
Abstract
This study investigated the impacts of risk perception of COVID-19 on anxiety and depression symptoms among hospital pharmacists in China. We conducted a cross-sectional study with hospital pharmacists during the COVID-19 pandemic in China. Some 4,219 hospital pharmacists completed an online survey including demographic questions, risk perception of COVID-19, General Anxiety Disorder-7, Patient Health Questionnaire-9, and Positive and Negative Affect Schedule. Multivariate regression and mediation analyses were conducted. The results indicated that 41.9% and 29.4% of hospital pharmacists experienced mild to severe levels of anxiety and depression symptoms, respectively. In older age, a higher level of risk perception of COVID-19, and negative affect experience were risk factors, whereas positive affect experience was a protective factor for anxiety and depression symptoms among pharmacists. Experience of positive and negative affect mediated the relationship between risk perception of COVID-19 and anxiety and depression among hospital pharmacists in China. Timely mental health services need to be provided for hospital pharmacists during the COVID-19 pandemic.
Introduction
The COVID-19 pandemic is the most severe public health crisis since the establishment of the World Health Organization. By April 20, 2022, the COVID-19 pandemic has led to more than 504 million infections and more than 6.21 million deaths worldwide (Johns Hopkins University, 2021). Similar to previous pandemics of infectious diseases, such as SARS (Maunder et al., 2003) and Ebola (Lötsch et al., 2017), the COVID-19 pandemic not only caused severe threat to people's physical health but also induced wide-ranging impacts on people's mental health (Adhanom Ghebreyesus, 2020; Lai et al., 2020; Qiu et al., 2020; Unützer et al., 2020; Zhang, 2022; Zhang et al., 2022). Compared with the general public, frontline healthcare workers have a relatively higher level of risk for infection due to their close involvement in the efforts to contain the COVID-19 pandemic (Nguyen et al., 2020). It has previously been observed that the prevalence of mental health symptoms among healthcare professionals is relatively high. For example, a survey of 1,563 medical staff using General Anxiety Disorder –7, Patient Health Questionnaire –9, and the Insomnia Severity Index found that the prevalence of anxiety, depression, and insomnia was as high as 44.7%, 50.7%, and 36.1%, respectively, among medical staff in Southern China during the early stage of the pandemic in China (Liu, S. et al., 2020). Similar levels of mental health symptoms (44.6%, 50.4%, and 34% for anxiety, depression, and insomnia, respectively) were reported among healthcare workers based on another survey conducted during the COVID-19 pandemic in China (Lai et al., 2020). These results highlighted the needs of timely mental health services to improve the mental health of frontline healthcare workers during the COVID-19 pandemic (Bo et al., 2021; Yang et al., 2021; Zhang et al., 2020 2022).
However, just as pharmacists are sometimes left off in the list of frontline healthcare workers, pharmacists’ mental health status during the pandemic is often overlooked (Elbeddini, Wen, et al., 2020). In fact, alongside intensive care unit (ICU) nurses, physicians, and respiratory therapists, many pharmacists belong to one of the groups that face the greatest Coronavirus risks both physically and mentally (Al-Quteimat & Amer, 2021; Elbeddini, Prabaharan, et al., 2020). This is because, in addition to their increased daily burden of ensuring drug supply, many of them actively engaged in frontline treatment work such as developing local treatment protocols and participating in patient rounds (Carico, 2020; Grabenstein, 2020; Li et al., 2020; Worthington & Tedder, 2020). For example, A recent study in France demonstrated that up to 35% of pharmacists experienced a high level of psychological disturbance during the lockdown period (Lange et al., 2020). However, this study was conducted among community pharmacists in France and mainly focus on perceived stress, burnout symptoms, and psychological disturbance. It's not clear how the COVID-19 pandemic influence hospital pharmacists’ mental health in China, which has a different medical system compared to France and other western countries. Although previous research raised awareness on the necessity to improve pharmacists’ mental health during the COVID-19 pandemic, there is a dearth of research on how hospital pharmacists’ risk perception of COVID-19 influenced their mental well-being during the pandemic.
One pathway through which risk perception influences people's mental health is their affective experience during the COVID-19 pandemic. For example, one study conducted during the peak period of the COVID-19 pandemic in China found that risk perception predicted people's experience of mental health distress and flourishing, and the effects were mediated by people's experience of positive and negative affect (Zhang, 2022). Similarly, another multinational study across 112 countries around the world also found that risk perception of COVID-19 significantly predicted people's experience of higher negative emotions, lower positive emotions, and worse mental health status during the pandemic (Han et al., 2021). Besides, the results revealed that the effect of risk perception on mental health was significantly mediated by people's experience of emotional distress (Han et al., 2021). This line of research highlighted the importance of understanding the underlying mechanisms that explain the impact of risk perception on people's mental health during pandemics of infectious diseases.
The current research filled this gap by investigating the relationship between risk perception of the COVID-19 pandemic and prevalence of anxiety and depression among hospital pharmacists during the peak period of the COVID-19 pandemic in China and explored the mediating effect of positive and negative affect experiences. In previous research, risk perception has been well documented as a predictor of people's responses and intentions to engage in preventative behaviors (Brug et al., 2004; Park et al., 2021; Smith, 2006; Vartti et al., 2009; Zhang et al., 2021). However, recent evidence from China suggests that it might also play a significant role in influencing people's mental health during pandemics (Ding et al., 2020; Han et al., 2021; Zhang, 2022). To better understand such influence, we explored a number of risk and protective factors of mental health symptoms among hospital pharmacists, including level of risk perception, affective experiences during the pandemic, and demographic variables. Among them, we had a particular interest in delineating the effects of positive and negative affect on pharmacists’ mental health during the pandemic. Based on previous research documenting the buffering effect of positive affect for psychological distress such as the broaden-and-build theory of positive emotions (Folkman & Moskowitz, 2000; Fredrickson et al., 2003; Huppert et al., 2004), we predicted that experiences of positive and negative affect would mediate the relationship between risk perception and anxiety, depression symptoms among hospital pharmacists. Specifically, experience of positive affect would be protective of pharmacists’ mental health, whereas experience of negative affect would be detrimental for pharmacists’ mental health during COVID-19. Therefore, we hypothesized that pharmacists experienced a higher level of positive affect during the pandemic would report a lower level of anxiety and depression during COVID-19, whereas those who experienced a higher level of negative affect would report a higher level of anxiety and depression during COVID-19.
Materials and methods
Study design and participants
We conducted a cross-sectional survey research study on February 14–15, 2020, during the peak period of the COVID-19 pandemic in China (the figures of newly confirmed cases, existing confirmed cases, and mortality reached the highest levels during this pandemic period; The State Council Information Office of the People’s Republic of China, 2020) through an online survey platform (www.wjx.com). The research team invited pharmacists working in hospitals within Mainland China to participate in the survey through social networks of pharmacists’ professional associations in China. Some 4,219 pharmacists completed the study voluntarily without compensation. Among them, 98 were excluded from further analyses based on selection criteria decided before data analyses: two of them reported extreme values for age, and the other 96 took less than 240 or more than 7,200 s to complete the study. Those who took too short or too long to complete the questionnaire are treated as “did not take the study seriously.” Therefore, 4,121 pharmacists were included in the final analyses. To assess the study's robustness, we repeated all analyses with the full dataset, and the results did not change significantly.
Measurements
Risk perception of COVID-19
We measured pharmacists’ risk perception of the COVID-19 pandemic with the following four items adapted from previous research on risk perception during the SARS pandemic (De Zwart et al., 2009): (1) “How severe do you think the COVID-19 pandemic is?” (1 = not severe at all, 5 = very severe); (2) “How do you perceive the health risk of COVID-19?”; (3) “How do you perceive your risk of being infected with COVID-19?”; (4) “How do you perceive your risk of infection compared to a normal Chinese with the same age and gender to you?” (1 = very low risk, 5 = very high risk). Cronbach's α for risk perception in the current study is .64.
Anxiety
Participants’ anxiety symptoms were measured using the General Anxiety Disorder 7-item (GAD–7) scale developed by Spitzer and colleagues as a valid measure of anxiety symptoms (Spitzer et al., 2006). Participants respond to the question “Over the past 2 weeks, how often have you been bothered by the following problems?” on a four-point scale (0 = Not at all, 1 = Several days, 2 = Over half the days, 3 = Nearly every day). Sample items include “Feeling nervous, anxious, or on edge,” “Not being able to stop or control worrying.” The scale was translated into Chinese and verified for its psychometric properties and usability in China by Zeng and colleagues (2013). Cronbach's α for GAD–7 in the current study is .91.
Depression
Participants’ depression symptoms were measured using the Patient Health Questionnaire (PHQ–9) developed by Kroenke and colleagues (2001, 2002) as a valid and sensitive measure of depressive symptoms. Participants responded to the question “Over the past 2 weeks, how often have you been bothered by any of the following problems?” on a four-point scale (0 = Not at all, 1 = Several days, 3 = More than half the days, 4 = Nearly every day). Sample items include “Little interest or pleasure in doing things,” “Feeling down, depressed or hopeless.” The questionnaire was translated into Chinese and verified for its psychometric properties and usability in China by Bian and colleagues (2009). Cronbach's α for PHQ–9 is .90 in the current study.
Positive and negative affect
Pharmacists also completed the Positive and Negative Affect Schedule (PANAS) developed by Watson and colleagues (1988). PANAS is a self-report measure composed of two mood scales, one measuring positive affect and the other measuring negative affect. The scale consists of 20 words (e.g., interested, distressed) describing positive and negative feelings. Participants indicated the extent to which they felt this way over the past one to two weeks on a five-point scale (1 = Very slightly or not at all, 2 = A little, 3 = Moderately, 4 = Quite a bit, 5 = Extremely). The scale was translated into Chinese and verified for its psychometric properties by Qiu and colleagues (2008). Cronbach's α for positive affect and negative affect is .92 and .90, respectively, in the current study.
Finally, we asked pharmacists whether they need psychological support and if they replied “yes,” what kinds of psychological support they would like to receive, including support from family and friends, education on maintaining mental health, mental health screening, psychological counseling through hotlines, psychological therapy, and support and interaction with neighbors. They also completed questions on demographic variables, including age, gender, marital status, whether they have child(ren) or not. The study received ethic clearance from the authors’ hosted institution.
Statistical analyses
Data were analyzed using SPSS 24.0 and AMOS 23.0. Given the cross-sectional nature of the current survey, a Harman univariate test was conducted for the common method bias. And we compared group differences between key variables using independent sample t-tests and used correlational analyses to explore the relationships between key variables. Then, we used multivariate regression analyses to investigate the predictors of anxiety and depression symptoms among hospital pharmacists. Finally, we used the process macro developed by Preacher and Hayes (2008) for investigating the mediating effects of positive and negative affect. And we tested the two dependent variable (i.e., anxiety symptoms and depression symptoms) in one structural equation model (SEM) to compare their path coefficients. A value of p < 0.05 was considered statistically significant.
Results
Harman univariate test shows that the explanation rate of the total variance of the first common factor is 31.1%, which is less than the recommended threshold of 50%, so it can be considered that there is no serious common method bias (Podsakoff et al., 2003). Hospital pharmacists’ age ranges from 20 to 73 years (Mage = 35.96 years, SD = 8.25) in this study. Most of them are female (75.8%), married (76.4%), have at least one child (72.3%), and are well educated (96.4% have a bachelor's degree or above). Most pharmacists (77.8%) have working experience longer than ten years.
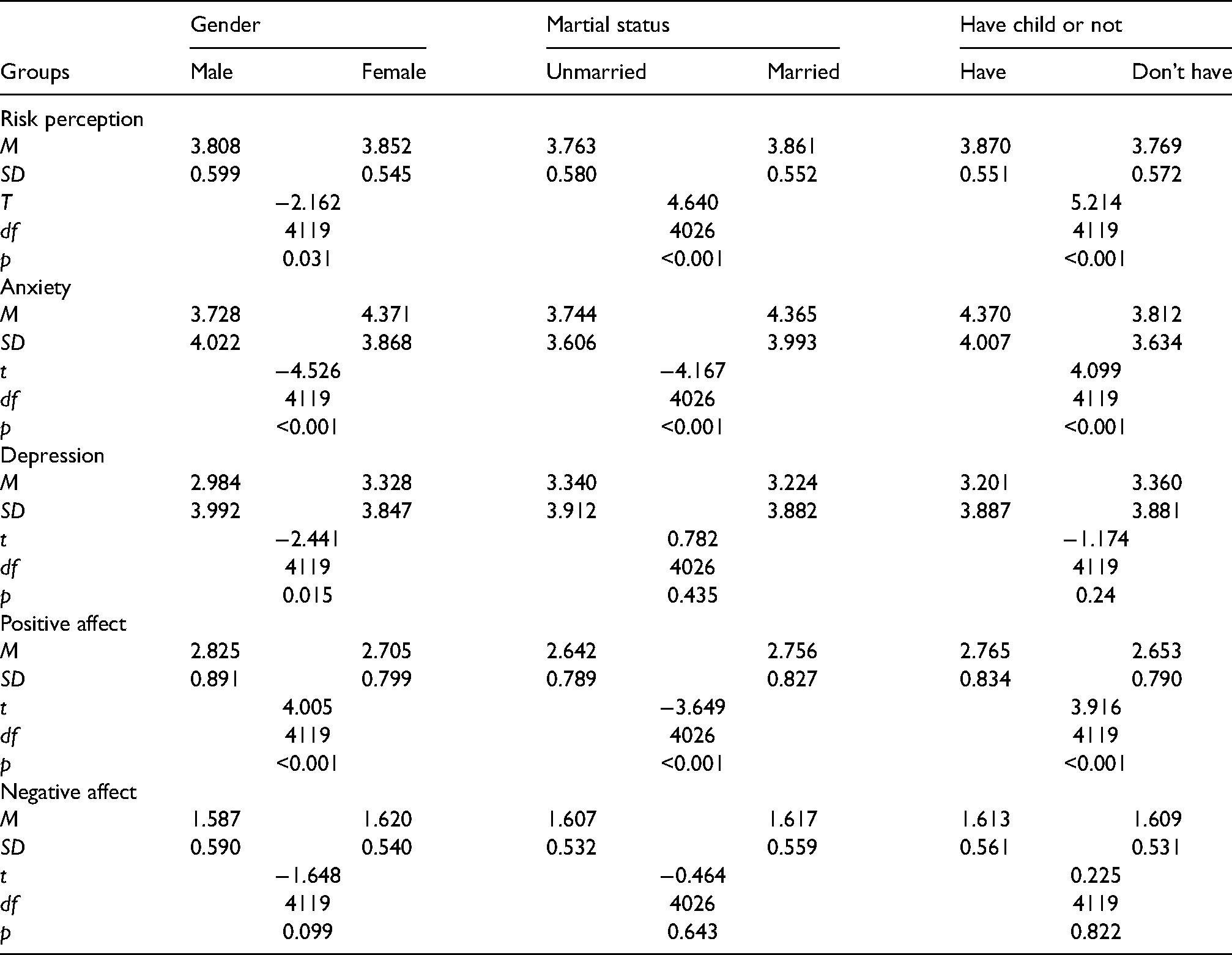
Group differences on key variables
Independent sample t-tests revealed that female pharmacists reported a higher level of risk perception, anxiety, and depression symptoms than male pharmacists. Female pharmacists also reported a lower level of positive affect than male pharmacists. Married pharmacists reported a higher level of risk perception and anxiety symptoms than unmarried pharmacists, but they also experienced a higher level of positive affect than unmarried pharmacists. Pharmacists who have child(ren) reported a higher level of risk perception and anxiety symptoms than those who do not have child(ren), and they also experienced a higher level of positive affect (see Table 1).
Group differences on key variables
Distribution of anxiety and depression symptoms among pharmacists
Based on the scoring guidelines of GAD–7 (Zeng et al., 2013), the proportion of pharmacists reported mild, moderate, and severe anxiety symptoms was 33% (n = 1361), 6.5% (n = 268), and 2.4% (n = 98), respectively. According to the scoring guidelines of PHQ–9 (Kroenke & Spitzer, 2002; Kroenke et al., 2001), the proportion of pharmacists who reported mild, moderate, moderately severe, and severe depression symptoms was 23.6% (n = 972), 4.3% (n = 179), 1.1% (n = 47), and 0.4% (n = 18), respectively. Therefore, 41.9% of pharmacists experienced mild, moderate to severe anxiety symptoms, and 29.4% of pharmacists experienced mild, moderate to severe depression symptoms. Besides, 25.0% of pharmacists (n = 1030) experienced both symptoms of anxiety and depression during the peak period of the COVID-19 pandemic in China. However, when asked about whether they needed psychological support, only 273 (6.6%) pharmacists responded that they did, including support from family and friends (n = 137, 3.3%), mental health education (n = 60, 1.5%), mental health screening (n = 34, 0.8%), psychological therapy (n = 29, 0.7%), online psychological counselling (n = 12, 0.3%), and support from neighbors (n = 1).
Correlations between key variables
Correlational analyses suggested that age was positively correlated with risk perception, anxiety symptoms, positive affect, and negatively correlated with depression symptoms and negative affect. Pharmacists’ self-reported level of risk perception was positively correlated with their experience of anxiety and depression symptoms. Their self-reported level of anxiety was positively correlated with their experience of depression symptoms and negative affect, but was negatively correlated with their experience of positive affect. Their self-reported level of depression symptoms was positively correlated with their experience of negative affect and negatively correlated with their experience of positive affect (see Table 2).
Correlations between key variables in the current study

Note. GAD–7 = General Anxiety Disorder 7-item scale, PHQ = Patient Health Questionnaire 9-item scale, M = Mean, SD = Standard deviation. *p < .05. ** p < .01.
Predictors of anxiety and depression symptoms among pharmacists
Next, we conducted a series of regression analyses to predict the severity of anxiety and depression symptoms among hospital pharmacists. A regression analysis with the severity of anxiety symptoms as the dependent variable revealed that gender, age, risk perception, and experience of positive and negative affect were significant predictors of the severity of anxiety symptoms among pharmacists. These results suggest that women, older age, a higher level of risk perception and experience of negative affect, and lower experience of positive affect are all risk factors of anxiety symptoms among hospital pharmacists during the COVID-19 pandemic (see Table 3).
Predictors of anxiety symptoms among pharmacists

Note. B = unstandardized regression coefficient, SE = Standard error, β = standardized regression coefficient, 95% CI = 95% Confidence interval. p < .001 for all the significant predictors of anxiety symptoms.
Similarly, a regression analysis with the severity of depression symptoms as the dependent variable revealed that age, risk perception, and experience of positive and negative affect are significant predictors of the severity of depression symptoms among pharmacists. These results suggest that older age, a higher level of risk perception and experience of negative affect, and lower experience of positive affect are risk factors of depression symptoms among hospital pharmacists during the COVID-19 pandemic (see Table 4).
Predictors of depression symptoms among pharmacists

Note. B = unstandardized regression coefficient, SE = Standard error, β = standardized regression coefficient, 95% CI = 95% Confidence interval. p < .05 for age as a significant predictor of depression symptoms, p < .001 for all other significant predictors of depression symptoms.
Positive and negative affect mediated the relationship between risk perception and anxiety, depression symptoms
To further investigate the role of experiencing positive and negative affect in the onset of anxiety and depression symptoms among hospital pharmacists during the COVID-19 pandemic, we conducted two mediational analyses using Preacher and Hayes’s (2008) indirect macro. First, a mediation analysis was conducted with risk perception as the independent variable, pharmacists’ anxiety symptoms as the dependent variable, and experience of positive and negative affect as the mediators, controlling for gender and age as the covariate. The indirect effect of risk perception on the severity of anxiety symptoms through the experience of positive and negative affect was significant (B = 1.168, p < .001). Bootstrapping analysis revealed that the 95% bias-corrected CI for positive affect [.0118, .0507] and negative affect [.7182, .9990] did not include zero. The Sobel tests confirmed the mediation effect by positive affect (Z = 3.05, p = .002) and negative affect (Z = 13.53, p < .001). Therefore, the experience of positive and negative affect significantly mediated the relationship between risk perception and severity of anxiety symptoms among hospital pharmacists during the COVID-19 pandemic (see Figure 1).

Mediational model of positive and negative affect on risk perception and severity of anxiety symptoms (GAD–7).
Second, another mediation analysis was conducted with risk perception as the independent variable, pharmacists’ depression symptoms as the dependent variable, and experience of positive and negative affect as the mediators, controlling for age as the covariate. The indirect effect of risk perception on the severity of depression symptoms through the experience of positive and negative affect was significant (B = .4485, p < .001). Bootstrapping analysis revealed that the 95% bias-corrected CI for positive affect [.0257, .1133] and negative affect [.7805, 1.0812] did not include zero. The Sobel tests confirmed the mediation effect by positive affect (Z = 3.34, p < .001) and negative affect (Z = 13.67, p < .001). Therefore, the experience of positive and negative affect significantly mediated the relationship between risk perception and the severity of depression symptoms among hospital pharmacists during the COVID-19 pandemic (see Figure 2).

Mediational model of positive and negative affect on risk perception and severity of depression symptoms (PHQ–9)
Third, a structural equation model was conducted by AMOS 23.0 with risk perception as the independent variable, both pharmacists’ anxiety and depression symptoms as the dependent variables, and experience of positive and negative affect as the mediators. The indirect effects of risk perception on the severity of anxiety and depression symptoms through the experience of positive and negative affect were still significant (B = 1.17, p < .001; B = .45, p < .001, respectively). This result corroborates the results that experience of positive and negative affect mediated the relationship between risk perception and severity of anxiety and depression symptoms among hospital pharmacists. Based on the regression coefficients, the results also indicated that mediation effect of positive and negative affect was stronger for the severity of depression symptoms than that of anxiety symptoms (Figure 3).

Structural equation model of positive and negative affect on risk perception and severity of anxiety symptoms (GAD–7) / severity of depression symptoms (PHQ–9) Note. Parameter estimates are standardized regression coefficients. ***p < .001.
Discussion
Through a large-scale study among hospital pharmacists during the peak period of the COVID-19 pandemic in China, we found that 41.9% of pharmacists reported experiences of anxiety symptoms, and 29.4% of them experienced depression symptoms. Among them, 8.9% experienced moderate to severe levels of anxiety symptoms, and 5.8% experienced moderate to severe levels of depression symptoms. The results coincide with recent research documenting risk perception as a risk factor of anxiety and PTSD symptoms among healthcare professionals fighting against COVID-19 (Yin et al., 2021) and anxiety among citizens in China (Liu, M. et al., 2020). Although the percentage of hospital pharmacists who experienced moderate and more severe anxiety and depression symptoms in China is lower than that reported in Singapore among nonmedical healthcare personnel (20.7% for anxiety and 10.3% for depression, respectively) (Dai et al., 2020) and the level of psychological disturbances among community pharmacists in France (Lange et al., 2020), it's comparable to the level of depression observed among COVID-19 survivors in South Korea (Oh et al., 2021). This relatively lower level of anxiety and depression symptoms could be because many pharmacists were not working in the severely affected areas of COVID-19, and their hosted hospitals were not designated hospitals for treatment of infected patients of COVID-19, which reduced their risk of infection. Nonetheless, the results should raise awareness among hospital pharmacists and administrators about pharmacists’ mental health during the COVID-19 pandemic. Given that China had 550,000 pharmacists in total, many of them were and still are working in hospitals during the coordinated efforts to contain the pandemic. They were very likely to experience an even higher level of anxiety and depression symptoms during the COVID-19 pandemic than that reported in this study. Therefore, hospital administrators should take measures to improve the mental health well-being of hospital pharmacists.
Another surprising finding is that only 6.6% of hospital pharmacists in this study thought that they needed psychological support during the pandemic, while more than two-fifths of hospital pharmacists experience some degree of anxiety and depression symptoms. Therefore, proactive measures should be taken to increase the accessibility of mental health services for pharmacists to improve their mental health during the pandemic (Elbeddini, Wen, et al., 2020).
Comparisons between different subgroups on anxiety and depression symptoms revealed that female pharmacists experienced a higher level of anxiety and depression symptoms than male pharmacists. This finding is in line with previous research on psychological distress among healthcare workers that females tend to perceive a higher level of infection risks than males (Dai et al., 2020). Married pharmacists and pharmacists who have child(ren) experienced a higher level of anxiety symptoms than unmarried pharmacists and pharmacists who did not have child(ren). This could be because pharmacists who are married and have child(ren) are more worried about the possibilities of infection among their family members, which is in line with Dai and colleagues’ (2020) research on the psychological impact of COVID-19 pandemic among healthcare workers in Wuhan. Male pharmacists, married pharmacists, and pharmacists who have child(ren) experienced a higher level of positive affect than female pharmacists, unmarried pharmacists, and pharmacists who do not have child(ren). This suggests that marriage and child-rearing could be protective factors in response to the stress induced by the COVID-19 pandemic. The protective effect of marriage is in line with decades of research on marriage's beneficial impact on subjective well-being (Diener et al., 1999). At first look, it seems conflicting that married pharmacists reported a higher level of anxiety and a higher level of positive affect during the pandemic. It could be that married pharmacists were more worried about their families’ risk of infection but also gained more from the experience of staying together and receiving social support from family members during the pandemic. The result that pharmacists who have child(ren) reported a higher level of positive affect is in line with the research finding that child-centrism enhanced parents’ well-being (Ashton-James et al., 2013). The enhanced social connections between parents and their children could buffer them from mental health distress during the COVID-19 pandemic (Tso et al., 2022).
Regression analyses revealed that gender, age, risk perception, and experience of positive and negative affect were significant predictors of anxiety symptoms among pharmacists. Age, risk perception, and experience of positive and negative affect were predictors of depression symptoms among pharmacists. These results suggested that older age, a higher level of risk perception, and higher experience of negative affect were risk factors of mental health among pharmacists. In contrast, higher experience of positive affect was a protective factor of mental health among pharmacists. Mediational analyses demonstrated that experience of positive and negative affect were significant mediators of the relationship between risk perception and experience of anxiety and depression symptoms among pharmacists during the COVID-19 pandemic. This is in line with research demonstrating the buffering effect of positive emotions after experiencing traumatic events (Folkman & Moskowitz, 2000; Fredrickson et al., 2003; Huppert et al., 2004). It is probably because that experience of positive affect enhances people's level of social connectedness, which in turn helps them cope with stress and improve psychological functioning during difficult times (Mauss et al., 2011). Together these findings contribute to improving mental health services. They suggest mental health services reducing experiences of negative affect, increasing experiences of positive affect and enhancing social connectedness could be effective strategies to relieve the profound mental health impacts of the COVID-19 pandemic among pharmacists, other healthcare workers, infected and suspected patients, and the general public.
The current research has several limitations. First, the study is cross-sectional, which limited the generalization of the results during other stages of the COVID-19 pandemic. Future research using a longitudinal research design will enrich our understanding of the dynamic relationships between risk factors and mental health symptoms among pharmacists. Second, with the current design, the results are correlational rather than causal. Although mediational analyses help us understand the underlying mechanisms of the effect of risk perception on mental health symptoms (e.g., anxiety, depression), future intervention research is needed to provide causal evidence on the buffering effect of positive affect on mental health during pandemics. Future research exploring both mediation and moderation effects will enrich our understanding of the mechanisms through which risk perception influences people's mental health. Third, the sample in the current study consists of pharmacists working in hospitals during the pandemic in China. The results may not be generalized to other professional groups or community pharmacists in other countries. Given that pharmacists are playing important supportive roles in the coordinated efforts to contain the COVID-19 pandemic and many pharmacists participated in this study were only indirectly exposed to the SARS CoV-2 virus, the results likely underestimate the mental health impacts of the pandemic on pharmacists who are directly involved in containing the pandemic. Future research using more representative samples will help us understand the enormous mental health impact of COVID-19 among different groups of people and provide empirical evidence for delivering tailored and precision mental health services to speed recovery and enhance resiliency in response to emergent public health crises like COVID-19.
The current research has several implications for all stakeholders, including governments, health authorities, administrators, and healthcare professionals to be prepared for coping with the mounting level of stress they would likely experience during emergent public health crises such as COVID-19. First, given that there is a large number of healthcare professionals in China and pandemics of infectious disease such as COVID-19 are likely to induce widespread anxiety and depression among them, health administrators and governments should take proactive measures in improving the mental health of healthcare professionals. Second, governments should take measures to increase the accessibility and utilization of mental health services for healthcare professionals, especially during pandemics of infectious diseases. Establishment of telepsychiatry and telepsychology services networks would be a valuable option to increase preparedness for helping healthcare professionals to cope with stress they would experience during the COVID-19 pandemic (Zhang et al., 2022). Third, given that social connections and social support can buffer people from enormous stress (Labrague, 2021; Tso et al., 2022), governments and hospital administrators need to take measures to help people to maintain their social connections and enhance their social support network to cope with the mental health impact of public health crises like COVID-19. Fourth, as increasing experience of positive affect could be one effective strategy to empower healthcare professionals to expand their mental resources in face of adversities (Fredrickson, 2013), governments and hospital administrators can implement scalable and effective interventions to enhance experiences of positive affect during public health crises (Wang et al., 2021; Waters et al., 2021; Zhang et al., 2022).
In conclusion, this study suggested that the COVID-19 pandemic induced moderate levels of anxiety and depression symptoms among hospital pharmacists in China. Gender, older age, a higher level of risk perception, and experience of negative affect were risk factors whereas marriage, child-rearing, and a higher level of experience of positive affect were protective factors of anxiety and depression among hospital pharmacists in China. Future research using large-scale mental health screening and longitudinal design will enrich our understanding of the dynamic predictors of mental health symptoms among pharmacists and provide insights for tailoring mental health services to mitigate the pandemic's mental health impacts among healthcare professionals.
Footnotes
Author contributions
N. Z. designed the research, analyzed the data, and wrote the manuscript. D. S. H., H. Y. Y., X. H., and L. R. W. helped with data collection and provided comments on revising the manuscript. M. X. G. and A. R. W. helped with manuscript revising and editing. All the authors agree with the submission of this manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Fundamental Research Funds for the Central Universities, the Hundred Talents Program Research Initiation Fund from Zhejiang University, Leading Innovative and Entrepreneur Team Introduction Program of Zhejiang (2019R01007), and the Key Laboratory of Intelligent Preventive Medicine of Zhejiang Province (2020E10004). The funding organizations were not involved in design, analyses, and writing of the research, nor in the decision to submit the article for publication.