
Abstract
Hikikomori was included in the chapter “Culture and Psychiatric Diagnosis” of the DSM-5-TR Section III as an example of cultural concepts of distress. However, attempts over time to better define hikikomori emphasized different specific characteristics/criteria. The present study aimed to provide an overview of different criteria and definitions of hikikomori, and to examine whether hikikomori resembles social anxiety/phobia (and avoidant personality), depression, and adjustment and stress disorders. This narrative review followed available recommendations on reporting standards. A structured literature search was conducted in PubMed, MEDLINE, PsycINFO, PsycARTICLES, Web of Science, and Scopus on May 31, 2023. Hikikomori definitions and criteria diverge in their focus on specific criteria such as not working/attending school, avoidance/refusal of and disinterest/unwillingness to participate in social situations and relationships. Hikikomori resembles a (severe) variant of social anxiety disorder, a form of adjustment disorder, or a variant of depressive disorder, depending on the criteria in use. Empirical evidence on the clinical validity of some hikikomori definitions is scarce. If hikikomori criteria do not include indicators of dysfunction, the condition under study may reflect severe/extreme social isolation rather than a different diagnostic category. Updated hikikomori research criteria were proposed to foster future studies addressing diagnostic validity and clinical comorbidity. Alternatively, a “with (social) withdrawal” specifier in the definition of social anxiety, depressive, and adjustment and stress disorders should be considered. Finally, the inclusion of hikikomori in the DSM-5-TR was discussed.
Public health significance statements
Scientific evidence on the clinical validity of some hikikomori definitions is mainly lacking.
If no indicator of psychological dysfunction is included among the criteria for hikikomori, the condition may simply constitute severe/extreme social isolation, rather than a different diagnostic category.
The inclusion of a “with (social) withdrawal” specifier in the definition of social anxiety, depressive, and adjustment and stress disorders could be considered.
Introduction
Hikikomori is a psycho-social condition characterized by extreme social isolation and withdrawal that has attracted scientific attention worldwide (American Psychiatric Association, 2022; Teo & Gaw, 2010). The most recently proposed definition posits that marked social isolation at home, withdrawal duration of at least six months, and significant impairment or distress associated with social isolation are core criteria of the condition (Kato et al., 2019, 2020). However, there have been several attempts over time to better define hikikomori. Specifically, avoidance, disinterest, or unwillingness to attend school/work and to participate in social relationships/interactions, as well as the absence of other primary mental disorders have been considered core criteria of hikikomori (Japanese Ministry of Health, Labour and Welfare, 2003; Koyama et al., 2010; Saitō, 1998; Teo & Gaw, 2010). Previous research proposed the inclusion of hikikomori in the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) as a culture-bound syndrome (Teo & Gaw, 2010). In line with that proposal, the condition has been recently described under the paragraph “Examples of Cultural Concepts of Distress” in the chapter “Culture and Psychiatric Diagnosis” of the DSM-5-TR Section III “Emerging Measures and Models” (American Psychiatric Association, 2022). A review of hikikomori definitions might thus help in distinguishing hikikomori from social isolation due to other conditions (e.g., chronic physical illness, physical-medical condition), avoiding over-pathologization (Amendola, 2023), and correctly interpreting research findings employing different conceptualizations of hikikomori (Nonaka et al., 2022). Furthermore, recent studies (Amendola & Cerutti, 2023; Kato et al., 2023; Teo et al., 2023) have suggested examining symptoms of hikikomori “during the last month” rather than “during the last six months” increasing the risk of confounding hikikomori with other conditions (i.e., considering hikikomori present when, in fact, the symptoms might primarily be due to other conditions).
The scientific debate on the “position” of hikikomori in mental health and its validity as a separate diagnostic entity is ongoing (Amendola, 2023; Amendola & Cerutti, 2022; Kato et al., 2012; Nonaka et al., 2022; Suwa & Suzuki, 2013; Tajan, 2022; Tateno et al., 2012). Benarous et al. (2022) synthesized the main conceptual models for the characterization of hikikomori in current psychiatric classifications. The authors distinguished what they label “strictly medical,” “sociological,” and “medical-anthropological” approaches. Hikikomori would be a component of a pre-existing psychiatric disorder according to the medical approach, a maladaptive reaction of distress according to the sociological approach, and an “atypical expression of psychiatric symptoms (such as anxiety and depression)” according to the medical-anthropological approach (Benarous et al., 2022) (p. 3). However, a critical discussion of hikikomori definitions was not provided.
Different contributions reviewed Japanese-specific historical and cultural factors possibly involved in hikikomori emergence such as the concept of amae (a culturally accepted relationship overdependence between children and parents) (Kato et al., 2019; Teo et al., 2013; Umemura et al., 2018), rigid educational systems (Furlong, 2008), labour market change resulting in a depressed economy (Furlong, 2008; Kato et al., 2011; Suwa & Suzuki, 2013), shame-prone and socio-phobic behaviours (Okano, 1994; Teo, 2010), and motivational factors (Cerutti et al., 2021). However, initially reported in Japan, hikikomori has been described worldwide (Amendola & Cerutti, 2022; Chauliac et al., 2017; Frankova, 2019; Kato et al., 2012; Malagón-Amor et al., 2010; Ranieri, 2018). It may thus represent a consequence of a modern lifestyle and a globally interconnected society (Furlong, 2008; Kato et al., 2011; Suwa & Suzuki, 2013). The development of information technology, based on indirect communication and play, may have influenced the worldwide emergence of hikikomori (Kato et al., 2019; Suwa & Suzuki, 2013). Prevalence estimates resulting from large/representative samples and epidemiological studies range from 1.1% to 6.7% (Amendola, Cerutti, & von Wyl, 2023; Fong et al., 2023; Koyama et al., 2010; Tajan et al., 2017; Uchida & Norasakkunkit, 2015; Umeda et al., 2012; Wong et al., 2015; Yong et al., 2020; Zhu et al., 2021) with this variability potentially due to methodological factors such as sampling procedure and hikikomori definition used (Amendola, 2023; Nonaka et al., 2022).
Previous research on the view of mental health professionals about hikikomori showed that more than 90% of two Japanese samples of paediatricians (N = 26) and psychiatrists (N = 80) chose an underlying psychiatric disorder as the most applicable diagnosis of hikikomori according to the ICD-10 (Tateno et al., 2012). Specifically, most paediatricians indicated “neurotic, stress-related, and somatoform disorders” (50%), while psychiatrists preferred “schizophrenia, schizotypal, and delusional disorders” (30%) (Tateno et al., 2012). Only about 8% of psychiatrists and paediatricians had no idea about what available diagnostic category could be applied to hikikomori (Tateno et al., 2012). Another study (Kato et al., 2012), published in the same year, showed a different result indicating that around 55% of a sample of Japanese psychiatrists (N = 123) believed that an ICD-10 or DSM-IV diagnosis could not be applied to two hikikomori vignette cases. However, the limitations of using clinical vignettes have recently been discussed in hikikomori research, in particular the typification of an ideal type of hikikomori that represents only a minority of the cases (Tajan, 2022).
Furthermore, many hikikomori symptoms are non-specific and can be found across various conditions leading to difficulty when a differentiation between hikikomori and the early stage of other psychiatric disorders needs to be made (Stip et al., 2016). Similarities and differences between social withdrawal due to hikikomori, schizophrenia, autism, and technological addictions have been already discussed (Amendola, Cerutti, & Presaghi, 2023; Kato et al., 2019; Muris & Ollendick, 2023; Stip et al., 2016). Recently, Muris and Ollendick (2023) suggested that, in schizophrenia and autism, hikikomori appears to be an extreme variant of pathognomonic symptoms of the disorder; whereas in social anxiety disorder and depression, it may be a consequence of the disorder.
Study aims
In light of the above, the present narrative review aimed at improving the debate on the hikikomori condition providing an overview of and clarification on the definitions and criteria of hikikomori proposed and used in the scientific literature. Specifically, the first aim was to focus on different criteria and definitions of hikikomori to provide a more complete and clear picture of to what hikikomori refers. Whether hikikomori fits with the current DSM-5-TR definition of mental disorder or not was considered. The second aim was to examine whether hikikomori resembles other mental health disorders. Differences and similarities between hikikomori and social anxiety/phobia (and avoidant personality), depression, and adjustment and stress disorders were analysed to fill a gap in the literature.
Methods
This narrative review was performed following previous recommendations on standards for reporting of narrative reviews (Baethge et al., 2019; Byrne, 2016; Gasparyan et al., 2011; B. N. Green et al., 2006; Kable et al., 2012; Pautasso, 2013). The conduction of a narrative literature review was preferred over a systematic review due to its flexibility in dealing with broader issues, evolving knowledge, and concepts, benefiting from the analysis of different types of scientific contributions (e.g., previous reviews, viewpoints and commentaries, case reports, and empirical articles).
Literature search
The electronic databases of PubMed, MEDLINE, PsycINFO, PsycARTICLES, Web of Science, and Scopus were searched (in “all fields” except Scopus which was searched in “title, abstract, keywords”) for retrieving useful articles—informing the review—published until May 31, 2023, using the following keywords: hikikomori AND (“social anxiety” OR “social phobia” OR “avoidant personality”); hikikomori AND (depression OR depressive*); hikikomori AND (“adjustment disorder*” OR “stress disorder*”).
Study selection
The presence of possible duplicates in the obtained pool of records was separately examined for each search strategy using Zotero 6.0.26 for Windows. Subsequently, full-text screening was directly performed rather than screening titles and abstracts. The full-text-assessment occurred in June 2023. The eligibility criteria were studies analysing definitions and criteria of hikikomori as well as the relationship between hikikomori and social anxiety, avoidant personality, depressive, and adjustment and stress disorders. The study selection process is shown in Figure 1. A total of 108 full texts were selected to inform the review. Other scientific articles of which existence the author was aware of were also used. Articles published in English, French, Spanish, and Italian were considered.
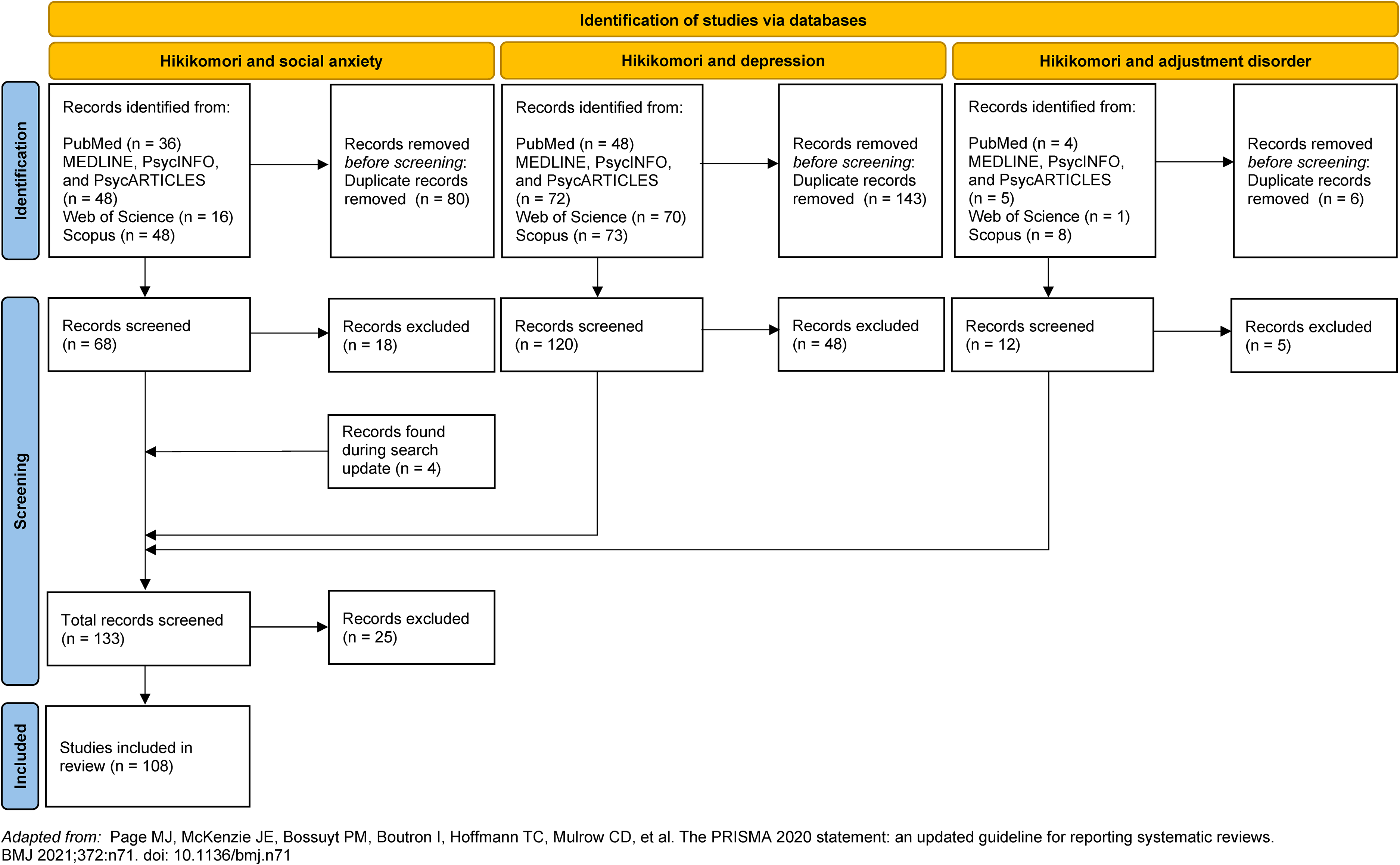
Adapted PRISMA flow diagram.
Study presentation and analysis
Hikikomori definitions and criteria were first described, and then they were examined according to the current DSM-5-TR definition of mental disorder. Subsequently, studies were grouped and discussed according to the main psychological symptom considered in the hikikomori definition and the mental disorder analysed. Specifically, studies including “refusal or avoidance of social situations and social relationships” as a criterion of hikikomori were examined when discussing similarities and differences between hikikomori and social anxiety, while those analysing “no interest or willingness to attend school or work” were considered particularly useful for discussing the association between hikikomori and depression. Then, studies on the relationship between hikikomori and trauma- and stressor-related disorders were addressed. The presentation was structured according to whether a categorical or dimensional approach was used for hikikomori evaluation to improve clarity in interpreting results and differentiate comorbidity—based on hikikomori definition and with a focus on the co-occurrence of hikikomori with the mental disorders of interest—from symptoms association – based on the use of hikikomori questionnaires and correlations between symptoms.
Results
Similarities and differences across definitions and criteria of hikikomori proposed over time
The definitions of hikikomori proposed over time are reported in Table 1.
Definitions and criteria of hikikomori
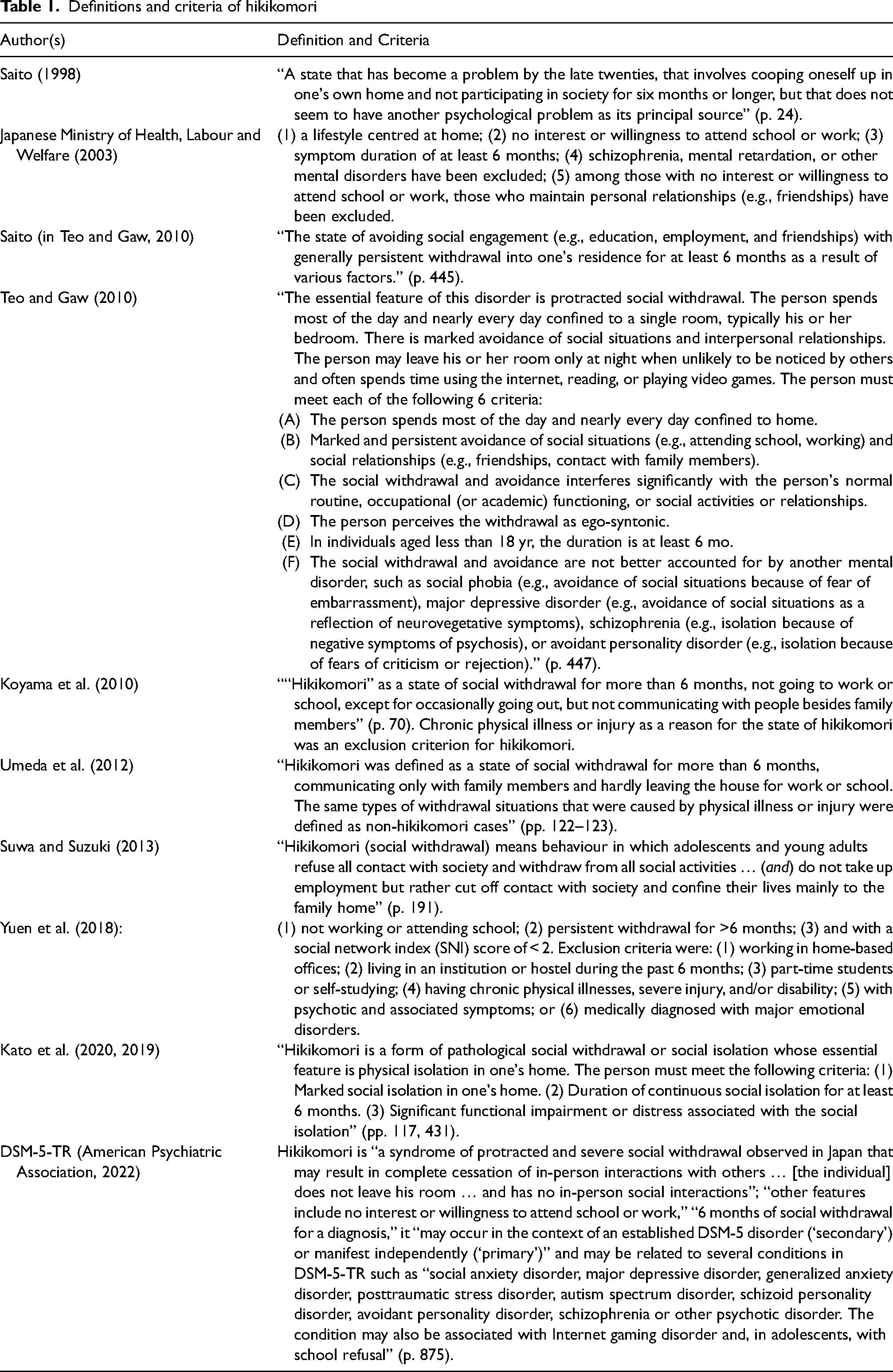
Regarding similarities, some criteria have consistently been proposed across definitions, that is, lifestyle centred at home, symptom duration of at least 6 months, and significant impairment and/or distress caused by the condition (i.e., it interferes with the person's normal routine, occupational/academic functioning, or social activities or relationships). Furthermore, all proposals included as a criterion lack of participation in society, no interest or willingness to attend school or work, and refusal or avoidance of social situations (e.g., attending school, working) and social relationships (e.g., friendships, contact with family members) with some exception (Kato et al. (2019, 2020)).
On the other hand, the proposals differ in considering the need to exclude other mental health disorders and/or medical conditions for diagnosing hikikomori. Some authors advised the exclusion of other mental disorders and/or medical conditions for hikikomori to be present (Japanese Ministry of Health, Labour and Welfare, 2003; Koyama et al., 2010; Teo & Gaw, 2010; Umeda et al., 2012; Yuen et al., 2018) whereas others did not consider those as an exclusion criterion of hikikomori (American Psychiatric Association, 2022; Kato et al., 2019; Saitō, 1998; Suwa & Suzuki, 2013). According to the latter view, hikikomori is regarded as a different psychiatry entity or a disorder that tends to co-occur with other conditions.
What does hikikomori refer to according to the different proposals?
Hikikomori could be better understood as an objective behavioural indicator of impairment/distress—possibly resulting from a psychosocial dysfunction—rather than a different psychiatric entity based on the definition of hikikomori proposed by Kato et al. (2019, 2020). In fact, no clear and valid (symptom of) dysfunction is mentioned among the proposed criteria (Amendola, 2023; Amendola, Cerutti, & von Wyl, 2023). The definition of mental disorder in the DSM-5-TR requires both the presence of symptoms that are manifestations of “a dysfunction in the psychological, biological, or developmental processes underlying mental functioning” and “significant distress or disability in social, occupational, or other important activities” (American Psychiatric Association, 2022) (p. 14). Marked physical isolation associated with significant impairment/distress may not be caused by an underlying psychological dysfunction but result from stressful events, adverse social/environmental conditions, physical or medical conditions, or because of mental health problems. The presence of a psychological dysfunction cannot be inferred from marked physical isolation only (i.e., it is a general symptom). Therefore, defined as a prolonged marked physical isolation in one's own home causing impairment/distress, hikikomori may better represent a negative outcome/consequence or harm—corresponding to severe/extreme social isolation—rather than a different diagnostic category. As such, it may be associated with different psychosocial factors and symptoms/disorders (Amendola et al., 2021; Hayakawa et al., 2018; Kato et al., 2019; Katsuki et al., 2019; Setoyama et al., 2022; Zhu et al., 2021).
Recognized that marked physical isolation in one's own home may be considered a general symptom more indicative of harm or negative outcome/consequence and distress, may its presence be an indicator of severity (i.e., of a more severe condition)? A possible way to answer this question is to examine findings of studies comparing participants from the same population with and without hikikomori—defined as marked physical isolation at home for at least six months—in comorbidity. Findings from five studies mainly involving patients with major depression associated with or without hikikomori and conducted in Japan provide valuable information. Katsuki et al. (2019) compared adult participants mainly with a diagnosis of depressive disorder with and without hikikomori. Participants with a psychiatric diagnosis associated with hikikomori showed higher scores of avoidant, depressive, narcissistic, paranoid, passive-aggressive, schizoid, and schizotypal personality traits compared to participants with a psychiatric diagnosis not associated with hikikomori, as expected (Katsuki et al., 2019). In a subsequent study, with mostly overlapping recruitment periods to the previous one, the authors (Katsuki et al., 2020) compared adult patients with hikikomori to those without it. Findings showed that patients with hikikomori scored higher on symptoms of preference for solitude, loneliness, depression, and autistic traits and lower on social support compared to patients without hikikomori (Katsuki et al., 2020). In a third study from the same research group (Kyuragi et al., 2023), with mostly overlapping recruitment periods to the previous studies, adult patients with major depression with hikikomori reported higher scores of loneliness compared to depressed patients without hikikomori. Similarly, a fourth study (Teo et al., 2020) compared two groups of adult patients with major depression associated with and without hikikomori. Patients with hikikomori showed higher functional impairment/distress as indicated by prior episodes of depression (despite no difference in mean age), higher loneliness and suicidal ideation, and lower frequency of leaving home, compared to patients without hikikomori. Finally, a fifth recent study (Yamada et al., 2023) compared adult patients with autism in association with and without hikikomori. As for previous studies, the presence of hikikomori was associated with higher depressive and anxiety symptomatology.
Taken together these findings are consistent with the notion that marked and prolonged physical isolation in one's own home could be a consequence or an indicator of a more severe symptomatology irrespective of the mental health disorder that would cause it (at least according to the results from these studies mainly conducted with samples of depressed and autistic patients).
Other definitions of hikikomori specified symptoms potentially reflecting an underlying dysfunction among the criteria for the condition, supporting its potential status as a different psychiatric entity. Specifically, other definitions included:
not participating in society (Saitō, 1998); no interest or willingness to attend school or work and not maintaining personal relationships (e.g., friendships) (Japanese Ministry of Health, Labour and Welfare, 2003); marked and persistent avoidance of social situations (e.g., attending school, working) and social relationships (e.g., friendships, contact with family members) (Teo & Gaw, 2010); refusal of all contact with society and withdrawal from all social activities (Suwa & Suzuki, 2013); not going to work or school, except for occasionally going out, but not communicating with people besides family members (Koyama et al., 2010).
Like marked physical isolation in one's own home (discussed in the previous paragraph), not participating in society (e.g., work, school) or not going to work/school is an objective behavioural indicator of impairment/distress and may represent harm or negative outcomes/consequences rather and/or better than an underlying specific dysfunction in the psychological, biological, or developmental processes underlying mental functioning. Consequently, it is not surprising that it is associated with (symptoms of) different mental health disorders such as anxiety, depression, and autism in samples of young and adult participants (Bowker et al., 2019; Costa et al., 2019; Ferrara et al., 2020; Hamasaki et al., 2021; Imai et al., 2021; Koyama et al., 2010; Umeda et al., 2019).
On the other hand, no interest or willingness to attend school or work, and not maintaining personal relationships as well as refusal or avoidance of social situations (e.g., attending school, working) and social relationships (e.g., friendships, contact with family members) may be psychological manifestations or indicators of underlying dysfunctions. These psychological symptoms were considered core criteria of hikikomori (Japanese Ministry of Health, Labour and Welfare, 2003; Suwa & Suzuki, 2013; Teo & Gaw, 2010) besides confinement at home, duration of at least six months and significant impairment and/or distress. The inclusion of such psychological symptoms and indicators in hikikomori definitions highlights some characteristics common to hikikomori and other conditions mainly belonging to the category of anxiety disorders, depressive disorders, and trauma- and stressor-related disorders. Therefore, scientific articles were grouped and discussed in different sections according to the main psychological symptom considered in the hikikomori definition and the mental disorder examined (see also “Study presentation and analysis” paragraph).
Is hikikomori a (severe) variant of social anxiety disorder?
Many authors highlighted the need to consider anxiety disorders when evaluating an individual whose symptomatology resembles hikikomori (Aguglia et al., 2010; Cerniglia et al., 2017; Japanese Ministry of Health, Labour and Welfare, 2003; Teo & Gaw, 2010; Yuen et al., 2018) while others emphasised similarities between social anxiety (Martinotti et al., 2021; Piotti, 2022), school phobia/refusal and hikikomori (Boë, 2020; Guiavarc’h, 2020; Piotti, 2022; Suzuki, 2020).
Avoidance of social situations that provoke marked fear or anxiety is indicative of social anxiety disorder and individuals with social anxiety disorder may live at home longer (Amendola, Cerutti, & von Wyl, 2023; American Psychiatric Association, 2022). Accordingly, “anxiety in social interactions may precipitate hikikomori” (p. 429) (Kato et al., 2019). One may thus wonder whether the strong relationship shown between social anxiety and avoidant personality disorder also applies to social anxiety disorder and hikikomori (Amendola, Cerutti, & von Wyl, 2023).
Refusal or avoidance of social situations and social relationships as well as social isolation may bring together social anxiety disorder and hikikomori. Narcissistic traits, shame, and technology use could increase the risk of both social anxiety and hikikomori (Piotti, 2022). Furthermore, Guiavarc’h (2020) stressed how the term hikikomori underlines “the impossibility for these young people to establish relationships with others” and that “this absence of social relations is not only limited to work or school” (p. 47), according to Fujiya Tomita.
In line with the above, Nagata et al. (2013) suggested that hikikomori could be a severe form of social anxiety disorder. The authors retrospectively analysed data from adult patients with a primary diagnosis of social anxiety disorder referring to an outpatient clinic during seven years. They found that 19% of patients with social anxiety disorder fulfilled the criteria for hikikomori. These patients had significantly earlier hikikomori onset, worse symptoms, less formal education, and were more likely to suffer from obsessive-compulsive disorder. However, the hikikomori definition applied by the authors included “no interest in going to school or working and not maintaining personal relationships” rather than “refusal or avoidance of social situations and social relationships” and, as such, the observed frequency could be an underestimation of the true frequency of hikikomori in patients with social anxiety disorder.
Studies using a categorical approach
Among studies including “refusal or avoidance of social situations and social relationships” as a hikikomori criterion, Kondo et al. (2013) showed that most young adult hikikomori referring to mental health centres in Japan had psychiatric problems, in particular, schizophrenia, anxiety and mood disorders, developmental disabilities, and personality problems. Of those diagnosed with hikikomori, 30.7% (50 out of 163 for whom a diagnosis was available) showed anxiety disorders. Similarly, Lee et al. (2013) analysed adolescents and young adults with hikikomori referred by community mental health centres and psychiatric clinics. Anxiety disorder (especially social anxiety and generalized anxiety disorder) was among the most common major or comorbid mental disorders with an overlapping frequency higher than 30%. Among others were oppositional defiant disorder, depression, and attention deficit hyperactivity disorder.
Teo et al. (2015) examined a sample of adult US and Japanese hikikomori showing a high frequency of social anxiety and avoidant personality disorders in comorbidity, of 27% and 41%, respectively. While depression was observed in 32% of cases.
Regarding findings of studies conducted in other Western countries, Malagón-Amor et al. (2015, 2018) analysed a group of Spanish adults treated at home because of social withdrawal. The authors demonstrated that premorbid dysfunction was high, that is, 74.5% had a personal psychiatric history, with psychotic, anxiety and affective disorders being the most frequent (Malagón-Amor et al., 2015). Psychosis, anxiety, and affective disorders were the most prevalent comorbid disorders at that moment as well, and only a few cases had no symptoms suggestive of mental disorder (Malagón-Amor et al., 2015). Anxiety disorders were present in 23–25% of cases. The authors concluded that hikikomori is not a new psychiatric disorder since nearly all cases showed a psychiatric disorder justifying the isolation. On the contrary, hikikomori without another psychiatric disorder in comorbidity would be rare (Malagón-Amor et al., 2015).
Another study conducted in Ukraine by Frankova (2019) analysed adult inpatients or outpatients with hikikomori referring to a mental health department during three years. The author found that two-thirds of hikikomori cases had neurotic, somatoform, or stress-related disorders in comorbidity while in one-third no comorbid condition was present. Of those cases with a comorbid diagnosis, 40.9% (29% if both hikikomori with and without comorbidity were considered) showed an anxiety disorder (13.7% social phobia; or, as above, 9%) and 36.4% a trauma- or stress-related disorder (or, as above, 23%). The two hikikomori groups did not differ on anxiety, dysthymia, negativism, number and impact of traumas, and quality of life. On the contrary, differences between those groups and a control group were mainly significant.
Recently, Benarous et al. (2022) retrospectively analysed hikikomori based on Teo and Gaw's (2010) criteria in a French sample of adolescent inpatients consecutively admitted in two inpatient units during two years. The authors reported that, at admission, 7% met hikikomori criteria, one out of six adolescents with social withdrawal and/or school refusal. Youths with hikikomori did not significantly differ from those with social withdrawal and/or school refusal in terms of demographic factors, academic performance, or psychosocial factors. Remarkably, at discharge, all inpatient adolescents with hikikomori had a diagnosis of anxiety disorder (100%), especially performance anxiety, and depressive disorder was also frequent (64%). Adolescents with hikikomori had a longer duration of symptoms, longer hospitalization, and required more daily care facilities at discharge compared to adolescents with anxiety disorder. The authors concluded that their findings support the notion that hikikomori represents an atypical pattern of psychiatric symptoms (anxiety and depression) associated with family and social factors. Passivity and avoidance of feared situations were viewed as two relevant clinical dimensions of the condition (Benarous et al., 2022).
Another recent study conducted in France (Hamasaki et al., 2022) analysed differences between psychiatric outpatients aged 12–15 years with hikikomori and a healthy control group. The hikikomori group scored higher than the healthy group on all subscales of the Child Behavior Checklist.
Bellini et al. (2023) explored differences between two groups of Italian adolescent patients, one presenting social withdrawal and the other suffering from anxiety or depressive symptoms. They used Teo and Gaw's (2010) hikikomori diagnostic criteria. No between-group difference was shown in socio-demographic variables and symptoms of anxiety, depression, and loneliness. A unique meaningful difference was found in the results of the clinical interview showing that participants of the hikikomori group were more likely (50% against 13.6%) diagnosed with social phobia compared to the group of anxious/depressed. The authors noted that hikikomori is mainly associated with anxiety and mood disorders. However, 31.8% of the hikikomori group did not meet the criteria of any disorder included in the DSM-5. Finally, the clinical severity of patients with hikikomori was comparable to that of patients with anxiety/depression.
Studies using a dimensional approach
Overall, previous studies showed a significant association between symptoms of hikikomori and symptoms of anxiety both in clinical and non-clinical samples of adolescents and young adults (Amendola et al., 2022b; Amendola, Cerutti, & Presaghi, 2023; Lin et al., 2022) with few exceptions (Amendola et al., 2021) probably due to methodological limitations such as reduced sample size influencing power to detect a significant effect.
Is hikikomori a variant of depressive disorder?
Similar to anxiety disorders, the need to exclude depressive disorders before considering a diagnosis of hikikomori has been encouraged (Aguglia et al., 2010; Japanese Ministry of Health, Labour and Welfare, 2003; Teo & Gaw, 2010; Yuen et al., 2018).
No interest or willingness to attend school or work and not maintaining personal relationships as a psychological symptom of hikikomori represent an aspect in common with depressive disorders. Diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day is listed as one of the diagnostic criteria for major depressive disorder in the DSM-5-TR (American Psychiatric Association, 2022) and may also be the main symptom for diagnosing an unspecified or other specified depressive disorder (i.e., depressive episode with insufficient symptoms) (Kaiya, 2018; Kato & Kanba, 2018). In depressive disorders, the individual may avoid leaving home because of apathy, loss of energy, low self-esteem, and anhedonia (American Psychiatric Association, 2022; Kato et al., 2019). Likewise, some scholars identified apathy and no interest in the world as the main characteristics of hikikomori (Aguglia et al., 2010; Saitō, 1998). Aguglia et al. (2010) pointed out that social anxiety could be diagnosed rather than hikikomori. However, the authors considered that apathy and no interest in the world is the main characteristic of hikikomori that differentiates it from social anxiety: social situations would be avoided not because of fear or anxiety of negative evaluations but because of apathy.
Studies using a categorical approach
Unfortunately, the literature search found no study analysing the association between depressive disorders and hikikomori defined as also including the criteria of no interest or willingness to attend school or work and not maintaining personal relationships.
Studies using a dimensional approach
Previous studies showed a significant association between symptoms of hikikomori and symptoms of depression in both community (Amendola et al., 2022b; Amendola, Cerutti, & Presaghi, 2023; Hihara, Kambara, et al., 2022; Kubo et al., 2022; Liew et al., 2021; Lin et al., 2022) and clinical samples (Fino et al., 2023) of young people and adults, whereas non-significant associations were also pointed out (Amendola et al., 2021; Fino et al., 2023).
Is hikikomori a form of adjustment disorder?
Most authors agree on the need to consider and/or exclude schizophrenia and/or personality disorders before diagnosing hikikomori (Aguglia et al., 2010; Costa et al., 2019; Ferrara et al., 2020; Japanese Ministry of Health, Labour and Welfare, 2003; Teo & Gaw, 2010; Yuen et al., 2018). Similarly, scholars (Koyama et al., 2010; Umeda et al., 2012; Yuen et al., 2018) discussed that chronic physical illness or injury as a reason for the state of hikikomori should be judged as an essential exclusion criterion of hikikomori. This could help to avoid the risk of an erroneous hikikomori diagnosis when prolonged home-based physical isolation is triggered and/or follows a stressful or adverse event. A diagnosis of adjustment disorder could be appropriate in such cases accompanied by inappropriate emotional symptoms and significant impairment. According to the DSM-5-TR, it could be additionally specified whether anxiety and/or depressive symptoms are predominant and an additional specification including with (social) withdrawal or work/academic inhibition (American Psychiatric Association, 1987; Patra & Sarkar, 2013) (“unspecified” elsewhere (American Psychiatric Association, 2000, 2022)) might be usefully applied to hikikomori showing mild/moderate anxiety and/or depressive symptoms but for whom a stressful or adverse event may be identified as the main cause of the withdrawal behaviour.
The possibility that adjustment disorder could take the form of social withdrawal and mimic a hikikomori condition should thus be considered (Amendola, Cerutti, & von Wyl, 2023; Ungvari & Hantz, 1991b). As described in detail below, stressful or humiliating experiences (e.g., bullying) may exert a major role in leading to hikikomori (Tajan, 2017, p. 201) but also to the onset of both social anxiety and avoidant personality disorder (American Psychiatric Association, 2022). In adjustment disorders, the stressor can be of any severity or type and the emotional or behavioural symptoms in response to an identifiable stressor occur within three months of the onset of the stressor (American Psychiatric Association, 2022). In addition, the definition includes marked distress that is out of proportion to the severity or intensity of the stressor and significant impairment (American Psychiatric Association, 2022).
Studies using a categorical approach
Current knowledge indicates that hikikomori is associated with stressful or adverse events in general (Amendola & Cerutti, 2022; Frankova, 2019; Lee et al., 2013; Muris & Ollendick, 2023; Tajan et al., 2017; Wong et al., 2015) rather than childhood traumatic experiences specifically (Umeda et al., 2012). Lee et al. (2013) analysed adolescents and young adults with hikikomori referred by community mental health centres and psychiatric clinics. The authors found that 54.3% of the hikikomori group reported experience of neglect, rejection, or bullying, compared to 13.4% of a healthy control group of students. Furthermore, 17.1% of the hikikomori group thought that bullying had directly caused their social withdrawal, and post-traumatic stress disorder from school bullying or caretaker violence was not infrequent (Lee et al., 2013). Teo et al. (2015) found a prevalence of post-traumatic stress disorder of 27% in adult hikikomori. Similarly, Frankova (2019) found that 36.4% of adult hikikomori cases with a comorbid condition (23% if the two hikikomori groups, with and without comorbidity, were considered as a whole) showed a trauma- or stress-related disorder, that is, 22.7% (or, as above, 14%) adjustment disorder and 13.7% (or, as above, 9%) post-traumatic stress disorder. The author highlighted that “in reality, however, in both primary and secondary hikikomori cases, there was a high frequency of past traumatic and life adverse events, which prevented them from overcoming the challenges” typical of young adulthood (p. 5). Indeed, both the number and impact of traumatic events were higher in hikikomori groups compared to the control group. Some examples of adverse events were emotional disturbances of significant others, parental divorce, and emotional insult or neglect. The observed associations between negative life events, such as those related to job, relationships with colleagues, friends, and classmates, being bullied by others, and hikikomori have been confirmed by other studies (Krieg & Dickie, 2013; Wong et al., 2015).
The importance of stressors for the emergence of social withdrawal behaviours and hikikomori is also evident in the description of some clinical cases of adolescents and adults (see for example Gondim et al., 2017; Malagón-Amor et al., 2010; Roza et al., 2020; Silić et al., 2019; Souilem et al., 2019; Stip et al., 2016).
These findings are in line with the conceptualization of hikikomori as a reaction to stressful social situations (Kato et al., 2019; Komori et al., 2019). Stressful or adverse events and/or what is perceived as such, in the presence of social anxiety, interpersonal/rejection sensitivity, and/or dysfunctional communication, may lead to hikikomori (Kaiya, 2018; Kato & Kanba, 2017; Lee et al., 2013; Piotti, 2022; Saitō, 1998; Suwa et al., 2003; Suwa & Suzuki, 2013; Tajan et al., 2017). Therefore, the possibility of a diagnosis of adjustment disorder rather than hikikomori or that hikikomori represents a specific form of adjustment disorder with withdrawal should be examined. Paying attention to personal history, vulnerabilities, and withdrawal reasons could improve scientific knowledge on the relationship between hikikomori and adjustment disorder.
Studies using a dimensional approach
In line with the above, a recent study found a significant association between symptoms of hikikomori and stress in a community sample of young adults (Lin et al., 2022).
Hikikomori as social breakdown
The study of individuals who are housebound or spend little time away from home is not new (Guedj-Bourdiau, 2011; Rapp, 1984). Stressful events generally precede another condition characterized by social withdrawal and physical isolation at home, the Social Breakdown or Diogenes syndrome. The syndrome is characterized by extreme self-neglect, passive accumulation of rubbish, and social withdrawal/living reclusively (Belcher & Rife, 1989; Gruenberg, 1982; Proctor & Rahman, 2021, 2022; Ungvari & Hantz, 1991a). Interestingly, overlapping characteristics between this syndrome and hikikomori are evident in some reports of clinical cases describing poor hygiene in hikikomori (Moriuchi et al., 2015) and social avoidance in Diogenes syndrome (Biswas et al., 2013; Camps & Le Bigot, 2019; Proctor & Rahman, 2021) in adulthood. According to some authors, the condition could be best classified as an adjustment disorder with profound social withdrawal (Ungvari & Hantz, 1991a, 1991b). These authors (Ungvari & Hantz, 1991b)—applying the Jaspersian concept of personality development—suggested that adjustment disorder could be understood as a form of “personality development” and the social breakdown “as a slow development of the personality in response to a difficult life situation, which was becoming increasingly complex and overwhelming to the individual” (p. 447). In accordance with other scholars (Amendola et al., 2021, 2022a; Amendola & Cerutti, 2022; Hihara, Kambara, et al., 2022; Hihara, Sugimura, et al., 2022; Piotti, 2022), overall personality (dys)functioning may define a condition of vulnerability while stressful or adverse events may represent precipitating factors for the emergence of hikikomori, especially during specific developmental phases. The potential role of attachment and inhibition of exploration was also suggested (Krieg & Dickie, 2013; Umemura et al., 2018).
Discussion
The present review debated the potential nosographic classification of hikikomori discussing its criteria, whether it is a clinical entity to be defined within already known categories or could represent a new different psychopathological entity.
Several definitions of hikikomori (Japanese Ministry of Health, Labour and Welfare, 2003; Suwa & Suzuki, 2013; Teo & Gaw, 2010) emphasized the importance of social withdrawal/avoidance and/or refusal of social participation and interactions. Further, clinicians and researchers underscored the need to distinguish primary and secondary hikikomori. Other definitions (Kato et al., 2019, 2020) deemed hikikomori as a trans-diagnostic condition equated with a severe form of social isolation (regardless of psychological tendencies of social withdrawal and avoidance). Yet others (Koyama et al., 2010; Saitō, 1998) were not specific in defining hikikomori psychological characteristics when indicating not participating in society (e.g., not working, not being in education) as a symptom of hikikomori.
Notably, the current scientific knowledge does not exclude that hikikomori could be a sociological problem rather than a separate diagnosis and a new way of expressing distress in an interconnected society (Amendola, Cerutti, & Presaghi, 2023; Amendola et al., 2021, 2022a; Cerutti et al., 2021; Furlong, 2008; Kato et al., 2011, 2019; Piotti, 2022; Suwa & Suzuki, 2013). In line with this, the present narrative review of the literature indicated that if hikikomori simply corresponds to a severe form of social isolation (i.e., home-based physical and social isolation), it represents a behavioural symptom common to many disorders and there would be no need for a new diagnosis since it does not reflect—and it may not indicate the existence of—a specific dysfunction—and, thus, mental health disorder—but rather an extreme form of social isolation secondary to pre-existing mental health disorders or stressful/socioenvironmental events. It has previously been noted that “social disconnection by itself is not a clinical disorder” (M. F. Green et al., 2020). Severe social isolation may be common to different conditions because mental health disorders are generally associated with and predict impaired social functioning (Finsaas et al., 2020; Matthews et al., 2015; Nemoto et al., 2020; Pucker et al., 2019; Solomon & Mikulincer, 2007; Takahashi et al., 2020). Consequently, this could not justify the existence of hikikomori as a different psychiatric entity. Similarly, Tajan (2022) considers hikikomori not as a mental disorder but rather as a social or psychosocial condition. In light of the above, hikikomori—defined as marked isolation, not working and not being in education—may represent harm, negative consequences of previous existing mental health problems, of dysfunctional social environment and/or difficulty in social relationships. Therefore, in this situation, the simplest terms of severe social isolation or home-based physical isolation might be preferred. This would avoid confusing such a condition of severe social isolation with the presence of a mental health disorder. Similarly, it would limit the risk of over-pathologizing individuals at risk of social isolation due to other different circumstances (Amendola, 2023; Amendola, Cerutti, & von Wyl, 2023).
This narrative review may represent a valuable contribution to the hikikomori debate because highlighted that considering refusal or avoidance, disinterest or unwillingness to attend school/work and to participate in social relationships/interactions for the definition of hikikomori (Japanese Ministry of Health, Labour and Welfare, 2003; Suwa & Suzuki, 2013; Teo & Gaw, 2010) may help in going beyond behavioural symptoms (i.e., physical isolation, not working, not being in education) providing useful psychological indicators of dysfunction for hikikomori, besides impairment/distress (Amendola, 2023; Wakefield et al., 2005). The inclusion of psychological indicators of dysfunction as criteria of hikikomori may improve the differentiation of hikikomori from other psychosocial difficulties that include social isolation and avoiding over-pathologization. Piotti (2022) also considers that the attention on hikikomori has been narrowly focused on “external aspects,” despite reducing the discourse to hikikomori cases with high involvement in technology use with the risk of confusing hikikomori with technological and internet gaming addictions.
Prolonged social withdrawal can occur in severe cases of depression, social anxiety, and adjustment disorder (American Psychiatric Association, 2022). The present study suggests that the use of different hikikomori criteria and conceptualizations, that is, which psychological symptoms are considered central, if any, may influence the interpretation of studies’ findings analysing clinical symptoms and comorbidity. If the main psychological characteristic of hikikomori is no interest or willingness to attend school or work and not maintaining personal relationships, hikikomori could be better conceptualized as a specific variant of depressive disorders or diagnosed as a depressive disorder with insufficient symptoms, unspecified depressive disorder, or adjustment disorder with depressed mood, or mixed anxiety and depressed mood if at least one stressful event is identified. In such cases, the main symptom could be apathy.
If the main psychological characteristic of hikikomori is refusal or avoidance of social situations and social relationships, hikikomori could be a severe variant of social anxiety disorder. The latter view would be consistent with findings highlighting the association of hikikomori with avoidant personality both according to categorical and dimensional approaches (Hayakawa et al., 2018; Katsuki et al., 2019; Teo et al., 2015) as well as the opinions of those scholars who consider the role of personality functioning of relevance for the emergence of hikikomori (Amendola et al., 2021, 2022a; Amendola & Cerutti, 2022; De Luca et al., 2020; Hihara, Kambara, et al., 2022; Hihara, Sugimura, et al., 2022; Muris & Ollendick, 2023; Piotti, 2022).
There is the possibility that the difference between the above specifications is an issue of semantics and that, in nature, psychological functioning can be hardly reduced to simple descriptions of psychological indicators with clear boundaries. However, categories are needed to interpret and study psychological phenomena. Subsequent research is needed to prove their validity. The harmful dysfunction analysis (Wakefield, 1992b, 1992a; Wakefield et al., 2005; Wakefield & First, 2012) perspective may be especially useful to understand the above differentiation. Hikikomori, including the criterion of no interest or willingness to attend school or work and not maintaining personal relationships, and depression may share a dysfunction in regulating emotions and/or motivation. However, as discussed in the results section of this review, no study included this hikikomori criterion to examine depression comorbidity rate and impairment/distress in daily functioning. A dysfunction in motivation or amotivation as one of the main characteristics of hikikomori may differentiate it from social anxiety. Future hikikomori research may also benefit from including the denial and repression of needs as an additional psychological indicator of dysfunction in motivation or amotivation (Cerutti et al., 2021).
Hikikomori, including the criterion refusal or avoidance of social situations and social relationships, and social anxiety disorder may be due to a dysfunction in social functioning (Nesse, 2023; Wakefield et al., 2005). The results of the studies examined in the present review seem to support the notion that hikikomori may be a specific and/or severe variant of social anxiety disorder. On the one hand, a significant proportion (41% in Frankova (2019), 50% in Bellini et al. (2023) and 100% in Benarous et al. (2022)) of hikikomori showed anxiety disorders in recent studies employing the hikikomori criteria of Teo and Gaw (2010). On the other hand, two of these studies, and another one, identified individuals who did not meet the criteria for an already-known psychiatric diagnosis (Bellini et al., 2023; Frankova, 2019; Hamasaki et al., 2022).
Finally, the results of the present review underscore that the diagnosis of an adjustment disorder with characteristics of social anxiety, depression, and/or withdrawal should be considered when in the presence of individuals with prolonged social withdrawal or hikikomori.
In their innovative work, Teo and Gaw (2010) highlighted the possibility that hikikomori could be a “superficial atypical variant of conventional psychiatric diagnosis” (p. 446). The authors noted that, in such cases, social withdrawal is “a symptom that may be part of an underlying anxiety, mood, developmental, or other disorder” and could represent a specifier of a clinical feature of a recognized clinical entity. The authors considered such cases as presenting hikikomori-like states rather than true hikikomori (also indicated as “secondary social withdrawal or hikikomori”). After more than ten years and the publication of relevant empirical studies, it is judicious to recommend that the inclusion of a “with (social) withdrawal” specifier in the definition of anxiety, depression, or adjustment disorders may be considered for hikikomori cases whose symptoms are primarily due to or better explained by those disorders. The specifiers “with withdrawal” and “with work (or academic) inhibition” were previously included for adjustment disorder (American Psychiatric Association, 1987) (now “unspecified” (American Psychiatric Association, 2000, 2022)). The label of hikikomori would be appropriate for the remaining subset of hikikomori cases that would not fall into an existing disorder (also known as “primary social withdrawal or hikikomori”) (Teo & Gaw, 2010).
What could be done to improve the debate on hikikomori?
This review represents an initial useful guide for future research aimed at comparing different definitions of hikikomori and their influence on clinical phenomenology, comorbidity, and daily functioning. In accordance with Nonaka et al. (2022), the use of different definitions of hikikomori across studies may lead to findings also influenced by scholars’ perceptions of hikikomori.
To note, symptoms of psychopathology may change over time, especially during a period of prolonged social withdrawal and isolation (Muris & Ollendick, 2023; Saitō, 1998). Therefore, exploring social withdrawal motivations may further improve clinical understanding informing diagnosis. For example, the similarities and overlap between social anxiety and hikikomori may be underestimated if social anxiety leads to hikikomori and, thereafter, symptoms of social anxiety may become less evident—and an individual less aware of them—after a long period spent in social isolation (Amendola, Cerutti, & von Wyl, 2023). Subsequently, such an individual could be diagnosed with depression or another psychopathology different from the one that initially caused prolonged social withdrawal and isolation. Indeed, the interaction between social anxiety disorder and social isolation may result in major depressive disorder (American Psychiatric Association, 2022) and previous research (Cox et al., 2009) found that mood disorders were particularly common in individuals with comorbid social anxiety and avoidant personality disorder.
Epidemiological longitudinal studies on its phenomenology, comorbidity, and unique impact on daily functioning/impairment/distress are thus required to enlighten the debate (Amendola & Cerutti, 2022, 2023). In accordance with other scholars (Benarous et al., 2022), the possible role of separation anxiety disorder, behavioural inhibition, and anxious-avoidant attachment style as risk factors of hikikomori should be investigated. Future research needs also to study the potential role of anhedonia (Seeman, 2017), and specifically social anhedonia, in hikikomori.
Concomitantly, a well-planned and -conducted Delphi Study involving both scholars studying hikikomori (e.g., those who authored as first or last author at least one publication on the topic) and professionals working in university and/or hospital departments of mental health could help in refining the definition and classification of hikikomori. This would represent a relevant step towards a research agreement/consensus on hikikomori informing future research.
A systematic review of clinical cases published in scientific journals may provide new insights and information, especially on core criteria of the condition.
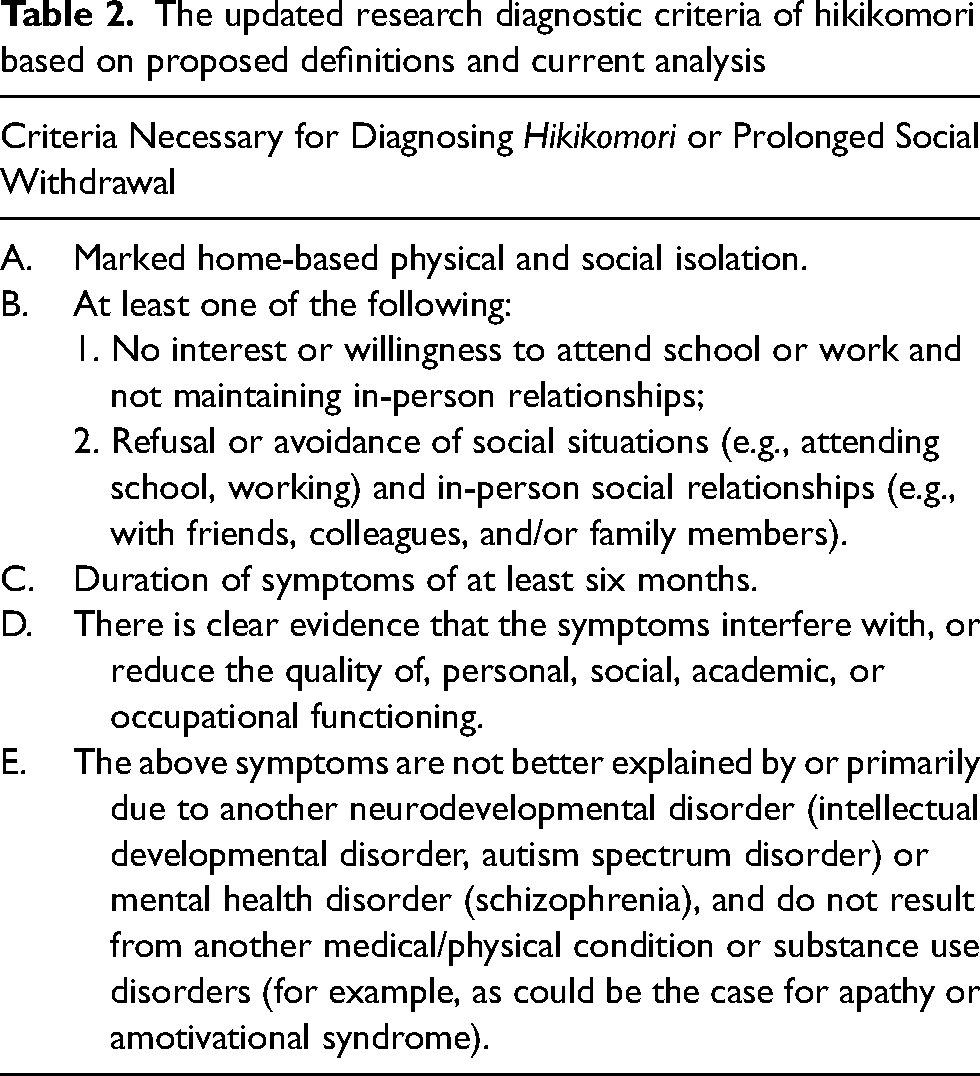
If additional psychological symptoms and indicators of dysfunction are included in the hikikomori definition, this would have implications for exclusion criteria as well. Table 2 updates the proposed research diagnostic criteria for hikikomori based on the different, previous definitions (Japanese Ministry of Health, Labour and Welfare, 2003; Kato et al., 2019, 2020; Suwa & Suzuki, 2013; Teo & Gaw, 2010) and the results of the present review. This might not necessitate the need to exclude specific individuals or mental health disorders because a clear dysfunction is mentioned among the defined criteria (criterion B in Table 2). Most importantly, future research employing these criteria will further clarify similarities and differences between hikikomori, social anxiety, depressive and adjustment disorders, addressing clinical validity. Future studies should investigate whether hikikomori according to the criteria in Table 2 primarily occurs in comorbidity with the mental health disorders analysed in the present review, of which it might be a variant, or whether it can occur by itself. The former scenario would further support the usefulness of a “with (social) withdrawal” specifier (as argued above).
The updated research diagnostic criteria of hikikomori based on proposed definitions and current analysis
Hikikomori and the DSM-5-TR
Hikikomori was included under the paragraph “Examples of Cultural Concepts of Distress” in the chapter “Culture and Psychiatric Diagnosis” of the DSM-5-TR Section III “Emerging Measures and Models” (American Psychiatric Association, 2022) despite the lack of consensus on the hikikomori definition and well-conducted epidemiological studies on hikikomori phenomenology and clinical comorbidity to clarify overlap with other disorders and unique impact on daily functioning.
The main aspects of the description are reported in Table 1. The definition does not specify inclusion and exclusion criteria despite no interest or willingness to attend school or work and no (or complete cessation of) in-person social interactions are described among the characteristics of hikikomori (besides marked home-based physical isolation, for at least six months, causing distress) (American Psychiatric Association, 2022). As documented in the present review, to date, no study used the hikikomori definition including the criteria “no interest or willingness to attend school or work and no (or complete cessation of) in-person social interactions” to analyse similarities and differences with depressive disorders.
In a previous article co-authored by some of the members of the DSM-5-TR Review Group for the chapter “Culture and Psychiatric Diagnosis,” hikikomori was initially used to provide a model to personality disorder research due to hikikomori “similarities to some aspects of personality disorder” (p. 40) while considering the role of culture and local context (Ryder et al., 2015). Then, in a subsequent article, hikikomori was discussed as a condition related to social anxiety disorder suggesting a possible influence of cultural norms as well (Kirmayer & Ryder, 2016).
Considering the above, one may reasonably wonder whether the choice of including hikikomori was premature and/or justified by the actual scientific knowledge. The inclusion of hikikomori in the DSM-5-TR, with a particular focus on adolescents, may have been premature, especially in the current post-COVID-19 pandemic scenario in which adolescents may socially withdraw for different reasons.
A recent systematic review of the literature (Nonaka et al., 2022) showed that most studies (88.5%) examining hikikomori did not consider significant impairment or distress and, thus, the validity of their findings is—at least—uncertain. Therefore, more evidence resulting from good-quality research is necessary to elucidate its validity, that is, the phenomenology of and indicators/criteria of hikikomori as well as clinical comorbidity and unique impact on impairment in daily functioning/distress.
Study limitations
The present study provides an extensive literature review of studies examining the relationship between hikikomori and other well-known mental health disorders. However, it has some limitations that should be considered when interpreting its findings. First, the present review considered only those articles published in English (n = 97 out of 108 records identified with the literature search, 90%), French (n = 7, 6%), Spanish (n = 1, 1%), and Italian (n = 3, 3%). Therefore, potential studies may have been missed because published in a different language than those specified. Despite this, at least some Japanese authors—as well as authors from other Asian countries—fortunately published in English and/or French. Future research may expand the breadth of the present investigation to include studies published in languages not considered in the current work. Second, as for most narrative reviews, a qualitative assessment of included studies and an empirical synthesis of their findings were not provided. Third, as for all narrative reviews, the quality of reported findings relies on the quality of original studies. Fourth, narrative syntheses are at higher risk of bias compared to systematic reviews. However, the research questions, literature search strategy, and study selection procedures were described and reproducible.
Conclusions
The present narrative review aimed to provide a deeper understanding of hikikomori definitions and their overlap with already-known mental health disorders. Its added value to the scientific knowledge consists of having examined similarities and differences between different hikikomori definitions as well as their limitations. Empirical evidence on the clinical validity of some hikikomori definitions is scarce. At the current state of knowledge and waiting for a consensus on the hikikomori definition and comprehensive epidemiological studies, hikikomori—depending on the criteria in use—seems to resemble a (severe) variant of social anxiety disorder, a form of adjustment disorder with anxiety, depression, and/or social withdrawal, as well as a variant of depressive disorder. The inclusion of a “with (social) withdrawal” specifier in the definition of these mental health disorders could be considered. If no clear and valid indicator of dysfunction is included among the criteria for hikikomori, the condition examined may simply constitute severe/extreme social isolation, that is, a negative outcome, consequence, or harm of other psycho-social conditions and/or adverse events rather than a different mental health disorder.
Footnotes
Acknowledgement
The author wishes to thank Professor Rita Cerutti (Department of Dynamic and Clinical Psychology, and Health Studies—Sapienza University of Rome) for her inspiring collaboration over the years. This work was first conceived and planned as an oral presentation for the XXIII National Congress of the Clinical and Dynamic Psychology Section of the Italian Association of Psychology (September 14–17, 2023, Florence, Italy). The initial abstract was submitted on April 15, 2023, and accepted on May 19, 2023. The abstract was published in a Special Issue of the Mediterranean Journal of Clinical Psychology in 2023 (Vol. 11, n2 Supplementum) available at https://cab.unime.it/journals/index.php/MJCP/issue/view/331/showToc. For additional information see ![]() .
.
Author contributions
The author confirms being the sole contributor to this work and approved it for publication.
Author's Note
Dr. Simone Amendola is currently an independent researcher.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The author has no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author was supported by a Swiss Government Excellence Post-Doctoral Scholarship (2022.0033) to conduct a meta-analysis of longitudinal studies on the associations between gaming disorder, internalizing symptoms of psychopathology, and psychological distress. This funder had no role in this review, data analysis, data interpretation, or writing of the report.