
Abstract
Background:
ICD-11’s digital architecture and granularity distinguish it from previous revisions and expand its applicability beyond mortality statistics and public health. The official ICD-11 version is updated annually. However, a separate online Maintenance Platform is continuously updated and hosts the Proposal Platform: a novel online tool that enables interested parties from all over the world to contribute to ICD-11 content. Anyone can register on the Platform to propose updates, such as adding new medical terms or improving existing descriptions, helping keep the classification relevant and inclusive. As a public, transparent system, users can view or comment on other users’ proposals. Proposals are carefully reviewed by expert WHO committees through a transparent, multi-step process that ensures scientific accuracy and consistency. High-priority updates, like emerging health conditions, can be fast-tracked for quicker inclusion. Once a proposal is accepted, it becomes effective in the following update. A clear justification is provided for rejected proposals. Since ICD-11 came into effect, most suggestions from users have been successfully implemented.
Objective:
This article describes the proposal submission process, the rigorous proposal review process, and the roles of the WHO reference groups and committees involved.
Conclusion:
ICD-11 is a free, digital global health classification that anyone can help improve by submitting proposals through an open, transparent platform.
Implications for health information management practice:
This inclusive system empowers users worldwide to shape ICD-11 to reflect the evolving real-world medical and public health practice and emerging needs. This also prevents the need for country-specific modifications, ultimately improving the comparability of clinical data at the international level.
Keywords
Introduction
For decades, the International Classification of Diseases (ICD) has been the basis for collecting and reporting statistics on diseases and health conditions. In January 2022, the latest ICD revision, ICD-11, came into effect. ICD-11’s innovative digital architecture and high level of granularity distinguish it from previous revisions and widen its use beyond traditional mortality statistics and public health (Chute and Çelik, 2021). ICD-11 is both a classification and an international terminology standard. Thanks to a wealth of index terms (which include preferred terms, synonyms, inclusion terms, lay terms and clinical term variants), extension codes, and the ability to post-coordinate (combine) multiple codes into single clusters, ICD-11 can now comprehensively describe medical diagnoses. These features and more, qualify ICD-11 as an instrument for capturing diagnoses for casemix and Diagnosis-Related Grouping (World Health Organisation, 2022a), healthcare quality and safety (Southern et al., 2021), rare disease registration (Mazzucato et al., 2023) and recording external causes of injury or poisoning. As such, ICD-11 eliminates the need for country-specific modifications (Feinstein et al., 2023). For the first time, the world can really speak one language on health, leveraging our ability to achieve semantic interoperability in digital health data systems (Pan American Health Organisation, 2021).
To keep ICD-11 clinically up to date, while maintaining the stability of the classification, three different release cycles are scheduled by the WHO. Updates concerning high-level entities with a big statistical impact are released every 5 years to ensure stability for international use. Updates at a finer level of detail are released annually including updating index terms, postcoordination options and entity descriptions as well as correcting errors. The third release cycle concerns mortality and morbidity coding rules which are updated every 10 years. Updates that involve restructuring can only be made during major revisions of the ICD (World Health Organisation, 2025a). In 2032, an assessment will determine whether a new revision of the ICD is needed (World Health Organisation, 2019). ICD-11 is a living classification and terminology undergoing continuous improvement not only due to the never-ending scientific advances and newly emerging diseases but also to meet the needs of its users worldwide (Harrison et al., 2021). Suggestions for the enhancement of ICD-11 content will likely increase as more countries prepare for the transition to ICD-11 (Lee and Kim, 2023; Ooi et al., 2024) or have already started its implementation (Ibrahim et al., 2022; Zhang et al., 2024). The WHO describes ICD-11 as “by the people, for the people,” the “people” being all users from: different countries, healthcare systems, scientific interest groups (e.g. rare diseases, quality and safety, psychiatry), levels of health services (primary, secondary, tertiary care), professions (clinicians, coders), and partners (e.g. OrphaNet and Iris; Mazzucato et al., 2023). The “people” are allowed to contribute to ICD-11 and enhance its content through a standardised, open, transparent, evidence-based proposal mechanism on an online platform developed by the WHO (World Health Organisation, 2025a). This ensures that the needs of all users are continuously met, further underlining the idea that ICD-11 is “the” international classification and terminology and can be used “as-is” without additional stakeholder-specific modification.
The ICD-11 proposal mechanism
The innovative digital infrastructure and information framework of ICD-11 are fundamental to the proposal mechanism. ICD-11 for Mortality and Morbidity Statistics (ICD-11 MMS) is a traditional hierarchical classification used for standardised international statistical tabulation. However, unlike previous ICD revisions, ICD-11 MMS is only one layer of ICD-11. Another important layer is the Foundation, a huge online knowledge base or semantic network of more than 80,000 units called “entities” representing “the whole ICD universe” (Harrison et al., 2021; World Health Organisation, 2025a). Each entity has a unique Uniform Resource Identifier (URI) and a standardised template of attributes describing the entity and its relationships called the “Content model” (World Health Organisation, 2025a). ICD-11 MMS is a “linearisation” that is, a selected subset of mutually exclusive entities from the Foundation.
The official release of the classification, the ICD-11 MMS “blue browser” (also called the frozen version) is updated annually, whereas the Foundation is a living database continuously updated (World Health Organisation, 2025b). Ongoing updates to the Foundation are performed through and reflected in the ICD-11 online Maintenance Platform, commonly referred to as the “orange browser” (World Health Organisation, 2025a, 2025c). The orange browser is not the official release of the classification and should not be used for coding as its content is constantly changing, sometimes daily. The Maintenance Platform hosts the Proposal Platform which provides the infrastructure for submitting proposals by users, delivering them to the appropriate reviewing body and providing feedback to authors. This is all done in an online transparent environment where anyone can view and comment on other users’ proposals and view WHO feedback. The Maintenance Platform also shows the updated ICD-11 where the proposed change, if accepted by WHO, has become part of the classification (World Health Organisation, 2025a). It is important to note that country-specific needs are captured in the Foundation, unless they also call for new categories in the standard linearisation.
The proposal submission process
Registration
The WHO-FIC Maintenance Platform can be reached via the ICD-11 homepage “Be Involved” section. The ICD-11 orange browser, Foundation and the Proposals menu (where proposals are submitted, viewed and commented on) can be accessed by clicking “ICD‑11 MMS” under “Reference Classifications” in the “Browse” box. No registration is needed to use the ICD-11 orange browser and explore the Foundation component. However, only registered users have access to the proposals menu. The registration process requires mandatory user information, including the user’s name, organisation or affiliation and country. This information will be displayed to other users along with each proposal or comment outlining the transparency of the process (World Health Organisation, 2025d).
Locating the ICD-11 entity to which the proposal relates
The proposal process starts with browsing the ICD-11 hierarchy on the orange browser to find the entity to which the proposal relates. ICD-11 MMS is organised into 28 chapters and sections. Proposals can be submitted at any entity in any of the chapters or sections. Once the desired entity is selected, the right side shows the Content model components of the entity including its parent, description, index terms, exclusions and permitted postcoordination axes. Postcoordination is the process by which additional codes are combined with the code of the selected entity to form a code cluster that provides a more granular representation of a diagnosis or health condition (Mabon et al., 2021; World Health Organisation, 2025a).
Identifying the type of proposal
At any given entity, proposals can be submitted to modify the position of the entity in the hierarchy and/or its content model components. The Proposal Platform allows users to submit five types of proposals: adding a new entity, removing an entity, enhancing an entity’s Content model components, changing postcoordination axes, and proposing complex hierarchical changes involving an entity. The latter includes any hierarchical change other than adding or removing an entity. Hierarchical changes in the Foundation, like adding or removing entities, apply to entities both above and below the shoreline (World Health Organisation, 2025e).
Each entity in the WHO-FIC Foundation has a unique identifier, namely a URI. In the ICD-11 MMS linearisation, which is a subset of the Foundation, some entities become categories and are given ICD-11 codes. These are described as “above the shoreline.” Other entities exist below the shoreline that is, they become index entries in the classification coded to (classified at) the categories under which they are indexed (Chute and Çelik, 2021). For example, functional dyspepsia, post-prandial distress syndrome and atonic dyspepsia are three separate entities in the Foundation. Each has a unique URI. However, in ICD-11 MMS, only functional dyspepsia is a category “DD90.3 Functional dyspepsia” (above the shoreline), while the other two entities exist below the shoreline as index entries under DD90.3. Although all three conditions are coded to DD90.3, they retain their uniqueness through their URIs (World Health Organisation, 2025b). If an entity is missing in ICD-11, users can propose to “add a new entity.” This proposal should be attached to the entity to which the new entity will become a child (Box 1, example 1). Users could also propose to “delete an entity” when an entity is considered incorrect or is a duplicate of another entity in the classification (Box 1, example 2). Suggesting amendments to an entity’s Content mode components is done through a “Content enhancement proposal.” Such proposals can be submitted to change the entity title, description, synonyms, or exclusions. Supplementing ICD-11 content with the widely used abbreviations and synonyms from different countries and specialties enriches the classification and ensures that it becomes a common language for medicine while maintaining its robust classification structure (Ibrahim et al., 2022; Box 1, example 3).
Proposal examples.
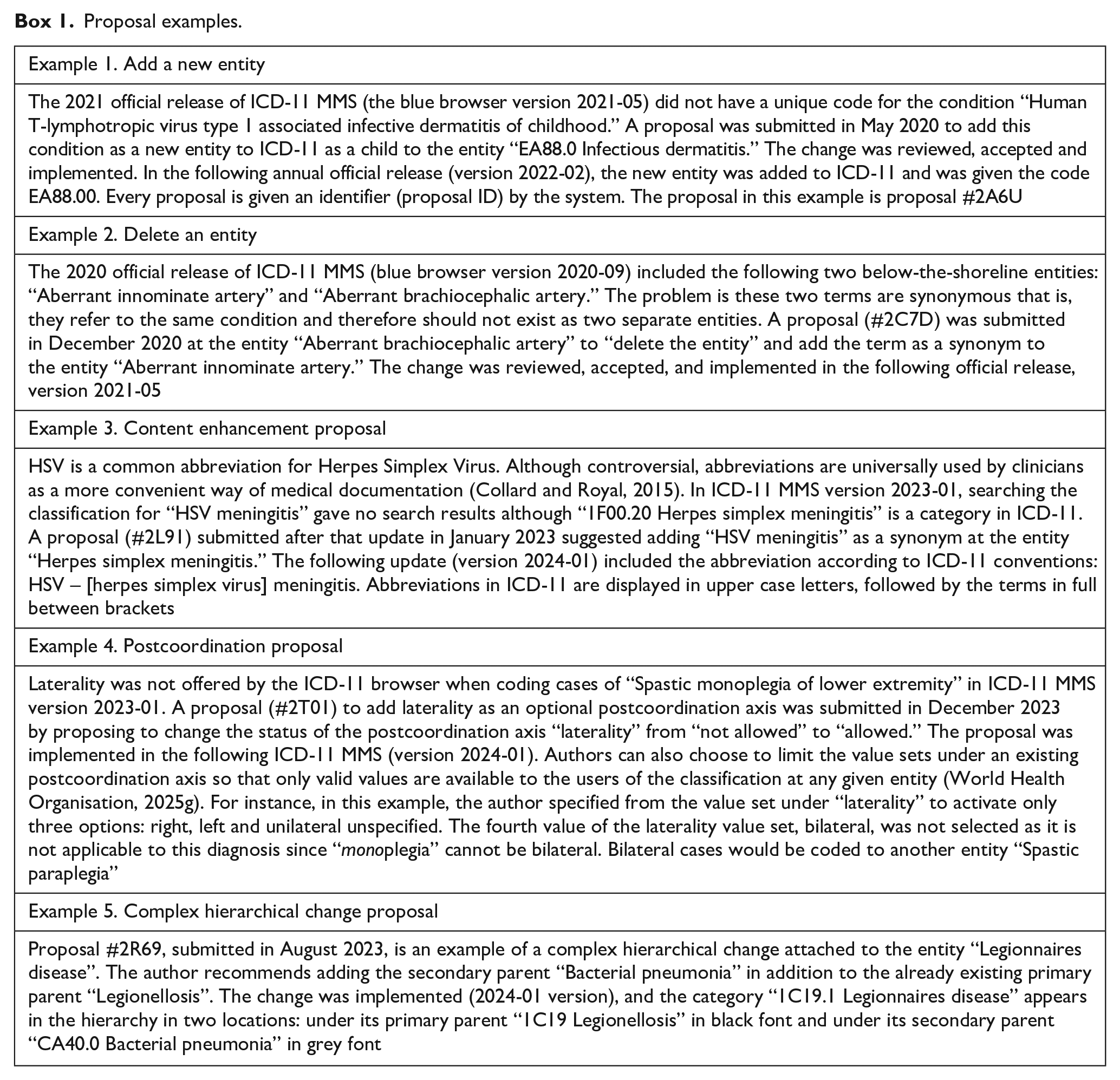
Postcoordination proposals are used to change the axes from which more codes could be added to the selected entity to form a cluster. From a list of possible postcoordination axes, one can change the status of each axis with respect to the selected entity by selecting “allowed,” “required” or “not allowed” from a drop-down menu. Selecting “allowed” means the author proposes to have this axis available to users for optional postcoordination. Selecting “required” means the author believes that this axis should be made mandatory that is, users must “code also” a value from this axis. “Not allowed” means that this axis should not be offered by the browser at this entity (World Health Organisation, 2025g; Box 1, example 4).
Proposals concerning changes other than the above should be submitted under “complex hierarchical changes.” This includes changing the coding status of an entity by moving it from below to above the shoreline or vice versa. This type of proposal also includes proposing structural changes such as reassigning the entity’s primary parent or secondary parent/s. In the ICD-11 Foundation, an entity may be classified under two or more parents. This is called multiple parenting. However, in the ICD-11 MMS linearisation, an entity can have only one primary parent for tabulation of statistical outputs to standardise statistical reporting. Any other parents become secondary parents (World Health Organisation, 2025f; Box 1, example 5).
Preparing the evidence
All proposals must be built on scientific evidence and knowledge of how health classifications work. A compelling rationale for the proposed change is needed together with supporting references from recognized peer-reviewed journals, WHO publications, official WHO meetings, or government and university publications or websites. An additional requirement when proposing to add a new entity is to provide a comprehensive “description” for the proposed entity. Descriptions are a key component of the Content model as they guarantee consistency in the meaning of coded data by all ICD-11 users, for all purposes (e.g. coding, analysis, translation), and in all settings. Furthermore, a detailed explanation is needed when submitting a “Complex Hierarchical Changes Proposal” explaining the nature and implications of the change (World Health Organisation, 2025a).
Creating the proposal
To submit a proposal, the author must be logged into the ICD-11 Maintenance Platform. Through the Proposals menu, clicking “ICD- add proposals/see in hierarchy” leads to the “Proposals home” where proposals are submitted. On the left-hand side, authors can browse the foundation hierarchy to find and select (click) the entity to which they wish to attach their proposal. Existing proposals attached to the selected entity automatically appear in a “proposal list” on the right-hand side of the screen. To avoid duplicating earlier proposals and reduce the burden of proposal review by the WHO, it is important to check whether others have already proposed the same changes. If so, there is an option to agree with the earlier proposal by simply clicking an “agree” icon. There is a “disagree” icon as well, should that be the case, with the option to add a comment (World Health Organisation, 2024a).
To create a new proposal, the author must select the type of proposal from the given list of options. After providing all requirements including rationale and references, authors can choose to save or submit their proposal. Submitted proposals are visible to all users of the Platform; saved (unsubmitted) proposals are not. Submitted proposals can be edited by the initiating author anytime if they have not been accepted or rejected by the WHO. Authors can also retract their proposals, in which case the proposal can no longer be accessed by the author or viewed by other Platform users.
Anyone can author an ICD-11 proposal once they register to the Maintenance Platform. This includes academics, clinicians, coders, health information managers, representatives of scientific communities, patient advocacy groups and the wider public. In some cases, proposals are submitted directly by the author and in others, they are submitted by a national body on their behalf such as a WHO-FIC Collaborating Centre or a country’s national health information or statistics office.
As more countries adopt ICD-11, piloting and translations often result in suggestions to improve the content of the classification such as proposals submitted from piloting in Kuwait and China by their WHO-FIC Collaborating Centres (Ibrahim et al., 2022; Zhang et al., 2024), and during the translation to the Czech language by the Czech Institute of Health Information and Statistics (Dankova and Zvolský, 2022). Numerous national government institutions and international medical associations have also submitted proposals to ensure that ICD-11 fulfils their needs such as the German Society for Endoprosthetics, the American Academy of Sleep Medicine, Orphanet, the International Association for the Study of Pain, the International Society for Nomenclature of Paediatric and Congenital Heart Disease. Proposals by the public including patients and advocacy groups mainly focused on changing disease names such as the 44 proposals submitted in August 2022 on renaming Mpox (Monkeypox) to avoid stigmatizing comments observed at the time (World Health Organisation, 2025h). Non-profit organisations supporting individuals with certain disorders also submitted proposals. Examples include proposals submitted by the Timothy Syndrome Alliance (proposal #2M6N), STXBP1 Foundation (proposal #2W2N) and the Ehlers–Danlos Society (proposal #2P56; World Health Organisation, 2025i).
Viewing proposals
The Proposal Platform allows users to view all submitted proposals, theirs and others. They can agree, disagree or comment. Proposals attached to an entity can be viewed in the same place where authors create proposals, the Proposals home browser (World Health Organisation, 2024a), by simply clicking that particular entity in the hierarchy. On the other hand, to view the full list of proposals, users need to click the “Proposal List/Search” option (World Health Organisation, 2025g).
The Proposal list shows all submitted proposals including the title of the entity, type of proposal, identifying number, date and time of submission, author name and proposal status. By default, the list is organised chronologically by submission date with the newest proposals appearing on top. With over 20,000 proposals submitted since July 2014, the filters and text search options provided by the Platform can help with the search (World Health Organisation, 2025i). Author names are clickable revealing the author’s organisation or affiliation and country. Clicking a proposal on the list opens it in full including author-provided details and any earlier comments made by other users or the WHO. Figure 1 show examples of the different types of proposals: adding a new entity (panels a and b), removing an entity (panel c), content enhancement proposal (panel d), postcoordination proposal (panel e) and complex hierarchical proposal (panel f).
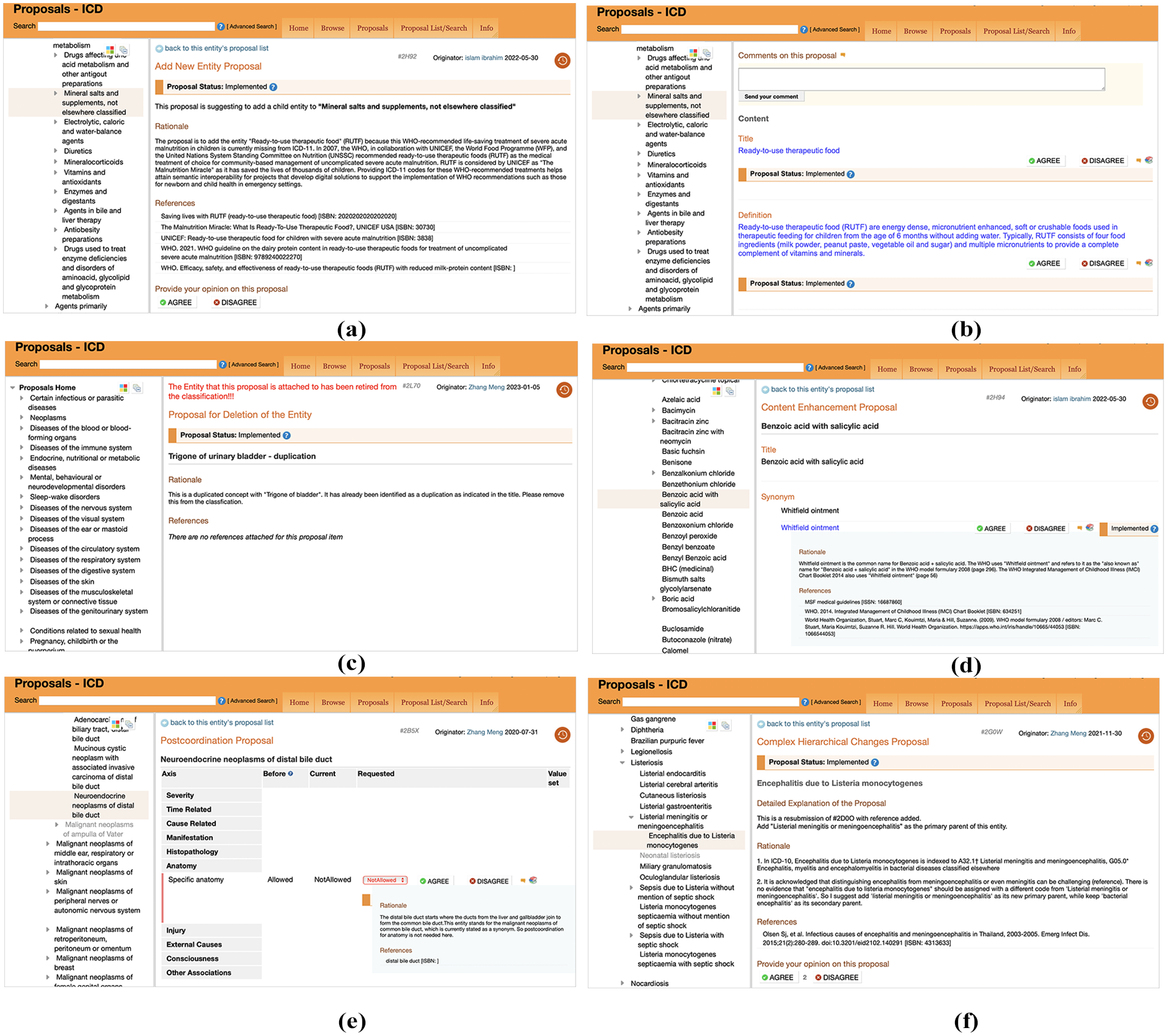
Examples of proposals. (a) An example of a proposal to add an entity. Panel (a) shows the top part of the screen which includes the rationale and references provided by the author. (b) An example of a proposal to add an entity. Panel (b) shows the lower part of the screen when scrolling down to reveal the title and definition proposed by the author for the new entity. (c) An example of a proposal to delete an entity. The entity itself is not highlighted in the hierarchy since the proposal has been implemented and the entity has been deleted from the classification. (d) An example of a content enhancement proposal where the author proposes to add a synonym to an entity. (e) An example of a postcoordination proposal where the author proposes to disallow the axis specific anatomy that was previously allowed for this entity. (f) An example of a complex hierarchical changes proposal.
The proposal review process
Proposals are forwarded to reviewers through the Proposal Platform where feedback and proposal status at various stages of the review process, as well as the outcome, are provided. An initial triage evaluates completeness. Incomplete proposals (e.g. lacking rationale or references, or lacking a description in case of “add entity proposals”) are returned to authors. Only complete proposals are considered for review. Proposals found to address urgently needed updates, such as the addition of emerging health conditions, are fast-tracked by the WHO (2025a).
The review workflow set by the WHO guarantees the consistency of the review process and maintains the structural integrity of ICD-11 as a classification. The aim is to ensure that the proposed changes are scientifically sound and serve the different use cases of ICD-11. Reviewers include scientific experts, classification experts, WHO-FIC network reference groups and advisory committees and WHO experts. The workflow involves four main WHO-FIC network reference groups and advisory committees: the Medical and Scientific Advisory Committee (MSAC), Mortality Reference Group (MRG), Morbidity Reference Group (MbRG) and the Classification and Statistics Advisory Committee (CSAC). Two more reference groups may be involved where applicable: the Functioning and Disability Reference Group (FDRG) and Traditional Medicine Reference Group (World Health Organisation, 2025a).
CSAC advises the WHO on maintaining the main purpose of the classification: producing morbidity and mortality statistics. The activities of the CSAC include deciding on the primary parents in the classification hierarchy, determining the optional postcoordination axes offered at different categories and deciding on whether an entity should be placed above or below the shoreline in ICD-11 MMS. Carrying out activities of this calibre requires a proficient level of knowledge and expertise in WHO classifications; hence, only professionals from WHO-FIC Collaborating Centres and officially nominated technical representatives from WHO member states can become CSAC members. Selecting the proposals to be submitted for final approval by the WHO-FIC Network Advisory Council for the following annual ICD-11 MMS update is also the responsibility of CSAC (World Health Organisation, 2024b).
As the main advisory committee, CSAC plays a crucial role in moderating the proposal review process. Proposals are reviewed by a “CSAC Small Group” (CSAC-SG) consisting of CSAC co-chairs and secretariats, WHO staff and WHO-FIC selected experts to determine whether the proposal is ready for review by the wider CSAC. The CSAC-SG may recommend to the wider CSAC that the proposal be accepted, rejected or accepted with modification. All decisions concerning the recommendations submitted to the wider CSAC require consensus among CSAC-SG (World Health Organisation, 2025a). If more information is needed to make a recommendation about a proposal, CSAC-SG can assign the proposal to relevant Reference Groups based on the type and nature of the proposal including MbRG, MRG, MSAC or FDRG (World Health Organisation, 2024b). For example, all proposals attached to the entity “sudden infant death syndrome” were referred to MRG for advice. Where necessary, proposals are submitted to external reviewers such as the proposal attached to the entity “Health devices, equipment and supplies” (proposal #230H); World Health Organisation, 2025i). CSAC-SG reviews the resulting feedback and comments before making a recommendation (World Health Organisation, 2025a).
The proposal is handed over to the wider CSAC for voting with transparency. The CSAC Secretariat documents CSAC-SG recommendations, suggested modifications, and any other comments on the Proposal Platform at the respective proposals. After several voting rounds, the final CSAC consensus recommendation to accept, reject or undergo further discussion is reached at the WHO-FIC annual meeting in October. The accepted proposals are handed over to the WHO for implementation (World Health Organisation, 2025a). Figure 2 depicts an overview of the submission and review process.
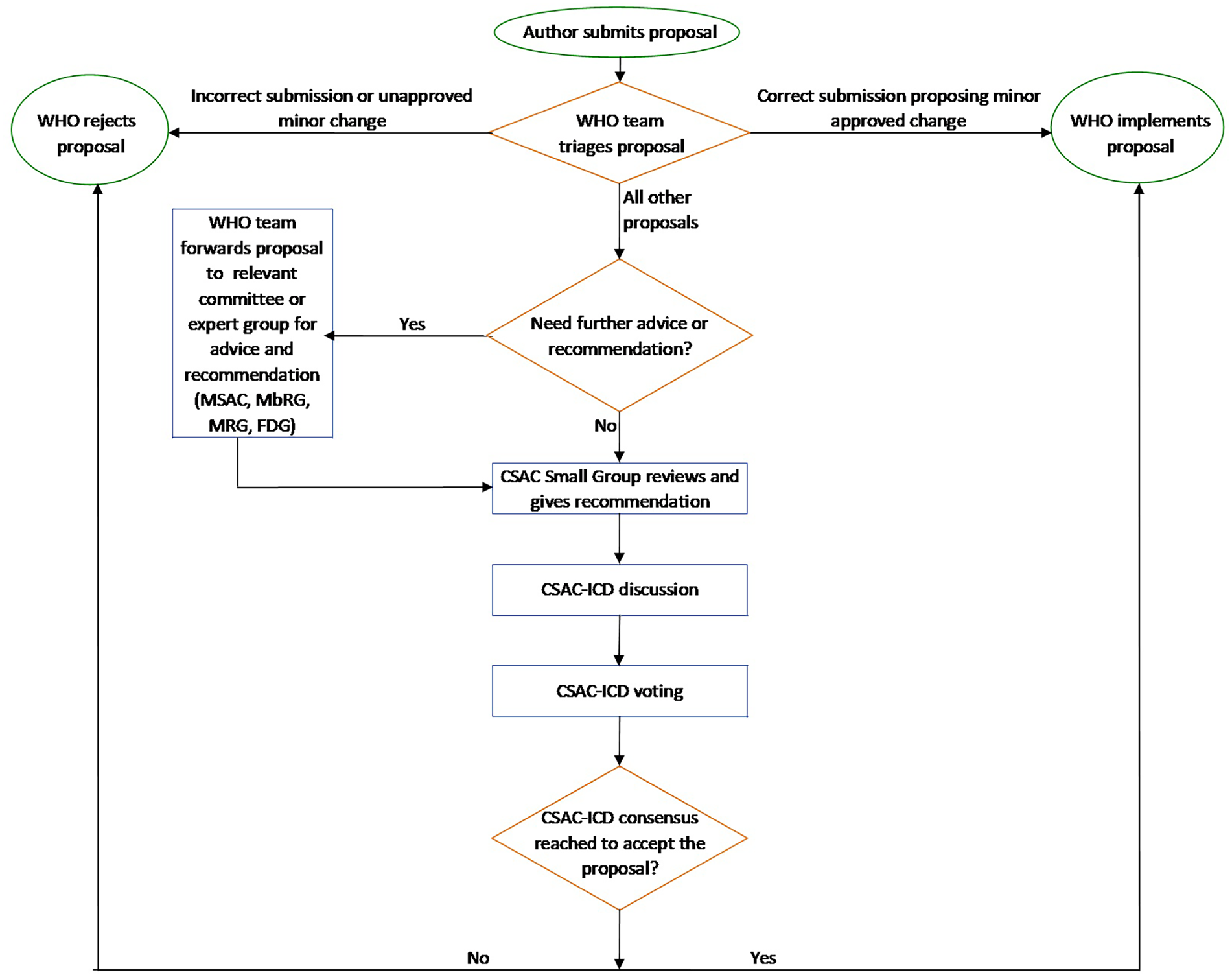
Flowchart of the proposal process.
Proposal outcomes
Once a final decision is reached on a proposal, it can no longer be edited by the author. A proposal may be “accepted” as-is or “accepted with modification”. Accepted proposals are implemented on the ICD Collaborative Authoring Tool (iCAT), the Platform that allows WHO editors to edit ICD-11 content. The change will be reflected in the orange browser the following day, and in the official release (the blue browser) in the following annual update. However, structural changes, such as altering a code, are deferred to the next major ICD-11 update (World Health Organisation, 2025a). To compare the content of successive annual releases, users can access earlier versions of ICD-11 via the “Earlier releases and update history” from the “Info” tab on the ICD-11 MMS blue browser (World Health Organisation, 2025b).
If a proposal is “rejected,” the reason behind the rejection is explained in the comments section. Proposals could be rejected for multiple reasons including but not limited to suggesting a change that already exists in ICD-11 (e.g. proposal #2W4L), disagrees with ICD-11 conventions (e.g. proposal #2V27), is not related to ICD-11 (e.g. proposal #2U3N), or does not respect the principles of the classification (e.g. proposal #2S8L) (World Health Organisation, 2025i). From July 2014, when the Proposal Platform was open to the public, through July 2024, a total of 20,600 proposals were submitted. Of these, around 14,500 proposals (70.4%) have been implemented or implemented with modification (World Health Organisation, 2025h). Figure 3 displays the total number of submitted ICD-11 proposals during that period by year and proportion rejected and implemented.
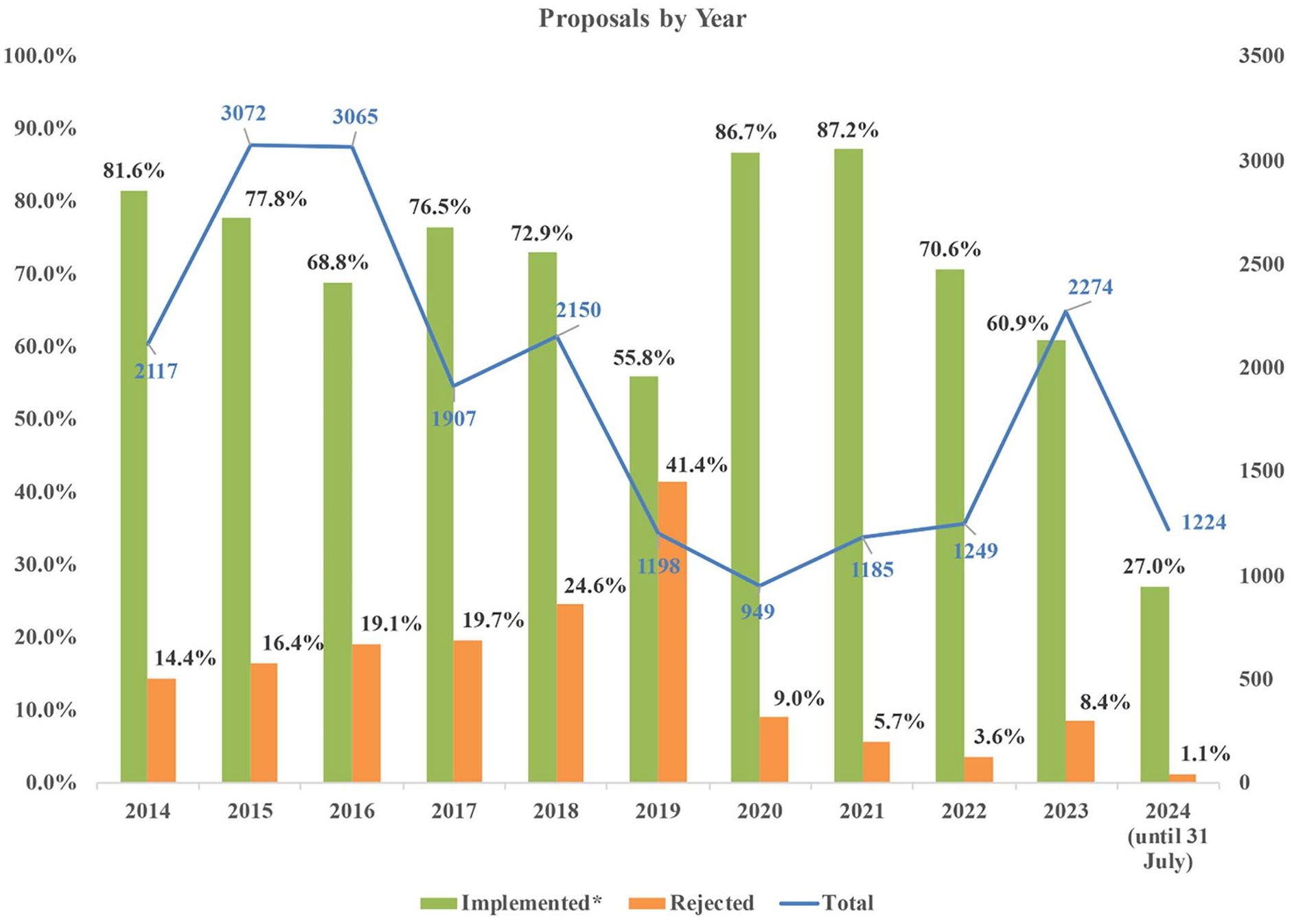
Total number of proposals by year and proportion implemented* and rejected (1 July 2014–31 July 2024).
Discussion
At the start of the 21st century, the role of digital health in enhancing health outcomes became increasingly clear. The WHO recognised that implementing digital health solutions requires resources and capabilities that may not be accessible to all countries. To foster equitable, affordable and universal access to digital health technologies, the WHO developed the global strategy on digital health 2020–2025 which “promotes the appropriate use of digital technologies as digital public goods which are adaptable to different countries and contexts to help address key health system challenges to support equity in access to digital resources so that no one is left behind”. Approved by the World Health Assembly in 2020, the strategy builds on various WHO reports and resolutions including the resolution on ICD-11 and the WHO Family of international classifications and terminologies (World Health Organisation, 2021).
ICD-11 is free to use. Its digital tools are easy to install and can be used online or offline (World Health Organisation, 2022b). The Proposal mechanism reinforces ICD-11’s status as a “global public good”. By offering a free, accessible platform to all users, the WHO ensures that ICD-11 is adaptable to the needs of various countries. This means that developing countries no longer need to rely on developed ones for modified ICD versions which require fees for licensing and updates. The authors of the proposals submitted to the WHO (July 2014–July 2024) were from 72 countries of which 40 were developing ones (UN Department of Economic and Social Affairs, 2022; World Health Organisation, 2025h).
The proposal mechanism is a major enabler of the annual ICD-11 updates. Proposals enable ICD-11 to reflect the needs of its users in real time, leading to continuous improvement of the content of the classification and minimising the need for frequent major revisions (Harrison et al., 2021). The proposal mechanism has proved to be a practical tool with ICD-11 piloting and implementation on the ground. An article published from the ICD-11 pilot in Kuwait reported that proposals were submitted to resolve issues encountered by doctors who used ICD-11 at the point of care in a public hospital. Proposals from this pilot addressed adding synonyms and abbreviations to the classification. The pilot team valued the benefits of the proposal mechanism and included an educational video on ICD-11 proposals on the Kuwait WHO-FIC CC YouTube channel (Ibrahim et al., 2022; Kuwait National Centre for Health Information, 2021). The ICD-11 pilot in China resulted in ICD-11 proposals to add new concepts to ICD-11 and improve postcoordination options. To encourage users in the country to contribute to ICD-11, the team in China developed a national platform to collect proposals from all over the country in the Chinese language. Proposals considered relevant were then translated into English and submitted to the WHO Proposal Platform (Zhang et al., 2024).
The WHO Family of International Classifications (WHO-FIC) are derived from a single Foundation and share the same digital infrastructure. This setup allows proposals to be submitted not only for ICD-11 but also for other WHO classifications namely the International Classifications of Health Interventions (ICHI) and the International Classification of Functioning (ICF), Disability and Health. Proposals can also be submitted to improve the ICD-11 Reference Guide which was developed by the WHO to aid users in understanding and using ICD-11 (World Health Organisation, 2025a, 2025c).
As described in this article, ICD-11 Proposals can be submitted by anyone, are based on selecting a specific proposal type from a predefined set of options, are fully transparent, undergo a meticulous validation workflow process, and once accepted, are reflected in all languages available on the browser. These criteria give strength to the proposal mechanism, but they are not without potential unintended consequences that should be considered. As a classification and terminology “by the people for the people,” ICD-11 proposals can be submitted by anyone. Real-life users can directly contribute to enhancing ICD content making it practical, user friendly and fit for purpose from a user’s perspective. This is particularly useful given that ICD-11 has more use cases than ICD-10 and consequently more users who may not have access to the WHO-FIC committees and reference groups that were exclusively in charge of updating the earlier ICD revisions. However, the open submission process also means that individuals without sufficient scientific background or experience with health classifications have access to the Proposal Platform potentially leading to submissions that are incorrect, unfounded or driven by cultural or personal beliefs. This is more likely to happen with conditions relating to topics that may be viewed by the public as sensitive or touch on moral or personal beliefs. For instance, several proposals related to “Gender incongruence” were submitted by the public without scientific evidence to support the proposed changes (examples: proposals #1B7W and #226N). While these proposals are rejected through WHO’s thorough review process with no impact on the classification, they still increase the workload for reviewers and WHO teams.
When submitting proposals, authors are given a choice from five predefined types, all of which pertain to the content and structure of ICD-11. However, to search this content, users rely on the ICD-11 Coding Tool, an automated search engine developed by the WHO that enables retrieval and assignment of codes (World Health Organisation, 2025a). As ICD-11 becomes more widely implemented around the world, users may encounter issues with the search results produced by the Coding Tool that are not caused by a problem with the content of the classification, but rather by an issue with how the Coding Tool functions. For instance, the Coding Tool might occasionally present non-terminal codes as destination entities, even though they are invalid for coding and reporting. Because this kind of proposal does not fit any of the five predefined proposal types, authors resort to the “propose complex hierarchical changes” option because it allows free text submission, although it is not the correct type for the proposed change (example proposals #2W1D and #2R8U). The functionality of the Coding Tool has improved over the years and these problems are becoming less frequent. Nevertheless, it’s important to provide a specific way to propose improvements to Coding Tool functionality where needed.
The proposal workflow guarantees that each proposal undergoes a thorough review process. While this is essential to maintain a robust scientifically accurate classification, it can be a lengthy process depending on the complexity or impact of the change. When a large number of proposals are submitted simultaneously or within a short timeframe (e.g. proposals generated from country evaluations of ICD-11 in preparation for implementation or from country translation workstreams), this routine workflow may be inefficient. In these cases, it may be more practical for the WHO to implement a more streamlined workflow, potentially by forming ad hoc teams to handle the volume of proposals within required deadlines.
The digital framework of the Foundation allows proposals to be linked to specific entities. While English is the authoring language, the Foundation entities themselves are language-independent, allowing accepted proposed changes for ICD-11 updates to be simultaneously implemented across different languages (World Health Organisation, 2025a). However, translators need adequate time to translate the accepted changes to the content model components on the Translations Platform before the next annual release (World Health Organisation, 2025j)
The transparency of the Proposal process builds trust in the classification and the review process. It’s a documentation of the evolution of an ICD entity over time allowing users to track how and why an entity has changed. While many developed countries are accustomed to detailed classifications, such as country-specific modifications of ICD-10, users from developing countries should be encouraged to engage with the proposal mechanism. To promote the use of the Proposal mechanism in developing countries, ICD-11 training and education should include guidance on the value and methodology of using the Proposal Platform. Among the 40 developing countries that have submitted proposals to date, 27 (67.5%) have submitted five or less proposals, compared to 8 (25%) of the 32 developed countries (UN Department of Economic and Social Affairs, 2022; World Health Organisation, 2025h).
The Proposal Platform is expected to play an increasingly vital role in supporting the development and maintenance of other WHO-FIC classifications as well. In 2020 and 2021, respectively, ICHI and ICF became accessible through the Maintenance Platform and since then, ICHI and ICF proposals, which allow improvements in user guidance and scientific updates, can also be submitted on the Proposal Platform in a similar manner to ICD proposals (World Health Organisation, 2022c, 2025k). As ICHI is now stable and is being piloted in several countries, a gradual rise in related proposals is anticipated, mirroring the pattern observed with ICD-11.
Conclusion
The improvement in ICD-11 content, facilitated by the ICD-11 Proposal mechanism, has the potential to satisfy users from different countries, enhancing the classification in ways that reduce any need for country-specific modifications ultimately improving the comparability of clinical data at the international level. ICD-11 stands out as a classification and terminology for the 21st century, evident through its transparent review process which is open and accessible to everyone. ICD-11 is truly “for the people, by the people” as a global language that ensures data comparability and interoperability in digital and analogue health information systems.
Footnotes
Acknowledgements
The authors acknowledge the contributions of individuals and institutions worldwide who have submitted proposals to the WHO’s open online Proposal Platform, thereby contributing to the content of ICD-11.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This article describes a public, online platform and does not involve human participants, personal data or interventions. Therefore, ethical approval and informed consent were not required.