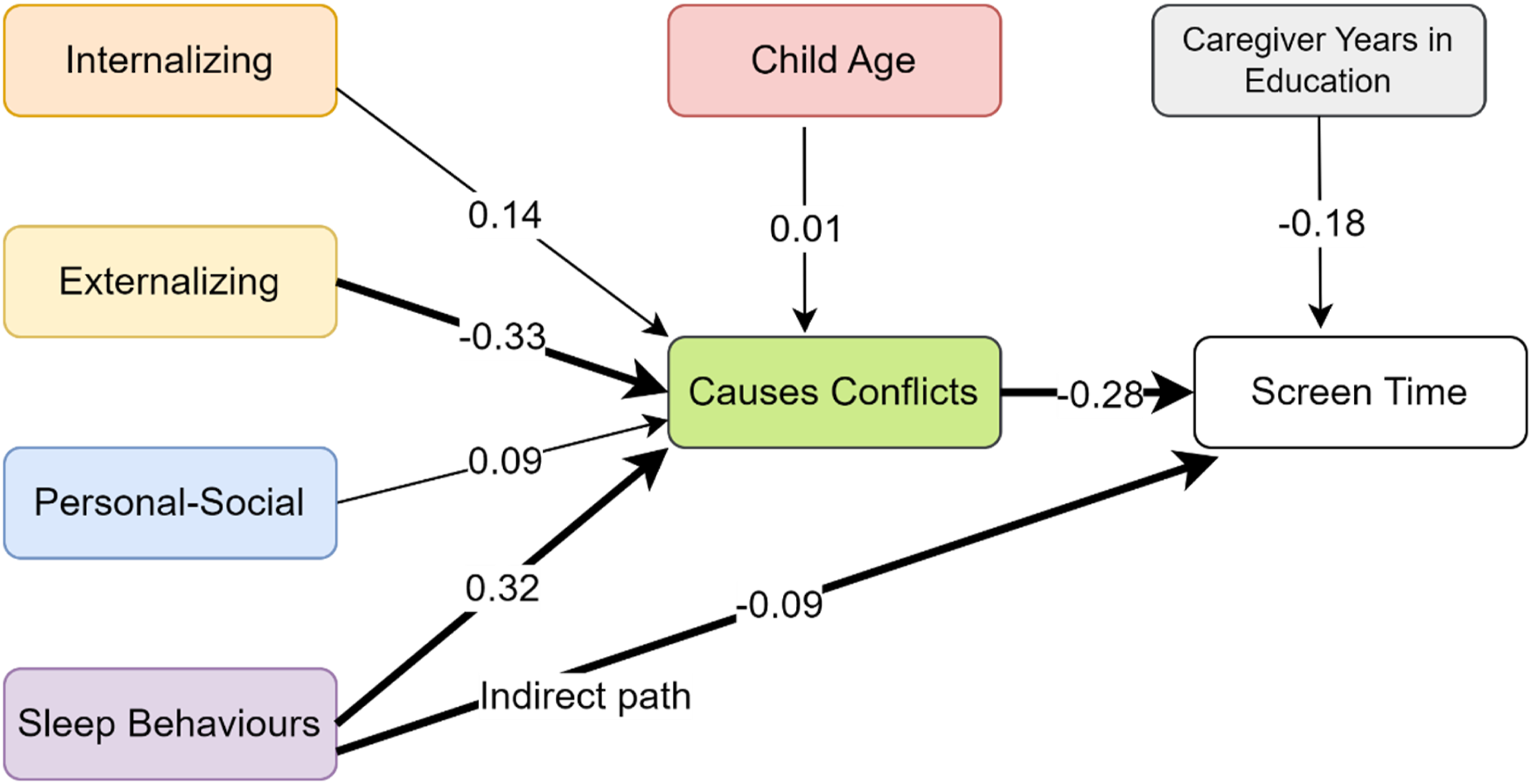
Path Plot of Relationships Between Children’s Behaviours, Caregiver Perception ‘Screen Time Limits Cause Conflict’, and Screen Time
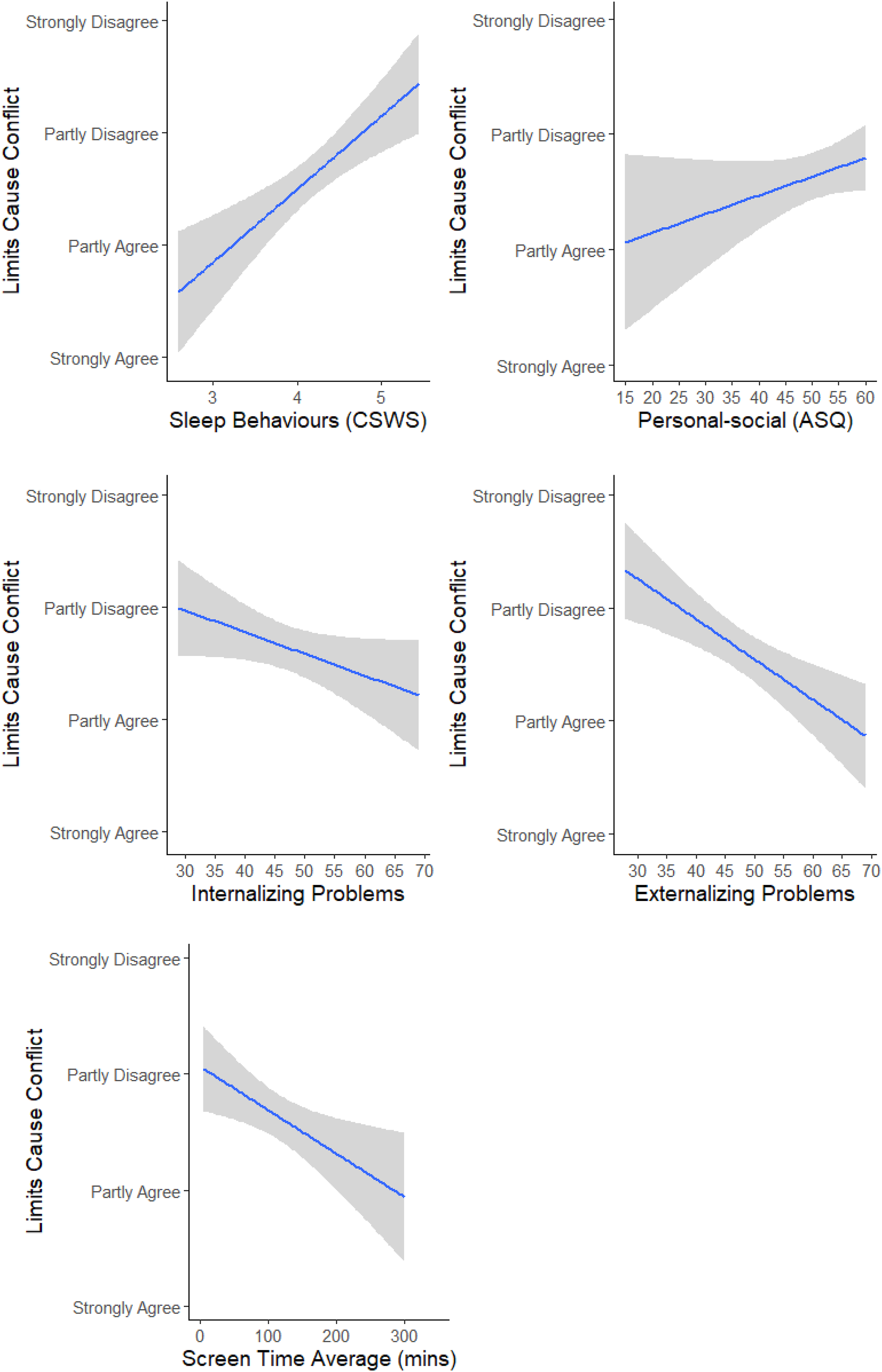
Caregiver Perception ‘Screen Time Limits Cause Conflict’ and Relationships With Children’s Behaviours and Screen Time.
Discussion
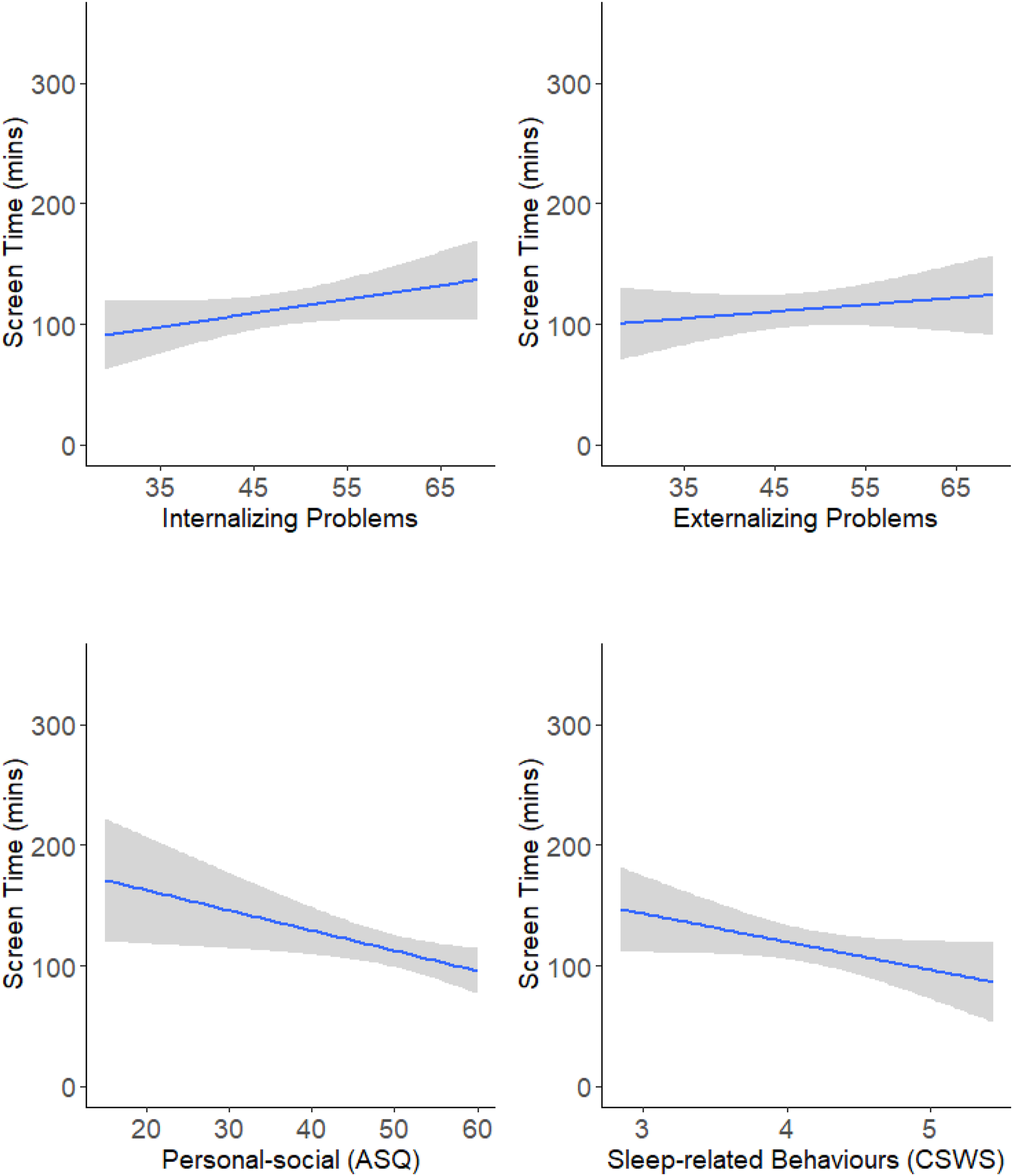
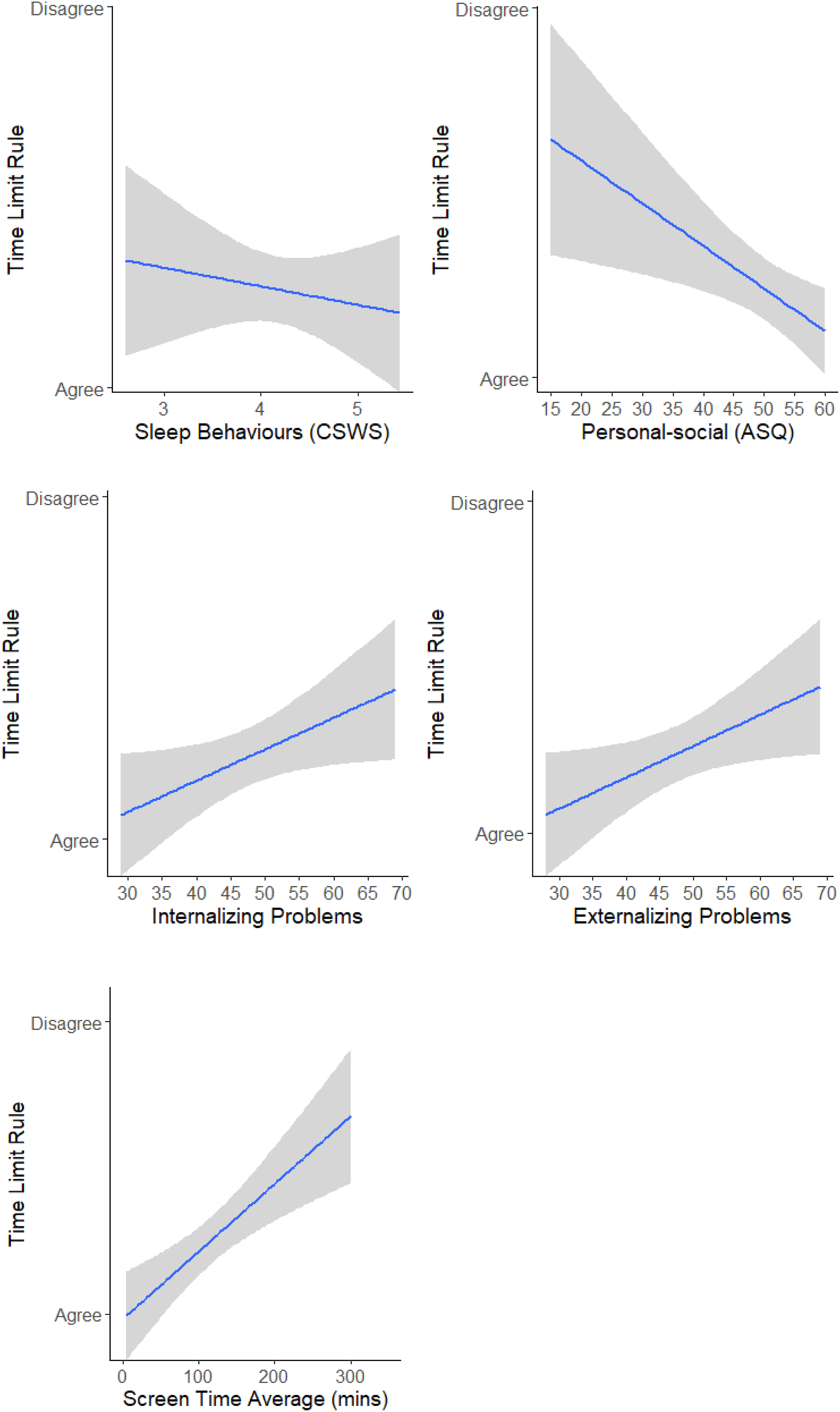
Screen Time and Behaviour. We found that preschoolers’ poorer personal-social development was associated with greater screen time. The personal-social variable reflects self- and other- directed knowledge and behaviours, such as knowing their name and cooperation with others. This finding could suggest that children with lower personal-social development are prone to engage with screens or that greater screen time hinders personal-social development. Greater screen time is linked with less time interacting with others (Brushe et al., 2024), and less socially expressive behaviours (Hinkley et al., 2018). Aishworiya et al. (2022) found that screen time earlier in life predicted poorer social development by preschool age, but not vice versa. Personal-social scores below 30-45 are classified as concerning, and these scores were associated with screen times beyond 2 hours (see Figure 1).
Caregivers’ Perceptions of Screen Time. Consistent with previous findings (e.g., Fitzpatrick et al., 2023; Pedersen et al., 2022), caregivers’ inclination to disagree about setting limits was associated with longer screen times suggesting that caregivers’ involvement is influential. Believing that limits cause conflicts was also associated with greater screen time suggesting caregivers avoid difficulties when attempting to reduce children’s screen time (Coyne et al., 2021).
Children’s Behaviours and Caregivers’ Perceptions of Screen Time. Lower personal-social development was associated with caregivers’ belief that limits are unnecessary, possibly reflecting an assumption that their child prefers screen engagement and that this aligns with their child’s personal-social tendencies. The indirect relationship between better personal-social development, a belief in time limits, and lower screen time was also significant (see Figure 2), highlighting the benefit of regulating screen time.
Believing that limits cause conflicts was associated with children’s greater externalising behaviours. Caregivers might avoid conflicts provoked by setting limits if their child acts out. More permissive parenting is linked with greater externalising and internalising behaviours (Almeida & Santos, 2024; Pinquart, 2017), so fewer rules or conflict avoidance in the context of screentime may reflect a broader parenting style.
Children’s poorer sleep-related behaviours also predicted caregivers’ belief that limits cause conflicts, which predicted greater screen time (see Figure 6). Avoiding conflicts around bedtime might occur if children demonstrate difficulties going to or staying asleep, and allowing more screen time might be a way to avoid battles surrounding bedtime.
Caregivers’ belief that screen time is calming was non-significantly related to children’s externalising behaviours, but the standardised coefficient for the relationship (−0.26, p = .052) was similar to the coefficient for the significant relationship with personal-social development (−0.25). Therefore, caregivers might view screen time as pacifying difficult behaviours, which should be further investigated.
Implications
Despite the ease of engagement with screens, limits are necessary to avoid poorer development associated with extended screen time (Guellai et al., 2022; Reus & Mosley, 2018). We found further evidence of caregiver factors in children’s screen time, but also that child factors influence caregivers’ perceptions. Challenging behaviours such as hyperactivity or aggression might contribute to caregivers’ permissive approach to screen time. Longitudinal research could help determine if caregivers’ beliefs develop because of children’s behaviours, caregivers’ beliefs about screen time precipitate screen times, and if screen time precipitates behaviours. Using screen time as a behaviour-controlling strategy (Neshteruk et al., 2021), could be problematic over time if it reinforces disruptive behaviours.
The findings also have implications for children’s sleep as caregivers’ struggles with setting limits were associated with greater difficulties at bedtime. This needs further attention as sleep is important for children’s behaviour (Touchette et al., 2007), and screen time is associated with poorer sleep (e.g., Janssen et al., 2020).
Limitations and Future Directions
Unlike previous work, we did not find significant relationships between screen time and internalising and externalising behaviours (McArthur, Tough, & Madigan, 2022; Xie et al., 2020), adding to the inconsistent findings (Neville et al., 2021; Oliveira et al., 2022; Tamana et al., 2019). While greater screen time non-significantly predicted greater internalizing and externalizing T-scores, T-scores were largely below clinical levels (60-63). Only a small portion reached clinical levels and these corresponded with screen times over 2 hours, the same duration linked with concerning personal-social scores (see Figure 1). Future studies including children with scores in clinical ranges could help determine the screen time durations associated with problematic behaviours.
A potential limitation is that participants were self-nominated, which could involve a population bias. Inviting participants from schools and medical settings could help diversify the sample as would a nationwide larger sample. Social desirability bias might also have affected reporting of children’s screen times. Therefore, objectively measuring times directly from devices or audio recordings (e.g., Brushe et al., 2024) may provide more precise data. Concurrent diaries of screen times also increase accuracy (Parry et al., 2021), and are less dependent on memory. Including behaviour ratings from others familiar with the child such as teachers, and incorporating direct observations of children’s behaviours (e.g., Early Years Toolbox behavioural tool ‘PRSIST’) could also provide more accurate data.
Another possible limitation is that during 20% of the data collection period (16th September to 14th October 2021), parts of Australia had COVID-19 pandemic-related restrictions. There were some limits on routines such as attending preschool or work, but people could socialise (in limited numbers), and engage in outdoor activities. This may have led to longer screen times and more anxieties with managing screen time (Baxter et al., 2020; Olive et al., 2020). However, the majority of the data collection period occurred when isolation requirements ended (15th October to 21 February 2022) and Kwon et al. (2024) found that screen time durations returned to pre-pandemic levels in 2021.
Practical Implications
The findings highlight the children’s behaviours that influence caregivers’ views of screen time and greater screen times. Therefore, guidelines should help caregivers not only manage screen times, but also behaviours and conflicts that can arise when setting limits. Education about practical approaches to managing screen time could help in applying screen time limits (COMMUNICATIONS et al., 2016). Kildare and Middlemiss (2017) recommend that caregivers communicate the benefits of healthy screen time habits and engage in joint decision-making when managing screen time.
Footnotes
Acknowledgements
We gratefully acknowledge funding from University of Newcastle’s College of Engineering, Science and Environment and the Centre for Brain and Mental Health Research
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the University of Newcastle’s College of Engineering, Science, and Environment and Centre for Brain and Mental Health Research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.