
Abstract
Sleep quality and perceived social support (PSS) are acknowledged to play indispensable roles in enhancing the adaptation of later life and improving the health condition and well-being of older adults. Both have received widespread attention from researchers. Some researchers have begun focusing on physical factors or health-related behaviors, such as sleep, that have significant effects on PSS. Good sleep quality has been widely established to be significantly associated with a high level of PSS. However, research on the temporal effects of sleep quality on PSS is limited, and the potential health mechanisms of the relationship between sleep quality and PSS in older adults are mixed. This study aims to investigate the temporal relationship between sleep quality and PSS, including the mediating role of depressed mood in the relationship between sleep quality and PSS in older adults. A total of 281 older adults completed the self-reported questionnaires assessing sleep quality, PSS, and depressed mood at three time-points: at intake, a 6-month follow-up, and a 12-month follow-up. Cross-lagged panel analysis using structural equation modeling indicated that sleep quality at Times 1 and 2 positively predicated PSS at Times 2 and 3, respectively. In addition, the longitudinal mediation analysis showed that depressed mood mediated the effect of sleep quality on PSS. The study found that sleep quality influences PSS through depressed mood in older adults, which enriched the theoretical basis of the field. Findings also offer some practical implications. Particularly for community practitioners, the current findings suggest that improving sleep quality can be a strategy for improving psychological health and social functioning (e.g., PSS) in older adults.
Keywords
Introduction
Old age is the last stage in human development, in which older adults have to face the physical and mental challenges of aging (Gupta & Singh, 2019). In the face of these challenges, sleep quality and perceived social support (PSS) are acknowledged to play indispensable roles in enhancing the adaptation of later life and improving the health condition and well-being of older adults. Both have received widespread attention from researchers. In previous studies, the significant correlation between sleep quality and PSS in older adults has been consistently supported (de Grey et al., 2018). Specifically, good sleep quality has been widely established to be significantly associated with a high level of PSS in older adults (e.g., de Grey et al., 2018). By contrast, people with poor sleep quality tend to exhibit some deterioration of psychological health, leading to a more deprived social contact and more limited PSS (Beck et al., 1976; Li & Zhang, 2015).
However, studies using longitudinal designs to investigate the temporal direction of the relationship between sleep quality and PSS in older adults are still relatively few. Furthermore, the empirical evidence of potential health mechanisms in the relationship between sleep quality and PSS is relatively lacking. Based on the above limitations, the current study aims to investigate the causal relationship between sleep quality and PSS in older adults by employing a one-year cross-lagged design. The study also aims to examine the role of depressed mood in the relationship between sleep quality and PSS. In the following section, we first develop a detailed theoretical rationale of the existing research and then present our hypothesis.
PSS in older adults
With the death of relatives and friends, relocation, retirement, and the occurrence of chronic diseases, older adults face many challenges in the maintenance of their social support (Turner, 1988). Social support can be defined as an exchange of emotional, instrumental, or informative resources in the context of informal relationships (i.e., nonprofessional) (Cohen, 2004). In identifying the structure and components of social support, beyond actual received social support (RSS), researchers proposed PSS. PPS mainly refers to recipients’ perceptions concerning the general availability of support and global satisfaction with support provided (Sarason et al., 1990). Some researchers suggested that RSS may improve outcomes only with modifications to the PSS. Compared with RSS, PSS, which has stronger linkages to other psychological variables, such as ego-resiliency and subjective well-being (Chen et al., 2021; Lee & Holtzer, 2020; Melrose et al., 2015), is a more consistent predictor of outcome variables (Haber et al., 2007).
The stress-buffering theory proposed that as an important resource in social life, PSS plays a buffering and protective role in the relationship between stress and psychological well-being (Cohen & Wills, 1985; Holt & Espelage, 2005). Previous studies indicated that PSS can help older adults obtain the beneficial effects of the reduction in anxiety levels or the solution to problems from several sources, such as family, friends, or neighbors (Lee & Holtzer, 2020), thereby significantly affecting the levels of mental health in older adults (Bozo et al., 2009). In addition, PSS can provide health and survival benefits to older adults by strengthening coping and recovery when ill or by enhancing biological mechanisms, such as the immune, metabolic, and cardiovascular systems that protect against illness (White et al., 2009).
Given the significance of PSS, researchers explored the factors that have significant effects on PSS. The previous literature had established that some personality traits, including self-esteem, social conformity, and feelings of personal control, are all significant predictors of PSS (Pierce et al., 1997; Xia et al., 2012). In addition, researchers tend to discuss the influence of physical factors or health-related behaviors on PSS from the perspective of the mind–body interaction. That is, the mind and body reflect two fundamentally different entities that influence and interact with each other (Simpson et al., 2006). The effects of physical illness and health-related behaviors on PSS cannot be ignored and warrant further in-depth investigation.
Sleep quality in older adults
Among physiological factors influencing PSS, exploring the role of sleep quality is an avenue of great interest. Sleep is a vital regenerative behavior that promotes individual health and well-being (Chen et al., 2016). For older adults, continuous poor sleep quality has also been increasingly considered an important behavioral risk factor for cognitive decline, chronic diseases, health-related quality of life decrease, and mortality (Zisberg et al., 2010). Sleep is not only important for physiology, cognition, and behavior but is also closely associated with various psychosocial outcomes (Chen et al., 2016). Epidemiologists and social scientists have demonstrated that after controlling for factors, such as health and functional ability (Hanson & Ruthig, 2012; Lau et al., 2015), poor sleep is still significantly associated with pessimism (Lau et al., 2015), impaired decision-making (Killgore et al., 2010), and negative interpersonal responses to frustration (Kahn-Greene et al., 2006). Thus, we can expect that sleep plays an important role in the performance and perception of various psychosocial outcomes, including PSS.
Relationship between sleep quality and PSS
In recent years, the relationship between sleep quality and PSS in varying populations has received increasing attention from researchers (de Grey et al., 2018). Presently, researchers generally accepted that the relationship between sleep quality and PSS is bidirectional (Nordin et al., 2012). On the one hand, several previous cross-sectional studies showed that stronger relations with friends and relatives may lead to less sleep disturbance (Ailshire & Burgard, 2012; Yao et al., 2008). On the other hand, a growing body of research also emphasized that increased sleep continuity and better sleep quality are closely associated with positive social support and successful late-life adaptation (de Grey et al., 2018; Kent et al., 2015; Troxel et al., 2010). On the contrary, the presence of sleep disorders, such as sleep apnea, adversely affects relationship functioning (McFadyen et al., 2001). Some studies provided more direct evidence on the bidirectional relationship between sleep quality and social support in older adults. A four-year longitudinal study by Yang et al. (2013) found that poor marital quality, an important dimension of social support, was a risk factor for sleep disturbance for older adults. In turn, sleep disturbance may lead to lower marital quality. Cheng et al. (2018) also found that restless sleep and weak social networks reciprocally influence each other through depressed moods among the elderly.
However, few studies systematically investigated how sleep quality affects PSS in older adults using a longitudinal design, whereas previous studies mainly focused on explaining how social network affects sleep condition (e.g., Chung, 2017; Mai et al., 2017). For example, researchers argued that social support appears to provide social timekeeping that promotes the control of circadian rhythms and thus helps individuals enforce a more consistent circadian sleep–wake regulation with the outside world (Zisberg et al., 2010). By contrast, the longitudinal effect of sleep quality on PSS has been greatly neglected in previous studies, as shown by the limited attention and investigation. Killgore et al. (2008) suggested that sleep loss is associated with increased blame and hostility, reduced willingness to make concessions and restitution, and a general increase in atypical or impulsive responses, all of which are antithetical to harmonious interpersonal relations. On the contrary, adequate sleep serves as a resource of recovery that buffers the effect of negative social interactions and maintains the smoothness of social interactions. Nevertheless, direct evidence to test the effect of sleep quality on PSS is still lacking, and no definitive conclusions can be drawn regarding causality.
Health mechanism in the relationship between sleep quality and PSS
In reviewing the effect of sleep quality on PSS in older adults, we also noted that previous studies overlooked potential mechanisms underlying the linkage between sleep quality and PSS. Troxel and his colleagues (2007) proposed a model to explain the reciprocal associations between sleep and interpersonal function. They argued that sleep is linked with relationship functioning through psychological, behavioral, chronobiological, and physiological mechanisms. Specifically, sleep disturbance caused by a sleep disorder or temporary perturbations may have adverse effects on relationship functioning. Such relationship functioning is affected by affecting emotion regulation, increasing the risk for certain psychiatric illnesses, influencing health-risk behaviors, and altering physiological responses. Among the range of biopsychosocial factors mentioned above, as a critical domain of psychological health, the depressed mood has been widely documented to have significant relationships with sleep and social relationships (Cheng et al., 2018; Liu et al., 2016; Zimmerman et al., 2013).
In older adults with a general decline in sleep quality, depressed mood may be an underlying mechanism for the relationship between sleep quality and PSS. According to the model suggested by Troxel et al. (2007), impaired sleep adversely affects emotion regulation in the form of depression, confusion, and anger, including greater subjective feelings of frustration with sleep loss (Kahn-Greene et al., 2006), which in turn leads to more negative interpersonal situations. Moreover, the physiological dysregulation associated with insomnia or sleep disturbance results in psychological problems, such as depression, which cause individuals to be withdrawn from networking activities (Maier & Watkins, 1998). More specifically, poor sleep has always been shown to disrupt efforts to regulate emotion (Lillis et al., 2018), amplifying negative emotions in response to unpleasant events and reducing positive responses to pleasant ones (Dov et al., 2005). Some researchers argued that sleep quality is one of the root causes of depression in older adults (Zhang et al., 2020). Scholars also demonstrated that with the decline of psychological health, older adults tend to passively withdraw from their social world, which would weaken an individual's social participation (Aartsen et al., 2004) and be detrimental to the maintenance of social networks (Li & Zhang, 2015). Based on the previous literature reviewed above, depressed mood may be a potential mediator of the relationship between sleep quality and PSS.
Current study
Drawing on the literature reviewed above, a growing number of studies focused on the relationship between sleep quality and PSS in various populations. However, for the older population, two issues still need to be further addressed. First, to our knowledge, prospective longitudinal investigations on the causal relationship between sleep quality and PSS in older adults are still lacking. Second, studies focusing on the health mechanisms, particularly for the mediating role of depressed mood in the relationship between sleep quality and PSS, have received limited attention in previous studies.
Based on the limitations mentioned above, the current study systematically examined the temporal relationship between sleep quality and PSS and the mediating role of depressed mood in older adults using a one-year three-wave longitudinal design at six-month intervals. We hypothesized the following:
Method
Participants
This study was from a community-based survey project that was conducted on a rolling basis and updated continuously. Participants were recruited from six medium-sized (about 10,000 population) communities in Xi’an that were established at different times: established for less than 10 years, established for about 20 years, and established for about 30 years. We publicized our study by posters in the community square or activity room of the neighborhood committee and recruited participants who were aged 55 (female) or 60 (male) and above (according to the current regulations on the statutory retirement age in China), with normal or corrected vision, and no cognitive impairment or brain disease. Additionally, we also used a snowball sampling method, in which recruited participants were also encouraged to invite their friends or acquaintances, who also might be interested, to join our survey. The participants who agreed to allow follow-up contact left their phone numbers and then completed the booklet of questionnaires independently in a quiet room. The researchers assured the participants that the study was conducted purely for research purposes and their participation was voluntary. The participants were free to decline participation without any negative consequences. Three waves of data were collected, followed by follow-up measurements at six-month intervals. The respondents participated in subsequent waves only if they had participated in previous waves. Out of 707 participants that completed our measures at Time 1 (starting in April 2018), 411 participants completed at Time 2 (starting in October 2018), and finally 281 participants completed at Time 3 (starting in April 2019), representing a total of 281 participants who completed all three time measurements. The age range of the participants was 55–87 years at Time 1, with a mean of 68.09 years (SD = 7.51). All participants in the study received a gift worth 20 to 25 yuan as a reward for each of the assessments.
Measures
Perceived social support
Perceived social support was assessed with five items (specific items include “I get emotional help and support I need from my family,” “I can talk about my problems with my family,” “I have friends with whom I can share my joys and sorrows,” “There is a special person in my life who cares about my feelings,” and “I can talk about my problems with my friends”) from the Chinese version of the Multidimensional Scale of Perceived Social Support (MSPSS) (Jiang, 1999; Procidano & Heller, 1983). According to the study conducted by Cheng and Chan (2004), with a sample of 2,105 high school students in Hong Kong, the five items had the highest factor loadings among the items in the full scale. Participants were asked to rate the five items on a 7-point Likert-type scale from 1 (very strongly disagree) to 7 (very strongly agree). Higher scores reflect greater perceived adequacy of support. Cronbach's α for the scale in the current study were 0.816 (T1), 0.802 (T2), 0.799 (T3), respectively.
In previous literature, the MSPSS has shown good reliability and validity across a number of different groups, including older adults (Stanley et al., 1998), adolescents (Edwards, 2004), and university students (Zhang et al., 2018). On this basis, evidence for the reliability and validity of a simplified version of the scale consisting of representative items selected from the full scale should, to some extent, be transferable from one group to another. Therefore, to increase statistical confidence of the validity of the current five items, we used another sample of 1,614 Chinese adolescents (consisting of 821 males and 793 females, with a mean age of 15.96 ± 0.92 years for males and 15.84 ± 0.89 years for females) to examine the relevance of the five items to the 12-item full scale. The result showed that the correlation between the total score of five items and the total score of 12 items was 0.94, p < .001, indicating that the selected five items reflect the original scale well with acceptable compatible validity.
Sleep quality
Overall sleep quality perceived by participants was assessed with the Chinese version of the Pittsburgh Sleep Quality Index questionnaire (PSQI) (Buysse et al., 1989), which was revised by Liu and Tang (1996). Sample items for the assessment are, “During the past month, when have you usually gone to bed at night?” and “During the past month, when have you usually gotten up in the morning?” Nineteen individual items were recoded and transformed into seven components: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction (Buysse et al., 1989), each of which has a range of 0 (no difficulty) to 3 (severe difficulty) (e.g., calculate the time spent in bed by subtracting the time to go to bed from the time to get up, and then divide actual sleep duration by it to generate the component of habitual sleep efficiency). The sum of scores for these seven components yielded one global score ranging from 0 (good sleep quality) to 21 (poor sleep quality). This self-report tool is frequently used to evaluate sleep quality in various populations (Mollayeva et al., 2016), including older adults (Beaudreau et al., 2012). In the current study, Cronbach's α were 0.819 at T1, 0.818 at T2, and 0.809 at T3.
Depressed mood
We measured depressed mood using the five items with the highest factor loadings (e.g., “I felt sad” and “I could not get ‘going’”) from the Chinese version of the Center for Epidemiological Studies Depression (CES-D) Scale (Dang et al., 2020; Feng et al., 2016; Kohout et al., 1993). Participants rated the frequency that each mood or symptom occurred “during the past week” on a 4-point scale, with 0 being “less than one day” and 3 being “five to seven days,” with higher scores representing higher levels of depressed mood in the last week (Andresen et al., 1994). To verify the validity of these five items, the correlation between these five items and the 13 items of the original scale was further examined using the same sample of 1,614 adolescents (see the above paragraph for the detailed information), which showed a significant positive correlation (r = .93, p < .001). It indicated that these five items have acceptable compatible validity. In the present study, Cronbach's α for the three measurements were 0.738 (T1), 0.830 (T2), and 0.796 (T3).
Demographic factors, socioeconomic status, self-rated health
Demographic factors included gender (male/ female) and age (in years). Socioeconomic status included education (low/ intermediate/ high) and income per year (<11,999 CNY/12,000–35,999 CNY/>36,000 CNY). In addition, we used a one-item self-assessment to measure participants’ health status (i.e., “Overall, how do you feel about your health”). Participants indicated their degree of agreement with the item on a 5-point Likert scale (1 = very unhealthy, 5 = very healthy).
Data analysis strategy
In this study, the data analyses were carried out in the following steps. First, to test whether the loss of participants was random, chi-square tests and t-tests were conducted to evaluate possible differences in the participants’ characteristics between the included and excluded participants. Next, we mainly focused on descriptive statistics and correlations between the variables. Then, we used AMOS 23.0 to evaluate the cross-lagged panel model and longitudinal mediation model, which enabled the analysis of longitudinal relationships. According to the standards of the model and data fitting, the criteria and acceptable thresholds for evaluating model fit were χ2, df, CFI (>0.90), GFI (>0.90), SRMR (<0.08), and RMSEA (<0.08) (Bentler & Bonett, 1980).
Results
Attrition analyses
To evaluate possible differences between the participants who completed all three waves and those who dropped out, chi-square tests and t-tests were conducted. The demographic characteristics of the included and excluded participants based on whether they completed all three-wave measurements are presented in Table 1. The chi-square tests showed no significant differences between excluded and retained participants in terms of gender (χ2(1) = 1.17, p > .05), income (χ2(2) = 1.13, p > .05), or education (χ2(2) = 0.65, p > .05). Similarly, the results of the independent sample t-tests showed no significant differences in self-rated health (t (705) = 0.29, p > .05) between the participants who completed all three waves and those who dropped out. This indicates that the attrition was random.
Demographic characteristics of the participants.

The gender ratio was a little skewed and could potentially affect the stability of the results. To test whether the gender ratio of the sample had any effect on the results, we used SPSS to randomly select 86 participants from an overall female sample and constituted a new sample of 172 participants with the original 86 male participants. Then we performed the same data analysis using the new sample of 172 participants. We compared the results of the 172 participants with the results of the 281 participants and found that there was no significant difference between the results from the two samples. Therefore, the skewed gender ratio should not affect the stability of the results.
Correlation analyses
The descriptive statistics and bivariate Pearson correlations of the continuous variables are presented in Table 2. As shown in Table 2, the correlations between scores of PSQI, depressed mood, and PSS were significant across all three waves. Besides, the correlations between sleep quality at the three measurement times, the correlations between depressed mood at the three measurement times, and the correlations between PSS at the three measurement times were significant. Finally, the synchronization correlation coefficients between sleep quality, depressed mood, and PSS were significant.
Means, standard deviations, and correlations of sleep quality, PSS, and depressed mood.
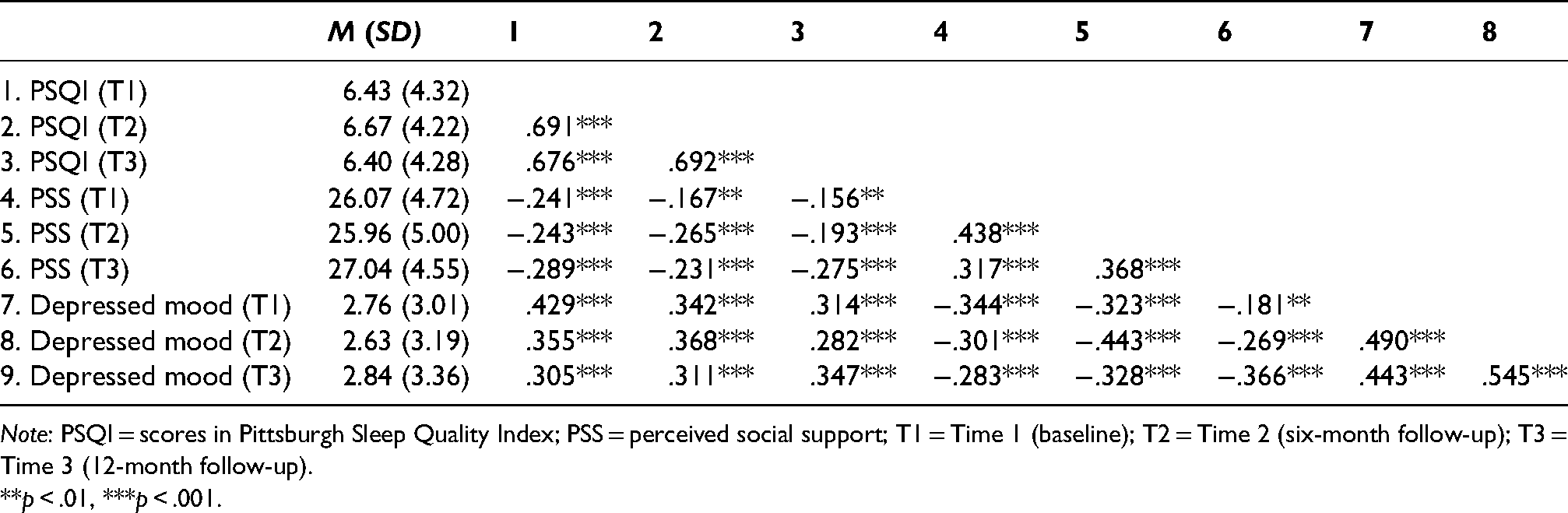
Note: PSQI = scores in Pittsburgh Sleep Quality Index; PSS = perceived social support; T1 = Time 1 (baseline); T2 = Time 2 (six-month follow-up); T3 = Time 3 (12-month follow-up).
**p < .01, ***p < .001.
Cross-lagged panel analysis
To explore the temporal relationship between sleep quality and PSS more rigorously, we followed Martens and Haase’s (2006) suggestion to test four-nested models in cross-lagged panel analyses. The first model (M1) was an initial model that includes just the autoregressive correlations of the baseline variables (i.e., the pathways from sleep quality at T1 to sleep quality at T2, sleep quality at T2 to sleep quality at T3 and the pathways from PSS at T1 to PSS at T2, PSS at T2 to PSS at T3). The second model (M2) added the prediction of one variable at T1 and T2, respectively, on the other variable at T2 and T3 (i.e., autoregressive paths plus the paths from sleep quality at T1 to PSS at T2 and sleep quality at T2 to PSS at T3). The third model (M3) examined the other cross-lagged path (i.e., autoregressive paths plus the paths from PSS at T1 to sleep quality at T2 and PSS at T2 to sleep quality at T3). Finally, the fourth model (M4) had fully cross-lagged paths and autoregressive paths. The model-fitting indices are shown in Table 3.
Model-fit statistics.

As can be seen in Table 3, the autoregressive model (M1) showed a reasonable fit to the data, as reflected by the fact that CFI, TLI, GFI, and SRMR were within the desired range, and RMSEA was marginally acceptable. Next, we used the difference between the χ2 for each model and the χ2 given by the autoregressive model (Δχ2) to evaluate whether the other three models improved the autoregressive model (M1). When a nonsignificant Δχ2 was found between the nested models, the more parsimonious model was deemed superior. As shown in Table 3, M2 provided a significantly better fit to the data than M1, Δχ2(2) = 12.573, p < .01.
M3 was tested next and also fit the data well, as reflected in CFI, TLI, GFI, and SRMR, values that were all within the desired range except for the value of RMSEA. For the comparison between M1 and M3, M3 did not provide a significantly better fit to the data than did the autoregressive model Δχ2(2) = 0.065, p > .05.
Finally, M4 showed a better fit than M1, Δχ2(4) = 12.670, p < .05. However, M4 did not show a better fit than M2, Δχ2(2) = 0.097, p > .05. Besides, neither of the pathways from PSS (at either Time 1 or Time 2) to subsequent values of sleep quality were statistically significant (see Figure 1). Based on the above results, M2 provided the more parsimonious result, and M2 can therefore be accepted as the optimal model.
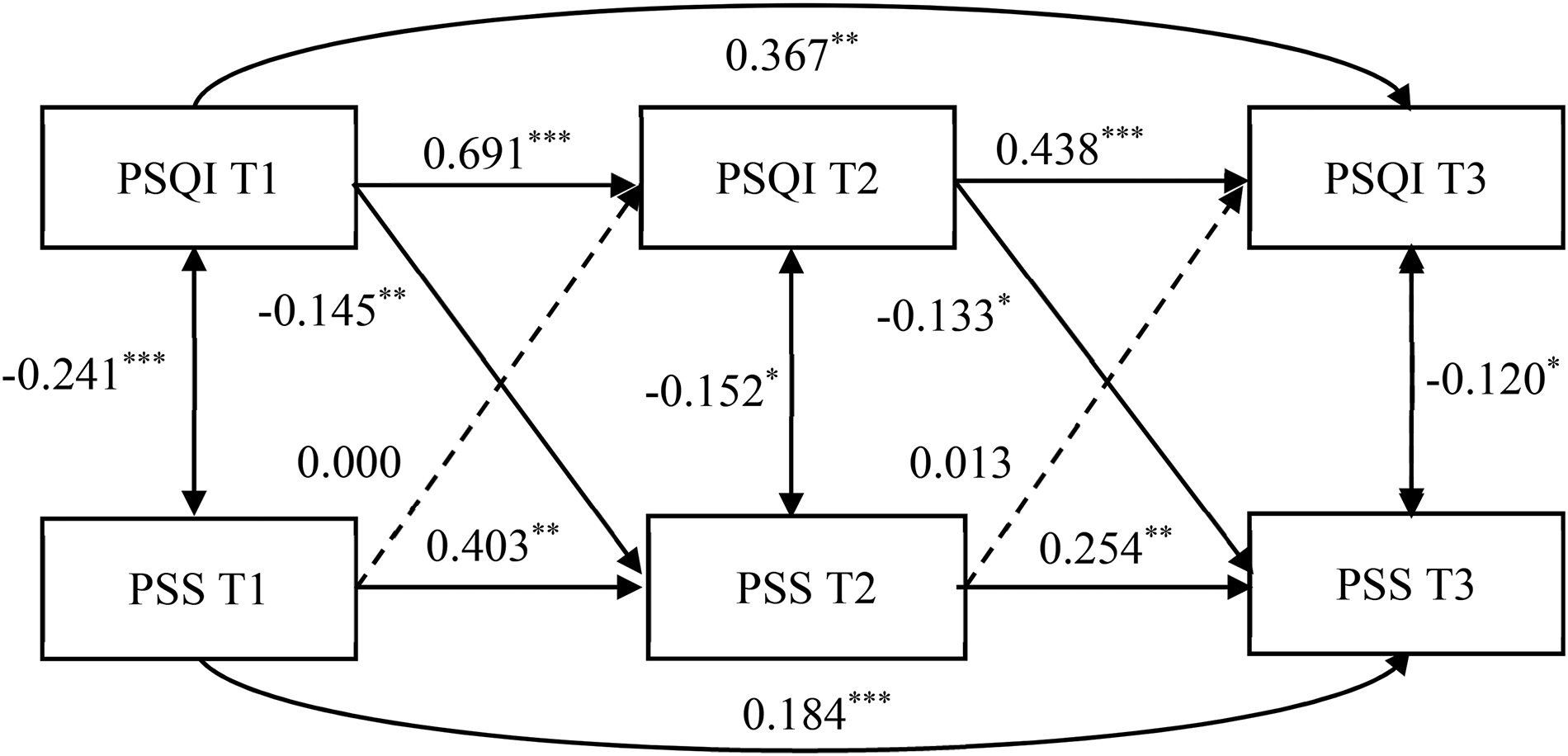
A cross-lagged panel model of older adults’ sleep quality and PSS, with all coefficients standardized. Note: T1 = Time 1 (baseline); T2 = Time 2 (six-month follow-up); T3 = Time 3 (12-month follow-up). PSQI = scores in Pittsburgh Sleep Quality Index; PSS = scores in Multidimensional Scale of Perceived Social Support. Solid lines indicate statistically significant paths (p < 0.05), dotted lines denote nonsignificant paths, and curves represent the autoregressive coefficients of variables from T1 to T3. *p < .05, **p < .01, ***p < .001.
The final cross-lagged panel model for the relationship between sleep quality and PSS across time is presented in Figure 1. In this model, the paths from sleep quality at T1 to PSS at T2 (β = −0.17, SE = 0.063, p < .01) and from sleep quality at T2 to PSS at T3 (β = −0.14, SE = 0.061, p < .05) were both statistically significant. These results indicated that sleep quality predicted PSS after six months in older adults, which supported our Hypothesis 1.
Longitudinal mediation analysis
To verify the causal relationship between sleep quality and PSS, and to further explore the potential mechanism underlying the association between sleep quality and PSS, we developed a longitudinal mediation model based on the results of the cross-lagged analysis. Specifically, we regressed the depressed mood at T2 on sleep quality at T1 and regressed PSS at T3 on depressed mood at T2. The longitudinal mediation analysis reported the following model-fit finding: χ2 (16) = 39.22, CFI = 0.974, GFI = 0.971, SRMR = 0.076, RMSEA = 0.072.
As shown in Figure 2, sleep quality at T1 predicted depressed mood at T2 (β = 0.12, SE = 0.040, p < .01). Moreover, depressed mood at T2 negatively predicted PSS at T3 (β = −0.17, SE = 0.083, p < .05). Bootstrapping procedures showed that sleep quality at T1 exerted a statistically significant indirect effect on PSS at T3 through depressed mood at T2 (indirect effect = −0.019, 95%CI = [−0.051, −0.001]). In conclusion, the depressed mood could mediate the relationship between sleep quality and PSS, supporting our Hypothesis 2.

The longitudinal mediation relations among sleep quality, depressed mood, and PSS, with all coefficients standardized. Note: T1 = Time 1 (baseline); T2 = Time 2 (six-month follow-up); T3 = Time 3 (12-month follow-up). Standardized coefficients are reported. Solid lines indicate statistically significant paths (p < 0.05), dotted lines denote nonsignificant paths. *p < .05, **p < .01, ***p < .001.
Last, we tested a longitudinal mediation competition model by swapping the independent and dependent variables, which regressed the depressed mood at T2 on PSS at T1 and regressed sleep quality at T3 on depressed mood at T2. The results showed that PSS at T1 predicted depressed mood at T2 (β = −0.16, SE = 0.04, p = .003), while the path coefficient for depressed mood at T2 predicting sleep quality at T3 was not significant (β = −0.00, SE = 0.06, p = .923). Further, Bootstrapping analyses demonstrated that depressed mood at T2 did not mediate the effects of PSS at T1 on sleep quality at T3 (indirect effect = 0.001, 95%CI = [−0.015, 0.019]). Therefore, the pathway of T1 PSS leading to T2 depressed mood leading to T3 sleep quality was not stable and the competition model did not hold. These results further supported our hypothesis regarding the causal direction between sleep quality and PSS and the mediating role of depressed mood in this relationship.
Discussion
The present study explored the causal relationship between sleep quality and PSS, and the mediating role that depressed mood played in the relation between sleep quality and PSS over one year. The cross-lagged panel analysis demonstrated that the path from sleep quality at T1 to PSS at T2, and the path from sleep quality at T2 to PSS at T3 were statistically significant. In addition, the longitudinal mediation analysis revealed that sleep quality at T1 negatively predicted depressed mood at T2, and depressed mood at T2 later negatively predicted PSS at T3. These analyses revealed the temporal order of the relationship between sleep quality and PSS, and that this relationship was mediated by depressed mood.
Based on sleep quality as a predictor of PSS over time in older adults, our findings were consistent with the views of epidemiologists. They argued that sleep provides fundamental supports for adaptive social and cognitive functioning. Specifically, lack of sleep adversely affects the ability to regulate emotions (Baldwin & Daugherty, 2004) and behavioral responses to interpersonal situations (Kahn-Greene et al., 2006), which brings about a propagating, self-reinforcing cycle for social withdrawal and separation (Ben Simon & Walker, 2018). Sleep is a resource of recovery. Continuous poor sleep quality may result in inadequate resources available for older adults to interact with family, friends, and significant others to obtain a sense of belonging (Hagerty et al., 1992); on the contrary, high quality of sleep ensures older adults would acquire enough energy for interpersonal communication and social participation to maximize the satisfaction of PSS.
In the present study, the depressed mood was found to mediate the relation between sleep quality and PSS, which further supports our hypothesis of the causal direction between sleep quality and PSS. How can depressed mood mediate the effect of sleep quality on PSS? The cognitive theory of depression argues that older adults with insomnia endorsed stronger beliefs about the negative consequences of insomnia (Beck et al., 1976). Similarly, older adults with poor sleep quality expressed more despair about the fear of losing control of their sleep and experienced more helplessness about its unpredictability, which leads to a higher level of depression. The study of Sadler et al. (2013) also suggested that poor sleep increases daytime tiredness and makes individuals more vulnerable to developing maladaptive sleep beliefs, a sense of hopelessness, and depression. The deterioration of psychological health, represented by the depressed mood in the current study, further leads older adults to withdraw from the social world and limit their activity to less-resourceful social networks (Li & Zhang, 2015) and eventually feel it is difficult to perceive support from social contacts.
Notably, inconsistent with the study of Cheng et al. (2018), who found that restless sleep and weak social networks reciprocally affect each other through depressed mood, our results only supported the effect of sleep quality on PSS through depressed mood. These differences across studies could be due to different operationalization and study time frame. We speculated that the effect of PSS on sleep quality may require a longer interval of data collection, a fact mainly reflected in previous longitudinal studies suggesting that bidirectional relationships between sleep and social functioning in older adults have a follow-up interval of more than two years (e.g. Cheng et al., 2018; Yang et al., 2013). In contrast, the current six-month follow-up interval may not be sufficient to observe the effect of PSS on sleep quality. The speculation remains to be further tested and addressed through multiple study designs and outcome measures, or in future meta-analyses.
The present longitudinal study illustrated that poor sleep quality influences PSS in older adults through depressed mood. This finding furthers the field's understanding of the causal relationship between sleep quality and PSS, and the underlying health mechanism of the linkage between the two in older adults. Practically, the current study also has significant implications for practitioners who are working on community service. Interventions such as meditative movement (a new category of exercise integrating physical activity and meditation) (Wu et al., 2015) could be designed to protect community-dwelling older adults from insomnia and improve their sleep quality. This would further contribute to their psychological health, increase their participation in social activities and conversation, and ultimately achieve a mutually reinforcing cycle between sleep quality and PSS.
This study has some limitations that should be addressed in future research. First, this study was conducted in the Chinese cultural context. Under the influence of Chinese traditional culture and social desirability (Wu et al., 2010), Chinese are likely to pay more attention to maintaining harmonious interpersonal relations and have a higher level of need for social support, which requires individuals to devote more energy and resources to maintain a certain level of PSS. This may lead to a greater sensitivity of PSS to changes in sleep quality in Chinese older adults. In contrast, studies in western culture found relatively weaker effects of sleep on relationship functioning and paid more attention to the effect of PSS on sleep quality, the opposite direction (e.g., Chung, 2017; Eriksen et al., 2007; Jansson & Linton, 2006; Pow et al., 2017). In future research, similar studies should be conducted in other cultural contexts to further strengthen the knowledge in this research area. Second, the sleep quality was based on subjective and self-report measures. Although measuring the subjective perception of sleep is important, and subjective sleep quality has been linked to objective sleep indicators, we do not have measures (e.g., actigraphy, polysomnography) that might provide converging evidence for such links (Kent et al., 2015). Future studies using methods with more refined sleep measures may illuminate these issues.
Footnotes
Acknowledgements
The authors would like to thank the National Social Science Fund of China (17BSH153) for funding this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the National Office for Philosophy and Social Sciences (grant number 17BSH153).