
Abstract
COVID-19 has brought awareness of the daily threat of death to everyone in the world and provided a natural context for raising widespread awareness of the salience of mortality. Previous researchers have found that mortality salience has rendered proposers more likely to make a fair offer in the dictator and ultimatum game, but there has been no study focusing on the psychological changes in the responders. Study 1 was an exploratory study of the effect of mortality salience on the threshold for acceptance of unfair offers, comparing the effect of unnatural deaths, such as those caused by COVID-19, and that of natural deaths, such as those caused by aging. The results showed that COVID-19 mortality salience could lower the acceptance threshold in responders, thus increasing their tolerance of unfairness, while the mortality salience from aging would not. In Study 2, we established an evolutionary game model to simulate the influences of tolerance of unfairness in allocation of resources on epidemic spread using agent-based modeling. The study compared two societies with different levels of the fear of death, and the results showed that the society with a relatively high death fear would produce more inequality in distribution by increasing the tolerance of unfairness. This ultimately leads to worse pandemic conditions and slower control of the spread in the first stage of the pandemic.
Introduction
Death is a problem everyone will encounter. In daily life, however, death does not come to our mind often. However, since the COVID-19 outbreak in early 2020, information related to death has become more frequently present to our minds. Research has found that death awareness induces changes in an individual's cognition, emotion, and behavior. Past studies have examined these influences across a large variety of aspects, but few have paid attention to the impact on social allocation of resources, especially the mindsets and behavior of people responding to allocation. The present study attempts to focus on this question and explores the influence of those psychological changes on macro-level epidemic development in society.
Mortality salience effect
Terror management theory (Greenberg et al., 1986) is the most influential theory in the domain of mortality salience. It posits that, due to the need to buffer anxiety around death, a set of defensive mechanisms is activated when facing mortality salience, including improving self-esteem and strengthening cultural values and self-identification to gain a sense of abstract immortality (e.g., Greenberg & Kosloff, 2008), which is supported by a large body of research. For example, studies found that mortality salience would induce less dishonest behaviors (Schindler et al., 2019), higher neural activities related to guilt and shame (Xu et al., 2022), more intense punishment of moral violators (e.g., Rosenblatt et al., 1989), and higher prosocial tendencies and altruism (Dong et al., 2019; Dunn et al., 2020; Jin & Ryu, 2022). It would also lead to enhanced ingroup bias, intergroup prejudice and conflict (e.g., Castano et al., 2002; Reiss & Jonas, 2019), more identified religious beliefs (Vail et al., 2019), and firmer political views (Burk, Kosloff & Landau, 2013).
Despite the large body of examinations, studies on the role of mortality salience in resource allocation are limited. One study found that people tended to make a more equal distribution in a dictator game or ultimatum game under a context of heightened mortality salience, in that they were able to derive higher satisfaction from prosocial behaviors (Zaleskiewicz et al., 2015). However, until now, there has been no study focusing on the psychological changes in responders, for example, whether they are more willing to accept or reject lower offers. The first aim of the present research is to address this question and focus on the mortality salience effect on the acceptance of unfair offers among responders.
There has been some discussion on the effect of mortality salience on fairness. It is believed that mortality salience could increase people's adherence to salient norms; thus, fairness would become more important when there is a heightened awareness of death. Studies indeed found that mortality salience could enhance concerns about procedural fairness (Cook et al., 2004) and strengthen the need for organizational justice (Wang et al., 2021). From this perspective, it seems that respondents should be more inclined to decline unfair offers in resource allocations to maintain fairness beliefs.
However, many studies have also discovered that under mortality salience, people have a relatively high tendency towards materialism in terms of higher financial expectations and enhanced materialistic consumption choices, and are greedier when consuming resources (Kasser & Sheldon, 2000; Zein et al., 2020). A context of mortality salience, such as a disaster, would cause people to place more emphasis on possessions and material things (Passannante, 2019; Jiang et al., 2021). These results are also in line with terror management theory, as materialistic pursuits would help reduce the insecurity and uncertainty brought about by death (Chang & Arkin, 2002; Christopher et al., 2006). In addition, mortality salience might enhance the desire for instant gratification, as studies have shown that disasters induce more frequent impulsive consumption (Jiang et al., 2021), and the context of COVID-19 mortality salience increases delay discounting as people are less willing to trade money now for more money in the future (Sonmez, 2021). Therefore, the high tendency to adhere to materialistic things could help reduce insecurity, and this high desire for instant gratification might prompt respondents to accept offers at the cost of some level of fairness in an ultimatum game.
Specifying different types of mortality
Past studies on mortality salience often adopted a typical experimental paradigm to activate death awareness, where participants were instructed to imagine the scenario of their death and write down their emotions, thoughts, and physiological changes (e.g., Greenberg et al., 1994; for a review, see Burke et al., 2010). However, this traditional paradigm did not differentiate the manner of death, simply using the abstract word “death.” There are various manners of death, some of which are abrupt and unnatural, such as death due to a fatal traffic accident, a natural disaster, or the early stage of a dangerous pandemic such as COVID-19, while some deaths are predictable and natural, such as death from aging or progressive illness. We cannot know which specific scenario each participant imagined in the traditional paradigm, but we believe that it is necessary that we take the manner of death into consideration, as priming participants with an awareness of an abrupt and unnatural death might have different mortality salience effects than doing so with awareness of predictive and natural death. The former might induce a higher fear of death that would cause the typical mortality salience effect, while the latter might not.
To date, only one study has paid attention to the manner of death and compared the mortality salience induced by death in a traffic accident and death by aging. The study found that mortality salience induced by traffic accidents increased people's materialism compared to deaths from aging (Wang & Wang, 2012). This was a study in consumer research, but there has been no replication or examination in other research fields. In the present study, we discriminate the contexts between death due to COVID-19 and death due to aging, and suppose that COVID-19 mortality salience might influence respondents’ acceptance threshold to a greater extent than that caused by aging mortality salience and the control conditions.
Influence of unfair resource allocation on epidemic development
During a pandemic such as COVID-19, especially in its early period, social resources such as masks, medicine, medical equipment, and vaccines are very precious and limited. In this case, distribution could be unequal. As shown from World Bank statistics, there are 125.3 vaccines per 100 people in high-income countries and only 45.3 vaccines per 100 people in low-income countries (Rydland et al., 2022). This unequal distribution tends to reoccur within a society. Those who own many resources in hand could gain access to needed resources more easily, while those who do not have many resources were left behind and ignored. There was a computational study that suggested if all agents in society displayed inequality aversion, in that they showed the desire to keep inequality within a certain range, inequality constraints would be built that benefited the vulnerable and delayed the spread of the epidemic (Kordonis et al., 2020).
However, as we assume, if individuals in society have reduced inequality aversion, in that they display a higher tolerance of unfairness and do not exert constraints on inequality, the inequality or unfairness in social resource distribution would be sharpened, which leaves the most disadvantaged with the fewest resources at a high risk of being exposed to the virus. This also tends to be risky for society as a whole and impedes epidemic control. Therefore, we hypothesize that if people have a high tolerance for unfairness due to a high level of the fear of death, this social context would not facilitate epidemic control. Higher fear of death induces tolerance of unfairness, leading to higher inequality in resource allocation, which further impacts the severity and control of the speed of the epidemic. In this way, the epidemic and tolerance of unfairness tend to have some reciprocal influences.
The present study
The present research contained two studies. Study 1 focused on the influence of mortality salience on the tolerance of unfairness among respondents in the ultimatum game. The study modified the traditional mortality salience paradigm using COVID-19 and aging death contexts and compared respondents’ acceptance thresholds under different conditions. It was hypothesized that the acceptance threshold in the ultimatum game under the COVID-19 mortality salience condition would be lower than that under the aging mortality salience condition and the control condition (H1). Study 2 explored the influence of the tolerance of unfairness on epidemic development using agent-based modeling. It compared how societies with high and low tolerances for unfairness induced by the fear of death would influence epidemic severity (total infections, total deaths, days) as well as control speeds (overall speed, stage 1 speed, stage 2 speed). It was hypothesized that a high level of tolerance for unfairness would lead to a more unfair distribution of resources in society, which would further result in higher numbers of infections and deaths, a greater number of days to end the epidemic (H2a), and slower control speeds in both stages (H2b). The whole study demonstrated a loop and bidirectional influence of pandemic fatality and tolerance for unfairness.
Data availability statement
The data and codes that support the findings of this study are available at: https://osf.io/b6zgk/?view_only = 7390203213684366894aa0c99bbbd721.
Study 1
Method
Participants
We recruited 310 participants in this study through the online survey platform Credamo, which is a public response collection website open to anyone. Twenty-two participants were screened out: 11 participants were deleted because their response time was shorter than 200 ms (the average response time was 818 ms); there were some highly similar or duplicated answers (especially in the written part), which might have been answered by the same participant using different devices, and 4 such responses with later answering times were deleted; 7 participants who wrote down contexts unrelated to the instructions (death or dental surgery) were deleted, among whom 5 wrote down senseless words to pad out the paragraph, and 2 wrote down feelings unrelated to the subject without explanation. After screening, 288 valid participants remained. There were 123 males and 165 females, and the age of the participants ranged from 18 to 60, but the majority were between 20 to 40 (as could be seen from Supplemental Figure S2 in Supplementary Material), with a mean age of 28.5 (SD was 7.4). Eight of the participants were in high school, 127 were undergraduate students (including junior college), 42 were postgraduates, 111 were employed (Supplemental Figure S1). The sample was constituted by students as well as working-class participants, and thus has better representativeness than a pure student sample. The average age among the student sample was 26.7, and that among the employed group was 31.3 (Supplemental Figure S3). One plausible reason for the relatively older average age among students probably was that the question asked participants about their current status or identity in life, but some participants interpreted it as asking their education level. So for example, some participants chose “undergraduate” as his/her identity, but wrote down their age as 34 or even 57. This misunderstanding must have elevated the student group's average age. The geographical locations of the sample were widespread across China, covering 30 provinces, municipalities, and autonomous regions. A post hoc sensitivity analysis of a one-way ANOVA with 288 participants across three groups was carried out using Gpower (Faul et al., 2009), and it was sensitive to effects of f = 0.18 with 80% power (α=0.05).
Procedure
Participants were randomly allocated into one of three conditions: the COVID-19 mortality salience condition, the aging mortality salience condition, and the control condition. In the COVID-19 mortality salience condition, participants were first presented with a short paragraph introducing the characteristics of coronavirus, emphasizing the deadliness (details can be found in the supplementary material). Then, participants would see an instruction, “Please spend some time imagining a scenario: you caught the coronavirus unfortunately, the medication isn’t working as expected, and death is approaching …” Participants would imagine the scenario while this page appeared for approximately 20 s. In aging mortality condition, participants were presented with a paragraph introducing aging and death of aging. The imaginary scenario is presented as follows: “You have experienced growth, maturity and the aging process, and now death is approaching …” In the control condition, participants were presented with information on how to perform dental surgery, and the imaginary scenario was as follows: “Now you are about to receive dental surgery …” After reading and imagining, participants in mortality salience conditions were faced with two questions: “What feelings do you have when thinking of death?” and “What changes will happen to your body during and after death?,” which are typical questions used in all mortality salience paradigms. In the control condition, the two questions asked were, “What feelings do you have when thinking of the surgery?” and “What changes will happen to your body during and after the surgery?” After the mortality salience manipulation, participants completed a Positive and Negative Affect Schedule (PANAS; Watson et al., 1988) as a distractor task.
Then, all participants would engage in an ultimatum game as the responder, choosing whether to accept or reject the allocations displayed on the screen. The instruction was Now imagine there is a 100-yuan reward to share between you and one other random participant. He or she will propose an allocation plan, and you have to make a choice to accept or reject it. If you choose to accept it, the allocation will be made according to the plan; if you choose to reject it, neither of you will get the reward.
Before the game, participants would answer the question, “What is the minimum amount of money that you would accept when he or she makes an allocation? Please write down a number between 0 and 100,” as the pretest of their subjective threshold value.
During the ultimatum game, the allocations displayed on the screen started with a fair plan (50–50) and then became gradually more unfair by enlarging the gap between two sides (55–45, 65–35, etc.), until it reached an extremely unfair allocation, 90–10. Then, the allocations gradually became less unfair until they reached 50–50 again. The aim of this orderly display was to determine at which point participants would switch their choice, either from acceptance to rejection or from rejection to acceptance.
After the experiment, participants were instructed to write down their minimum acceptable amount of money again as the posttest of their subjective threshold value. They then answered five questions on their perceived fairness of each allocation and filled in their demographic information at the end of the survey.
Statistical analysis
A one-way ANOVA was conducted with SPSS in this study to examine if there was a significant difference between the acceptance thresholds under three different conditions: COVID-19 mortality salience condition, aging mortality salience condition, and the control condition.
Results
As a manipulation check, we invited two PhD students to encode the frequency of words indicating negative emotion or death-related concepts in the contents of participant answers to the first question after manipulation, that is, “What feelings do you have when thinking of death/the surgery?” In other words, we counted how many words with a negative emotion (e.g., “sad” or “fear”) or with relevance to death (e.g., “death” or “after-life”) participants used in their responses. The consistency between two coders was above 95%, and discrepancies were solved through discussion. Then, we compared the word frequency among the three conditions (COVID-19 mortality, aging mortality, and the control condition) using one-way ANOVA. The results showed that the frequencies of words related to negative emotion and death were significantly different among the three conditions, F (2, 285) = 14.95, p < .001. Post hoc tests showed that target word frequency was significantly higher in the COVID-19 mortality condition (M = 3.57, SD = 1.80) than in the aging mortality (M = 2.73, SD = 1.77), p < .001; and it was also significantly higher than control condition (M = 2.30, SD = 1.25), p < .001, and there was no significant difference between the aging mortality and control conditions, p = .062. Therefore, we concluded that the manipulation of different types of mortality salience and mortality salience relative to the control condition was effective.
For each respondent, we first recorded the offer in the ultimatum game when he or she switched from “accept” to “reject” as the displayed offers became more unfair and determined the lower bound for the acceptance threshold. For example, a participant would choose “accept” for 45 but choose “reject” for 35, and we assumed the lower bound of his threshold was 35. Likewise, we recorded the upper bound when the participant switched from “reject” to “accept” as the offer became fairer. For example, he would choose “reject” for 30 but choose “accept” for 40, and the upper limit of the switch point was assumed to be 40. Then, we averaged the lower and upper bounds to obtain the dependent variable in the analysis, named the acceptance threshold. If participants chose “accept” or “reject” in all of the allocations, then the acceptance threshold was determined by their written responses to the question asking for a minimum acceptance value. The correlation between these two limits was r = .85.
A one-way ANOVA was conducted with mortality salience manipulations as the independent variable and acceptance threshold as the dependent variable. The results were close to significant, F (2, 285) = 2.94, p = .055, effect size f = 0.16, and close to the effect size in sensitivity analysis. Post hoc tests revealed that respondents in the COVID-19 mortality salience condition had a significantly lower acceptance threshold (M = 34.15, SD = 10.91) than those in the control group (M = 37.29, SD = 9.71), p = .029, and were also lower than those in the aging mortality salience group (M = 37.03, SD = 8.99), p = .045. The aging mortality salience group did not differ in acceptance threshold from the control group, p = .85 (Figure 1). Thus, hypothesis (H1) was confirmed. We also obtained statistics for how participants perceived unfair allocations, with perceived fairness calculated by the average ratings of fairness on three unfair allocations: 90–10, 80–20, and 70–30. The ANOVA on perceived fairness did not reveal a significant difference among the three conditions, F (2, 285) = 0.53, p = .59. However, considering the high correlation between perceived fairness and the acceptance threshold, r = −.33, p < .001, we still tested a mediation model with perceived fairness as the mediator between mortality salience conditions and the acceptance threshold, and the results can be found in the supplementary material.

Acceptance thresholds in the ultimatum game under different experimental conditions (error bars indicate SEM; * represents p < .05; ** represents p < .01).
Study 2
Method
We adopted the method of agent-based modeling (ABM) to reveal the influence of the fear of death on epidemic severity through tolerance of unfairness in resource allocation during a pandemic. ABM simulates a complex social system by modeling behaviors and interactions among real individuals (and between individuals and the environment) using virtual agents (Twomey & Cadman, 2002), which is an approach often adopted in studies related to epidemics (e.g., Hoertel et al., 2020).
Model assumptions
We referred to the SEIRD model to describe the development of the COVID-19 epidemic (Korolev, 2020; Huang et al., 2022). A basic SEIRD model includes five types of populations in a society: the susceptible, who are uninfected, healthy people; the exposed, who are infected but haven’t show symptoms; the infected, who are infected and show symptoms; the recovered, who have recuperated from COVID-19 and will not be infected again; and the dead, who are deceased. The model assumes that (a) the susceptible could be infected when the exposed or the infected are in their surroundings; (b) in the infection process, the exposed do not immediately display symptoms such as coughing and fever but experience an incubation period. After the incubation period terminates, they display symptoms and become known infected agents; (c) the infected have a certain possibility of recovering or dying, and the recovered will not be infected again; (d) when there are no longer exposed or infected individuals in society, the COVID-19 virus could not be spread further, and the model terminated.
Parameters and behavioral rules
The model has the following set of parameters and behavioral rules for agents.
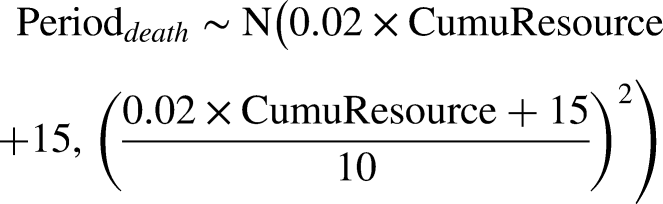
(A) Initial parameters: There are 9,000 agents in society. Ten of the agents are set as initially exposed individuals, who are infected without symptoms, and they are marked in yellow. The remaining 8,990 agents are healthy agents who are susceptible, marked as green. The initial resources of agents in society conform to a normal distribution with a mean of 30 and a standard deviation of 5. The initial fear of death of agents also conforms to a normal distribution, with a mean of 10 and a standard deviation of 2. (B) Rule One: Movement: We assume that during the pandemic, the movement of agents is a behavior governed by probability (Cuevas, 2020), and the probability of movement of agents conforms to a uniform distribution (C) Rule Two: Infection: In society, all agents move randomly based on Rule One. If a susceptible agent is placed near an exposed or infected agent (within the range of a circle with radius of 1 unit), he or she has a probability of becoming infected. The infection probability conforms to a normal distribution (Huang et al., 2022): (D) Rule Three: Incubation and detection: After an agent is infected by another agent, he/she becomes an exposed agent and enters an incubation period before showing symptoms. The incubation period conforms to a normal distribution with a mean of eight days: incubation ∼ N (8, 2). The detection of infection for each exposed agent each day is a probability, influenced by the cumulative resources of the agent. For an exposed agent with higher resources, the detection of being infected is more likely to happen. (E) Rule Four: Recovery or death: Each infected agent must face two kinds of outcomes: to recover or die, and the probability of recovery or death is influenced by the resources he or she owns: (F) Rule Five: Resource allocation: The amount of resources to be allocated each day was fixed. In a society, resources are not allocated to all agents equally, but the Matthew effect is often observed (Perc, 2014). This suggests that the advantaged accumulate resources faster than the disadvantaged, and the more resources they own, the faster their resources increase. Similarly, in the present model, the resource accumulation process was influenced by the initial resources that agents owned. In addition, we supposed that there would be an accelerated Matthew effect under conditions of a high fear of death in this model. Based on the findings from Study 1, death awareness or fear of death could increase the tolerance of unequal resource distribution. We set unfairness acceptance as a societal variable, determined by the average level of the fear of death of all agents.










Model establishment
Based on the above assumptions, parameters, and rules, agent-based modeling was established and run in Netlogo 6.2. Figure 2 demonstrates the evolution of this model at the beginning, after 100 days, and at the end of the process in a random simulation trial and shows how agents in different states changed with time.

Demonstration of the evolution of the model under conditions of high and low death sensitivity.
Results
We compared the development of the epidemic under two societal conditions: death sensitivity = 100 or death sensitivity = 400.
When death sensitivity was 100, the fear of death among agents was low, and the mean level of the fear of death represented the societal level of acceptance of unfairness, which usually fell in the range of [10, 40], with an adjusted ratio of [0.5, 1.28]. When death sensitivity was 400, the fear of death was at a high level, acceptance of unfairness in society usually fell within [10, 220], and the adjusted ratio was within [0.5, 2.65].
We simulated 100 trials for each of the two conditions of societal death sensitivity (100, 400) and compared the severity of the epidemic as well as the rate of spread or speed of the epidemic. For severity, we chose infection number, death number, and the days that the epidemic lasted as dependent variables. The infection number indicates how many total people are infected during the whole epidemic, the death number indicates how many die, and the days are the period length of the epidemic.
We examined the normality of the simulation data using the Kolmogorov–Smirnov (K–S) test. Results revealed that when death sensitivity was low, infected cases conformed to a normal distribution (p = .20), but death number (p < .001) and days (p = .003) did not; and when death sensitivity was high, infected cases did not conform to a normal distribution (p < .001), while death number (p = .20) and days (p = .20) did. Therefore, we conducted Mann–Whitney U non-parametric tests to compare these indicators. Results showed that when death sensitivity was at a high level, the average infected number (M = 2,676, 95% |CI = [2,553, 2,798]) was significantly higher than the infected number when death sensitivity was at a low level (M = 2,121, 95% CI = [2,000, 2,242]), p < .001. The days of epidemic (M = 457, 95% CI = [454, 461]) and death number (M = 34, 95% CI = [32, 37]) were also higher when death sensitivity was 400 compared to the days (M = 431, 95% CI = [427, 435]) and deaths (M = 28, 95% CI = [25, 30]) when death sensitivity was 100, both p < .001. Therefore, hypothesis H2a was proven.
To obtain the data for the control speed of the epidemic, we fit the number of infected agents into a logistic curve in each trial. The turning point indicated the day or the time point where the growth speed of the infection number reached a maximum or inflection point in the logistic curve. The formula to fit the logistic curve was y = a/(1 + exp (−k*(x−xc))), where a represented the extreme value, which was the predicted infection number; k represented the growth speed of the infection number, where the larger the value was, the faster the epidemic was controlled; and xc represented the turning point. In reality, the logistic curve was normally not symmetrical before (stage 1) and after the turning point (stage 2); thus, the control speeds were different. Therefore, we also fitted the data in stage 1 and stage 2 into separate logistic curves to obtain separate control speeds, that is, k values (k1 and k2). Control speed before the turning point (stage 1), after the turning point (stage 2), and the control speed across the whole process were all treated as dependent variables.
K–S tests showed that the data could be considered as normal distribution, all p > .05. We conducted independent sample t-tests to compare these indicators. The results showed that there was no significant difference in the overall control speed between the two levels of death sensitivity (Klow = 0.0176, 95% CI = [0.0171, 0.018]; Khigh = 0.017, 95% CI = [0.0166, 0.0174]), t = 1.96, p = .051. However, control speed in stage 1 was significantly higher when death sensitivity was low (K1low = 0.0214, 95% CI = [0.0205, 0.0222], t = 2.54, p = .012; K1high = 0.0199, 95% CI = [0.0191, 0.0207]), and control in stage 2 was significantly higher when death sensitivity was high (K2low = 0.0182, 95% CI = [0.0177, 0.0187]; K2high = 0.0199, 95% CI = [0.0194, 0.0205]), t = −4.42, p < .001. Hypothesis H2b was partially confirmed.
As could be seen from Figure 3, there existed some outliers in the boxplot. These outliers existed because the simulation process was dynamic and stochastic, any minor difference in one step could lead to huge variances in following steps. Especially when DS was higher, the variation of fear of death was higher according to the calculation formula of death fear. Large variation in death fear could lead to larger variation in the final infected cases. We did not delete those outliers, because they could be the reasonable results due to the dynamic and stochastic nature of the simulation process. But we have also examined the results using values removing the outliers shown in Figure 3, and conclusions stayed the same. The results after removing outliers were displayed in Supplementary Material.

(a) The severity of the epidemic under different levels of death sensitivity; (b) the control speeds in the epidemic under different levels of death sensitivity.
To visually display the unfairness in societal resource allocation throughout the whole process, we simulated 10 trials under each of the two levels of death sensitivity, with each trial recording the resource distributions in society at the end of the first quartile (i.e., 25th percentile), the second quartile (50th percentile), the third quartile (75th percentile), and the turning point of the total epidemic process. Then, we averaged the results across 10 trials to obtain an averaged distribution of resources in society under low and high levels of death fear. As shown in Figure 4, at each stage of the epidemic, more agents acquired maximum resources when death sensitivity was high, but the lower bound of cumulative resources was also lower. The advantaged accumulated resources faster, but the disadvantaged were less likely to accumulate enough resources. This relative deprivation of the disadvantaged might be the reason why the control speed was slower in stage 1 under higher death sensitivity. When the advantaged gained enough resources, they exited the resource allocation process, leaving more resources to be more rapidly allocated to those with average and low levels of resources. This could be the reason why, in stage 2, the control speed was higher under the higher death sensitivity condition than under the lower death sensitivity condition.

The resource distribution at the 25th, 50th, and 75th percentiles as well as the turning point of the epidemic process; the advantaged were the agents with an initial resource over 37 (1 SD above the mean), and the disadvantaged were the agents with an initial resource below 23 (1 SD below the mean).
Discussion
Overall, the present study revealed the influence of the COVID-19 mortality salience effect on the process of resource allocation and how this further influenced the severity and control speed of the prevailing epidemic.
Influence of mortality salience on tolerance of unfairness in resource allocation
Study 1 used an experiment to show how activating COVID-19 mortality salience could influence the participants’ mindset toward resource allocation and found that responders in an ultimatum game under the COVID-19 mortality salience context would lower their threshold of minimum acceptance compared to the control condition and aging mortality salience condition. This influence was mediated by the perceived fairness of the unfair offers. The current finding of increased tolerance of unfairness seemed out of alignment with some of the previous studies showing that people tended to place more emphasis on fairness and justice when reminded of death (e.g., Wang et al., 2021). However, this finding is not necessarily contradictory. Terror management theory posits that people take action to reduce death anxiety in the context of mortality salience. Pursuing materialistic things is an effective way of reducing personal insecurity and anxiety (Chang & Arkin, 2002; Christopher et al., 2006). Many studies have discovered that people rely more on material things in a context of enhanced mortality salience, such as consuming more food and drink (Ferraro et al., 2005) and increasing pro-materialistic consumption choices (Zein et al., 2020). Moreover, a recent study found that people had lower delay discounting in the context of COVID-19 (Sonmez, 2021), meaning they preferred to have money now rather than wait for a higher value at a later time. This suggested that mortality salience would bring about a tendency toward instant gratification in a materialistic way, the extent of which might be more intense than the tendency to insist on fair norms. Accepting unfair offers could provide them with instant rewards, while rejection meant gaining nothing. Thus, higher acceptance of unfair offers under mortality salience was within interpretation.
The importance of specifying manners of death in mortality salience studies
The results of Study 1 showed that although COVID-19 mortality salience lowered people's acceptance threshold in an ultimatum game, mortality due to aging did not. Thus, we suggested that paying attention to or differentiating between the manners of death when considering the mortality salience effect was vitally necessary. A past study and the present study both showed that different death scenarios could have different influences on the following mindsets and behavior (Wang & Wang, 2012). The traditional mortality salience effect in past studies seems to resemble the mortality salience effect caused by unnatural deaths, such as traffic accidents (Wang & Wang, 2012) and COVID-19 (the current study), while natural death did not show a difference from the control condition and thus did not exert a mortality salience effect. There was a phenomenon in related research that, despite over 30 years of work (Pyszczynski et al., 2015), the mortality salience effect did not always appear in past studies and was constantly questioned as unstable (e.g., Klein et al., 2022; Sætrevik & Sjåstad, 2022). Combined with the present results, it would be plausible to assume that this could be due to failing to provide information on the manner of death or scenarios in the past, and we assume that specifying the manner of death and using scenarios including unpredictable, unnatural deaths might be able to enhance the possibility of observing the mortality salience effect.
Influence of tolerance of unfairness on the severity and control speed of COVID-19
Study 2 used the ABM method to simulate and compare how tolerance of unfairness changed in a society as a consequence of fear of death in the epidemic and how this tolerance would influence epidemic development through resource allocation. A higher tolerance of unfairness in society, brought about by higher fear of death, would render society resource allocation towards increased unfairness, which ultimately resulted in a higher severity and slower control of infections during the first stage of the epidemic.
The resulting higher severity of the epidemic from increased tolerance of unfairness suggested that the unfair distribution of social resources would deteriorate mitigation measures to halt the epidemic in number of infections, number of deaths, and duration. The effects of the tolerance of unfairness on control speed displayed different patterns in the two stages of the pandemic. In the early, first stage, lower tolerance of unfairness produced by fear of death led to faster control of the spread. However, in the second stage, higher tolerance of unfairness produced by fear of death terminated the epidemic faster. We suggest that, in the first stage, resources were often precious and insufficient for everyone, and a more equal allocation could help the epidemic spread reach its peak faster. If resources were distributed in an increasingly unequal way, those who were already deprived to begin with would be targeted for lower distributions, which made it harder for them to accumulate enough resources to protect themselves. With fewer resources, the risks of getting infected among disadvantaged classes stayed high and decreased at a slower rate, which was a barrier that made it slower for the rate of spread in society to reach its peak. Advantaged people were faster in accumulating enough resources to defend themselves against the epidemic if the distribution was more inclined to benefit them. Therefore, in the second stage, more upper-class agents accumulated enough resources to leave the process of sharing resources, which meant that there were more resources left to be allocated to the disadvantaged. Thus, in the later period, the pandemic was terminated faster with highly unequal distribution.
Although control of the spread did not differ in overall speed, the costs induced by an increased acceptance of unequal distributions was larger as distributions were more unequal. The disadvantaged with few initial resources remained at high risk, making the number of infections and deaths higher. Taking severity and control of the spread into consideration together, interventions to restore the normative tolerance of unfairness or constrain unfair allocations in society with high levels of fear of death are necessary to help the disadvantaged, alleviate the pandemic severity, and better control the spread.
Notably, the logic and aim of the current evolutionary model was to examine how tolerance of unfairness, caused by mortality salience, would influence the dynamic epidemic process. The current model did not involve other influences or effects produced by mortality salience. While there must have been other routes produced by different mortality conditions that could also influence the epidemic, for example, taking more actions to protect oneself (e.g., washing hands) or conducting fewer social interactions with others, their influences on epidemics are not examined in the current model. Therefore, the current results should be interpreted cautiously, in that differences in epidemic outcomes found in this study were caused solely through different levels of tolerance of unfairness due to different levels of mortality salience. The present study could serve as a preliminary study specifically examining how mortality salience influences the epidemic process through the tolerance of unfairness, and effects other than the tolerance of unfairness produced by mortality salience should be explored in future studies.
Highlights and future directions
The first highlight of the present study was to determine the reciprocal influences of epidemic severity and tolerance of unfairness in a pandemic. COVID-19 mortality salience could enhance people's tolerance of unfairness by lowering their acceptance threshold in an ultimatum game, while the increased tolerance of unfairness might influence resource allocation, leading to more unfair allocations in society and inducing higher severity and slower control of the spread in the first stage of the epidemic.
The second highlight was that the present study discriminated between different manners of death in mortality salience activation. Past studies mostly obeyed the traditional paradigm and ignored death-related information. Through comparison, the present finding again proved that discrimination was necessary and that the mortality salience effect appeared when using COVID-19, an abrupt, unnatural death, as a context, while natural deaths, such as those due to aging, did not show a difference from the control condition. Therefore, to raise the effect of mortality salience in future research, it is recommended to choose to prime participants with a context of unnatural death.
For future directions, the results of the present study could be validated in real dynamic interactions of ultimatum games to raise the ecological validity of the study. Additionally, the psychological mechanisms of the mortality salience effect on the tolerance of unfairness should be explored more elaborately, whether it be through instant gratification, fatalism, numbness to unfairness, the desire to benefit, and so on. More hypotheses and explanations could be examined. Moreover, more studies should be carried out to explore the effects on epidemic development other than unfairness tolerance, which would be brought about by mortality salience.
Supplemental Material
sj-docx-1-pac-10.1177_18344909231165188 - Supplemental material for Exploration of tolerance of unfairness under COVID-19 mortality salience and its effect on epidemic development
Supplemental material, sj-docx-1-pac-10.1177_18344909231165188 for Exploration of tolerance of unfairness under COVID-19 mortality salience and its effect on epidemic development by Lin Peng and Siyang Luo in Journal of Pacific Rim Psychology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Natural Science Foundation of China (32071081) (S. L.); the Guangdong Basic and Applied Basic Research Foundation (Project 2020A1515010975) (S. L.); and the Humanities and Social Science Foundation of Ministry of Education of China (Project 20YJC190016) (L. P.).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.