
Abstract
The usage of the term “abnormal psychology” has been criticized for being pejorative, which may encourage mental illness stigma and impede seeking help. Although researchers generally endorse the advocacy of dignity-respecting terminology, “abnormal psychology” is still widely used due to the trade-off between the cost of making changes and the potential harm of keeping it. However, the risk of keeping the term has rarely been tested, leaving room for the mind of wishing a fluke that this inaccurate term may lead to few real-world consequences; this belief is challenged by this article. Five experiments were conducted in China (N = 1,283) to test the hypothesis that the term “abnormal psychology” encourages mental illness stigma through the mediation of moral attribution, reducing help-seeking intentions. Results revealed that, despite the identical detailed descriptions of mental illnesses, labeling mental illnesses as “abnormal psychology” (versus “psychopathology”; i.e., 变态心理学 versus 心理病理学) leads to a stronger emphasis on moral causes when explaining etiology and thus to more stigmatizing attitudes (Studies 1A, 1B, and 2). For external validity, the participants freely expressed their impressions and attributions (Study 3). Those cued by “abnormal psychology” were likelier to infer that people experiencing mental illness had twisted, inhibited, narrow-minded, dark, violent, antisocial, and split traits, as well as problematic values/morality. In an imaginary scenario (Study 4), “abnormal psychology” reduced the intention of seeking professional help through the serial mediation of moral attribution and self-stigma. A subtle difference in language can considerably affect people's attitudes and intentions, which suggests reconsideration of the terminology.
The Journal of Abnormal Psychology was rebranded Journal of Psychopathology and Clinical Science in 2022 because the term “abnormal” gradually took on a negative connotation over time, which may have been connected with stigma and discrimination, creating a barrier that hinders people from seeking support (Patalay & MacDonald, 2022). For a similar reason, the Journal of Abnormal Child Psychology was also renamed Research on Child and Adolescent Psychopathology (Frick, 2021).
Psychological researchers are becoming increasingly mindful of language, especially when describing human attributes or states that are not desired by society (e.g., Boccaccini et al., 2008; Dunn & Andrews, 2015; Zamzow, 2023). It is necessary to consider whether the terms may hurt the dignity and self-evaluation of the populations being studied and promote discrimination. Despite recognizing this trend, researchers sometimes underestimate the impact of their inappropriate language and thus follow naming conventions even if they are aware of its limitations. One example is “abnormal psychology,” which is still widely used in the names of university courses and professional textbooks, despite teachers and authors spending much effort explaining the limitations of this term. In the trade-off between the cost of making changes and the potential harm of keeping this questionable term, the former seems to prevail in many cases. However, the risk of keeping the term has rarely been tested, leading to the belief that, though this term is inaccurate and derogatory, it may lead to few real-world consequences.
Contrary to this belief, more and more evidence has been found for the significant effect of subtle differences in language on people's minds and behaviors, which is one way in which social context influences people. For example, labeling juvenile defendants by the colloquial term (i.e., “is a psychopath” versus “meets criteria for psychopathy”) led jurors to believe that they posed a greater risk of committing future crimes and deserved greater punishment (Boccaccini et al., 2008); using the grammatically feminine versus the masculine name of the disease (e.g., “COVID-19” versus “coronavirus”) influenced the perception of danger and behavior intentions of French and Spanish speakers (Mecit et al., 2022); using different names to describe a long COVID diagnosis (i.e., “long COVID” versus “ongoing COVID-19 recovery”) influenced how long the participants would expect to experience their symptoms and how the illness was understood by them (Mills et al., 2022); using generic language in videos to introduce a novel social group (e.g., “Zarpies like to eat flowers” versus “This Zarpie likes to eat flowers”) increased essentialist beliefs of children (Leshin et al., 2021); and describing targets with nouns versus adjectives (e.g., “Mark is a homosexual” versus “Mark is homosexual”) impacted the person perception by Italian and German speakers (Carnaghi et al., 2008). These findings warn us against presuming that the term “abnormal psychology” has little impact on people.
Moreover, the innate limitations of the term “abnormal psychology” leave more room for the stigma of mental illness. The use of “abnormal psychology” in the English-speaking world can be traced back to 1888 when the American Journal of Psychology started categorizing papers under this name (MacDonald et al., 2021). No later than 1890, the University of Pennsylvania offered a psychology course with “abnormal” in its name (Jastrow et al., 1890). No later than 1903, the term “abnormal” was translated into Chinese and used in psychology courses offered by the predecessor of Peking University (Ge, 2023b). The earliest publication that has yet been found to use the term “abnormal psychology” (变态心理学) in China was Principles of Psychology edited by Bingqing Fan in 1915 (Ge, 2023b). The original connotation of this term can be reflected in a review written by Prince (1905), the founding editor of the Journal of Abnormal Psychology, who divided “abnormal psychological phenomena” into two groups: (1) dissociations or weakened syntheses of conscious states, or (2) automatism. At that time, the topics within the scope of abnormal psychology were described in negative terms, but the term “abnormal psychology” was carefully chosen for its scientific neutrality (Patalay & MacDonald, 2022). However, unlike the term “psychopathology,” which focuses on whether people are pathological or healthy, the term “abnormal psychology” focuses on whether people are normal or deviate from the norm. This type of language directs people's attention to comparisons with socially desirable norms but less so to comparisons with healthy personal conditions. Therefore, no language barrier prevents people from overgeneralizing the term “abnormal,” referring to any deviation from socially desirable norms, not just from psychologically healthy conditions (Ge, 2023b). From this, the term “abnormal” becomes increasingly moralized and may be used by some people to label people who are unacceptably different from “us” and distinguish them from what is considered normal. As Frick (2021) criticized, this term is now used to refer more to the person than to the condition that the person has. Link and Phelan (2001) conceptualized stigma as distinguishing and labeling differences, associating human differences with negative attributes, and separating “us” from “them.” According to these criteria, the term “abnormal psychology” has the potential to isolate people experiencing mental illness from those who do not and to imply that they are fundamentally different from nonabnormal people.
In China, where the present studies were conducted, the term “abnormal” is now empirically found to be synonymous with obscene, indecent, hooliganism, nauseating, filthy, malformed, and so on in nonacademic contexts (Ge, 2023b). These connotations cannot be permanently excluded from academic settings of mental illness. Thus, it is possible that the academic term “abnormal psychology” activates these pejorative connotations. Several Chinese researchers have raised concerns about this term, criticizing it on the grounds that it is illogical (Zhu, 1930), inappropriate (Sun, 1934), and inaccurate (Ding, 1964). In light of these, I posit that the term “abnormal psychology” now acts as a cue for encouraging mental illness stigma (Hypothesis 1).
Why does the term “abnormal psychology” encourage mental illness stigma? Attributions may serve as an underlying mechanism. According to the attributional theory of stigma (Weiner et al., 1988), adverse events in particular initiate an attributional search; thus, people typically act as etiologists when knowing someone who is experiencing mental illness. Because the term “abnormal” is more moralized and implies deviating from socially desirable norms compared with “psychopathology,” it may lead people to infer that mental illness is a result of demoralization. These causal beliefs shape the emotional, attitudinal, and behavioral responses (Hegarty & Golden, 2008). For example, Krendl and Pescosolido (2020) found that moral attributions for mental illness (e.g., bad character and the way an individual was raised) were associated with mental illness stigma; Corrigan et al. (2003) found that attributions for mental illness to abusing illegal drugs increased the likelihood of rejecting the focal person. Therefore, I posit that the term “abnormal psychology” leads people to make more moral attributions for mental illness (Hypothesis 2), and moral attributions mediate the effect of the term on mental illness stigma (Hypothesis 3).
One possible downstream consequence of the above effects may be a decreased intention to seek professional help. According to the person-level model of stigma and care-seeking (Corrigan et al., 2014), knowledge impacts care-seeking through the mediation of stigma. Corrigan et al. (2014) emphasized the vital role of how the unsettling state is labeled in promoting care-seeking because some labels may act as a signaling cue that makes people put off or spurn care-seeking to avoid stigma. The term “abnormal psychology” may act as such a stigmatizing cue, because it does not promote the view that the person needs professional intervention because of pathological conditions; instead, it is often viewed as a signal which indicates that the person is defective (Frick, 2021). Additionally, previous research has supported the associations of the attributions (Deacon & Baird, 2009; Goldstein & Rosselli, 2003) and stigma (Barney et al., 2006; Han & Pong, 2015; Loya et al., 2010) of mental illness with the attitudes toward and the intention of seeking help. Thus, I posit that the stigma of mental illness increased by the cue “abnormal psychology” is associated with a reduced intention of seeking professional help (Hypothesis 4).
Overview of the present studies
Taken together, the present work aims to examine the effect of the term “abnormal psychology” on mental illness stigma, shedding light on the underlying mechanism and testing the downstream consequence of help-seeking intentions. In this way, we can empirically assess whether the potential harm of this term is insignificant and overstated or is real and noteworthy. Specifically, participants were assigned to the “abnormal psychology” or “psychopathology” condition (变态心理学 versus 心理病理学). The difference between the two groups was tested in terms of the stigma of six types of mental illness (Studies 1A and 1B), the scores of inventories of the three focal variables (Study 2), and the freely generated contents of impression inferences and causal explanations (Study 3). Additionally, a self-perspective scenario was simulated in Study 4.
The reason for selecting “psychopathology” as the reference group is that these two terms are generally used interchangeably. One example is renaming the two journals mentioned in the beginning paragraph of this article (Frick, 2021; Patalay & MacDonald, 2022). In addition, the APA Dictionary of Psychology (n.d.) records that the term “psychopathology” is used synonymously with “abnormal psychology.” The two terms are also used synonymously in the Chinese language, as evidenced by professional textbooks (e.g., Qian, 2006).
The target sample sizes of Studies 1A–4 were all determined prior to data collection using G*Power (Faul et al., 2009). The focal tests were 2 × 3 ANOVA with within-between interaction for Studies 1A and 1B, independent-samples t test and multiple linear regression for Studies 2 and 4, and the Mann–Whitney U test for Study 3. Minimum sample sizes of 54, 128, 55, and 134 were required, respectively, to yield medium effect sizes (f = .25, d = .50, f2 = .15, d = .50) and power = .80. The target numbers were fulfilled in all studies.
Transparency and openness
The present studies were approved by Peking University. The data for all studies are publicly accessible at https://osf.io/djrf9/?view_only = 79c1f3aac4984c6590c7343272ff2f41. The materials and questionnaires are included in the Supplemental Material. None of the studies reported in this article was preregistered. I report all manipulations, measures, and exclusions in these studies.
Study 1A
Method
Participants
I recruited 423 Chinese residents on WJX.cn (a sample-collecting website in China, similar to MTurk). The participants who failed the attention check or the manipulation check were excluded. (The criteria of this exclusion are elaborated on in the procedure section.) The data of the other 208 participants were considered valid (female: 59.13%; average age = 30.44 years, SD = 7.55; 29.81% learned professional knowledge in psychology or worked in psychology-related careers). Their IP addresses indicated they were from 26 provinces, autonomous regions, and municipalities.
The participants were randomly assigned to one of two groups: “abnormal psychology” versus “psychopathology” (140 and 68 participants, respectively). The results of the Mann–Whitney U test and independent-samples t test indicated that there were no significant differences between the two groups in terms of gender (U = 4738.00, p = .949), age (t (206) = 0.06, p = .949), educational attainment (U = 4574.00, p = .477), or psychology-related experience (U = 4732.00, p = .931).
The participants who were assigned to the “abnormal psychology” group were significantly less likely to fail the attention check (e.g., please tick “1” directly) than the other group (36.16% vs. 63.31%; U = 16,235.50, p < .001), whereas the two groups did not significantly differ in the likelihood to fail the manipulation check (7.59% vs. 13.07%; U = 21,067.50, p = .063). The possible reasons and limitations of the unbalanced exclusion rates are discussed in the General Discussion. No significant differences were found between the valid and excluded data in terms of gender (U = 22,345.50, p = .989), age (t (421) = 0.58, p = .560), educational attainment (U = 22,160.00, p = .812), or psychology-related experience (U = 21,849.00, p = .612).
Procedure and measures
The participants read identical descriptions about people experiencing mental illness but were told the descriptions were in line with symptoms included in either Abnormal Psychology or Psychopathology. The material of descriptions was adapted from Jacinto et al. (2021) and was deliberately designed as a fuzzy description. The descriptions did not contain any conclusive psychopathological labels (e.g., depression), which was intended to avoid participants relying on terms other than the book title to construct their impressions. Instead, these descriptions contained relevant behavioral and trait indicators (e.g., laziness), which participants could interpret from a pathological or non-pathological perspective. Three scenarios were tested: depression (described as laziness), obsessive–compulsive disorder (described as perfectionism), and generalized anxiety (described as insecurity). Different participants were shown these scenarios randomly in different orders. Detailed materials are presented in the Supplemental Material.
After reading each scenario, the stigma of mental illness was measured: “How do you describe a person like Zhao, who fits the description of mental illness in Abnormal Psychology?” Participants responded using a 5-item 7-point scale, adapted from Hegarty and Golden (2008). The Cronbach's αs of stigma for the three scenarios were .72, .73, and .69, respectively. Among these items, two questions of attention check were embedded (e.g., please tick “1” directly). After that, they moved on to the next page and reported their gender, age, educational attainment, and psychology-related experience. Finally, they were asked to choose the book title mentioned on the previous page (i.e., Abnormal Psychology or Psychopathology) from four options for a manipulation check. The online questionnaire did not allow them to return to the previous page. Data from the participants who failed to recall the correct name were excluded.
For the “psychopathology” group, everything was identical to that of the other group except the replacement of “abnormal psychology” with “psychopathology.”
Results
The result of the 2 × 3 ANOVA with the book title as the between-subject factor, with the mental illness scenario as the within-subject factor, and with the stigma of mental illness as the dependent variable indicated a significant main effect of the book title (F (1, 206) = 8.89, p = .003, partial η2 = .04). The participants who were cued by “abnormal psychology” scored significantly higher on the stigma of mental illness (M = 4.18, 95% CI = [4.04, 4.32]) than those cued by “psychopathology” (M = 3.81, 95% CI = [3.61, 4.01]). However, the interaction effect was not significant (F (2, 412) = 1.07, p = .346), which suggested that the effect of the book title on stigma was robust across different mental illness scenarios. The main effect of the illness scenario was significant (F (2, 412) = 24.56, p < .001, partial η2 = .11). The mean and 95% CI of each condition are presented in the three left charts of Figure 1.
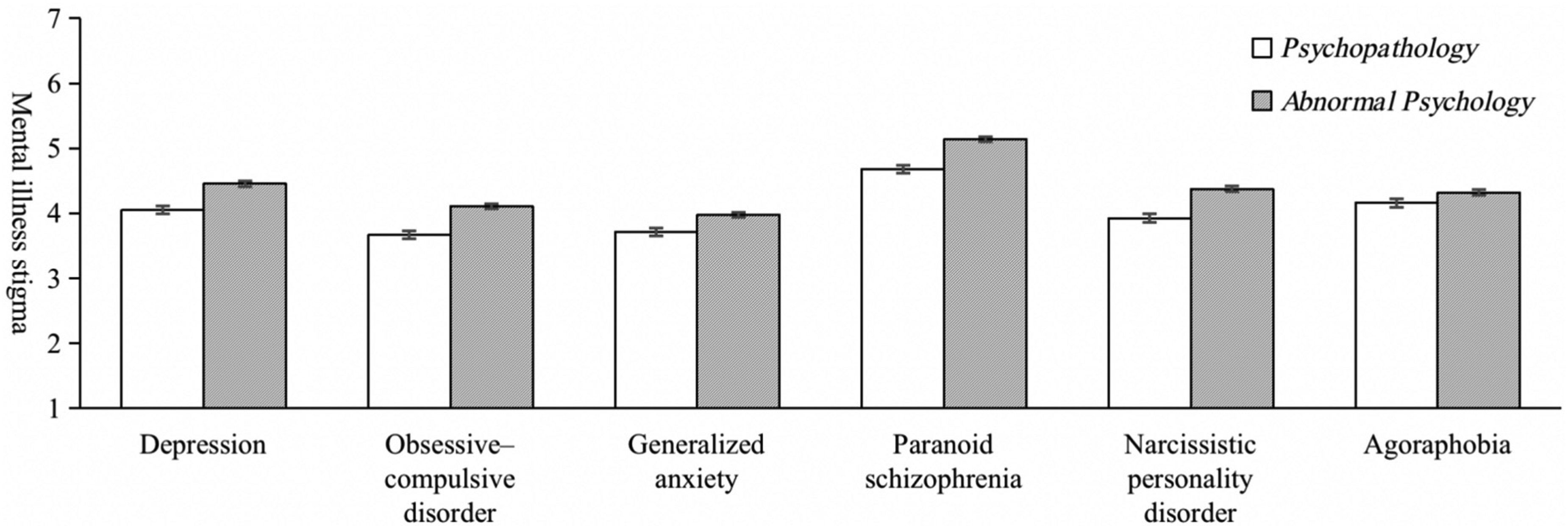
Effect of the term “abnormal psychology” on mental illness stigma (Studies 1A and 1B).
For a robustness check, four covariates (i.e., gender, age, educational attainment, and psychology-related experience) were added to the above ANOVA. The results indicated that the significance patterns remained unchanged: the main effect of the book title, F (1, 202) = 9.01, p = .003, partial η2 = .04; the main effect of illness scenario, F (2, 404) = 3.22, p = .041, partial η2 = .02; the interaction effect, F (2, 404) = 1.00, p = .370.
Study 1B
To test whether or not the effect found in Study 1A could be generalized to more scenarios of mental illnesses, Study 1B was conducted with the same procedure as that in Study 1A but with different mental illness scenarios.
Method
Participants
I recruited 539 Chinese residents on WJX.cn. The participants who failed the attention check or the manipulation check or reported invalid ages (e.g., one-year-old) were excluded. The data of the other 207 participants were considered valid (female: 58.45%; average age = 30.25 years, SD = 8.09; 34.78% learned professional knowledge in psychology or worked in psychology-related careers). Their IP addresses indicated they were from 29 provinces, autonomous regions, and municipalities.
The participants were randomly assigned to one of two groups: “abnormal psychology” versus “psychopathology” (144 and 63 participants, respectively). There were no significant differences between the two groups in terms of gender (U = 4347.00, p = .577), age (t (205) = −.05, p = .963), educational attainment (U = 4168.00, p = .201), or psychology-related experience (U = 4131.00, p = .216).
Similar to Study 1A, the participants assigned to the “abnormal psychology” group were significantly less likely to fail the attention check (e.g., please tick “1” directly) than the other group (53.09% vs. 72.84%; U = 28,578.50, p < .001), whereas the two groups did not significantly differ in the likelihood to fail the manipulation check (8.47% vs. 9.05%; U = 35,404.50, p = .813). No significant differences were found between the valid and excluded data in terms of gender (U = 34,058.50, p = .839), age (t (537) = −0.01, p = .991), educational attainment (U = 34,314.00, p = .970), or psychology-related experience (U = 33,795.00, p = .694).
Procedure and measures
The procedure was identical to that in Study 1A but with three different mental illness scenarios: paranoid schizophrenia (described as snooper), narcissistic personality disorder (described as egocentrism), and agoraphobia (described as fear). The materials were also adapted from Jacinto et al. (2021) and are presented in the Supplemental Material. The mental illness stigma measures were identical to those in Study 1A, and αs were .72, .73, and .70, respectively.
Results
The result of a similar ANOVA was consistent with that in Study 1A, which indicated a significant main effect of the book title (F (1, 205) = 7.42, p = .007, partial η2 = .04). The participants who were cued by “abnormal psychology” scored significantly higher on the stigma of mental illness (M = 4.61, 95% CI = [4.47, 4.75]) than those cued by “psychopathology” (M = 4.26, 95% CI = [4.04, 4.47]). The interaction effect was not significant (F (2, 410) = 2.87, p = .058), whereas the main effect of the illness scenario was significant (F (2, 410) = 69.16, p < .001, partial η2 = .25). The mean and 95% CI of each condition are presented in the three right charts of Figure 1.
A robustness check that was similar to that in Study 1A (i.e., controlling gender, age, educational attainment, and psychology-related experience as covariates) revealed that the main effect of the book title remained significant (F (1, 201) = 7.04, p = .009, partial η2 = .03). The interaction effect turned significant (F (2, 402) = 3.61, p = .028, partial η2 = .02), whereas the main effect of illness scenario turned nonsignificant (F (2, 402) = 1.197, p = .303). These findings supported Hypothesis 1 in different mental illness scenarios.
Study 2
Study 2 aimed to elucidate the mechanism underlying the effect found in Studies 1A and 1B and test all four hypotheses.
Method
Participants
I recruited 612 Chinese residents on WJX.cn. The participants who failed the attention check or the manipulation check were excluded. The data of the other 320 participants were considered valid (female: 65.00%; average age = 30.23 years, SD = 7.72; 33.75% learned professional knowledge in psychology or worked in psychology-related careers). Their IP addresses indicated they were from 28 provinces, autonomous regions, and municipalities.
The participants were randomly assigned to one of two groups: “abnormal psychology” versus “psychopathology” (191 and 129 participants, respectively). There were no significant differences between the two groups in terms of gender (U = 11,383.50, p = .163), age (t (318) = 0.23, p = .819), educational attainment (U = 11,610.50, p = .213), or psychology-related experience (U = 12,245.50, p = .911).
Similar to Studies 1A and 1B, the participants assigned to the “abnormal psychology” group were significantly less likely to fail the attention check (e.g., please tick “1” directly) than the other group (43.27% vs. 51.85%; U = 42,210.00, p = .035), whereas the two groups did not significantly differ in the likelihood to fail the manipulation check (6.14% vs. 10.37%; U = 44,217.00, p = .056). No significant differences were found between the valid and excluded data in terms of gender (U = 46,112.00, p = .737), age (t (610) = 0.10, p = .919), educational attainment (U = 46,071.50, p = .673), or psychology-related experience (U = 46,472.00, p = .890).
Procedure
For the “abnormal psychology” group, first, the participants read the material that briefly introduced abnormal psychology (see Section 3 of the Supplemental Material). This material was developed based on the main content of a Chinese professional textbook on abnormal psychology (Qian, 2006). After reading it, the participants completed the measures of attributions for mental illness, the stigma of mental illness, and help-seeking intention, among which three attention check questions were embedded. Finally, the participants reported their gender, age, educational attainment, and psychology-related experience and completed the manipulation check (i.e., recalling the mentioned book title).
For the “psychopathology” group, everything was identical except the replacement of “abnormal psychology” with “psychopathology.”
Measures
The measure of attributions for mental illness was adapted from Blais and Renshaw (2012). The participants were asked, “Why do some people have the mental illnesses described by Abnormal Psychology?” They rated 12 items on a 7-point scale. The adaptation notes and detailed items are presented in the Supplemental Material.
The measure of the stigma of mental illness was adopted from Krendl and Pescosolido (2020). The participants rated 27 items (α = .90) on a 7-point scale, including prejudice and discriminatory potential.
The measure of the intention to seek professional help was adapted from Oliver et al. (2005). The adaptation was made to fit the purpose of the present study. The participants were asked, “If you have the mental illnesses described by Abnormal Psychology, how possible will it be for you to seek the help of a psychological counselor or doctor?” They reported the likelihood on a 7-point scale.
Results
To test Hypothesis 1, an independent-samples t test was performed. The result indicated that the participants who were cued by “abnormal psychology” scored significantly higher on the stigma of mental illness (M = 4.24, SD = 0.83) than those cued by “psychopathology” (M = 3.86, SD = 0.83); t (318) = −4.10, p < .001, Cohen's d = −0.46. For a robustness check, the result of regression analysis with the book title as the independent variable, with stigma as the dependent variable, and with gender, age, educational attainment, and psychology-related experience as the covariates indicated a significant effect (β = .23, p < .001). These findings supported Hypothesis 1. Moreover, an additional analysis was performed to show further the effects of “abnormal psychology” on different dimensions of stigma, the results of which are presented in Table 1. Compared with those cued by “psychopathology,” the participants who were cued by “abnormal psychology” reported significantly stronger exclusionary sentiments and negative affect toward people experiencing mental illness, made significantly more prejudiced inferences about their traits, viewed them as significantly more dangerous, and were significantly more unwilling to interact with them and more intended to keep social distance from them.
Effects of “abnormal psychology” on different dimensions of mental illness stigma (Study 2).
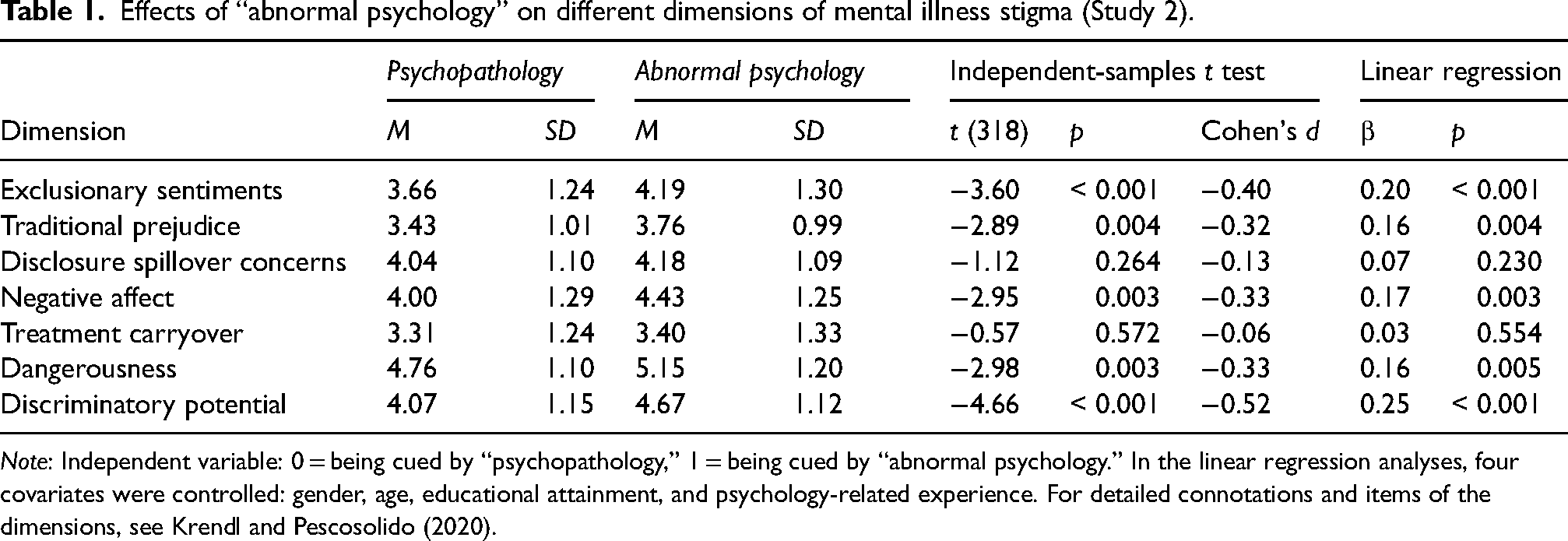
Note: Independent variable: 0 = being cued by “psychopathology,” 1 = being cued by “abnormal psychology.” In the linear regression analyses, four covariates were controlled: gender, age, educational attainment, and psychology-related experience. For detailed connotations and items of the dimensions, see Krendl and Pescosolido (2020).
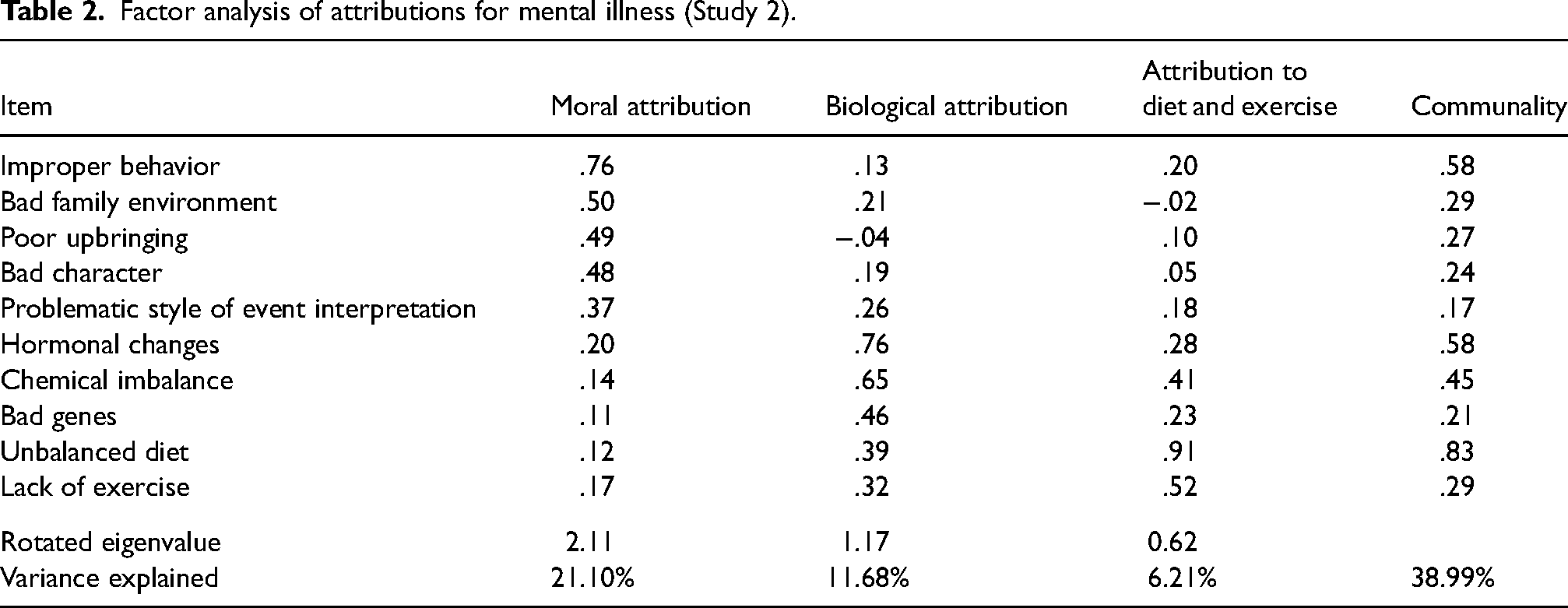
Before the tests of Hypotheses 2 and 3, a factor analysis of attributions for mental illness was performed to simplify the 12 items and facilitate the analyses. The result of Bartlett's test of sphericity indicated that χ2 = 709.85, df = 66, p < .001. The Kaiser–Meyer–Olkin measure of sampling adequacy was .73. I used exploratory factor analysis with principal axis factoring and a Promax rotation to estimate the factor correlations. The number of factors was determined according to the rule of eigenvalues larger than 1 and the scree plot. The items with factor loadings exceeding .35, communalities exceeding .15, and cross-loadings below .10 were retained. Based on these criteria, ten items were retained and loaded on three factors: moral attribution, biological attribution, and attribution to diet and exercise. The loadings, communalities, eigenvalues, and explained variance of the retained items are presented in Table 2. Notably, although situational attribution and attribution to substance abuse were not suitable for any of the three factors according to the factor analysis, they were still meaningful and included as single-item indicators in the subsequent analyses.
Factor analysis of attributions for mental illness (Study 2).
To test Hypothesis 2, several independent-samples t tests were performed. The result indicated that, compared with those cued by “psychopathology,” the participants who were cued by “abnormal psychology” were significantly more likely to believe that mental illness was caused by moral factors (e.g., bad character, improper behavior, and poor upbringing; t (318) = −2.42, p = .016, Cohen's d = −0.27) and situational factors (t (318) = −2.54, p = .012, Cohen's d = −0.28). In contrast, the manipulation of the book titles did not significantly influence biological attribution (t (318) = −0.52, p = .604), attribution to diet and exercise (t (318) = 0.41, p = .686), or attribution to substance abuse (t (318) = .80, p = .424). For a robustness check, the result of the regression analysis that controlled the four covariates indicated that the significance patterns remained unchanged. These findings supported Hypothesis 2.
To test Hypothesis 3, an analysis using Model 4 of PROCESS of SPSS (Hayes, 2013) was performed with the book title as the independent variable, with all five categories of attributions as the parallel mediators, with stigma as the dependent variable, and with the four covariates controlled. The result of 5,000 bootstrap samples with a 95% bias-corrected bootstrap confidence interval indicated a significant indirect effect through moral attribution (β = .03, 95% CI = [0.01, 0.07]). This finding supported Hypothesis 3, indicating that moral attribution mediated the effect of “abnormal psychology” on the stigma of mental illness. The coefficients and the other indirect effects are presented in Figure 2.
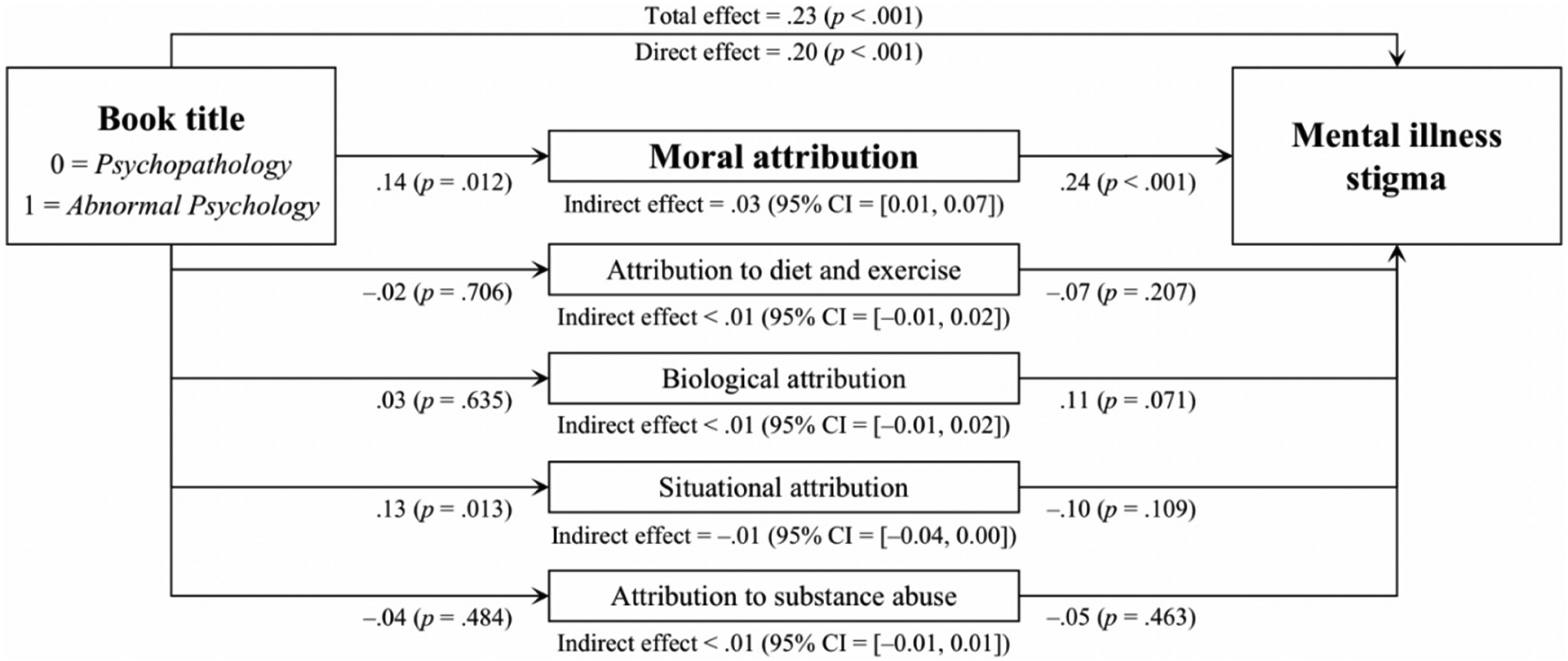
Moral attribution for mental illness mediated the effect of “abnormal psychology” on mental illness stigma (Study 2).
To test Hypothesis 4, an independent-samples t test was performed. The result indicated a nonsignificant effect of the book title on the intention to seek help (t (318) = −1.81, p = .071). The result of an analysis using Model 6 of PROCESS (Hayes, 2013) with the book title as the independent variable, moral attribution and stigma as two serial mediators, the intention of seeking help as the dependent variable, and the four covariates controlled indicated that the indirect effects were not significant. These findings did not support Hypothesis 4.
Discussion
There were two limitations to Study 2. First, the attributions for and the stigma of mental illness were measured by several items selected by the researchers. This kind of measure enabled a relatively controlled and structured comparison but might have interfered with the natural process of the respondents, threatening external validity. Attributions and stigma are sometimes implicit and subconscious; thus, explicitly asking participants whether or not they endorse some statements may fail to capture their honest thoughts. Additionally, the previously established measures might have neglected some points. Study 3 addressed this issue by letting participants freely express their opinions. Second, Hypothesis 4 was not supported. One possible reason was that the manipulation in Study 2 was not conducted from a self-perspective; thus, it failed to change participants’ own intentions of help-seeking. Study 4 addressed this issue by simulating a self-perspective scenario.
Study 3
To address the issue of external validity, Study 3 conducted the same experimental manipulation as that in Study 2, but the participants were allowed to express their causal beliefs and trait inferences freely. This way, Hypotheses 1 and 2 were tested to see whether the differences captured by previously established items also emerged in participants’ unprompted responses.
Method
Participants
I recruited 234 Chinese residents on WJX.cn. The participants who failed the manipulation check or provided invalid answers to open-ended questions (e.g., only punctuation marks or “I don’t know”) were excluded. The data of the other 226 participants were considered valid (female: 69.91%; average age = 28.69 years, SD = 7.48; 38.05% learned professional knowledge in psychology or worked in psychology-related careers). Their IP addresses indicated they were from 29 provinces, autonomous regions, and municipalities.
The participants were randomly assigned to one of two groups: “abnormal psychology” versus “psychopathology” (109 and 117 participants, respectively). There were no significant differences between the two groups in terms of gender (U = 6111.00, p = .497), age (t (224) = −1.94, p = .054), educational attainment (U = 5804.50, p = .073), or psychology-related experience (U = 6317.50, p = 0.886).
Procedure
For the “abnormal psychology” group, the participants first read the material identical to that in Study 2. The participants were then asked, “Why do some people have the mental illnesses described by Abnormal Psychology?” Unlike in Study 2, there were no items offered in Study 3. Instead, the participants were asked to input the most important three causes into the textbox. Subsequently, they were asked, “What kind of people are more likely to have the mental illnesses described by Abnormal Psychology?” They input the most important three aspects into the textbox. Finally, the participants reported their gender, age, educational attainment, and psychology-related experience and completed the manipulation check (i.e., recalling the mentioned book title).
For the “psychopathology” group, everything was identical except the replacement of “abnormal psychology” with “psychopathology.”
Coding
Detailed information on coding procedures and schemes is presented in Section 4 of the Supplemental Material. Three coding tasks were conducted. First, two independent coders who were blinded to participant grouping coded the 678 ascription descriptions (i.e., participants’ responses to the first question). These ascription descriptions were labeled as one of 14 categories: ten were in line with the items in Study 2 (except chemical imbalance and lack of exercise; Blais & Renshaw, 2012), whereas four were newly created in Study 3 (i.e., stress, trauma/life-change/experience, interpersonal relationship, and other biological factors). Of the 678 descriptions, 92.04% were categorized consistently between the two coders. Disagreements were resolved through discussions among the coders and me. Second, a coder and I coded the 693 impressions (i.e., participants’ responses to the second question) independently. These impressions were labeled as one of 13 categories, which will be elaborated on in the results section. Of the 693 impressions, 90.91% were categorized consistently. Third, the 693 impressions were coded as per their favorable or derogatory senses. To make unbiased judgments, a Chinese dictionary with 13,428 favorable words and 14,099 derogatory words was established based on two sources (Ku & Chen, 2007; Li & Sun, 2007). Thus, whether or not participants used derogatory words to describe their impressions of people experiencing mental illness was determined by the previously established dictionary instead of human coders. Each of the 14 categories of ascription descriptions, the 13 categories of impressions, and whether the participant used derogatory words was coded as a person-level dummy variable (i.e., 1 = being mentioned by the participant, 0 = not).
Results
The categorizing result of the impression inferences freely generated by the participants is presented in Table 3, as well as the result of the Mann–Whitney U test between the “psychopathology” and “abnormal psychology” groups in terms of the prevalence of each category. Although the detailed introductions about mental illness were identical across the two groups, the participants who were cued by “abnormal psychology” were significantly more likely than the other group to infer that people experiencing mental illness had twisted, inhibited, narrow-minded, dark, violent, antisocial, and split personality traits, as well as problematic values and morality. In contrast, the participants who were cued by “psychopathology” were significantly more likely than the other group to infer that they had some problems in psychological resilience, coping style, and cognitive/thinking style. These impressions were more rational and less stigmatized and, more importantly, may function as a psychological foundation for seeking professional interventions.
Participant-generated impression inferences about people experiencing mental illness (Study 3).
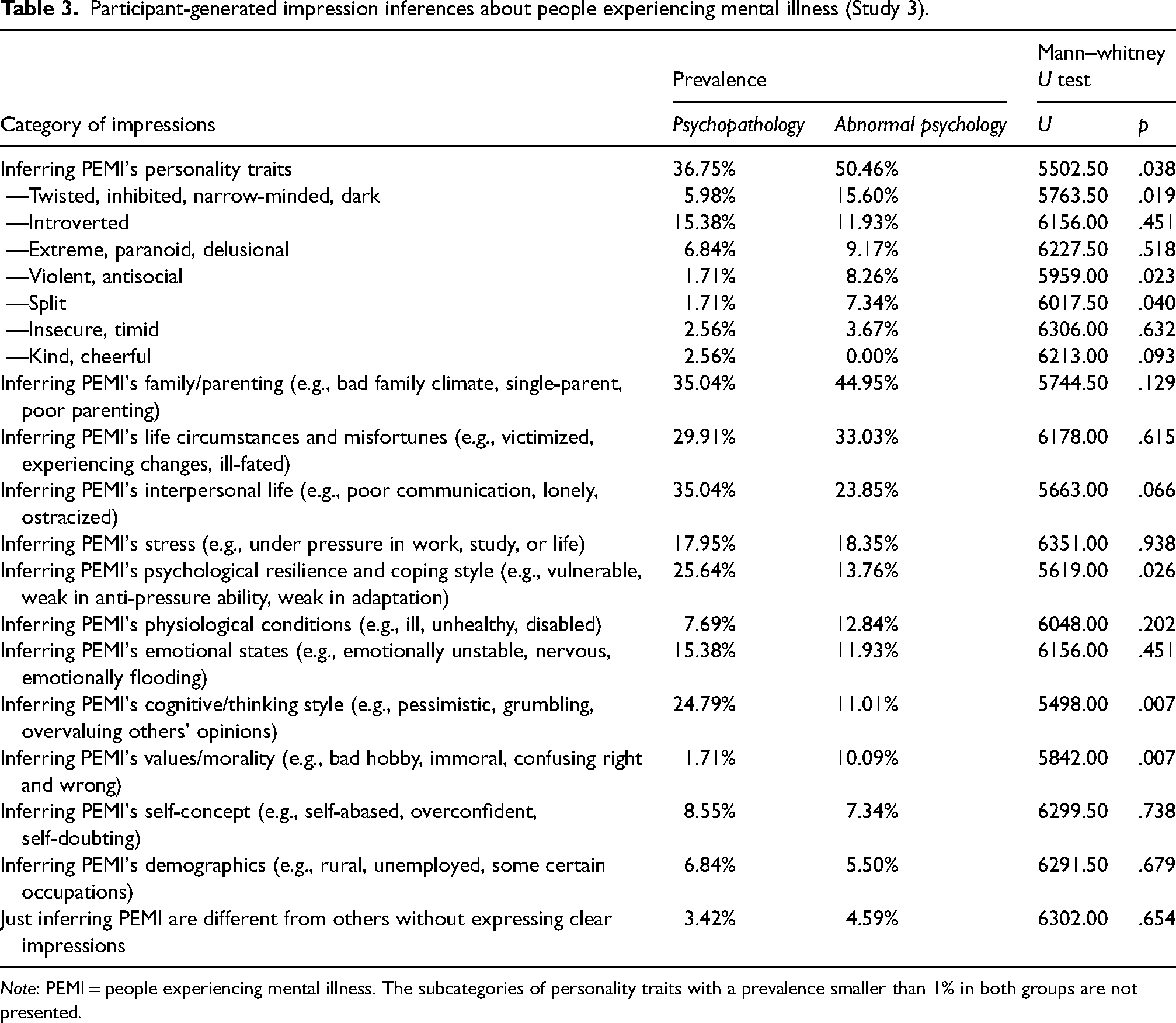
Note: PEMI = people experiencing mental illness. The subcategories of personality traits with a prevalence smaller than 1% in both groups are not presented.
In addition to categorization, a Mann–Whitney U test was performed to test whether or not the two groups differed in the prevalence of derogatory words, and the result indicated a significant difference (U = 5471.50, p = .014). Specifically, 68.38% of the participants who were cued by “psychopathology” used derogatory words (according to the previously established dictionary) to describe their impressions about people experiencing mental illness, whereas 82.57% of those who were cued by “abnormal psychology” did so. For a robustness check, the result of logistic regression with the four covariates controlled (i.e., gender, age, educational attainment, and psychology-related experience) indicated that the effect of the book title remained significant (B = 0.85, p = .011, OR = 2.33).
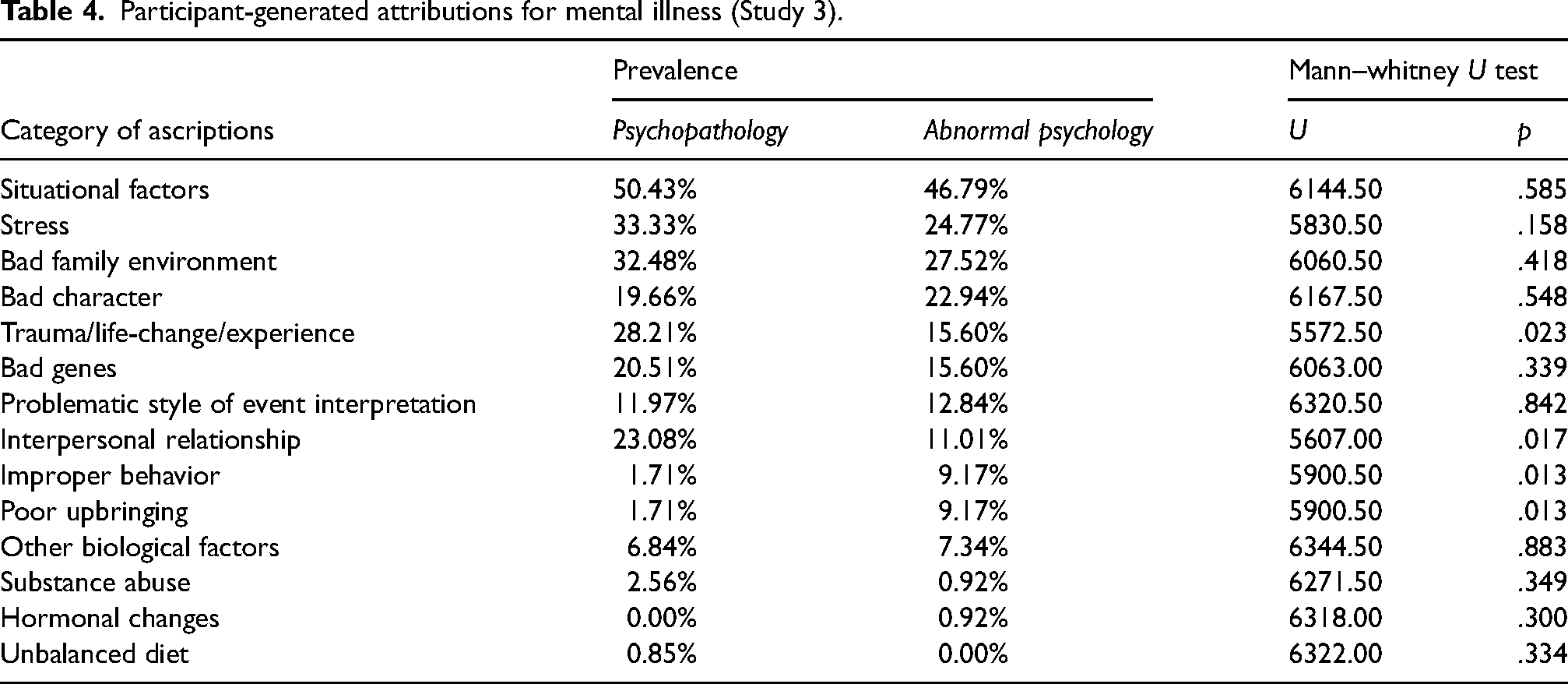
Similarly, the categorizing and Mann–Whitney U test results of the ascription descriptions are presented in Table 4. The participants who were cued by “abnormal psychology” were significantly more likely than the other group to believe that mental illness was caused by improper behavior and poor upbringing, two indicators of moral attribution (according to the factor analysis result in Study 2). Taken together, the effects of the book title on the stigma of and attributions for mental illness (Hypotheses 1 and 2) were found in both structured scales (Study 2) and freely generated contents (Study 3). Moreover, the participants cued by “psychopathology” were significantly more likely than the other group to believe that mental illness was caused by trauma/life-change/experience and interpersonal relationships, which reflected a less judgmental attitude toward people experiencing mental illness.
Participant-generated attributions for mental illness (Study 3).
Study 4
Study 4 also aimed at a comprehensive test of all hypotheses, as Study 2, but it focused on the self-perspective instead of the responses to others’ mental illness.
Method
Participants
I recruited 405 Chinese residents on WJX.cn. The participants who failed the attention check or the manipulation check were excluded. The data of the other 322 participants were considered valid (female: 67.08%; average age = 29.92 years, SD = 7.10; 33.54% learned professional knowledge in psychology or worked in psychology-related careers). Their IP addresses indicated they were from 29 provinces, autonomous regions, and municipalities.
The participants were randomly assigned to one of two groups: “abnormal psychology” versus “psychopathology” (164 and 158 participants, respectively). The results indicated that there were no significant differences between the two groups in terms of gender (U = 12,475.00, p = .479), age (t (320) = −1.42, p = .157), educational attainment (U = 12,869.50, p = .888), or psychology-related experience (U = 12,633.00, p = .636).
The participants assigned to the “abnormal psychology” group were significantly more likely to fail the manipulation check than the other group (24.43% vs. 14.04%; U = 19,610.00, p = .030), whereas the two groups did not significantly differ in the likelihood to fail the attention check (40.10% vs. 40.83%; U = 20,295.00, p = .803). No significant differences were found between the valid and excluded data in terms of gender (U = 13,311.00, p = .946), age (t (403) = 0.04, p = .970), educational attainment (U = 13,086.00, p = .693), or psychology-related experience (U = 12,906.00, p = .555).
Procedure
For the “abnormal psychology” group, the participants first read the material that described the scenario where they perceived their psychologically unsettling states and found that these symptoms were consistent with Abnormal Psychology in searching for relevant information. The material is presented in Section 5 of the Supplemental Material. After reading the text, the participants completed the measures of attributions for mental illness, self-stigma of mental illness, and help-seeking intention, among which an attention check question was embedded. Finally, the participants reported their gender, age, educational attainment, and psychology-related experience and completed the manipulation check (i.e., recalling the mentioned book title).
For the “psychopathology” group, everything was identical except the replacement of “abnormal psychology” with “psychopathology.”
Measures
The measure of attributions for mental illness was adapted from Krendl and Pescosolido (2020). The adaptation was made to fit the objectives of the present study. The participants were asked, “What factors might cause you to suffer from the mental illnesses described in Abnormal Psychology? Please consider all possible causes. Among all causes, how great is the proportion of moral causes?” They chose a response from 0%, 10%, 20%, …, 100%.
The measure of self-stigma of mental illness was adopted from Mak and Cheung (2010). The participants rated nine items (α = .90) on a 7-point scale. An example is, “My behavior fits Abnormal Psychology; such an identity taints my life.”
The measure of the intentions of seeking professional help was adapted from Have et al. (2010). The adaptation was made to fit the objectives of this study. The participants answered five questions (α = .71) on a 7-point scale. An example is, “When you find yourself in line with the descriptions of Abnormal Psychology, would you seek help from counselors or doctors?”
Results
As presented in Table 5, the results of the independent-samples t tests (without covariates) and linear regressions (with gender, age, educational attainment, and psychology-related experience controlled as covariates) indicated that if the participants were informed that their psychologically unsettling situation fit the descriptions in Abnormal Psychology (versus Psychopathology), they attached significantly more importance to moral causes when explaining the reasons for their alarming situation, scored significantly higher on self-stigma, and had significantly weaker intentions of seeking help. As for different aspects of the intention to seek help, the participants cued by “abnormal psychology” (versus “psychopathology”) were significantly less willing to seek professional help, predicted more strongly that they would feel uncomfortable talking about their problems with counselors or doctors, and believed more strongly that they would be embarrassed if their friends knew they were seeing counselors or doctors. In contrast, the two groups did not significantly differ in the belief that they would be helped if seeking professional help and would not get better without it. In other words, the reason why “abnormal psychology” reduced help-seeking intentions was not that the participants viewed professional help as useless; instead, the term made them uncomfortable and embarrassed.
Effects of “abnormal psychology” on attributions for mental illness, self-stigma, and intention to seek professional help (Study 4).
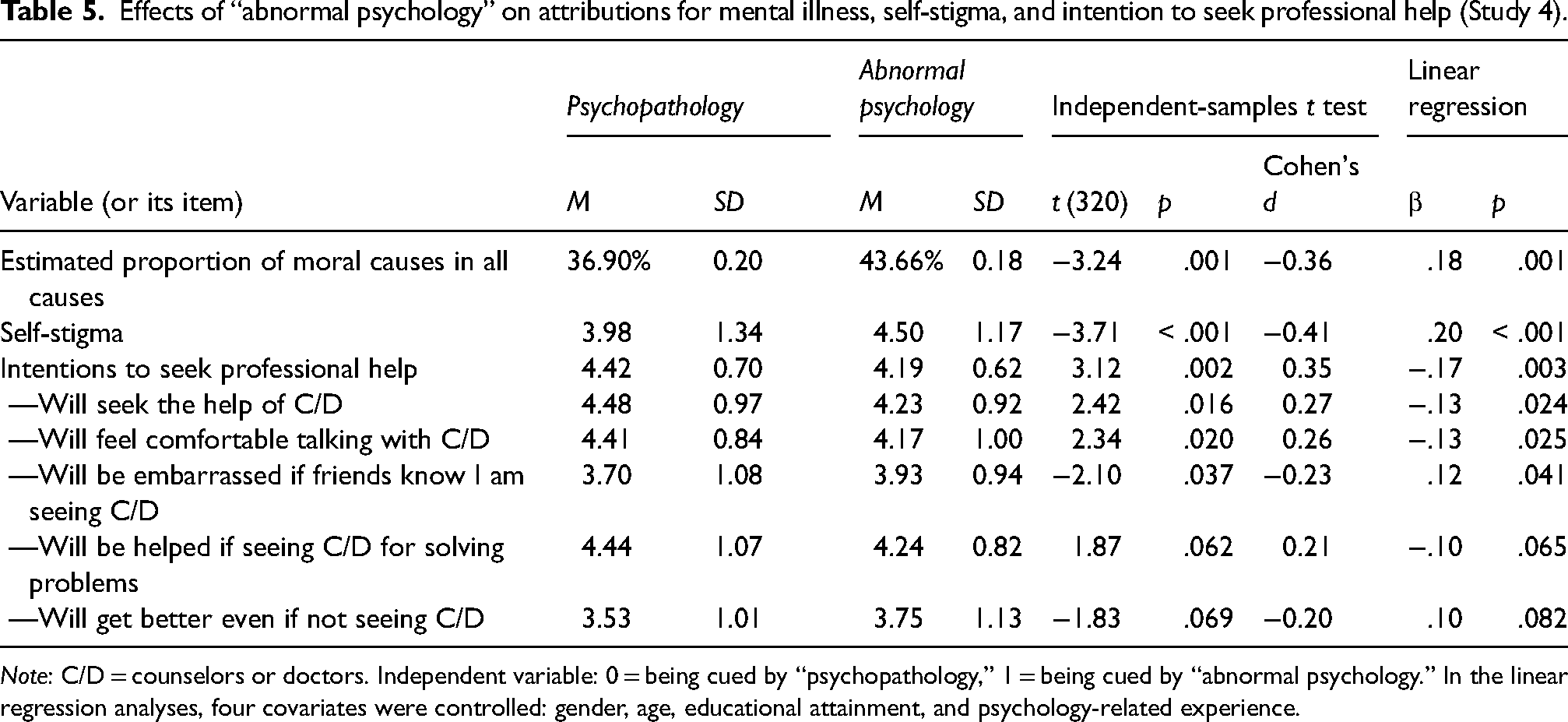
Note: C/D = counselors or doctors. Independent variable: 0 = being cued by “psychopathology,” 1 = being cued by “abnormal psychology.” In the linear regression analyses, four covariates were controlled: gender, age, educational attainment, and psychology-related experience.
The result of an analysis using Model 6 of PROCESS (Hayes, 2013) with the book title as the independent variable, with moral attribution and self-stigma as two serial mediators, with help-seeking intentions as the dependent variable, and with the four covariates controlled indicated a significant total indirect effect (β = −.05, 95% CI = [−0.09, −0.02]). In addition, the indirect effects through attribution (β = −.03, 95% CI = [−0.062, −0.004]), through self-stigma (β = −.02, 95% CI = [−0.049, −0.002]), and through both (β = −.004, 95% CI = [−0.0110, −0.0002]) were all significant. The coefficients are presented in Figure 3.
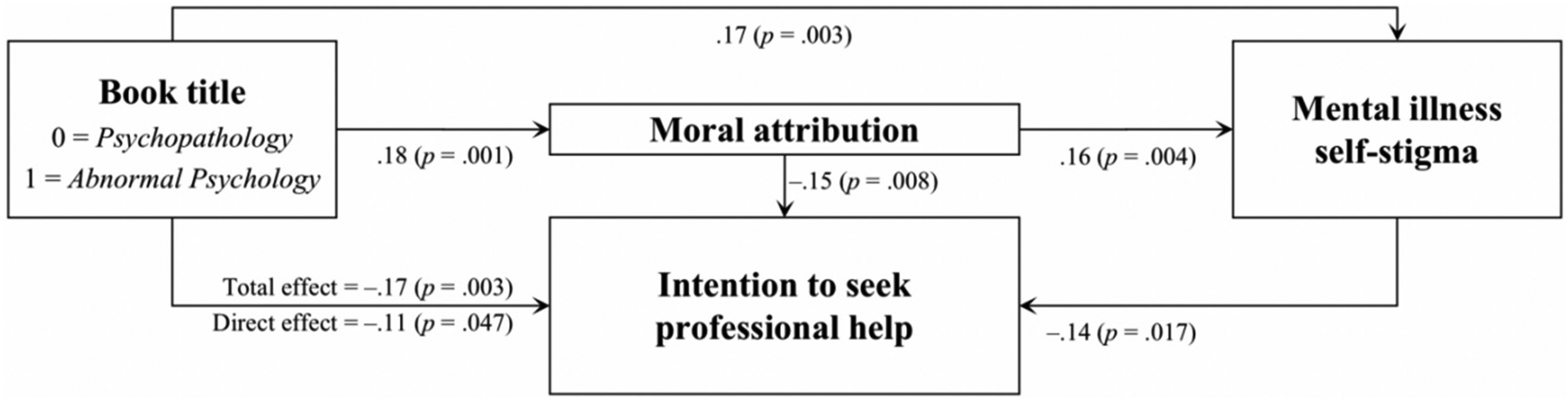
Effects of “abnormal psychology” on attributions for mental illness, self-stigma, and intention to seek professional help (Study 4).
General discussion
The findings of the present studies showed that a subtle difference in terms can make a considerable difference in people's attitudes and intentions. First, even though the detailed descriptions or introductions of mental illness were identical, labeling them as “abnormal psychology” (versus “psychopathology”) directed the participants to pay more attention to moral causes when explaining the etiology of mental illness and thus hold more stigmatizing attitudes toward people experiencing mental illness. Second, when asked to express their impressions about people experiencing mental illness freely, the participants who were cued by “abnormal psychology” were significantly more likely to infer that they had twisted, inhibited, narrow-minded, dark, violent, antisocial, and split personality traits, as well as problematic values and morality. Third, in the imaginary scenario where the participants searched for information in response to their own psychologically unsettling situation, the cue “abnormal psychology” reduced their intention to seek professional help through the serial mediation of moral attribution and self-stigma.
These findings align with previous predictions (Patalay & MacDonald, 2022), provide direct evidence for the dark side of the term “abnormal psychology,” and may function as an opportunity for researchers to reconsider the terminology of this field. The term “abnormal psychology” was challenged from early on, because researchers argued that it implies an essential distinction between normal and abnormal populations and thus leads to misunderstandings that may isolate those experiencing distress (Chen, 1920; Tao, 1922; Zhu, 1930). By contrast, the term “psychopathology” is regarded as a more accurate choice by many researchers. MacDonald et al. (2021) argued that “psychopathology” had not accrued stigma, though it had a relatively longer history than “abnormal psychology.” The findings of the present studies also demonstrated that the participants who were cued by “psychopathology” (versus “abnormal psychology”) were significantly likelier to attribute mental illness to trauma/life-change/experience and interpersonal relationships and infer that people experiencing mental illness had some problems in psychological resilience, coping style, and cognitive/thinking style. These impressions were less judgmental and implied a relatively more promising prospect of improving psychological adaptation and cognitive style with the help of professionals.
The present studies show how social contexts impact people's attitudes and behaviors through the mediation of social cognition. The fundamental assumption of social psychology is that contextual factors play important roles in determining or influencing how people think and act. Researchers aim to identify these kinds of factors and shed light on the mediating process through which contextual stimuli influence people's responses. Attributions have been established as a psychological process linking stimuli and intentions. When experiencing adverse events, attributional search is often activated (Weiner et al., 1988). Mental illness is one such adverse event that often prompts the focal people and observers to find causal explanations. Due to this kind of cognitive need, subtle cues in social contexts, such as “abnormal,” may be absorbed to construct their explanatory models. As a pejorative descriptor widely used in everyday life, the term “abnormal” may incorporate biased knowledge about mental illness. As Corrigan et al. (2014) argued, how people label psychologically unsettling phenomena sends a stigmatizing or destigmatizing signal, which in turn influences the decision to seek help.
Although the present work focuses on the intention of seeking help as the downstream consequence, the actual impacts may involve more aspects. Stigma may deprive people experiencing mental illness of opportunities critical to achieving life goals and impact the equitable allocation of economic and health resources (Corrigan, 2004). Additionally, the present studies demonstrate a negative association between “abnormal psychology” and healthcare-related solutions but leave a question open: What kind of solutions may this cue imply and promote? For example, criminal or penal solutions and religious or moral solutions may be differentially affected by this term. Thus, future research can extend the tests to more consequences. Other limitations of the present work are listed below. (1) The present studies focused on the general population's attitude toward the terms without distinguishing sub-populations. Future studies can further distinguish the attitudes of people in various roles, such as psychological researchers and practitioners or people who are experiencing distress and their family and friends. (2) Due to the attention and manipulation checks, the exclusion rates of the “abnormal psychology” and “psychopathology” groups were significantly different. One possible explanation is that the cue “abnormal psychology” is more eye-catching and associated with many popular news stories; thus, it attracts and motivates respondents to carefully complete the questionnaires. In contrast, the cue “psychopathology” is more scholastic and unattractive, but it is novel to laypeople. This may be a reason why the “psychopathology” group was observed to be more likely to fail the attention check (indicating carefulness) in Studies 1A, 1B, and 2 but pass the manipulation check (involving memory tests) in Study 4 than the other group. This selection bias should be noted, but the analyses also revealed that there were no detectable demographic differences between the retained and excluded participants. (3) I failed to find extant studies on psychometric validation in the Chinese context for the scales adopted in the present studies. While these studies provide initial insights into the use of these measures, it is important for future studies to further establish their cultural relevance. (4) One-item and two-item factors were used in Study 2, but this is not a recommended method due to issues around its reliability. However, these factors were retained because they were not for focal variables, and the benefits of taking them into account in models were arguably greater than those of omitting them. (5) Imaginary scenarios were adopted in Study 4. Although the online material may fit the situations where people search online for relevant information when they start perceiving their psychological difficulties, a question remains whether the term also affects someone suffering from mental illness. (6) Convenience sampling was adopted in the present studies. (7) α for one variable was smaller than .70 in Study 1A. (8) The mediation was only measured but not manipulated, so the relationship between the mediator and dependent variable was correlational rather than causal. The limitations of the measurement-of-mediation design have been documented by previous research (Ge, 2023a). (9) This study was conducted in China, so caution should be exercised in generalizing the findings to other countries. Nevertheless, it is generally informative for understanding how terminology can play a role in people's lives.
Making changes to combat structural and inveterate stigma is never easy; just as we all know, it is difficult to change the naming conventions of “abnormal psychology” overnight. But this article and many other advocating articles may serve as an impetus for psychological terminology that better respects dignity.
Supplemental Material
sj-docx-1-pac-10.1177_18344909241264771 - Supplemental material for The term “abnormal psychology” cues mental illness stigma: A study in China
Supplemental material, sj-docx-1-pac-10.1177_18344909241264771 for The term “abnormal psychology” cues mental illness stigma: A study in China by Xiaoyu Ge in Journal of Pacific Rim Psychology
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.