
Abstract
Public humiliation is a negative self-conscious emotion that results from experiencing public humiliation; that is, being humiliated in public in front of witnesses. In the current study, experiencing public humiliation refers to the humiliation that is caused by a perpetrator or perpetrators with negative intent at a location that is accessible or visible to the public and in the presence of a witness(es). To investigate the settings where public humiliation occurs, its prevalence, and its impact on victims’ mental health, a systematic review and meta-analysis approach were employed. A total of 33 studies with a sample size of 40,468 were included in the current study. The findings demonstrate the behaviour of public humiliation occurred in a variety of settings (e.g., medical training, healthcare provision, schools) and population groups. The pooled prevalence of experiencing public humiliation was 34.9% (95%CI [0.266, 0.442]). The pooled effect size of experiencing public humiliation on victims’ mental health outcomes was OR = 1.878, 95%CI [1.550, 2.276]. Public humiliation appears to have a substantial impact on victims’ mental health (including symptoms of emotional distress, anxiety, depression; increased stress; posttraumatic stress disorder; suicidal ideation/attempt; Stockholm syndrome, burnout, and being traumatised). A potential mental health pathway model depicting the mechanism underlying the relationship between experiencing public humiliation and mental health is proposed. Recommendations are provided for future research to isolate public humiliation to understand its specific effect on mental health and for developing interventions.
Keywords
Introduction
Public humiliation is a subtype of humiliation when humiliation is witnessed by people in public. Humiliation refers to a deep distressed feeling associated with the perception that one has been unfairly degraded, ridiculed, or belittled, particularly in relation to one's self and identity (Hartling & Luchetta, 1999). Humiliation is associated with negative consequences for the self, including perceived devaluation, significantly low self-esteem, depression, anxiety, post-traumatic stress disorder (PTSD), and suicidal ideation (Harter et al., 2003; Mann et al., 2017; McCauley, 2017). Humiliation is thus categorised as a self-conscious emotion that focuses on the self critically as the object of evaluation by the person him/herself or by others using internal or external standards, rules, or identity goals that are typically built-in shared cultural understandings (Lewis, 2016; Robins & Schriber, 2009; Tracy & Robins, 2007). In contrast to basic emotions (e.g., anger, surprise, disgust, enjoyment, fear, and sadness), self-conscious emotions involve a complex process that requires the capacity to form stable self-representations, to focus attention on those representations, and to activate them to generate a self-appraisal (Robins & Schriber, 2009; Tracy & Robins, 2004). As a result of the complex self-appraisal process (Tracy & Robins, 2007), self-conscious emotions consist of positive (e.g., pride) and negative (e.g., guilt, shame, humiliation, and embarrassment) emotions.
Positive and negative self-conscious emotions have different impacts on a person's behaviour and mental health. For example, pride often motivates achievements to enhance the value placed on the person by others (Sznycer, 2019). Negative self-conscious emotions, however, often raise mental health concerns. For instance, feelings of shame and guilt were significantly correlated with depression (Orth et al., 2006) and PTSD (Beck et al., 2011). Embarrassment is reported as a significant predictor for anxiety and depression (Qualter et al., 2021). Research conducted on the impact of negative self-conscious emotions on mental health has largely focused on shame, embarrassment and guilt, with humiliation only receiving greater attention in recent decades (Elshout et al., 2017; Harter et al., 2003; Hartling & Luchetta, 1999; Klein, 1991; McCauley, 2017).
Humiliation, an intense self-conscious emotion, often results in victims’ memories of a humiliating situation remaining vivid in their minds, regardless of the time that has passed (Klein, 1991). During a humiliating situation where a witness is present, the victim is likely to feel powerless, small, and inferior, which leads them to appraise the situation as unjust, resulting in a unique blend of self-conscious and basic emotions (Elshout et al., 2017). The self-conscious and basic emotions associated with humiliation include shame, disappointment, embarrassment, fear, and anger, and may result in self-directed violent ideation (e.g., suicidal ideation) and revenge (Elshout et al., 2017; Klein, 1991; Mann et al., 2017; McCauley, 2017). Empirical research investigating the neural processing of emotions suggests that a humiliating situation, especially when experienced publicly, is associated with a strong neural response, usually much stronger than other self-conscious emotions that are not specifically tied to a context of humiliation (Mann et al., 2017).
The effects of experiencing humiliation are likely to be more profound when the person being humiliated is self-conscious that the humiliating instance is witnessed by others in public (Mann et al., 2017); the humiliating experience becomes public humiliation. Public humiliation remains unclearly defined in the literature. One of the few definitions is that public humiliation is an experience of purposeful embarrassment caused by a perpetrator with negative intent (Markman et al., 2019). This definition focuses on the behavioural aspect of public humiliation and suggests that public humiliation is brought about by embarrassment, which tends to oversimplify the complex self-conscious emotion of humiliation. Moreover, the definition fails to reflect the nature of the humiliation being a public act because the purposeful embarrassment could be caused by a perpetrator with negative intent in a private setting without a witness(es). A lack of conceptual clarity to address the public nature of humiliating experiences leads to difficulties in distinguishing the focal concept of humiliation from other similar concepts, such as embarrassment and shame (Podsakoff et al., 2016), which limits research in understanding the full scope and impacts of public humiliation.
In the current systematic review, (experiencing) public humiliation refers to the behavioural instance of being humiliated in public, while humiliation refers to the affective aspect of the self-conscious emotion of humiliation. As such, the working definition of experiencing public humiliation for this review is the humiliation that is caused by a perpetrator or perpetrators with negative intent at a location that is accessible (with or without charge of fees) or visible to the public and in the presence of a witness(es). This working definition of experiencing public humiliation reflects Klein's (1991) triangular prototypic explanation of humiliation, which includes a humiliator who inflicts disparagement, a victim who experiences it as disparagement, and a witness(es) who observes it. Aligned with the working definition, this review excludes humiliation experienced in a domestic setting or a public place without a witness(es).
Public humiliation occurs in various settings including teaching/training by public humiliation in medicine (Grover et al., 2020), sports (Gervis & Dunn, 2004), the workplace (Lee & Lee, 2022), schools (Geiger, 2017), and punishment by public humiliation in immigration detention centres (Cleveland et al., 2018). Literature on public humiliation suggests that prevalence varies dependent on the settings and target populations. For example, studies investigating teaching by public humiliation in medical training have reported that between 5.7% and 37% of medical trainees have experienced public humiliation (Grover et al., 2020; Hallett et al., 2012; Harth et al., 1992). The experience of public humiliation occurring in workplaces ranged from 5.7% to 78% (Gadit & Mugford, 2008; Lee & Lee, 2022; Vessey et al., 2009).
According to Leask (2013), public humiliation is a demonstrative exercise of power against the victim, through which the victim experiences the ‘stripping of status, rejection or exclusion, unpredictability or arbitrariness, and a personal sense of injustice matched by the lack of any remedy for the injustice suffered’ (p. 131). Often, public humiliation occurs when there is an imbalance of power between the parties involved (de Wet, 2014). For example, in the medical training environment, where there is often a power imbalance between medical students and educators, public humiliation has been identified as the most common form of mistreatment (Cheng et al., 2020; Daugherty et al., 1998; Markman et al., 2019). This form of mistreatment often leads to medical student burnout (OR = 7.6, 95% CI [1.7, 34.4]) and poor mental health (Markman et al., 2019), including symptoms of anxiety and depression (OR = 3.8, 95% CI [1.6, 9.1]) (Cheng et al., 2020), emotional distress, alcohol abuse, prescription and/or illegal drug abuse (Daugherty et al., 1998), and feeling angry, embarrassed, fearful, and traumatised (Harth et al., 1992).
The impact of public humiliation on mental health may be understood by the perception of the public self; that is, the self as perceived by others (Robins & Schriber, 2009). The focus of attention in public humiliation is directed towards the public self, whereby the self is lowered and belittled in the eyes of others—losing social status, esteem and/or dignity—resulting in the person feeling humiliated (Elison & Harter, 2007). As such, acts of public humiliation provoke the victim's self-conscious emotions of humiliation, shame, embarrassment, and guilt. The self-conscious emotions may, in turn, elicit the basic emotions of anger and fear (Elison & Harter, 2007). These self-conscious and basic emotions may collectively contribute to the negative impact of public humiliation on the victim's mental health.
Although the term public humiliation has been frequently used in research, our searches in Cochrane, PROSPERO, and six databases (MEDLINE, Emcare, CINAHL Complete, PsycInfo, ERIC, and PubMed) indicated there were no systematic reviews and meta-analyses on the prevalence of experiencing public humiliation and its effect on victims’ mental health. This study aims to address this research gap by systematically reviewing existing empirical studies on public humiliation to answer the following research questions (RQs):
RQ1: Where are the settings public humiliation has occurred? RQ2: What is the pooled prevalence of experiencing public humiliation? RQ3: What are the effects of experiencing public humiliation on victims’ mental health?
Methods
The current systematic review and meta-analysis was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol (Page et al., 2021).
Inclusion and exclusion criteria
Inclusion criteria included qualitative, quantitative, and mixed-methods studies published in peer-reviewed journals, which examined how public humiliation, which takes place in an area that is accessible or visible to the public with a group of people present, affecting victims’ mental health.
Exclusion criteria included studies on humiliation that occurred in a domestic setting or public place without witness(es), where the outcomes of the studies were not related to mental health, where studies did not clearly separate humiliation and public humiliation. Additionally, studies where the target population were people with mental disorders, and books, theses/dissertations, non-empirical articles (e.g., editorial, opinion articles, letter to editors, and comments), and non-English publications were excluded.
Search strategy
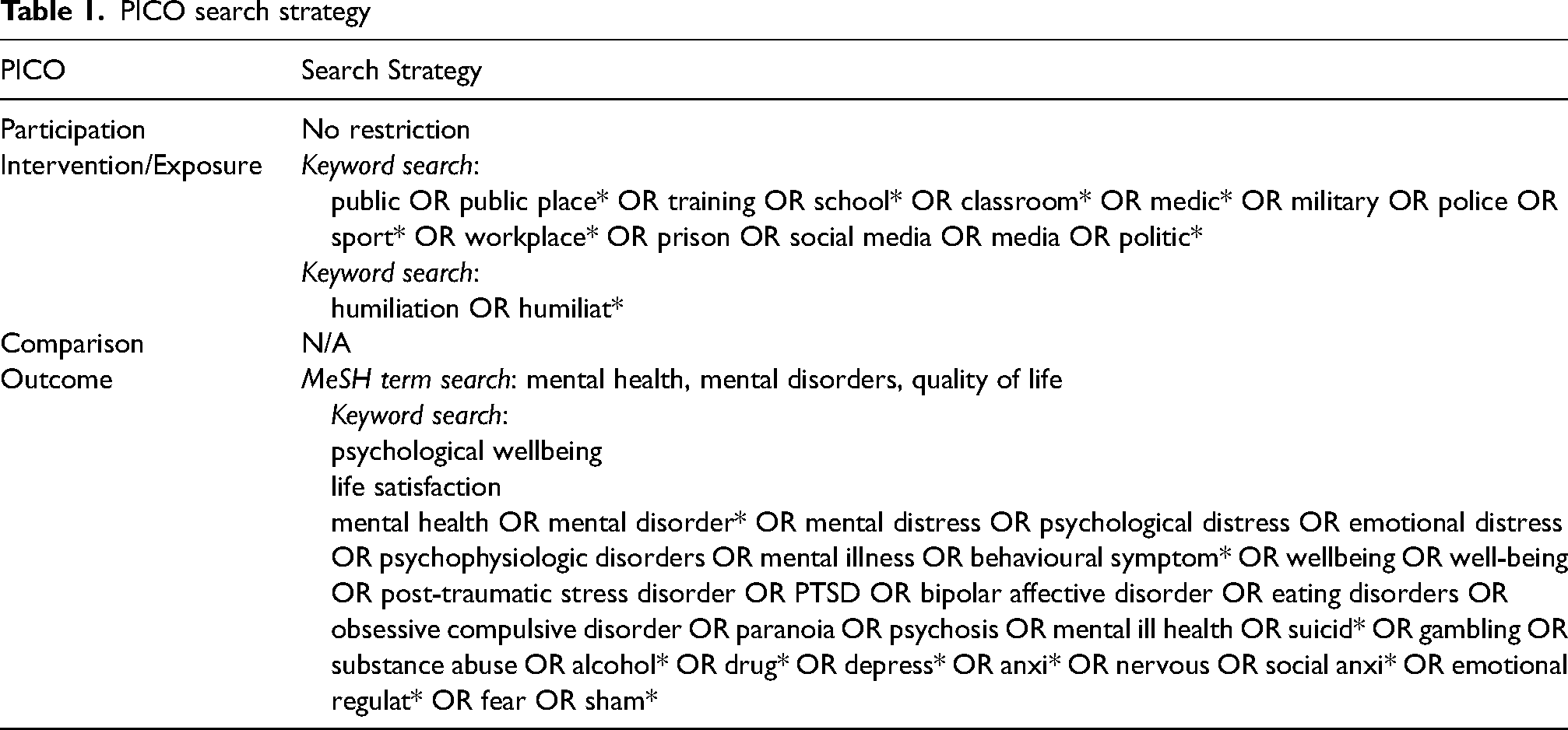
The data search for papers published since the inception of the databases was conducted on 29 April 2022 in six electronic databases (MEDLINE, EMCARE, CINAHL, PsycInfo, PubMed, and ERIC) by the first author (WL). Both Medical Subject Headings (MeSH) terms and keywords were used in the search. Table 1 presents the search strategy using the Cochrane's PICO (participants, interventions, comparisons, outcomes) search tool (Higgins et al., 2021). The fourth author (BA) repeated the search on 9 May 2022, resulting in a similar result (N = 2,068) to the first author's search (N = 2,062). An updated search was conducted on 3 May 2023 to retrieve articles published in the past 12 months, resulting in 185 new publications. The details of the searches are shown in S1 in the Online Supplemental Materials.
PICO search strategy
Study selection
As a first step in selecting studies, the titles and abstracts were screened against the inclusion and exclusion criteria. To determine whether the retrieved articles met the inclusion and exclusion criteria, authors independently assigned codes of ‘yes’, ‘no’, or ‘maybe’. Screening of all retrieved records was conducted by the first author. The remaining authors each reviewed 150–300 records. Studies unanimously coded as ‘yes’ qualified for full-text assessment, while studies undisputedly coded as ‘no’ were excluded. The studies coded as ‘maybe’ or with divergence were discussed among the authors until agreement was reached to include or exclude them (Fisher et al., 2023; Freedman et al., 2024; Li et al., 2021).
The full-text assessment using the Mixed Methods Appraisal Tool (MMAT; Hong et al., 2019) was the second step for study selection and was undertaken by three authors (WL, BA, and AM). Fleiss’s kappa (k) was used to assess the inter-rater agreement indexes: k < .20 indicates poor agreement, while k = .20–.39, .40–.59, .60–.79, and .80–1.00 indicate fair, moderate, substantial, and perfect agreements, respectively (Fleiss, 1971). There were five articles with k < .40 that the three raters deliberated on, and a post-discussion rating was conducted with ks over .40.
Data extraction
Data were extracted using a standard data-extraction form that included columns for the authors, publishing year, country, research methods, sample size, demographic variables, setting/context, and prevalence of experiencing public humiliation, and effects of experiencing public humiliation on victims’ mental health. To determine the evidence supporting the findings in each study, three authors (WL, BA, and AM) independently evaluated the extracted data using the codes of ‘unequivocal’, ‘credible’, or ‘unsupported’. The evaluation agreement was calculated by an agreement index = ((Nunequivocal + Ncredible) / Nreviewers) (Astridge et al., 2023; Fisher et al., 2023; Li et al., 2021). The evaluation agreement indexes ≥ 0.80 were included in this systematic review. All articles’ agreement indexes were higher than 0.80 without post-discussion.
Data synthesis
The data synthesis process was comprised of narrative synthesis and meta-analysis. The narrative synthesis was conducted following three steps: (1) developing a preliminary synthesis by tabulating the data using the standard data-extraction form, translating the data through thematic analysis as presented in the data-extraction form, grouping and clustering themes, and vote-counting of emergent themes; (2) exploring relationships within and between studies to identify similarities and differences across the included studies; and (3) assessing the robustness of the synthesis by employing best evidence synthesis in which only studies meeting standards of methodological adequacy (e.g., MMAT inter-rater agreement k > .40) and relevance to the review were included (Leamy et al., 2011; Popay et al., 2006).
The meta-analysis was conducted employing the Comprehensive Meta-Analysis V4 (Borenstein et al., 2013) using the random-effects model. The effect-size index of event rate was used to estimate the pooled prevalence of experiencing public humiliation. The effect-size index of odds ratio (OR) was employed to report the pool effect size of experiencing public humiliation on the victims’ mental health. For studies reporting multiple prevalence of experiencing public humiliation (e.g., public humiliation by different sources and with different frequencies) and effect sizes of experiencing public humiliation on mental health (e.g., multiple effect sizes on different frequencies of alcoholic drinks), a two-step meta-analysis was conducted (Astridge et al., 2023; Fisher et al., 2023). A synthetic effect size for the study was first computed using the fixed-effect model, the result of which was then entered into the main meta-analysis (Freedman et al., 2024; Leow et al., 2024). The results of the analyses are presented in S2 and S3 in the Online Supplemental Materials.
Study heterogeneity was evaluated with I squared (I2). According to Borenstein (2019), I2 = 25, 50, and 75 and over represent low, medium, and high heterogeneity, respectively. The significance of the p value of the Q-test indicates substantial heterogeneity. Prevalence studies do not perform statistical significance tests, therefore publication bias, the assumption that studies are not published because their findings are not significant (Borenstein, 2019), was not assessed. Egger’s test was performed to detect potential publication bias.
Assessing risk of bias in included studies
The Prediction Model Study Risk of Bias Assessment Tool (PROBAST) was employed to assess the risk of bias and concerns with regards to the applicability of the included studies (Wolff et al., 2019). Four domains (participants, predictors, outcome, and analysis) were applied to the evaluation that rates risk of bias as low, high, or unclear. The overall risks of bias across the four domains of all included articles were rated as low by two authors (WL and BA).
Results
The current systematic review was registered in the Open Science Framework (https://osf.io/8n2rk) on 3 May 2023 after the repeat search and before the data re-extraction. The PRISMA flow diagram (Page et al., 2021) of included and excluded articles is shown in Figure 1. The full text of one study was not available. The corresponding author was approached to request the full test and the study was excluded due to no response being received. A final sample of 33 studies were included in the systematic review and 19 studies were included in the meta-analysis.
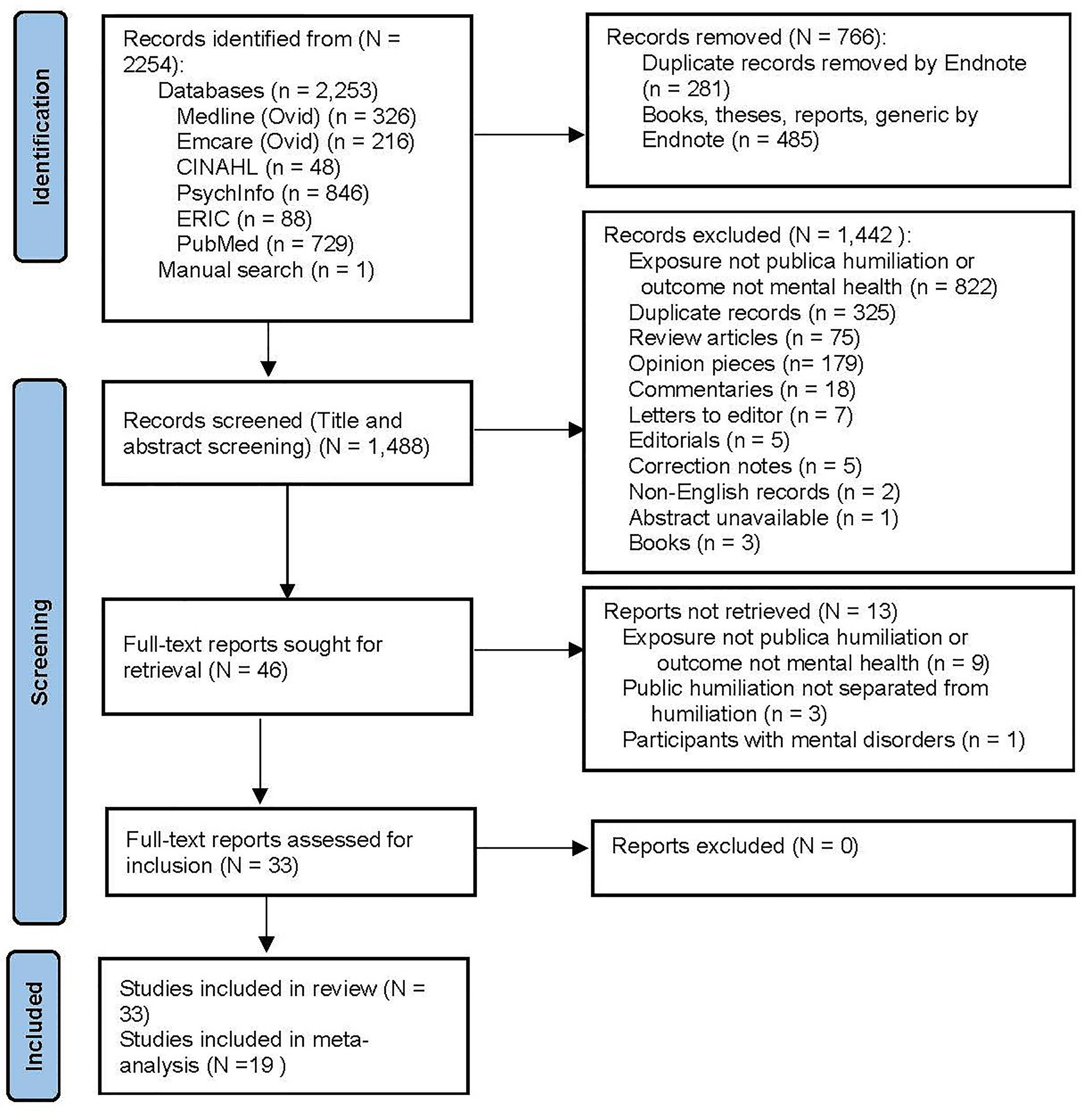
The PRISMA flow diagram.
Among the 33 studies, eight were conducted in the USA, followed by the UK (n = 3), Canada (n = 3), Australia (n = 2), South Africa (n = 2), and France (n = 2). There was one study in each of the following countries: Austria, Denmark, Germany, Ghana, Iran, Israel, Italy, Kosovo, Nigeria, Pakistan, Poland, South Korea, and Turkey. The sample size of the individual studies varied considerably (n = 1–12,040). The total number of participants was 40,468. The summary of the included studies is reported in Table 2.
Summary of the included studies
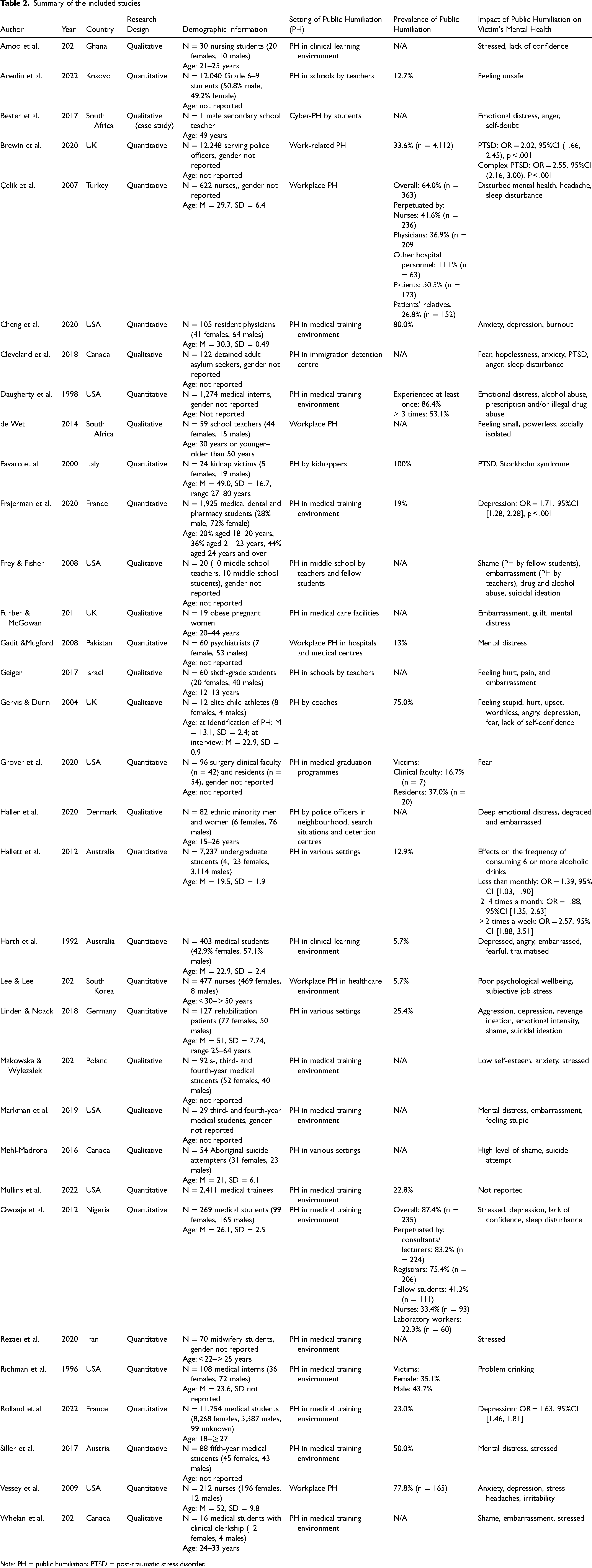
Note: PH = public humiliation; PTSD = post-traumatic stress disorder.
Analysis of RQ1: The settings where public humiliation occurred
To answer RQ1, narrative synthesis was conducted. Fifteen of the 33 (45.5%) included studies reported public humiliation of medical residents/interns/students and nursing students in the medical training environment (Amoo et al., 2021; Cheng et al., 2020; Daugherty et al., 1998; Frajerman et al., 2022; Grover et al., 2020; Harth et al., 1992; Makowska & Wylezalek, 2021; Markman et al., 2019; Owoaje et al., 2011; Rezaei et al., 2020; Richman et al., 1996; Rolland et al., 2022; Siller et al., 2017; Whelan et al., 2021). Public humiliation was primarily perpetrated by medical educators, including consultants/lecturers, physicians, registrars, nurses, and other hospital personnel. Additionally, medical trainees were publicly humiliated by patients, patients’ relatives, and their fellow students.
Five out of 33 studies (15.2%) reported public humiliation in healthcare facilities against nurses, psychiatrists, and obese pregnant patients (Celik et al., 2007; Furber & McGowan, 2011; Gadit & Mugford, 2008; Lee & Lee, 2022; Vessey et al., 2009). The perpetrators of public humiliation against nurses and psychiatrists were mainly patients and their family members (Celik et al., 2018; Gadit & Mugford, 2008; Lee & Lee, 2022; Vessey et al., 2009), while the perpetrators of public humiliation against obese pregnant women were their doctors and midwives (Furber & McGowan, 2011).
Three studies (9.1%) investigated instance where teachers and peers publicly humiliated middle school students (Arenliu et al., 2022; Frey & Fisher, 2008; Geiger, 2017). Three studies (9.1%) explored public humiliation without specific settings, including public humiliation in any aspect of their everyday lives. The participants in the studies included undergraduate students (Hallett et al., 2012), patients in a rehabilitation centre (Linden & Noack, 2018), and Aboriginal people from Canada who had attempted suicide (Mehl-Madrona, 2016).
Seven studies (21.2%) each reported one of the following public humiliation experiences by the participants: a secondary school teacher experiencing cyber public humiliation by students (Bester et al., 2017); school teachers experiencing workplace public humiliation (de Wet, 2014); serving police officers experiencing work-related public humiliation (Brewin et al., 2020); detained adult asylum-seekers experiencing public humiliation in an immigration detention centre (Cleveland et al., 2018); kidnap victims experiencing public humiliation by kidnappers (Favaro et al., 2000); elite child athletes experiencing public humiliation by their coaches (Gervis & Dunn, 2004); and people from ethnic minorities experiencing public humiliation by police officers in their neighbourhoods, search situations, and detention centres (Haller et al., 2020).
Analysis of RQ2: The pooled prevalence of experiencing public humiliation
Meta-analysis was employed to test RQ2. Of the 33 included studies, 19 recorded prevalence of experiencing public humiliation ranging from 5.7% to 87.4% (Arenliu et al., 2022; Brewin et al., 2020; Celik et al., 2007; Cheng et al., 2020; Daugherty et al., 1998; Frajerman et al., 2022; Gadit & Mugford, 2008; Gervis & Dunn, 2004; Grover et al., 2020; Hallett et al. 2012; Harth et al., 1992; Lee & Lee, 2022; Linden & Noack., 2018; Mullins et al., 2022; Owoaje et al., 2011; Richman et al., 1996; Rolland et al., 2022; Siller et al., 2017; Vessey et al., 2009). The results of meta-analysis on the 19 studies with 51,468 participants showed a pooled estimate of prevalence was 34.9%, 95%CI [0.266, 0.442]. Figure 2 presents the forest plot of the results.
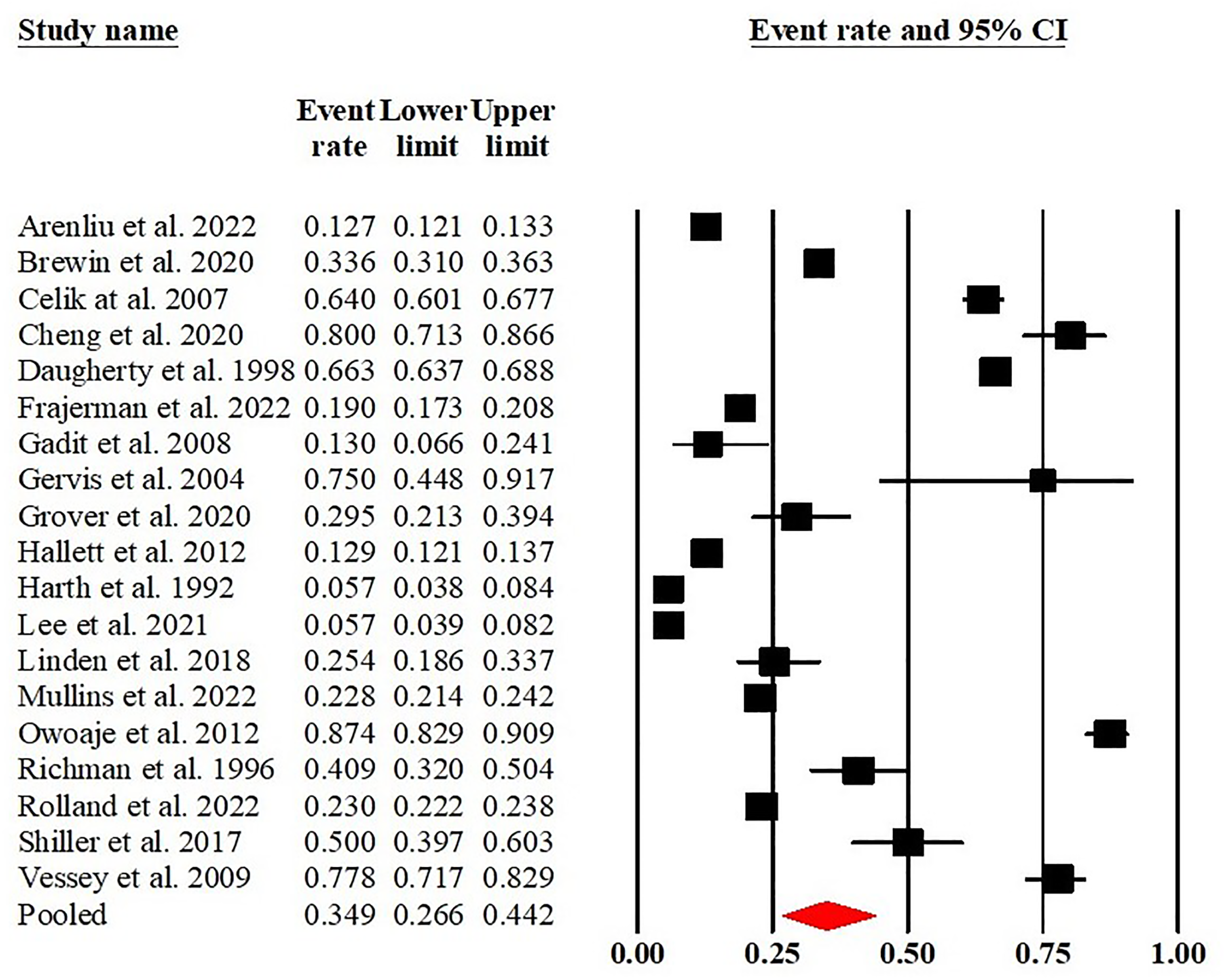
The forest plot of the meta-analysis of prevalence of public humiliation.
The heterogeneity indicator I2 = 99.48 (p < .001) indicated that heterogeneity among the studies was substantial, which warranted moderator analysis using meta-regression for metric variables and subgroups analysis for categorical variables. Moderators of sample size and publishing year were entered into the regression models. The meta-regression results found that country (study location; Q = 32.2, df = 10, p < .001), victim type (Q = 8.74, df = 3, p = 0.033), and publishing year (Q = 67.14, df = 12, p < .001) significantly contributed to the variations in the observed prevalence. Public humiliation setting (Q = 2.31, df = 2, p = 0.314) and sample size (Q = 5.17, df = 4, p = 0.271) were not predictive of the differences in the observed prevalence. Subgroup analyses were performed to explore the variations in prevalence based on the categorical variable of the public humiliation settings, victim type, and country using Q-test. The result of Q-test on public humiliation settings suggested a low level of heterogeneity (Q = 4.286, df = 2, p = .117). The Q-test on victim types of public humiliation (medical students, healthcare workers, and others) corresponded to the results of the Q-test of public humiliation settings (medical training, healthcare environments, and other). The result of Q-test on counties where public humiliation was present suggested significant heterogeneity (Q = 15.305, df = 3, p = .002).
A comparison analysis of prevalence in different settings where public humiliation occurred was conducted as a post-hoc analysis for RQ2. The prevalence in the following three settings was compared: medical training (Cheng et al., 2020; Daugherty et al., 1998; Frajerman et al., 2022; Grover et al., 2020; Harth et al., 1992; Mullins et al., 2022; Owoaje et al., 2011; Richman et al., 1996; Rolland et al., 2022; Siller et al., 2017), healthcare environments (Celik et al., 2007; Gadit & Mugford, 2008; Lee & Lee, 2022; Vessey et al., 2009), and other (Arenliu et al., 2022; Brewin et al., 2020; Gervis & Dunn, 2004; Hallett et al., 2012; Linden & Noack, 2018). The results indicated that the prevalence in these three settings was 40.1%, 95%CI [0.289, 0.523], (I2 = 99.07, p < .001); 34.3%, 95%CI [0.190, 0.537], (I2 = 99.37, p < .001); and 25.3%, 95%CI [0.141, 0.411], (I2 = 99.02, p < .001) respectively. The prevalence of public humiliation in those three settings reflected the prevalence of three victim types with the settings of medical training, healthcare environments, and other corresponding to medical trainees, healthcare workers, and others, respectively.
Analysis of RQ3: The effects of experiencing public humiliation on victims’ mental health
Both meta-analysis and narrative synthesis were used to answer RQ3. The meta-analysis included four studies with 33,164 participants, which quantified the effect of experiencing public humiliation on victims’ mental health outcomes, including PTSD (Brewin et al., 2020), depression (Frajerman et al., 2022; Rolland et al., 2022), and alcohol abuse (Hallett et al., 2012). The pooled effect size of public humiliation on victims’ mental health outcomes was OR = 1.878, 95%CI [1.550, 2.276], p < 0.001. Figure 3 presents the forest plot of the results.
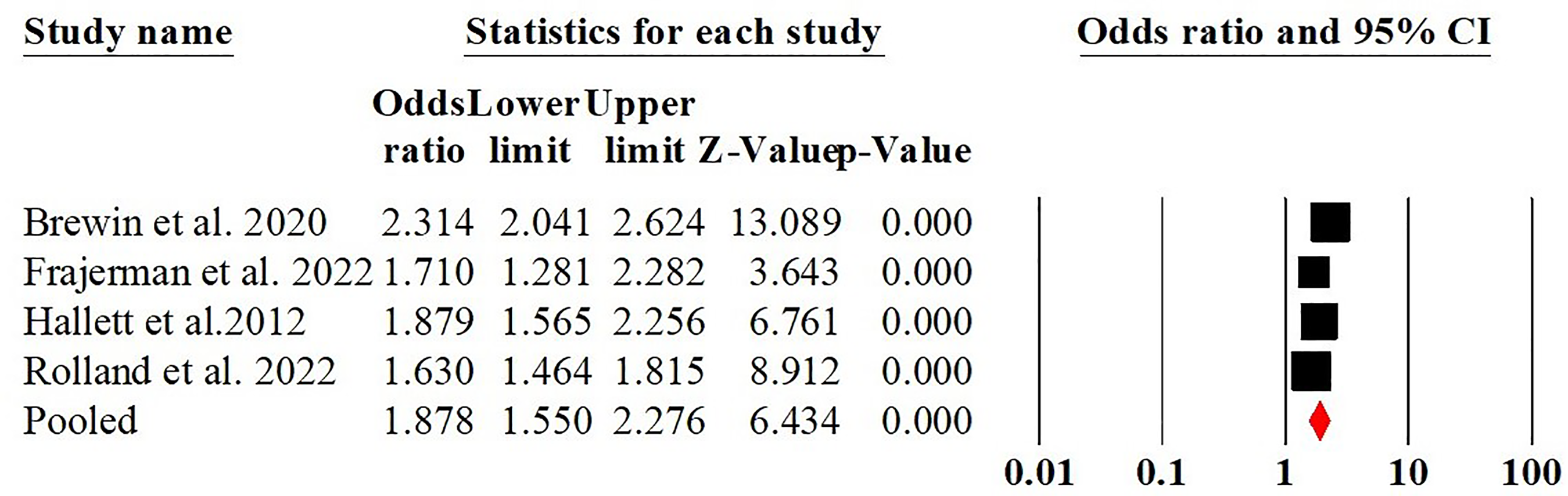
The forest plot of the meta-analysis of effects of public humiliation on mental health.
The heterogeneity indicator I2 = 83.04 (p < .001) indicated that heterogeneity was substantial, warranting moderator analysis using meta-regression. The moderator analyses for metric variable using meta-regression suggested that sample size (Q = 0.23, df = 1, p = .632) and publishing year (Q = 0.06, df = 1, p = .799) were not predictive of the differences in the observed prevalence. Due to the small number of included studies, subgroup analysis on categorical variables (e.g., country, victim type, public humiliation setting, and mental health outcomes) were not explored due to insufficient studies for the number of covariates. Hence, the factors contributing to the heterogeneity remained unclear. The Egger's test (intercept = 0.196, t = 0.043, df = 2, p = .485) suggested that publication bias was not detected.
The narrative synthesis found that of the 33 included studies, eight reported mental/emotional distress as a result of experiencing public humiliation (Bester et al., 2017; Daugherty et al., 1998; Furber & McGowan, 2011; Gadit & Mugford, 2008; Haller et al., 2020; Linden & Noack, 2018; Markman et al., 2019; Vessey et al., 2009); seven reported depression (Cheng et al., 2020; Frajerman et al., 2022; Gervis & Dunn, 2004; Harth et al., 1992, Linden & Noack, 2018; Rolland et al., 2022; Vessey et al., 2009); six reported stress (Amoo et al., 2021; Owoaje et al., 2011; Richman et al., 1996, Siller et al., 2017; Vessey et al., 2009; Whelan et al., 2021); four reported anxiety (Cheng et al., 2020; Cleveland et al., 2018; Makowska & Wylezalek, 2021; Vessey et al., 2009) and alcohol/drug abuse (Daugherty et al., 1998; Frey & Fisher, 2008; Hallett et al., 2012; Richman et al., 1996); three reported PTSD (Brewin et al., 2020; Cleveland et al., 2018; Favaro et al., 2000) and suicidal ideation/attempt (Frey & Fisher, 2008; Linden & Noack, 2018; Mehl-Madrona, 2016). Other effects on participants’ mental health included feeling unsafe (Arenliu et al., 2022), Stockholm syndrome (Favaro et al., 2000), burnout (Cheng et al., 2020), feeling socially isolated (de Wet, 2014), and trauma (Harth et al., 1992).
Nine studies found that experiencing public humiliation was associated with several negative self-conscious emotions, including embarrassment (Frey & Fisher, 2008; Furber & McGowan, 2011; Geiger, 2017; Haller et al., 2020; Harth et al., 1992; Markman et al., 2019; Whelan et al., 2021), shame (Frey & Fisher, 2008; Lee & Lee, 2022; Mehl-Madrona, 2016; Whelan et al., 2021), and guilt (Furber & McGowan, 2011). Additionally, five studies reported that experiencing public humiliation was associated with two basic emotions, fear (Cleveland et al., 2018; Gervis & Dunn, 2004; Grover et al., 2020; Harth et al., 1992) and anger (Bester et al., 2017; Cleveland et al., 2018; Gervis & Dunn, 2004; Harth et al., 1992). Four studies reported physical symptoms, including sleep disturbance (Celik et al., 2007; Cleveland et al., 2018; Owoaje et al., 2011) and headache (Celik et al., 2007; Vessey et al., 2009).
Discussion
The current systematic review and meta-analysis aimed to investigate the prevalence of experiencing public humiliation and the effects on victims’ mental health. A total of 33 studies with 40,468 participants were included in the systematic review and 19 studies were included in the prevalence meta-analysis.
The analysis of RQ1 and subgroup meta-analysis in RQ2 indicated that near half of studies (45.5%) reported public humiliation in medical/clinical training environments, with nearly half (a pooled prevalence of 40.1%) of medical trainees experiencing public humiliation. The Medical School Graduation Surveys conducted by the Association of American Medical Colleges (AAMC), indicate that public humiliation, specifically, teaching by humiliation (Scott et al., 2015), is consistently the most common form of mistreatment experienced by medical students in medical training programmes (AAMC, 2021; Daugherty et al., 1998; Markman et al., 2019). There is a concern about the phenomenon of teaching by public humiliation, particularly if the students who are now victims of public humiliation become future perpetrators of public humiliation against their own students, perpetuating a negative culture within medical education.
Teaching by public humiliation appears to be a manifestation of medical trainees’ relational powerlessness and reflects the superior–subordinate relationship between trainers and trainees (de Wet, 2014). The more powerful medical trainers employ the tactic of teaching by public humiliation to assert their power over their less powerful trainees. As discussed by Hodson et al. (2006), power and powerlessness are fundamentally relational in nature. Both individual and organisational power are likely to contribute to the creation and maintenance of teaching by public humiliation. Medical educational institutes should look beyond the current understanding of teaching by humiliation at the individual level. Medical educational institutes need to consider how their policies and procedures exercise institutional power that protect and reinforce dominant power structures (Hodgins et al., 2020) within the medical training culture, permitting the abuse of power and ill-treatment of medical trainees.
Public humiliation in healthcare facilities is additionally concerning, with 34.3% of healthcare participants reporting experiences of public humiliation within the workplace. Empirical studies have reported that doctors and nurses who are victims of public humiliation experience substantially higher rates of psychological distress (Bourne et al., 2014; Li et al., 2020; Schwenk et al., 2008). Future studies should explore the contribution of public humiliation to the high prevalence of mental distress among healthcare professionals.
The analysis of RQ1 also indicates that public humiliation was widely experienced in a variety of settings, among a variety of populations including school students, young athletes, obese pregnant women, detained adult asylum-seekers, people from culturally and linguistically diverse backgrounds, schoolteachers, coaches, doctors, midwives, detention centre officers, and police officers. Future research should continue to explore the different experiences of public humiliation on different populations and further explore the role of relational powerlessness.
The test of RQ2 indicated that on average 34.9% of the participants in the included studies experienced public humiliation and the mean prevalence in the universe of comparable studies is likely to fall between 26.6% and 44.2%. Results also indicated that heterogeneity in the prevalence among the included studies was substantial. The substantial level of heterogeneity, which was partially predicted by study location and publishing year, suggests that the prevalence of public humiliation is low in some populations and very high in others (Borenstein, 2019). Caution thus needs to be exerted when generalising the findings in different populations.
The analysis of RQ3 showed that public humiliation appears to have a substantial effect on victims’ mental health. The meta-analysis result indicated that the odds of mental health problems was 1.878 times higher in people who experienced public humiliation compared to those who did not (OR = 1.878, 95%CI [1.550, 2.276]). It is pertinent to note that this meta-analysis was based on a small number of studies (n = 4), which may not be adequate for reaching definitive conclusions. Heterogeneity among the studies was substantial, contributing factors of which were not identified due to the small number of studies included in the meta-analysis. Caution is needed when applying the findings to different populations. The narrative synthesis results showed that the mental health outcomes caused by experiencing public humiliation included mental/emotional distress, stress, depression, anxiety, alcohol/drug abuse, PTSD, suicidal ideation/attempt, Stockholm syndrome, burnout, and traumatisation. Experiencing public humiliation appears to evoke the high-intensity self-conscious emotion of humiliation, which has a negative direct effect on victims’ mental health. Humiliation as a self-conscious emotion appears to be associated with other negative self-conscious emotions (e.g., embarrassment, shame, and guilt), which in turn are positively associated with mental health conditions. Furthermore, humiliation appears to be associated with two basic emotions, fear and anger, which in turn are positively associated with mental health impacts. These findings lead to a potential pathway model that depicts the mechanism underlying the relationship between experiencing public humiliation and mental health, as shown in Figure 4. Future empirical studies are warranted to evaluate the proposed pathway, investigating the intermediate mechanism through which public humiliation exerts its influence on victims’ mental health.
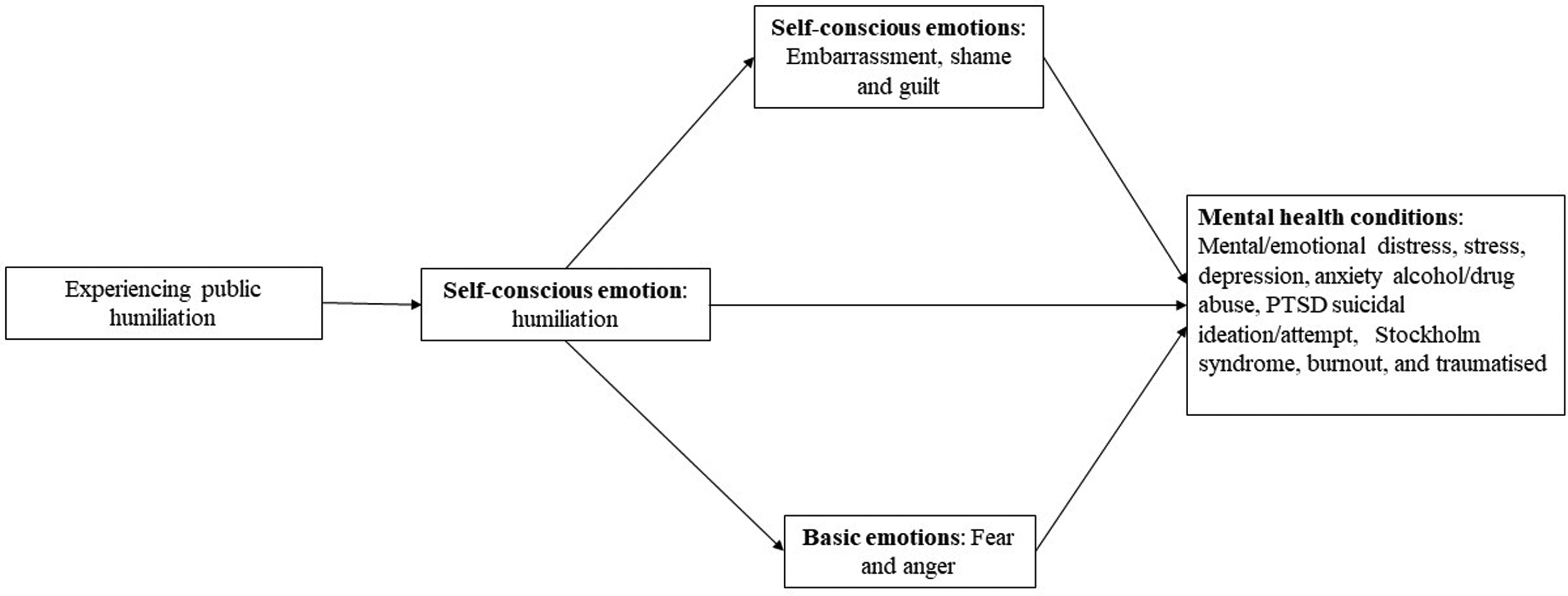
Proposed pathway model of the relationship between experiencing public humiliation and mental health.
Several limitations within this systematic review are identified as follows. First, although this review seeks to distinguish the emotions associated with humiliation (representing a self-conscious emotion) from the behavioural instances of public humiliation (referring to the actions the humiliator takes), separating the behaviour from the affective state(s) associated with it remains a challenging task. Future research to theorise and classify humiliation as a discrete emotion is needed. Second, based on the inclusion and exclusion criteria, studies that investigated only the prevalence of public humiliation without investigating its impact on mental health were excluded from this systematic review. This limitation warrants future meta-analysis that include all studies estimating the prevalence of public humiliation. Third, in most of the included studies, the investigation of public humiliation was embedded in the investigations of bullying and abuse. It is possible that the model presented (Figure 4) is consequential to the bullying or abuse rather than the public humiliation. Considering the high prevalence of experiencing public humiliation and the negative impact on the mental health of victims, stand-alone investigations of public humiliation are warranted. To achieve this goal, developing a conceptual definition of public humiliation that differentiates it from bullying and abuse distinctions is needed. Fourth, studies on public humiliation in social media are surprisingly limited. Further research into cyber public humiliation should be undertaken considering the high incidence of cyber bullying and public shaming in social media. Fifth, the heterogeneity of mental health outcomes and absence of measures of outcome severity (e.g., whether people terminated employment and/or study because of public humiliation) in included studies limits the analysis in the current meta-analysis. These limitations of this systematic review and in the research field of public humiliation in general justify further research.
Conclusion
Findings from this review indicate that public humiliation and the consequential self-conscious emotional impact affect the mental health of those that experience them. There is, however, a need for further research to confirm the impact of public humiliation, distinct from abuse or bullying, on the mediating self-conscious and basic emotions and subsequent impact on victims’ mental health. It is our hope that the current review will enable researchers to gain an understanding of what public humiliation is, where it is commonly employed, and the mental health consequences, as well as provide useful information for developing future theoretical and methodologically sound studies to advance this field. Importantly this review highlights the need for intervention in settings where public humiliation is more prevalent, and we hope that this will motivate researchers, policymakers, and administrators to work in this context to relieve unnecessary suffering and the perpetuation of the cycle of public humiliation.
Supplemental Material
sj-docx-1-pac-10.1177_18344909241252325 - Supplemental material for Prevalence of experiencing public humiliation and its effects on victims’ mental health: A systematic review and meta-analysis
Supplemental material, sj-docx-1-pac-10.1177_18344909241252325 for Prevalence of experiencing public humiliation and its effects on victims’ mental health: A systematic review and meta-analysis by Wendy Wen Li, Carolyn Heward, Alyssia Merrick, Belinda Astridge and Timothy Leow in Journal of Pacific Rim Psychology
Footnotes
Acknowledgments
The authors thank our librarian Mr. Stephen Anderson for his help with search terms.
Author contributions statement
WL contributed to the study design, database search, data analysis, and writing the manuscript. CH, AM, and BA contributed to the study design, database search, data analysis, and critically reviewing and editing the manuscript. TL contributed to data screening, and critically reviewing and editing the manuscript. All authors approved the final version of the manuscript.
Data-sharing statement
The data presented in this study can be accessed in the Online Supplementary Materials.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.