
Abstract
Early Childhood Education and Care (ECEC) services are critical points of intervention for children impacted by trauma. Intervention Mapping was utilised to develop an initiative for trauma-informed organisational change in ECEC. This paper describes how the research team understood the need and opportunity for the program using Intervention Mapping Step 1. This included: (i) convening a planning group, (ii) conducting needs assessment, (iii) describing the context for intervention, and (iv) establishing program goals. Benefits, challenges, and recommendations on using Intervention Mapping for program development in ECEC settings are discussed.
The prevalence of childhood trauma and the negative impact it has on children are increasingly recognised and documented. Childhood trauma, defined as “an experience, or pattern of experiences, that impairs the proper functioning of the person’s stress-response system, making it more reactive or sensitive” (Perry, 2016; Perry & Daniels, 2016), is increasingly present in Early Childhood Education and Care (ECEC) contexts. In Australia, a recent national survey of child maltreatment (up to age of 18) documented the prevalence of exposure to physical abuse (32%), sexual abuse (28.5%), emotional abuse (30.9%), neglect (8.9%) and domestic violence (39.6%) (Australian Child Maltreatment Study; Mathews et al., 2023). Extensive research evidence highlights the deleterious impact of childhood trauma on health and development (e.g., Powers et al., 2015; Shonkoff et al., 2012).
Increasingly, ECEC services support children and families impacted by trauma, playing a critical role in buffering the negative impacts of trauma (Bartlett & Smith, 2019; Loomis, 2018). However, ECEC professionals often lack training in trauma-informed practice through pre-service education (Sun, Tamblyn et al. 2023), and without adequate preparation and support, they face difficulty identifying and responding to trauma. This can negatively impact their wellbeing through emotional burden, frustration, burnout, and vicarious trauma (Sun, Tamblyn et al. 2023), influencing their capacity to provide quality education and care (Cumming, 2016; Kwon et al., 2022). A recent scoping review identified 12 trauma-informed interventions in ECEC settings, with promising effects on children’s social-emotional competence and behaviour, and teachers’ knowledge, attitudes, self-efficacy, and practice (Sun, Blewitt et al. 2023). However, most of the formally evaluated trauma-informed interventions focus on training and coaching of frontline educators (Sun, Blewitt et al. 2023).
While it is essential to upskill early childhood educators in supporting trauma-impacted children, simultaneous organisational change, driven by ECEC leaders, to support educators in adopting and sustaining new practices such as trauma-informed strategies is critical (Douglass, 2016). The responsibility to support children should not reside with educators alone, but rather the organisation through policies, procedures, culture, and professional supports that maximise educators’ capacity to attend to the needs of children. Recognising the importance of organisation-wide trauma-informed practices in ECEC, and its noticeable absence in research literature to date, the research team co-designed a Trauma-informed Early Childhood Organisations (TIO) program with early childhood educators, leaders and practitioners using Intervention Mapping methodology.
Understanding the need for trauma-informed early childhood education and care organisations
Intervention Mapping is a comprehensive and systematic framework for developing, implementing, and evaluating programs and interventions (Bartholomew Eldredge et al., 2016). Underpinned by participatory approaches, theoretical and evidence-based decision making, and systems perspectives that consider the individual, interpersonal, organisational, and community influences on behaviour and health outcomes, the framework offers a six-step iterative process, where each step builds on those before. These steps are: (i) develop logic model of the problem; (ii) determine program outcomes and objectives – logic model of change; (iii) design program; (iv) produce program components; (v) develop implementation plan; and (vi) develop evaluation plan. Each step includes a series of tasks that lead to the development of a product that informs the next, providing program developers with practical guidance integrating research evidence, theory, and stakeholder insights. The process is iterative rather than linear, enabling the backwards and forwards incorporation of all forms of evidence (Bartholomew Eldredge et al., 2016).
Intervention Mapping has been effectively used to develop behaviour change programs across a range of health problems such as physical activity (Krops et al., 2018), nutrition (Springvloet et al., 2014), and disease prevention (Garba & Gadanya, 2017). Increasingly, Intervention Mapping is applied in other fields, for example to design education-related programs such as the Educator-Parent-Child Relationship [E-PCR] program (O’Connor et al., 2017) and Social-Emotional Engagement and Development [SEED] Program (Blewitt et al., 2020). Early successes suggest Intervention Mapping offers the early childhood sector (O’Connor et al., 2018) an opportunity to engage stakeholders in a participatory, theory- and evidence-informed process that supports program design and decision-making.
The exploration and implementation of trauma-informed practices in early childhood is growing and requires a shift from a focus on educators, to organisations (Sun, Blewitt et al. 2023). Intervention Mapping supported the integration of research and theory with the perspectives of diverse stakeholders across education, social work, psychology, and public health; as well as the lived experience of those involved in delivering education and care to trauma-impacted children to ensure authenticity, trustworthiness, and rigour of the TIO program.
Study context and aim
This research project was conducted in partnership between Alannah and Madeline Foundation (the Foundation) and the Monash University in Victoria, Australia. An evaluation of the early childhood Trauma Consultancy Service (Blewitt et al., 2023) conducted by these collaborators highlighted the need for a trauma-informed ECEC organisational change. The current article describes how Intervention Mapping Step 1 was used to examine the needs and opportunities for trauma-informed support at all organisational levels, by: (i) describing how the multi-disciplinary research team understood and operationalised Step 1 within the ECEC context; (ii) presenting the logic model of the problem, generated and refined through the comprehensive needs assessment and stakeholder engagement, and (iii) sharing learnings on using Intervention Mapping to develop programs within this context.
Methods
Overview of step 1: Logic model of the problem
Overview of the step 1 tasks.
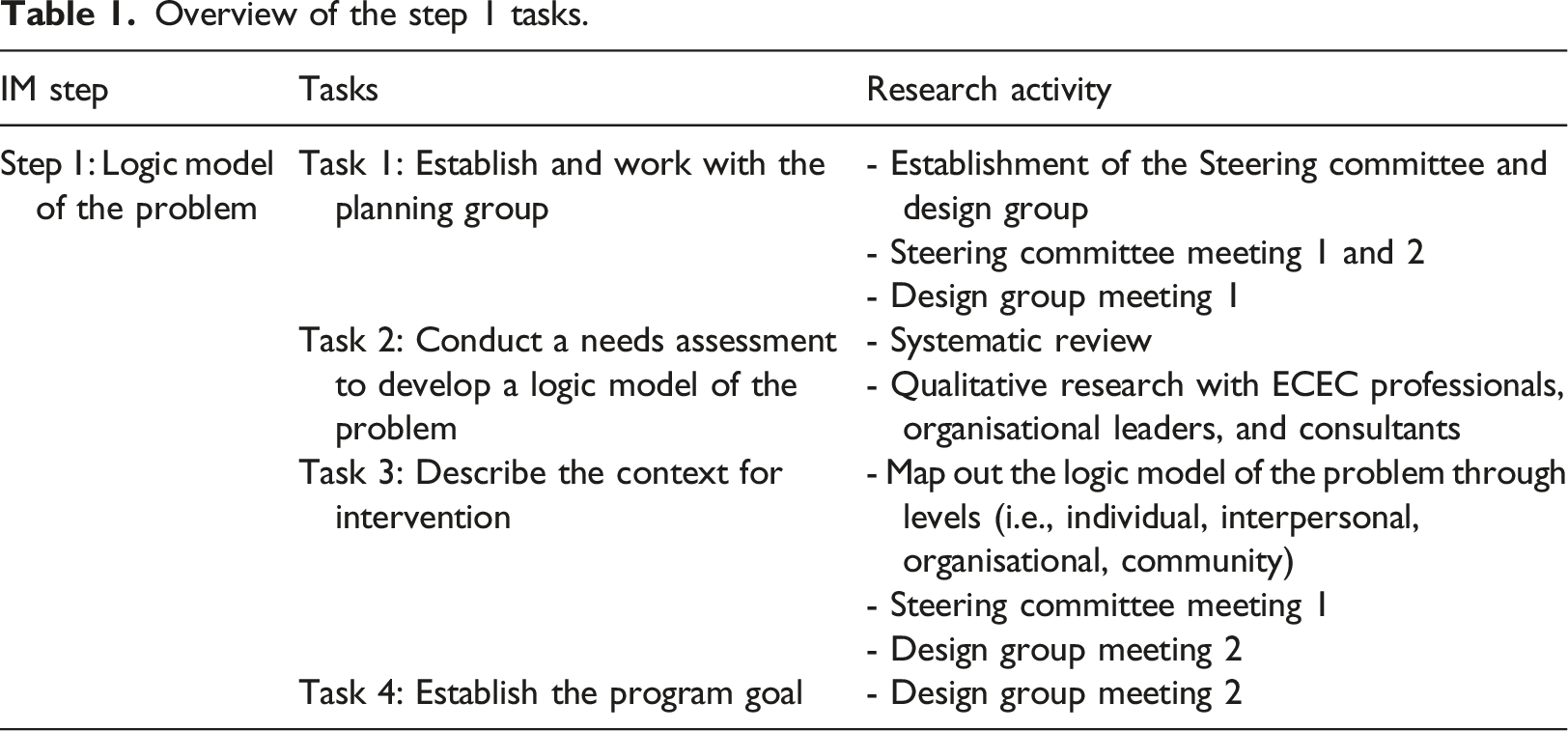
Task 1: Establish and work with a planning group
A multi-disciplinary research team was formed, including senior representatives from the industry partner and university academics with backgrounds in psychology, social work, public health, education, and co-design. The research team met weekly to plan program development and track progress. One of their first tasks was to convene two consultative groups – a Steering Committee and a Design Group.
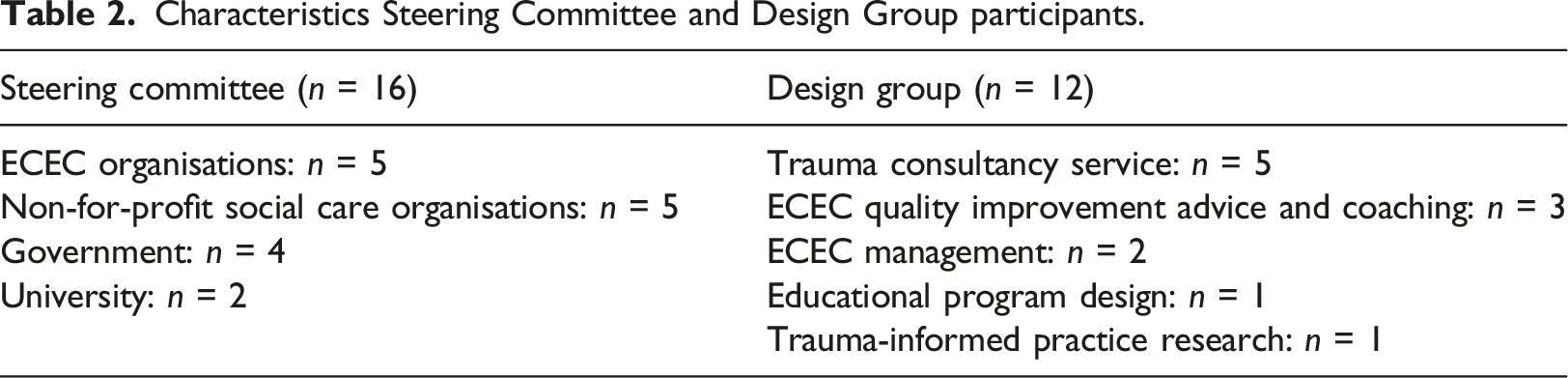
To form the Steering Committee, the Foundation’s existing knowledge and relationships within the ECEC sector were utilised. Using purposive sampling, potential participants with expertise in: (i) trauma, (ii) early childhood education, and/or (iii) organisational change were invited to join the Steering Committee. Committee members came from both metro and regional ECEC organisations, organisations representing and supporting First Nations and Non-English-Speaking children and families, and government departments involved in the delivery of services supporting children and families experiencing vulnerability. The Steering Committee: (i) provided strategic advice, expertise and project stewardship; (ii) helped the research team interpret and incorporate various data (e.g., from literature, needs assessment, consultations, etc.) into project design; and (iii) nominated other stakeholders to participate in research tasks or the Design Group.
A similar approach was applied when forming a Design Group, drawing on the Foundation’s existing relationships and knowledge, and recommendations from the Steering Committee. Sampling prioritised those in roles supporting frontline professionals, such as trauma consultants and coaches, leaders who advocate for trauma-informed practices, and educational program development specialists. This group shared their lived experience and “on the ground” reflections, and provided hands-on assistance to develop the program. To maximise participation, a Terms of Reference for both groups was shared at the point of invitation, outlining the groups’ purpose, scope, and member expectations.
Task 2: Conduct a needs assessment to develop a logic model of the problem
The second task in Step 1 was to conduct a needs assessment that would inform the creation of a logic model of the problem. Below, we describe the research activities that contributed to this model.
Literature review
A systematic literature review was conducted to explore the components and effectiveness of current trauma-informed interventions focusing on organisation-level change through education and social care. Searching and selection was conducted in accordance with the Preferred Reporting for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Page et al., 2021). Four electronic databases (i.e., PsycINFO, Medline, ERIC, IBSS) were searched in March 2022 using the following search concepts: trauma, organisations (e.g., organisation, system), intervention (e.g., program, framework, model, intervention), and educational or social care setting (e.g., school, early childhood, kindergarten, community service). Criteria for the selection of eligible articles includes: (i) intervention explicitly targeted trauma-informed organisational change; (ii) intervention was delivered within education or social care settings; and (iii) effectiveness of at least one component of the organisational change was evaluated. The titles and abstracts of 3,733 references were screened, with 198 articles read in full and assessed against the inclusion and exclusion criteria [YS & CB]. Example exclusion reasons include 1) program does not target organisation-level change, 2) study does not measure the effectiveness of at least one component of the intervention, 3) trauma is not the core focus of the intervention or program. A narrative review was then conducted to examine the determinants of organisational change with regards to trauma-informed practices.
Qualitative inquiry
Qualitative inquiry was conducted to understand the experiences of early childhood professionals working with trauma-impacted children, their practices and perspectives on the barriers and enablers of trauma-informed organisational change in ECEC organisations. In-depth, semi-structured interviews were held with 22 purposively sampled participants from Victoria, Australia via Zoom using an interview guide. Of the 22 participants, nine were early childhood professionals (e.g., teachers, educators, centre directors), eight were early childhood organisational leaders (e.g., area managers, practice coaches, approved providers), and five were childhood trauma consultants. Thematic analysis informed by Braun & Clarke (2006) six-step framework and Maguire & Delahunt (2017) practical guide was performed using NVivo. More detailed information for this qualitative inquiry is reported elsewhere.
Creating a logic model of the problem
The logic model of the problem captures the problem the program sought to address (i.e., compromised educator and child wellbeing), describing the factors and drivers of the problem at different levels (e.g., individual, interpersonal, organisational). Findings generated through the systematic review and qualitative inquiry were combined with Steering Committee and Design Group insights to develop the logic model.
Task 3: Describe the context for the intervention
At the first Steering Committee and Design Group meetings, the complexity of the ECEC context was discussed. This highlighted the diverse management bodies (e.g., government, early years management, parent committee) and operating models (e.g., long day care, sessional kindergartens, for-profit, non-for-profit) in existence.
Task 4: Establish the program goal
Drawing on knowledge generated in Step 1 and the logic model of the problem, several program goals were drafted by the research team for Design Group consideration. Design Group participants discussed, voted and agreed on an overarching program goal that was later endorsed by the Steering Committee.
Results
Task 1: Establish and work with planning group
Characteristics Steering Committee and Design Group participants.
Task 2: Conduct a needs assessment to develop a logic model of the problem
Literature review
Study Characteristics.
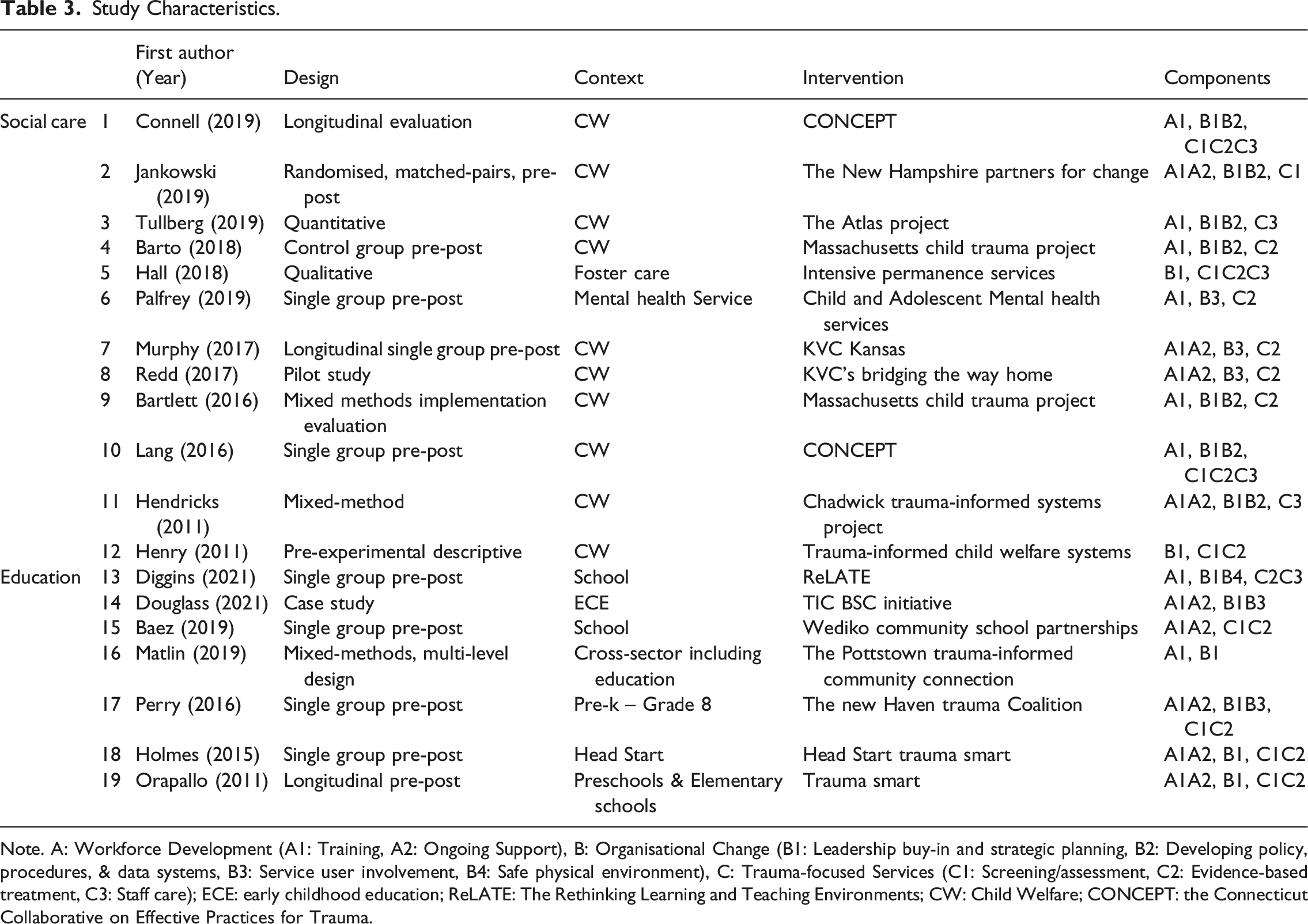
Note. A: Workforce Development (A1: Training, A2: Ongoing Support), B: Organisational Change (B1: Leadership buy-in and strategic planning, B2: Developing policy, procedures, & data systems, B3: Service user involvement, B4: Safe physical environment), C: Trauma-focused Services (C1: Screening/assessment, C2: Evidence-based treatment, C3: Staff care); ECE: early childhood education; ReLATE: The Rethinking Learning and Teaching Environments; CW: Child Welfare; CONCEPT: the Connecticut Collaborative on Effective Practices for Trauma.
The narrative review identified several factors enabling organisational-level trauma-informed practices, as shown in Figure 1. At the community level, cross-sector collaboration based on shared understanding of trauma (e.g., Barto et al., 2018), intra- and inter-organisation partnerships (e.g., Vendetti et al., 2017), and community education (e.g., Ahrens et al., 2022) to ensure shared trauma-informed language, are identified as critical factors. Organisations’ readiness to change (e.g., Winters et al., 2020), vision for trauma-informed approaches (e.g., Popescu et al., 2017), culture (e.g., Unick et al., 2019), climate (e.g., Maltzman et al., 2011), structure (e.g., Vona et al., 2018), and policy landscape (e.g., Winters et al., 2020) influence buy-in, intervention acceptance and sustainability. Leadership commitment (e.g., Atwool et al., 2019; Kim et al., 2021) is also an essential factor, as leaders are important drivers of organisational change. Determinants of trauma-informed change identified from systematic review.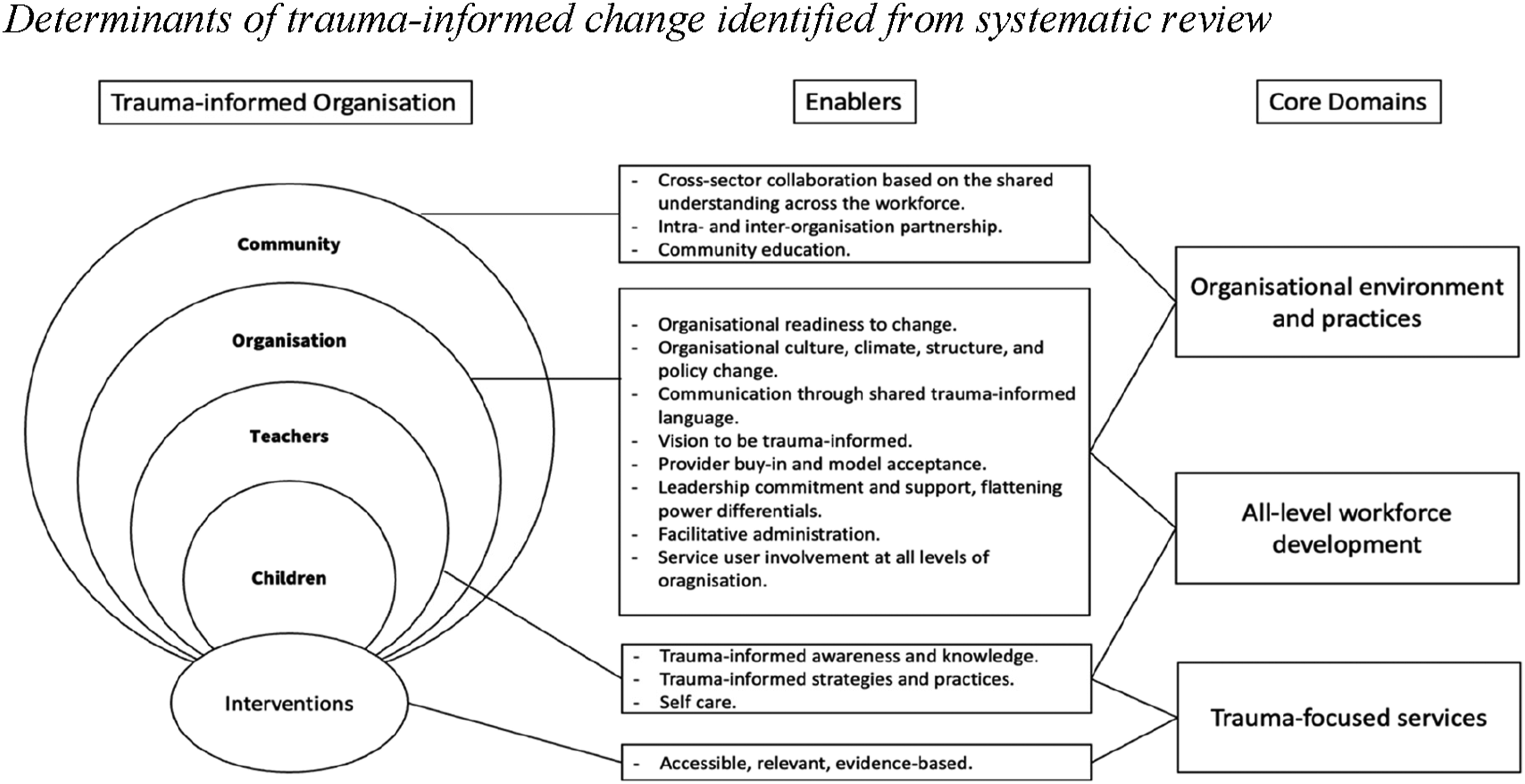
Qualitative inquiry
Thematic analysis of the 22 interviews confirmed that trauma is increasingly present in ECEC. Educators reported feeling unprepared (n = 12) and unskilled (n = 16) to support these children (e.g., “I feel like it’s not something that anyone knows, because we are not taught it.“); and when combined with other professional challenges, they feel overwhelmed (n = 22). Challenges reported by ECEC professionals include managing children’s challenging behaviours (n = 6), managing difficult communications with families of children impacted by trauma (n = 7), balancing the needs of trauma-impacted children with other children (n = 7), straddling multifaceted roles expected of educators (n = 4), educators’ lack of perceived and physical safety (n = 6), lack of trust and respect from leaders, and insufficient opportunities to have their voices heard (n = 13). Educator wellbeing was felt to be negatively impacted by working with children impacted by trauma (n = 22) (e.g., “I have almost been desensitised, from my empathetic nature, to be able to psychologically cope with this working environment.“; “We need the support just as much as the children need the support, I suppose.“). The wellbeing and support mechanisms within ECEC services currently relies on peer debriefing, and professional services are lacking (n = 17) (e.g., “I feel like we don’t have any professional support. But it would be more peer support, like us, reaching out to one another, but not actually implementing any, any professional things, which is definitely something that we can look into.“). Organisational leaders shared that educators often do not actively seek wellbeing support (e.g., “They would just try and get along on their own. Until it gets so bad that they’ll go to their area manager or contact someone else in the organisation. But up until then, they’re just on their own, they’ll just think, ‘oh, I have to deal with this on my own.’ But you don’t.“). Systemic and service barriers impacting the implementation of trauma-informed practices in ECEC were also identified. For example, system and service barriers impact opportunities for practice improvement (i.e., tight educator-child ratio, constricted time allocation, complex processes to access additional funding and support) (n = 16), sector diversity and complexity impacts transferability and unity (i.e., diverse governance and management arrangements) (n = 11). More detailed themes, subthemes, and quotes are reported elsewhere.
Creating a logic model of the problem
The Logic Model of the Problem (Figure 2) was developed from right to left, starting with the problem (i.e., compromised educator and child wellbeing) as it relates to the lack of organisational-level trauma-informed practices in ECEC (Phase 1). In Phase 2, the behavioural and environmental factors contributing to these are described across multiple ecological levels (individual, interpersonal, organisational, community, system). Phase 3 focuses on what underpins these behavioural and environmental factors, such as the knowledge, beliefs and skills that may influence individuals’ behaviours and the culture, resources, and funding that impact the environment and context. It is important to note that the generation and refinement of this Logic Model of the Problem was iterative and reflexive. Firstly, the research team shared the findings from the systematic review and qualitative study with the Steering Committee who were asked to share their professional expertise. Feedback was collated with needs assessment data and refined into a draft Logic Model of the Problem that was re-checked by the Steering Committee.
The research team then presented the logic model to the Design Group, who identified a number of additional determinants, for example, the influence of external professionals and services providing conflicting advice. Thus, shared understanding and language across multidisciplinary professionals working in the ECEC environment is critical, further highlighting the significance of cross-sector collaboration. These suggestions were included to further refine the Logic Model of the Problem, for example adding leaders’ trauma-informed awareness, knowledge, beliefs, and skills as determinants. Logic model of the problem.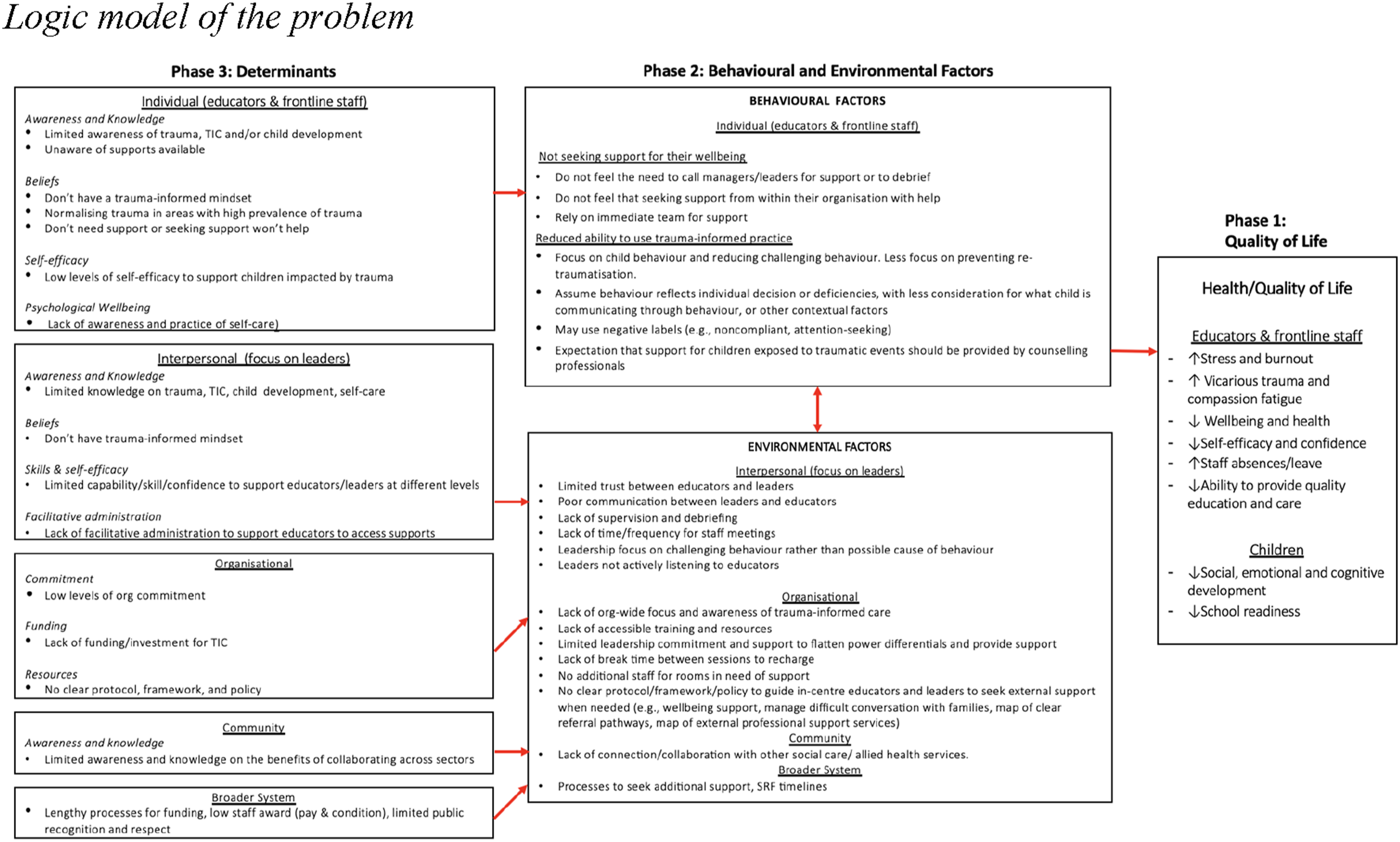
Tasks 3: Describe the context for the intervention
With the endorsement of the Steering Committee and Design Group, the priority population was determined as ECEC organisational leaders. Discussion with both groups suggest that the multiple leadership positions with diverse responsibilities situated within and out of ECEC centres adds to the complexity. For example, one insight from the qualitative inquiry was that long day care centres and sessional kindergartens need different forms of support to embed organisation-wide trauma-informed practices. In the first Steering Committee meeting, participants suggested that customisation is vital for the TIO intervention, highlighting the need for a relational approach that provides tailored support to tackle the challenges arising within the complex ECEC sector.
Task 4: Establish the program goal
The program goal identified with the Steering and Design Groups was “to promote experiences of safe and consistent support for everyone across ECEC services.”
Reflections
Benefits of IM in developing interventions for education settings
Intervention Mapping provides formal guidance for program developers to embed theory and research into the systematic design of programs for education professionals, who commonly draw on their tacit knowledge when engaging with children (O’Connor et al., 2017, 2019; Taylor, 2017). Currently, the extent to which interventions in education settings, including ECEC, draw on systematic, evidence-based approaches or incorporate lived experience voices is unclear, as studies rarely report their development processes (O’Connor et al., 2019). Similarly, within the realm of trauma-informed practice, interventions to support ECEC professionals to use a trauma-informed lens are growing (Sun, Blewitt, et al., 2023), however few studies describe the program development process in detail (e.g., Shamblin et al., 2016). For studies that report the development processes, descriptions are typically brief, and do not specify whether a systematic program development methodology or framework was used (e.g., Woods-Jaeger et al., 2018).
Guided by Intervention Mapping, knowledge gathered from diverse sources can be incorporated, which may lead to more cohesive, integrated, and meaningful plans for program implementation and evaluation (Fernandez et al., 2019). Several studies have highlighted that the first step of Intervention Mapping is the most time-consuming but critical to inform all subsequent steps (e.g., O’Connor et al., 2017). In the current study, the iterative process to generate and refine the Logic Model of the Problem, with the data from the systematic review, qualitative study, and consultation with the Steering Committee and Design Group was time- and resource-intensive. However, it enabled the meaningful integration of data from theory and research, by sharing the responsibility with stakeholders who have lived experiences and diverse perspectives (Bartholomew Eldredge et al., 2016). Valuing the community-based participatory approach, Intervention Mapping has the potential to (i) bridge knowledge hurdles between disciplines, such as social work, allied health, and education, and (ii) develop multi-level interventions tailored to the multi-level needs of the target population (e.g., early childhood educators, in-centre leaders, out-of-centre leaders, organisational leaders).
Challenges of using IM in developing an intervention for education
Making sense of the intervention Mapping vocabulary
One major challenge of using Intervention Mapping for this project related to its nuanced terminology and language. To build the Logic Model of the Problem, terms such as “determinants”, “behavioural factors”, and “environmental factors” can be unfamiliar to educational researchers and practitioners, creating barriers for internal communication in the development process which may prohibit program planners’ choice of this tool (Suzuki et al., 2012). The research team who included members experienced in Intervention Mapping, sought to build shared understandings of language with the Steering Committee and Design Group (Bird et al., 2021; Degotardi et al., 2022). For example, one researcher who is experienced in using Intervention Mapping guided the Design Group by explaining the Intervention Mapping vocabulary in plain language, and sharing examples of what each step looks like through case studies (i.e., the Cheshire Social-Emotional Engagement and Development (SEED) Educational Program; Blewitt et al., 2020). Depending on the sector/audience, developing more simplified, universal terminology would be beneficial in expanding access to this methodology; alternatively, it may be necessary to orient participants to Intervention Mapping throughout meetings to establish shared understanding and language.
Deficit-focuses versus strengths-based lens
As described earlier, Step 1 is deficit-focused, whereas education professionals often prefer strength-based framing. Wong and Press (2017) discussed the fundamental different paradigms between health and education, where health usually has a problem-based lens while education is more holistic and strengths-based. Ideological differences between health and education were a challenge for educational researchers who are new to Intervention Mapping, and for participants with a background in education who were engaged in the Steering Committee and Design Group. This was addressed through the development of a multidisciplinary research team with experience in both health and educational research and understanding of the philosophies of both disciplines; as well as deliberate efforts to meet participants where they were at, such as reframing terms using strengths-based language. For example, Steering Committee and Design Group members were consistently assured that comprehensively understanding the “problems” would support later program tailoring and therefore effectiveness.
Time and resources intensive
Intervention Mapping provides a systematic guiding framework for intervention development, and with such comprehensiveness comes the requirement of time and resources. The challenge of the time- and resource-intensiveness has been documented by previous co-design literature (e.g., Bird et al., 2021; Rogers et al., 2022). In our case, to form the Steering Committee and Design Groups whose membership reflects the experience- and skill-mix required, networks and connections were essential. This project’s industry partner, the Foundation, has long-established connections with ECEC services whose leaders are interested in trauma-informed practice and therefore see the benefits and significance of trauma-informed ECEC organisational change. Even with these existing connections, the journey from initial contact with over 16 organisations, to the first official meetings was lengthy. However, the time and resource investment paid off. Involving Steering Committee and Design Group members in iterative and deliberative sense-making and decision-making enhanced comprehensiveness, and collaboration with potential users maximised pragmatism and feasibility (Gray-Burrows et al., 2016). Meanwhile, the research team’s diverse methodological expertise was thoughtfully leveraged, with two members specialising in stakeholder engagement and participatory design, one member specialising in Intervention Mapping, and two members specialising in evidence synthesis and qualitative methodologies.
Recommendations
Despite its comprehensiveness and rigor, several limitations such as the ones described here may deter educational professionals’ use of the framework. To promote the utilisation of Intervention Mapping in education, a review of its vocabulary and terminology could increase accessibility and acceptability. For example, changing “quality of life” in the Logic Model of the Problem to “children’s learning and development”, and “behaviour” to “practice”. Training and resources to support the use of methodologies like Intervention Mapping can be developed and made accessible for educational program developers and/or researchers.
Future directions
After the completion of Step 1 (Logic Model of the Problem), program outcomes for each level will be established with the Design Group and Steering Committee. Using these outcomes, the Steering Committee and Design Group will be asked to articulate what change is required and what needs to be in place for this to occur. These will be presented visually in Change Matrices which will further help with selection and design of intervention activities and strategies.
Drawing on the change matrices, the program will be designed in Step 3 (program design). In this step, program content will be identified, including “components, scope, sequence, theory-and evidence-based methods and practical applications” (Bartholomew Eldredge et al., 2016, p. 345). Behavioural change theory will be used to inform methods and applications that are embedded within the intervention. Ultimately, the design will be discussed and voted by the Design Group and the Steering Committee. In Step 4, the research team will develop the intervention components using the data gathered through Step 1 – 3 with the Design Group. Once it has been developed, a pilot study will occur to gauge the feasibility of the program and make the refinements based on the reflections and findings. A program implementation plan (Step 5) and evaluation plan (Step 6) will then be developed.
Conclusion
To the authors' knowledge, this is the first study using Intervention Mapping to develop a trauma-informed program for education settings. This article describes how Step 1 of the framework was utilised to understand the needs of the ECEC sector to support organisation-wide trauma-informed practice. This study provides an example of how Intervention Mapping can support the development of evidence-based interventions that are tailored to the needs of the stakeholders. The reflections of how the research team operationalised Intervention Mapping, including enablers and barriers, and recommendations may inform future educational researchers to apply this practical and effective program development methodology.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.