
Abstract
Unrealistic Optimism in the context of COVID-19 is described as the tendency to perceive peers as being more at risk of infection. To date, however, no research has proposed more specific comparisons. The present article not only replicates the most recent body of literature showing that people perceive themselves as less prone to COVID-19 infection than their peers, but fills the aforementioned gap by providing additional and more specific comparisons between those vaccinated and unvaccinated against COVID-19. Such comparisons may be crucial to curb the possibility of resurgence of COVID-19 by assessing how unvaccinated individuals perceive the probability of being infected by coronavirus. Some 622 Prolific—(un)vaccinated against COVID-19—users participated in an online quasi-experiment. Participants estimated the risk of COVID-19 infection for themselves, their peers or the average (un)vaccinated peer, which is a new addition to the literature. Results showed that there was an unrealistic optimism effect. Participants estimated their risk for infection as lower in comparison to others. Surprisingly, results showed that for unvaccinated people, vaccines seem to be an effective tool to reduce the risk of infection, but not for themselves.
Introduction
In December 2019 COVID-19 emerged, and the question arises, why are we not seeing the end of this pandemic? In this article we claim that this global crisis may have its roots not only in medical science but also in psychology, namely via the Unrealistic Optimism (UO) bias.
Unrealistic Optimism and Pessimism
Decades of studies have demonstrated the robustness of UO. It is described as a situation in which “people believe that negative events are less likely to happen to them than to others, and they believe that positive events are more likely to happen to them than to others” (Weinstein, 1980, p. 807). On the one hand, participants believe that—in comparison to their peers—they will receive better grades on exams (Lewine & Sommers, 2016), and a higher salary after graduation (Shepperd et al., 1996). On the other hand, people believe that negative events like addiction (Nezlek & Zebrowski, 2001), divorce (Lin & Raghubir, 2005), or road accidents (Rutter et al., 1998) will affect others. Such a notion may be fully reasonable while a specific person experiences good fortune: live a healthy and secure life. This notion, however, becomes unrealistic when the vast majority of people present such an illusion.
UO is an efficient tool in dealing with threats (e.g., Shepperd et al., 1996) but it can influence one's health: unrealistically optimistic women increased their risk of breast cancer by not undergoing mammographic screening as often as unbiased women (McCaul et al., 1996). Dillard et al. (2006) proved that unrealistically optimistic smokers were not only less eager to quit smoking, but also underrated the probability of getting lung cancer. People who were unrealistically optimistic about their alcohol consumption experienced more alcohol-related problems (Dillard et al., 2009). Hanoch et al. (2019) demonstrated that patients underestimated the risk and overestimated chances for successful treatment leading to unnecessary, harmful, and counterproductive interventions.
Unrealistic Optimism and the COVID-19 pandemic
In the first months of the worldwide COVID-19 pandemic UO was found to influence risk estimations of COVID-19 infection in many countries proving the robustness of this effect: France, Italy, Switzerland and the United Kingdom (McColl et al., 2021; Asimakopoulou et al., 2020), United States of America (Salvador Casara et al., in press), Belgium and the Netherlands (Hoorens et al., 2022), Poland (Dolinski et al., 2020), Kazakhstan and Iran (Kulesza et al., 2021), and Italy and România (Druică et al., 2020). Citizens estimated that their peers were at greater risk of coronavirus infection than themselves, which unveils the “unrealistic” component of this claim.
Some studies proved the robustness of the UO bias in a different way: its persistence over time. It was measured in terms of days, months, and even a year. The possible day-to-day changes were taken into consideration by Dolinski and colleagues (2020). In this study, UO was measured three times: before the announcement of the first case of coronavirus in the country of measurement, immediately after the first lockdown announcement when the first cases were reported making the threat real, and a few days later when the epidemic had largely developed. UO was mainly observed in all three measures, indicating its persistence/durability over time. The next time perspective was proposed by Kulesza and colleagues (2021). In this study, UO toward the risk of COVID-19 infection was measured for a month in various countries. Lastly, UO bias was shown to be present in the course of an entire year among 120 participants (Izydorczak et al., 2022).
The aforementioned review shows that UO bias is robust in the context of the COVID-19 pandemic. Its presence and time persistence has been confirmed in different countries and continents for days, months, and even a year.
The present study
In all previous studies participants compared themselves to their peers. In this article we asked (un)vaccinated participants to compare themselves with (un)vaccinated peers and we expected the following: first, since the existing body of literature on UO delivers a large amount of data showing how widespread this bias is (people claim to be less threatened in comparison to others; e.g., Shepperd et al., 2015 also on the grounds of health; and Nezlek & Zebrowski, 2001) it is reasonable to expect the presence of UO in the present study: (a) vaccinated participants will estimate their own chances of COVID-19 infection as lower compared to other vaccinated participants, (b) unvaccinated participants will estimate their own chances of COVID-19 infection as lower compared to other unvaccinated participants.
Second, the decision to vaccinate represents an intentional decision, in which side effects like fever, high temperature, and aches and pains due to vaccine administration are taken into consideration. In this context, we assume that participants’ intention to vaccinate was based on the assumption that vaccination lowers the chances of COVID-19 infection. On this basis, it is reasonable to presume that vaccinated participants would expect lower chances of COVID-19 infection in comparison to an average Prolific user whose vaccination status is not stated as well as in comparison to an average unvaccinated Prolific user.
Third, predictions for comparisons made by unvaccinated participants (to average Prolific users, and (un)vaccinated users) are much harder to make. It is reasonable to expect that unvaccinated participants/“others” are more exposed to COVID-19 infection. We expect, however, that when unvaccinated participants compare themselves to an average peer, they will perceive themselves as less at risk, meaning that UO would be present. Since the “average Prolific user” is an abstract category of comparison, it is unknown if this person of reference is vaccinated or not. Due to this, an unvaccinated participant may expect that s/he is less threatened by the COVID-19 infection.
Comparisons between unvaccinated participants and vaccinated peers would be particularly interesting. Objectively, unvaccinated participants are more threatened. A question arises: would they present UO? If yes, UO would be unexpectedly delusional. Since this study is the first of its nature, we cannot provide a direct link to the existing body of literature and pose a more general lack of causality.
Addressing these issues is important from a more general—this special issue—point of view. It is interesting from the point of view of the resurgence of COVID-19 among the unvaccinated. In cases when unvaccinated individuals perceive themselves as less or even equally threatened by COVID-19 in comparison to the vaccinated, it is possible that the presence of UO among this group's members would be an interesting factor explaining the involvement of health-oriented behaviors like mask wearing, maintaining social distance, hand-washing, and so on.
Methods
Participants
All samples were collected in November 2021 through Prolific, in exchange for £11.50 per hour. In all, 660 participants from different nationalities aged 18–78 (324 women, 331 men, five non-binary: Mage = 27.2, SDage = 8.32) responded to the invitation and 38 participants (23 women, 15 men: Mage = 29.9, SDage = 11.32, ages 18 to 63) were excluded due to at least one missing answer to our questions, which we considered as a lack of attention. The final sample consisted of 622 participants (301 women, 316 men, and five non-binary), aged 18–78 years (Mage = 27.08, SDage = 8.1) from which 328 participants (158 women, 167 men, and three non-binary), aged 18–78 years (Mage = 26.45, SDage = 7.65) were vaccinated, and 294 participants (143 women, 149 men, and two non-binary), aged 18–65 years (Mage = 27.78, SDage = 8.53) were unvaccinated.
Procedure
In an online quasi-experiment participants who were vaccinated with at least one dose of any kind of the COVID-19 vaccine (N = 328) and unvaccinated against COVID-19 (N = 294) from an international sample estimated the risk of COVID-19 infection for themselves, their peers, and the average ([un]vaccinated) Prolific user by answering four questions:
The respondents rated their answers on an 11-point scale (1 = Absolutely impossible; 11 = Quite certain).
Results
Protocols from the performed power analyses, along with databases and reports, are accessible at the Open Science Framework (OSF; https://osf.io/3vhdq/).
A preliminary statistical analysis demonstrated that the gender distribution between groups (vaccinated vs. unvaccinated) did not differ: χ2(1, N = 617) = 0.01, p = .929, V = .004. Additionally, the distribution did not differ when participant age (using two cutpoints width 33.33%) was taken into consideration; first category (age 18–22), p = .792, V = .02; second category (age 23–28), p = .534, V = .04; third category (age 29 + ), p = .487, V = .05. See Table 1 for more details.
Descriptive statistics of all study variables.
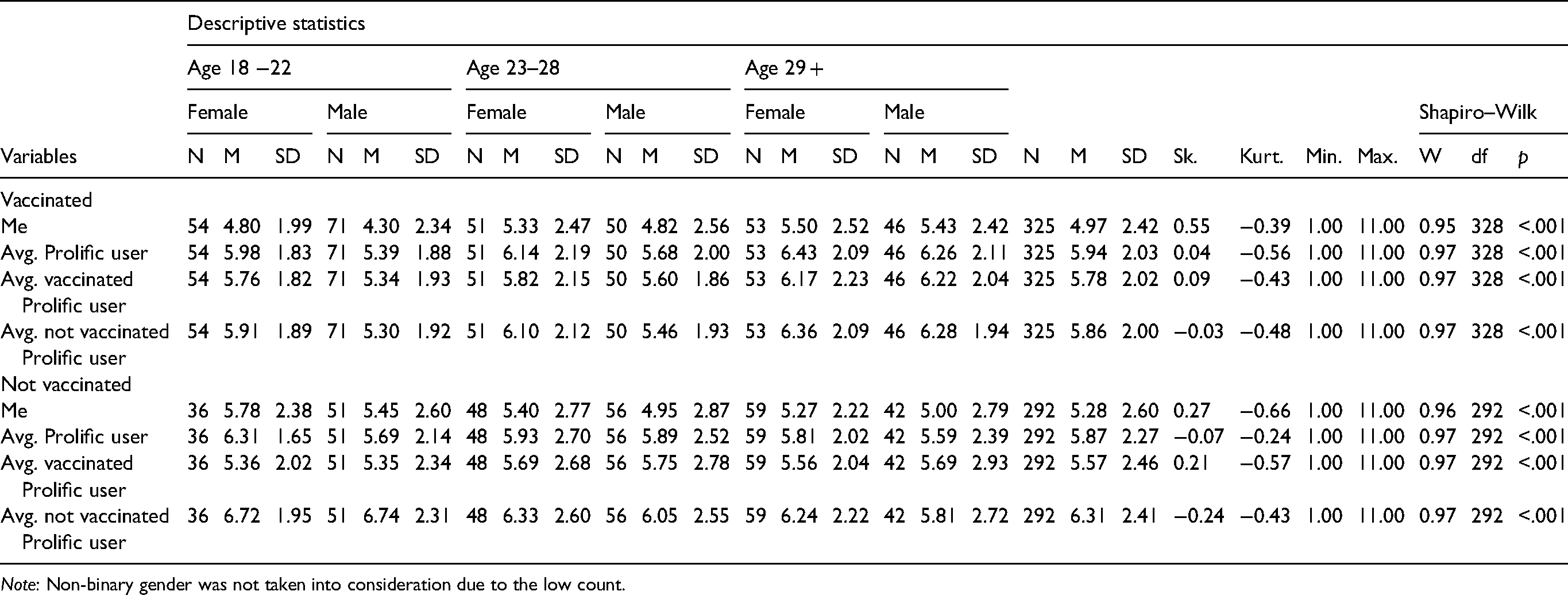
Note: Non-binary gender was not taken into consideration due to the low count.
A 2 × 4 mixed-design ANOVA was run with one between-subject factor—experimental condition (2: vaccinated, not vaccinated)—and one within-subject factor—social comparisons (4: COVID-infection risk assessment for “me,” “average Prolific user,” “average vaccinated Prolific user,” and “average not vaccinated Prolific user”).
Gender was also included in the model as a covariate (non-binary gender was not taken into consideration due to the low count), but the main effect of gender was not significant: F(1, 614) = 3.59, p = .058, ηp² = .01. Therefore, in subsequent analyses, gender was not taken into consideration.
An ANOVA with Huynh–Feldt correction (Sphericity test: p < .001; ε = .83) revealed a significant main effect of social comparisons, F(2.48, 1537.57) = 59.73, p < .001, ηp² = .09 (post-hoc test power: 1 – β = 1.). A post-hoc analysis with Bonferroni correction revealed that participants exhibited UO bias as they perceived themselves (M = 5.11, SD = 2.51) at a lower risk of contracting the COVID-19 infection than the average Prolific user (M = 5.91, SD = 2.14; t = −10.24, pbonf < .001; Cohen's d = − 0.34, 95% CI [ − 0.44, − 0.25]). All other comparisons turned out to be statistically significant (ts < 3.03; ps < .015), except for comparisons between the estimation for the average Prolific user and average unvaccinated Prolific user (pbonf = .118).
The main effect of the experimental condition was not significant, F(1, 620) = 0.58, p = .445, ηp² = .001 (post-hoc test power: 1 – β = .49).
The interaction effect of the experimental condition and social comparisons was significant, F(2.48, 1537.57) = 8.2, p < .001, ηp² = .01 (post-hoc test power: 1 – β = .99); thus, we performed a simple main effect analysis with a Bonferroni correction for all 28 comparisons. Both vaccinated and unvaccinated participants present UO while comparing themselves with a peer, which replicates the existing body of literature on COVID-19 and UO. Vaccinated participants perceived that they (M = 4.97, SD = 2.41) were at a lower risk of COVID-19 infection than the average Prolific user (M = 5.94, SD = 2.02; t = −9.22, pbonf < .001; Cohen's d = − 0.42, 95% CI [ − 0.57, − 0.28]), and unvaccinated participants also perceived that they (M = 5.28, SD = 2.6) were at a lower risk of COVID-19 infection than the average Prolific user (M = 5.87, SD = 2.27; t = −5.38, pbonf < .001; Cohen's d = − 0.26, 95% CI [ − 0.42, − 0.11]). Both [(un)vaccinated] groups, while comparing themselves with their in-group, still perceived themselves as less likely to be infected.
Results for the unvaccinated participants show that this group perceives vaccines as an effective tool against infection. They perceived that the average vaccinated Prolific user (M = 5.57, SD = 2.46) is less at risk than the average unvaccinated Prolific user (M = 6.31, SD = 2.41; t = −6.67, pbonf < .001; Cohen's d = − 0.32, 95% CI [ − 0.48, − 0.17]). In the same vein, unvaccinated participants do not perceive vaccines as a useful tool for themselves. They perceive that they are equally as likely to be infected as an average vaccinated Prolific user (pbonf = .233).
Lastly, results for vaccinated participants show that these participants perceived the average vaccinated Prolific user at the same risk as the average unvaccinated Prolific user (pbonf = .999). Sequentially, vaccinated participants perceived that they are at lesser risk than the average vaccinated Prolific user (M = 5.77, SD = 2.02; t = −7.71, pbonf < .001; Cohen's d = − 0.35, 95% CI [ − 0.5, − 0.21]). Data visualization can be found in Figure 1.

Est. COVID-19 Risk of Infection as a Function of Vaccinated and Unvaccinated Participants.
Discussion
This research brings new knowledge to the body of literature on social and health psychology as well as fresh understanding about this pandemic.
First, our results demonstrate the robustness of the UO: that not only do vaccinated people believe they are less at risk than an average vaccinated peer and an average unvaccinated peer, but also unvaccinated participants believe they are less at risk than their unvaccinated peers. In other words, comparisons for unvaccinated participants clearly show the presence of UO when making comparisons to unvaccinated peers.
Second, unvaccinated individuals believe that during a pandemic they are safe to the same extent as an average vaccinated person. It seems, therefore, that declining to use an obvious tool to fight the pandemic does not reduce UO.
Third, and of particular interest, the results indicate that unvaccinated participants think that vaccination leads to infection reduction. Additionally, the average vaccinated peer is—in the opinion of unvaccinated study participants—less exposed to danger stemming from COVID-19 than the average unvaccinated peer who is in fact an in-group member.
It is therefore clear that among the unvaccinated, as in previous studies, UO, as treated “classically,” appears when compared with unvaccinated peers. Paradoxically, this optimistic illusion seems to be even stronger when they compare themselves with an average vaccinated peer. What is even more surprising, on a general level they agree with medical authorities that vaccination helps to reduce the probability of being infected, but at the same time they believe that they are personally equally at risk as an average vaccinated peer.
The above demonstrated pattern of results is especially important because it contradicts the intuitive assumption that people who decide not to vaccinate are doing so on the basis of an opinion that vaccines are not effective tools to fight against infection. In the case of our study on the COVID-19 pandemic, unvaccinated participants claim that vaccines are effective in prevention. In our study, unvaccinated participants claim that the average unvaccinated Prolific user is more exposed to danger stemming from this virus in comparison to the average vaccinated user. On this basis, a very important question arises: why are unvaccinated participants not vaccinating themselves? The better-than-average effect (BTAE) may be a key factor in explaining this stunning result.
The BTAE is the tendency to perceive oneself (e.g., personality traits, skills) as better than the average person (e.g., Alicke, 1985). From this perspective it is possible that unvaccinated participants hold not only UO bias, but also the BTAE in terms of predictions about their own immune system. They may think that their health is more—in comparison to others—resistant to infections. If so, vaccination would not be needed, or at least would not be necessary. One should keep in mind that this reasoning is purely speculative and future studies should address this very issue.
One may easily notice that both vaccinated and unvaccinated participants demonstrated UO, but for both groups UO may mean and lead to different outcomes. In the case of vaccinated participants, UO has an illusory form. It is likely that they are optimistic because they took the vaccine. In the case of unvaccinated individuals, UO has a delusory form. They are optimistic despite the fact that they did not take a vaccine, or rather they did not take a vaccine because they may have believed they were invulnerable.
From a more general—theoretical—point of view, this study offers new knowledge. It is the first study on UO in which participants compared themselves to a more specific average in/out-group peer. Previously, comparisons were made with a general and unspecific “average peer,” and this has also been the case for research on UO during COVID-19. In this article we asked (un)vaccinated participants to compare themselves not only with an average peer but also with (un)vaccinated peers.
Recommendations
On the basis of this study some scalable health interventions are possible. First, for unvaccinated people, vaccines seem to be an effective tool to reduce the risk of infection, but not for themselves, showing a potential groundwork for encouraging them to vaccinate.
Second, it is possible that vaccines are a game changer in eradicating UO that could—in turn and in light of the literature described above—lead to more positive behaviors oriented toward health protection. Future research should address this issue.
Limitations
This study is not free from caveats. First, is this research applicable to any pandemic, or to any health danger, or even to any danger in general?
Second, another caveat is linked to the environment in which this study was run: online research and an internet-connected English-speaking population.
Third, according to the BTAE described above, it would also be interesting to assess the measurement of to which degree unvaccinated participants perceive their health, and—more importantly—immune system as better prepared against future infections.
Finally, we did not directly measure the attitude toward vaccination. In future studies it would be interesting to analyze the interaction between the directly measured attitude toward vaccination among vaccinated as well as unvaccinated participants and UO.
Conclusions
It seems that comparisons between unvaccinated and vaccinated peers form a more complex picture. In the light of our research, global communication boosting eagerness among skeptics to vaccinate should be shifted from “vaccines are good in the fight against COVID-19” to UO reduction: “you are vulnerable just like your peers.”
Footnotes
Data availability
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical committee statement
All experiments were reviewed and approved by the ethics committee of the SWPS University of Social Sciences and Humanities in Wroclaw, Poland (02/P/08/2020). Informed consent was obtained from all participants before enrollment in the experimental procedures and data collection.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by: The Polish National Agency for Academic Exchange (NAWA) within the Urgency Grants program granted to Wojciech Kulesza (number: PPN/GIN/2020/1/00063/U/00001).