
Abstract
Background:
Existing research has long established that direct exposure to patient trauma, such as severe injuries, chronic illnesses and end-of-life care, places clinical healthcare workers at heightened risk of secondary traumatic stress, compassion fatigue and burnout. However, comparatively little attention has been paid to the impact on non-clinical healthcare personnel, such as health information managers (HIMs) who, despite being removed from direct patient care, regularly handle distressing and sensitive patient information.
Objective:
This scoping review explores the literature concerning non-clinical healthcare professionals and the potential impact upon their biopsychosocial–spiritual (BPSS) well-being given prolonged exposure to medical and/or patient records.
Method:
Arksey and O’Malley’s five-stage scoping review strategy was utilised. An initial search of the literature yielded no results specific to HIMs and other non-clinical healthcare professionals. Therefore, the scope of the review was broadened, and a second search of the literature was conducted to explore comparable non-patient/client-facing populations such as transcriptionists.
Results:
In total 1226 articles were initially identified and 13 articles revealed either a biological, psychological, social and/or spiritual impact when professionals were exposed to traumatic and/or sensitive data.
Conclusion:
Exploring the roles of comparable non-patient/client-facing populations provides insight into the potential impact that exposure to traumatic and/or sensitive information may have on the health and well-being of HIMs and other non-clinical health professionals.
Implications for health information management practice:
Further research is recommended to explore the potential BPSS impact that HIMs and other non-clinical health professionals experience due to the exposure of traumatic and/or sensitive information.
Keywords
Introduction
Clinical healthcare workers (e.g. doctors, nurses, paramedics) are directly and regularly exposed to patient trauma. This exposure has been associated with negative physical, psychological and emotional effects (Beck, 2011), including the development of secondary traumatic stress, compassion fatigue, moral injury and burnout (Čartolovni et al., 2021; Granek et al., 2016; Ogińska-Bulik et al., 2021; Roche et al., 2022; West et al., 2018; Zheng et al., 2017). Despite the breadth of research examining the negative impacts in clinical settings (Samson and Shvartzman, 2017; Sorensen and Iedema, 2009; Wilson and Kirshbaum, 2011), clinical professionals are not the only healthcare workers exposed to traumatic and sensitive information. Health information managers (HIMs) and clinical coders (CCs) are responsible for collecting, organising, coding and maintaining medical records (Health Information Management Association of Australia, 2025). Unlike clinicians, whose roles typically include direct patient care and structured emotional support processes (Shapiro and Galowitz, 2016), HIMs and CCs are often distanced from patient interaction, instead working in a non-clinical capacity that supports healthcare delivery. Nevertheless, HIMs and CCs are still regularly exposed to traumatic and sensitive patient information, and this exposure may reasonably lead to potential negative impacts, such as secondary traumatic stress or compassion fatigue (Bride, 2007).
Defining “sensitive information”
In the Australian healthcare setting, the term sensitive information is often used to describe personal data protected by national legislation (Australian Government, 1988) along with various state-based health record laws. However, Lee (1993) notes that sensitivity extends beyond privacy and confidentiality concerns. Medical documentation may also be inherently sensitive due to the type and severity of information contained within the health record itself. It is the exposure to the content of sensitive data that is the focus of this review – particularly exposure to patient narratives and outcomes that may potentially impact the well-being of HIMs and other non-clinical healthcare professionals.
Biopsychosocial–spiritual model
A framework for understanding the potential impacts of sensitive data exposure is provided by the biopsychosocial (BPS) and biopsychosocial–spiritual (BPSS) models, which offer a holistic lens for examining the multifaceted effects on individual health and well-being. Introduced by Engel (1977), the BPS model challenged the purely biomedical perspective of health by acknowledging the interconnectedness of physical health (bio), cognitive and emotional factors (psycho) and sociocultural (social) influences. Each domain is considered equally significant in influencing health and well-being, with biological determinants often having psychosocial consequences and vice versa (Engel, 1977; McDaniel, 1995). For example, an individual experiencing sadness – a psychological or emotional response – may cry, reflecting a biological or physical manifestation. This illustrates the intrinsic interconnections between the domains, where a change in one (e.g. emotional) can precipitate outcomes in another (e.g. physical). Over two decades since Engel, the World Health Organization formally endorsed the BPS model in 2001 (World Health Organization, 2001).
Sulmasy (2002) further expanded this model by formally incorporating spirituality as a critical component of health, particularly in the care of patients at the end of life. Sulmasy (2002) acknowledged spirituality as an essential dimension contributing to inner peace, hope and purpose. For the purposes of this research, Sulmasy’s (2002) contemporary BPSS model has been utilised as a “frame of reference” to explore the different biological, psychological, social and spiritual impacts that may result from exposure to medical and/or patient records, upon HIMs and non-clinical healthcare professionals. An adapted form of Sulmasy’s (2002, p. 27) definition of BPSS has been utilised to explore the potential BPSS vicarious trauma that may affect these professions: Biopsychosocial-spiritual trauma is any impact as a result of a biological, psychological, social and/or spiritual event, whether it be a direct or indirect encounter, written or oral narrative, which impacts the health and well-being of an individual, community and/or or association of people.
While the BPS model is a validated model, the BPSS model has not yet been formally validated. Nevertheless, as an extension of the BPS model, the BPSS model has now largely been accepted as the more refined paradigm based upon surmounting evidence of spirituality and religion being influential health determinants (e.g. Cobb et al., 2012; Koenig et al., 2024), especially with regard to chronic conditions (e.g. Anim et al., 2022; Elias et al., 2015; Klawonn et al., 2019; Matteliano et al., 2014; Van Denend et al., 2022; Zegarra-Parodi et al., 2019). Thus, over recent years, the BPSS model has been used as a review framework (e.g. Miller et al., 2023; Umberger and Wilson, 2024) and likewise will be utilised as a frame of reference within the current study.
Spirituality – morals and ethics
While it is argued that spirituality extends beyond traditional religious concepts (Puchalski et al., 2014; Sulmasy, 2002), nevertheless there are integral components that overlap between spirituality and religion. Both consider moral behaviour and ethical decision-making about how one should act in the world and relate to others (Koenig, 2012). In understanding the BPSS impact upon HIMs and non-clinical healthcare professionals, ethical and moral issues are included in the spirituality domain, as these represent an individual’s personal engagement in the workplace with various bioethical principles (e.g. autonomy, beneficence, non-maleficence, justice, confidentiality; Carey and Cohen, 2015).
Aim
This scoping review was guided by the following research question: What are the BPSS impacts that HIMs and non-clinical health professionals experience when exposed to the content within medical and/or patient records? The primary objectives of this study comprised:
Investigating if there was any evidence of physical, psychological, social and/or spiritual impacts affecting the health and well-being of HIMs and non-clinical health professionals due to exposure to medical and/or patient records.
Determining whether the duration of occupational exposure to medical and/or patient records influences the physical, psychological, social and/or spiritual health and well-being among HIMs and non-clinical health professionals.
Identifying any educational strategies/training and/or resources located in the literature, that have been, or should be developed, to assist HIMs and non-clinical health professionals’ occupational health and safety with regards to the potential impact of exposure to medical and/or patient records.
Methods
Study design
A scoping review was conducted drawing upon the five-stage framework as constructed by Arksey and O’Malley (2005) and further informed by best practice guidelines from the Joanna Briggs Institute evidence synthesis methodology (Peters et al., 2020) and PRISMA Extension for Scoping Reviews checklist (Tricco et al., 2018). Unlike other forms of literature reviews such as systematic reviews or meta-analyses, the scoping review’s main goal is to identify gaps in the current body of literature, particularly in areas where limited or no prior research exists (Arksey and O’Malley, 2005).
Search strategy 1
To address the objectives, a modified population, exposure, comparison and outcomes (PECO) search strategy was utilised (Morgan et al., 2018; see Box 1). During January 2024, articles were sourced from the Medline/Ovid, CINAHL, Embase ProQuest Central, Cochrane Library, PsycINFO and SCOPUS electronic databases. Both keywords and controlled vocabulary terms (e.g. MeSH headings) were included in the search. Google Scholar was also utilised; however, due to the high number of hits, only the first 200 entries were considered. Although discipline-specific grey literature searches were planned, access to non-peer-reviewed discipline publications such as HIM-Interchange and the Journal of AHIMA was, at the time of the review, restricted due to subscription barriers. As a result, grey literature was omitted from this search. Despite a comprehensive exploration using the search strategy, no results were found.
Search strategy 1, key search terms.
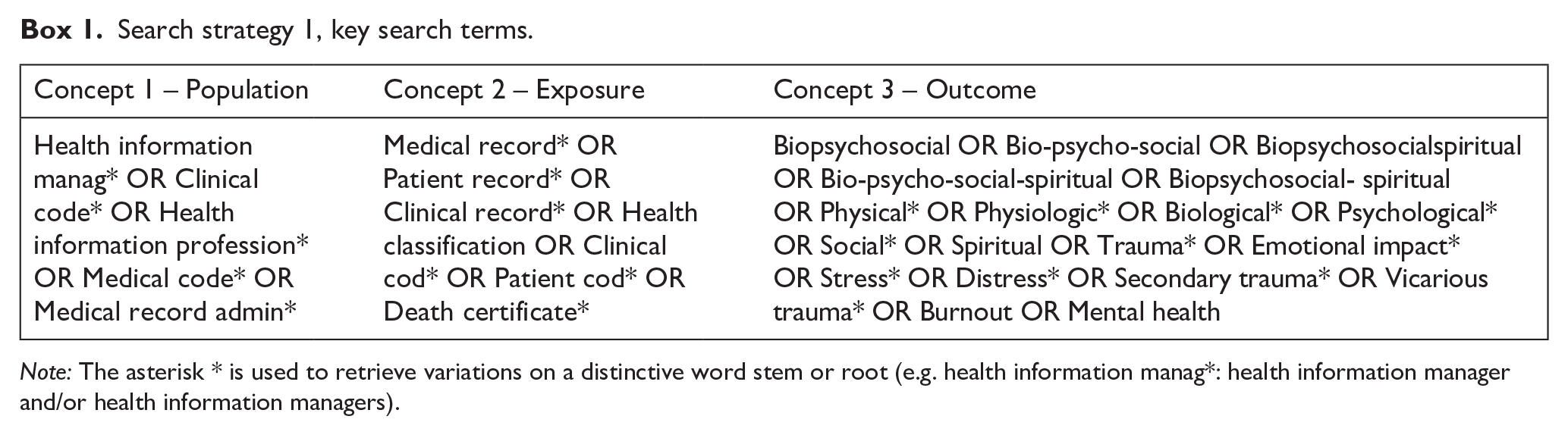
Note: The asterisk * is used to retrieve variations on a distinctive word stem or root (e.g. health information manag*: health information manager and/or health information managers).
Search strategy 2
Following the advice from a specialist librarian, and recognising the limited publications related to this topic within the health information management profession (Robinson et al., 2021), the search was expanded and replicated to include other similar non-patient/client-facing populations, including qualitative researchers, transcriptionists and administrators (Box 2). The revised populations are themselves often removed from their data source, and at times have no contact with the individual from which those data were obtained, similar to that of HIMs and non-clinical health professionals. As a result of the change in population, the exposure was broadened to include terms such as “sensitive data” and “sensitive research” to account for other types of information.
Search strategy 2, key search terms.
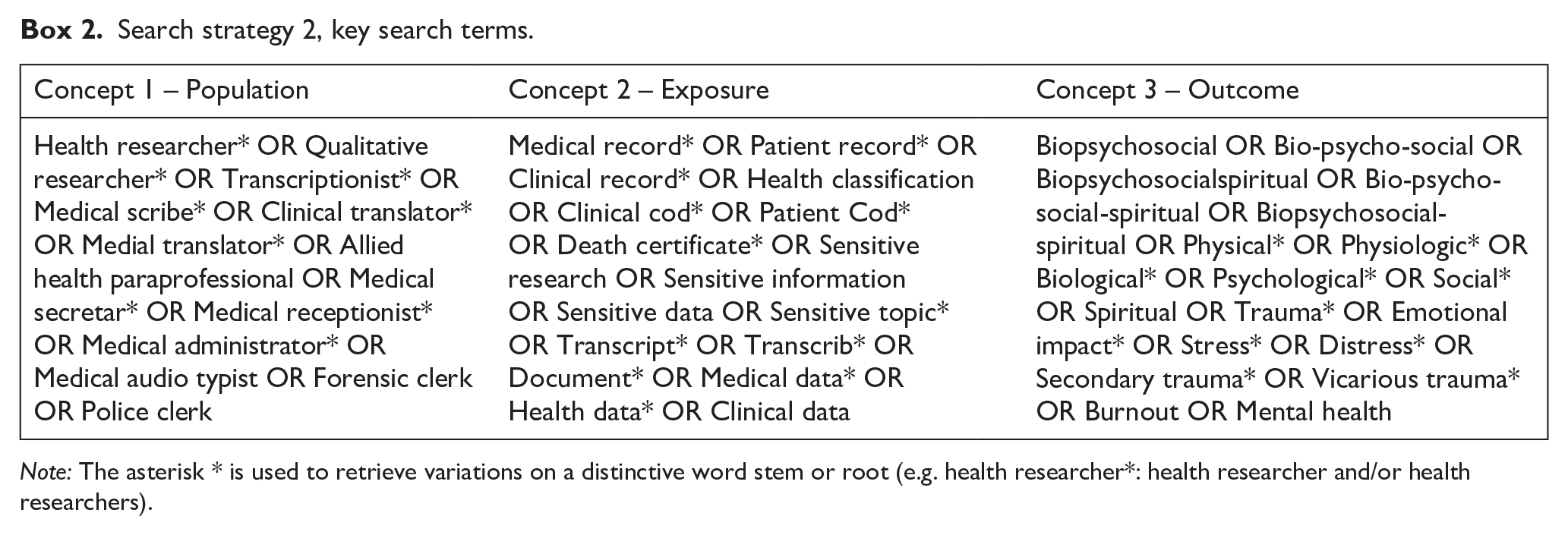
Note: The asterisk * is used to retrieve variations on a distinctive word stem or root (e.g. health researcher*: health researcher and/or health researchers).
Inclusion and exclusion criteria
The inclusion and exclusion criteria for both search strategies targeted articles published between 2000 and 2023 to capture contemporary studies. Only peer-reviewed and professional journal articles written in English were considered. Studies involving non-clinical health professionals, rather than those focused on patient-facing roles, were included.
Eligibility screening
All screening was conducted using Covidence Systematic Review Software (2024). Records were initially screened by title and abstract by two reviewers (MT and LBC), and conflicts were resolved by a third reviewer (MR). All records not excluded were passed on for full-text review. Two reviewers (MT and LBC) independently reviewed full-text records for potentially eligible studies, and any disagreements were resolved by a third reviewer (MR). Records deemed ineligible at full-text screening were excluded with the reason recorded.
Qualitative data extraction
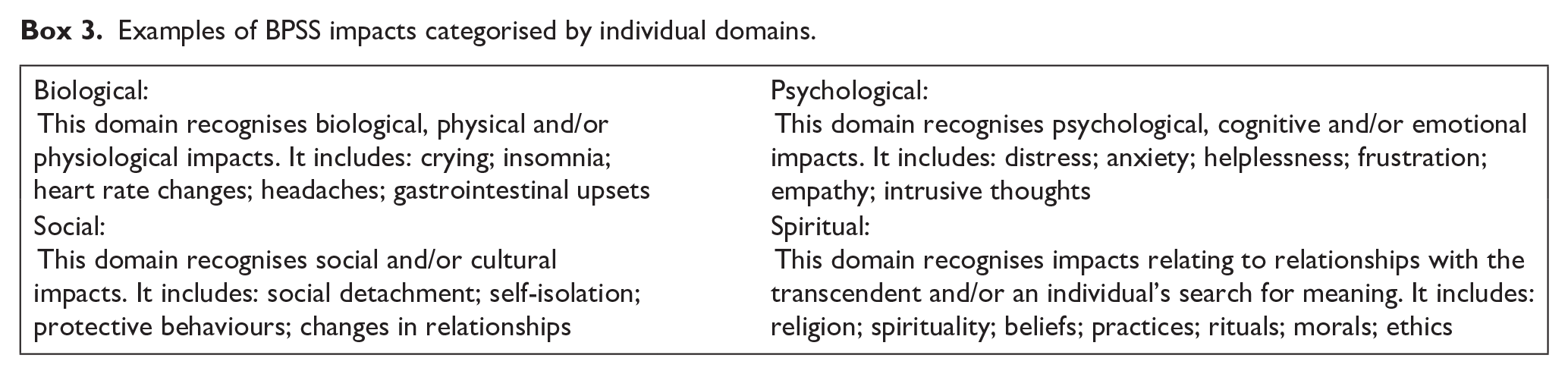
Following full-text review, initial data extraction was undertaken by one reviewer (MT). Thematic analysis was used to identify and systematically organise the various impacts experienced by individuals when exposed to traumatic and/or sensitive data. These impacts were then categorised into one of the BPSS domains (Box 3) for further analysis. Where the reviewer (MT) was unsure of categorisation, a second reviewer (LBC) provided advice. The final categorisation of impacts into the BPSS domains was agreed upon by two reviewers (MT and LBC). The following bibliometric and research details were extracted from all eligible studies, namely: study identification number; title; name of lead author; contact details of lead author; (first) year of publication (online or journal issue); title of journal; data source (state and/or country); study aims; study setting; study design; study time period; study participants (including occupation); sample size; data exposure type; length of exposure; biological domain impacts; psychological domain impacts; social domain impacts; spiritual domain impacts; participant education and/or training; participant support provision and limitations. As this is a scoping review, no quality assessment was performed.
Examples of BPSS impacts categorised by individual domains.
Results
Selection of articles
Search strategy 1 yielded a total of 1660 articles. After screening, 1376 abstracts were reviewed and 65 full-text articles were assessed for eligibility. No articles met the inclusion criteria and were considered irrelevant to the subject matter. To broaden the scope, a second search strategy was engaged to include other populations (occupational groups) not directly involved in patient/client-facing roles. Search strategy 2 yielded a total of 1226 articles for title and abstract screening and an additional six articles were identified through the manual review of eligible articles. This search identified 13 academic papers suitable for inclusion, each recognising at least one or more biological, psychological, social and/or spiritual impacts on individuals exposed to traumatic and sensitive data (Figure 1).
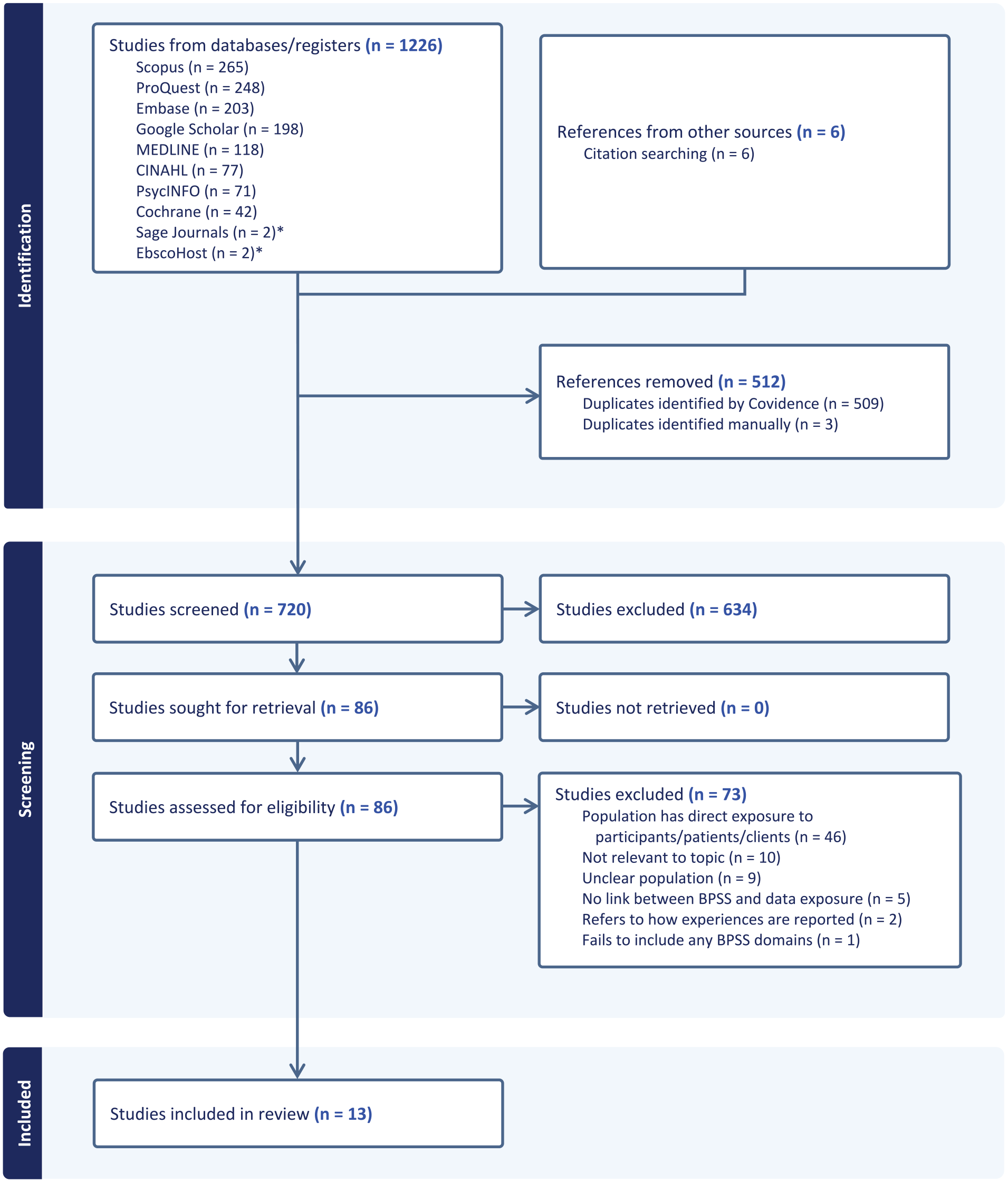
PRISMA flow diagram of the screening process for Search Strategy 2 (Covidence generated, Veritas Health Innovation).
Study characteristics
Table 1 summarises the key characteristics of the studies included in the review. Approximately 62% (n = 8/13) of the articles were published after 2013 and ~46% (n = 6/13) were undertaken in the United Kingdom. The articles used qualitative research methodologies and study designs including a narrative review, case studies and in-depth interviews. The populations studied were diverse, comprising qualitative researchers, transcriptionists, research assistants, research supervisors and postgraduate students. A common exposure type across many studies was the handling of trauma-related data, including audio files from trauma research interviews and written records such as autopsy reports, and clinical notes on self-harm and suicide attempts. Other exposure types included complaints of hate violence, fieldwork notes on foetal abnormalities and accounts of survivors who experienced childhood sexual abuse.
Sample characteristics of articles included in the review (n = 13).
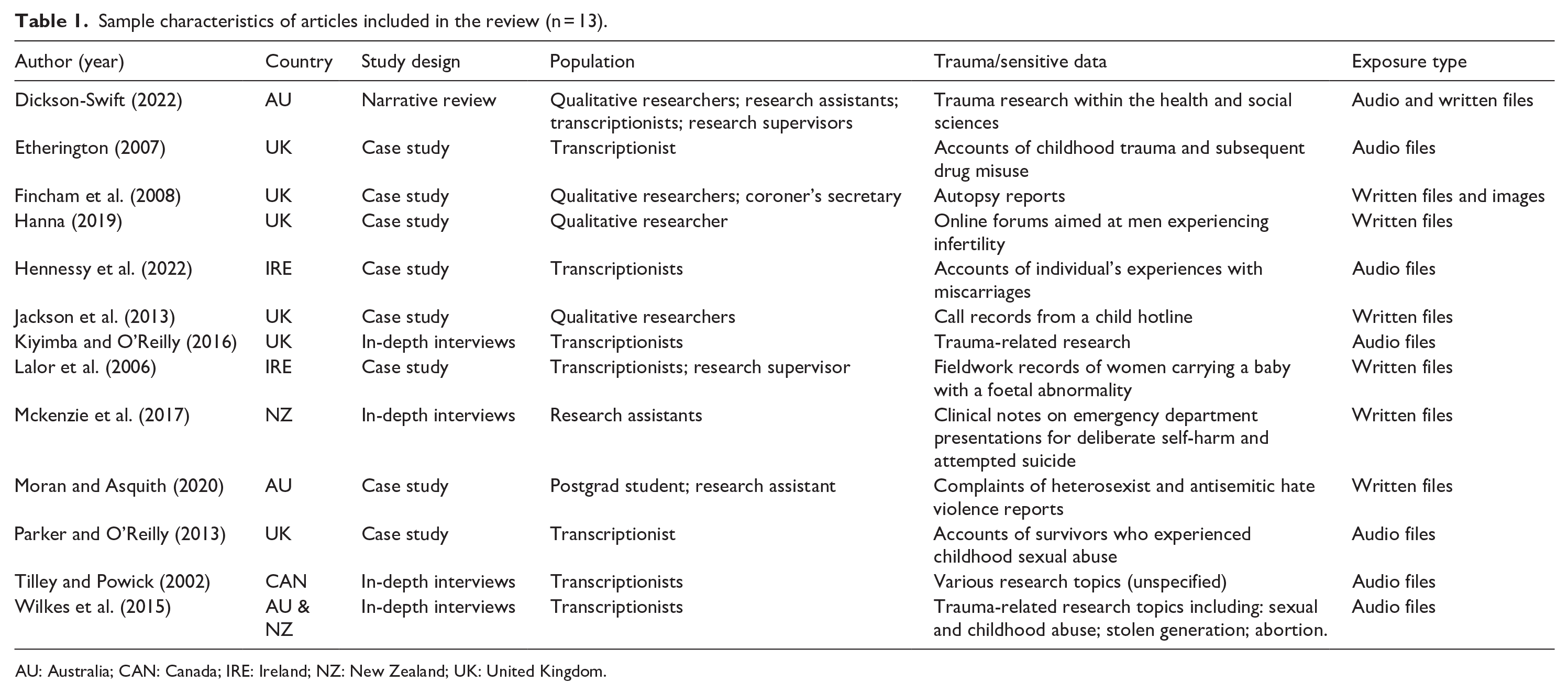
AU: Australia; CAN: Canada; IRE: Ireland; NZ: New Zealand; UK: United Kingdom.
BPSS impact
Table 2 provides a summary of the BPSS domains which impacted participants in each of the studies.
Summary of BPSS domains identified in each study (n = 13).
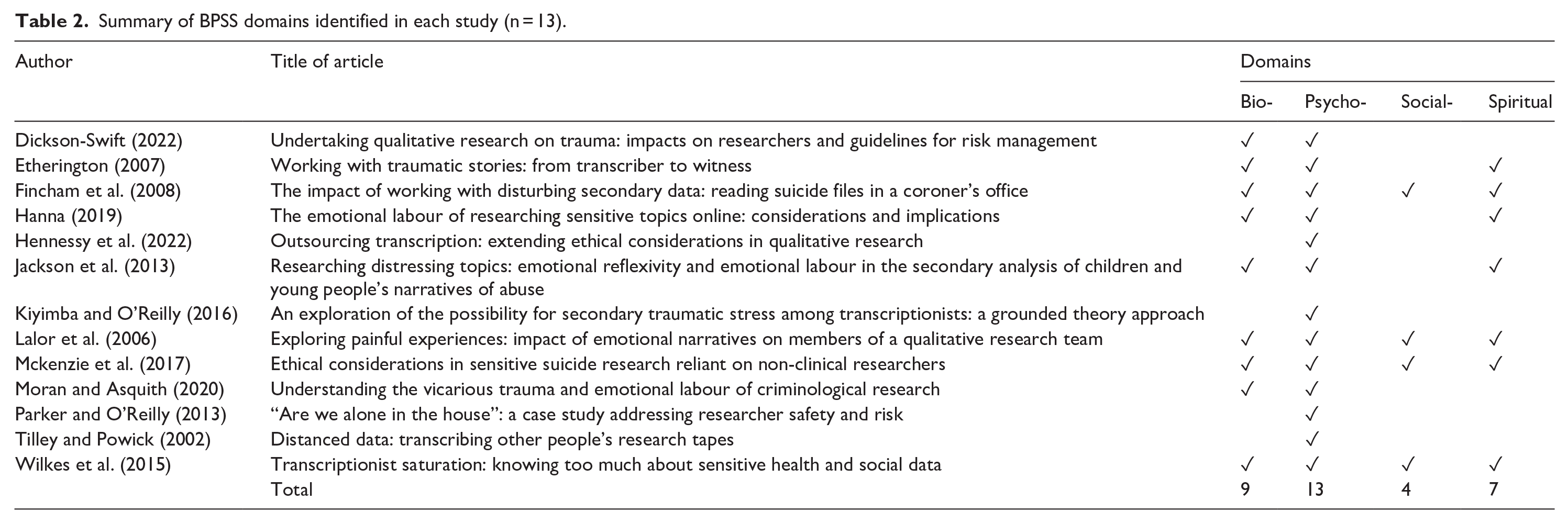
Biological
Of the 13 articles, 9 (69.2%) reported significant physical consequences affecting individuals involved in transcription and exposure to traumatic and sensitive data. For example, Etherington (2007) and Fincham et al. (2008) both noted disturbed sleep as an effect. Fincham et al. (2008) also observed nervous laughter and heavy sighing as physical signs of stress. Physical responses such as crying and or being brought to tears were identified by Jackson et al. (2013), Lalor et al. (2006) and Wilkes et al. (2015), where for example, a participant described an overwhelming moment stating, “In fact, I had to wander off, sit in a corner and cry” (Wilkes et al., 2015).
Hanna (2019) captured a different type of physical response, recounting a moment of excitement: “I shouted ‘Yes!’ out loud, at my desk – I was visibly moved for him,” after reading the positive news of a couple expecting twins. Moran and Asquith (2020) described a pattern of avoidance and physical reluctance, stating, “We procrastinate, and when forced to return to the task, we flinch away from the computer screen.” Mckenzie et al. (2017) echoed this noting that on some days “you can’t look.” Supporting these findings, Dickson-Swift (2022) identified similar physical effects including sleeplessness, vomiting, headaches and gastrointestinal upsets, further reinforcing the impact of working with sensitive information.
Psychological
All of the included articles (n = 13; 100%) identified one or more psychological impacts on individuals engaging with sensitive data. A common impact across the studies was the experience of distress, anxiety and emotional burden, with several authors noting that participants struggled to “switch off” after repeatedly being exposed to traumatic or deeply personal narratives (Hennessy et al., 2022; Moran and Asquith, 2020). Descriptors such as upsetting, deep emotional impact and distressing emerged frequently (Fincham et al., 2008; Lalor et al., 2006; Mckenzie et al., 2017), while several researchers noted more specific reactions like helplessness (Hanna, 2019; Parker and O’Reilly, 2013), anger (Dickson-Swift, 2022; Jackson et al., 2013) and frustration about not knowing the “end of the story” (Hanna, 2019; Kiyimba and O’Reilly, 2016). Jackson et al. (2013) and Mckenzie et al. (2017) both reported challenging visual disturbances, such as imagining traumatic events and visualising scenes from the research material. In addition, Jackson et al. (2013) highlighted auditory disturbances, including hearing voices after reading about traumatic cases. These negative emotions sometimes gave rise to intrusive or lingering thoughts, with some participants describing difficulty forgetting the material, visualising the trauma in vivid detail or continuing to hear the voices they had transcribed long after the project ended (Jackson et al., 2013; Mckenzie et al., 2017).
Several studies highlighted how these psychological impacts could accumulate over time, resulting in what was variously referred to as vicarious trauma, secondary traumatic stress or pain by proxy (Fincham et al., 2008; Jackson et al., 2013; Kiyimba and O’Reilly, 2016). Procrastination, avoidance behaviours and delayed engagement with the data were reported as attempts to cope with or postpone distress (Moran and Asquith, 2020). While some participants “got used to it” or described becoming desensitised over repeated exposures (Fincham et al., 2008; Mckenzie et al., 2017), others found that prolonged contact made them increasingly vulnerable to anxiety, burnout or exhaustion (Dickson-Swift, 2022; Wilkes et al., 2015). Personal circumstances also played a role in shaping responses: individuals who had endured similar life experiences, such as miscarriages or having children, reported intensified reactions to data concerning those same issues (Lalor et al., 2006; Wilkes et al., 2015).
Alongside these impacts, two studies (15.4%) also illustrated positive or more nuanced emotional responses. Etherington (2007) and Hanna (2019) both acknowledged moments of hope, empathy and even excitement or relief when reading about participants’ resilience or positive outcomes. While reflecting on stories of individuals who overcame adversity, some participants felt uplifted or inspired; thus, perceiving a sense of personal growth and validation that the insights gained outweighed their temporary distress (Etherington, 2007). Similarly, Hanna (2019) recounted instances where researchers expressed genuine joy and relief on learning that a difficult situation was resolved positively.
Evidence of a psychological toll to the exposure of sensitive data indicated that some participants frequently sought closure, either by finishing an entire transcript or receiving follow-up information about the outcome of a case (Hanna, 2019; Kiyimba and O’Reilly, 2016). Where closure was unavailable, a lingering sense of incompleteness contributed to individual’s ongoing worry, stress and mental preoccupation (Kiyimba and O’Reilly, 2016; Moran and Asquith, 2020).
Social
Of the 13 included articles, 4 (30.8%) identified notable social impacts resulting from exposure to traumatic and sensitive data. The most frequently reported social impact was withdrawal or diminished interpersonal engagement, particularly among family relationships. Wilkes et al. (2015) described how participants experienced “isolation from family,” became “monosyllabic in conversation,” and in some cases, “not being able to make eye contact,” indicating a disconnection from social interactions as a coping mechanism. Mckenzie et al. (2017) similarly noted how participants engaged in “limiting exposure to trauma events,” actively avoiding discussing or engaging with traumatic topics in social contexts. In contrast, Lalor et al. (2006) reported positive shifts in social relationships among some participants. Some transcribers noted “spending more time with family” and “appreciating their own children” after exposure to sensitive narratives, suggesting that such work, while distressing, could also encourage deeper familial connections and gratitude. Indeed, Fincham et al. (2008) described a pattern, where some participants expressed a “desire to talk and retell stories to family and friends.”
Spiritual
Of the 13 included articles, 7 (53.9%) identified spiritual impacts experienced by individuals engaged with traumatic and sensitive data, with reference to religious acknowledgements, existential reflections and shifts in attitudes and beliefs. Lalor et al. (2006) documented significant spiritual impacts, particularly among transcribers who conveyed a “change in attitude and gaining insight” from working with sensitive narratives. Some transcribers reported a sense of “privilege” in bearing witness to participants’ stories, while others described feeling “vicariously responsible for participants’ well-being” and expressed praise to God for their own good fortune. Similarly, Fincham et al. (2008) identified how engaging with distressing narratives led some researchers to become “more alert about their own mortality, and that of their loved ones,” reflecting a profound existential impact and heightened awareness of life’s fragility.
Spiritual themes of moral conflict and ethical dilemmas were also evident in several studies. Jackson et al. (2013) described “emotive dissonance between personal moral and ethical ideology” and the professional demands upon individuals in the analytics of the data. Similarly, Etherington (2007) highlighted “changed attitudes and beliefs about drug misusers,” indicating that exposure to traumatic narratives can prompt personal reflection and shifts in deeply held values. Hanna (2019) echoed this moral tension, describing how some individuals felt compelled to help vulnerable participants, stating they felt a “wanting to do more” for the men on an online forum but were ethically constrained from further involvement. Some studies also described protective or growth-oriented spiritual responses. Mckenzie et al. (2017) reported that participants became “more vigilant about safety” and developed a “recognition of the fragility of life” after working with traumatic data. Wilkes et al. (2015) described positive transformations, with some participants feeling like they were “making a positive impact,” as well as reporting a shift towards being “less judgemental and appreciating their own lives.”
Overall, among the 13 articles, 5 studies (e.g. Etherington, 2007; Fincham et al., 2008; Lalor et al., 2006; Mckenzie et al., 2017; Wilkes et al., 2015) included passages that could be recognised as spiritually salient. Whether explicitly invoked as religious language (“thanking God”) or more broadly situated in existential reflection (“recognising the fragility of life”), these findings illustrate how working with traumatic and sensitive data may prompt or intensify spiritual/meaning-making processes.
Duration of exposure
Of the 13 included articles, only 5 (38.5%) referred to the length of exposure to traumatic and/or sensitive data. However, these references lacked clear definitions of specific timeframes and were not based on empirical data, relying instead on anecdotal and experiential accounts. Fincham et al. (2008) and Mckenzie et al. (2016) both referred to the time spent conducting research. Fincham et al. (2008) described “prolonged exposure” to suicide files in a coroner’s office as an inherent aspect of the qualitative research process. Similarly, Mckenzie et al. (2016) emphasised the ethical complexities and psychological risks associated with sustained engagement in sensitive suicide research, though they did not specify exposure duration. Jackson et al. (2013) and Moran and Asquith (2020) highlighted the potential impact of analysing large volumes of distressing records over “prolonged periods of time,” though again, neither study identified specific timeframes. Hennessy et al. (2022) provided a more defined context, describing the transcription of audio files from June 2020 to February 2021.
Education and training strategies and support
The third objective of this scoping review was to determine whether the literature indicated if any educational strategies or support had been, or should be, developed to assist occupational health and safety training for non-clinical staff exposed to traumatic and/or sensitive data. Of the 13 included articles, only 5 (38.5%) explicitly discussed formal education or training designed to mitigate potential secondary trauma. Instead, most articles (n = 8/13; 62.5%) focused on informal or ad hoc measures, such as being forewarned about distressing material or developing personal coping strategies.
Type of training
When detailed, training varied considerably. Some qualitative researchers and transcribers had no formal clinical training that prepared them to listen to traumatic stories “over and over again” (Etherington, 2007). Others had no training when working with sensitive data recounting self-harm and suicide attempts (Mckenzie et al., 2017). Lalor et al. (2006) did not specify a formal training curriculum, however, recommended advance warning about sensitive content. Fincham et al. (2008) and Parker and O’Reilly (2013) highlighted the need to prepare researchers for the potential emotional toll inherent in dealing with highly sensitive material, although neither study provided a structured training framework.
Support strategies
Across all 13 articles, the most commonly identified support mechanisms (n = 12/13; 92.2%) were debriefing, either with peers or supervisory teams, and informal discussions that provided emotional offloading. Hanna (2019), Moran and Asquith (2020) and Wilkes et al. (2015) echoed these findings, emphasising how sharing experiences in a supportive environment helped to normalise emotional reactions and contributed to mitigating adverse emotional effects (Dickson-Swift, 2022; Hennessy et al., 2022). Dickson-Swift (2022) extended this view by recommending formal counselling and warning that inadequate debriefing or training heightened emotional risk. Self-care tactics also featured prominently, as noted by Jackson et al. (2013), Kiyimba and O’Reilly (2016) and Mckenzie et al. (2017), which included physical breaks, rationalising distress and identifying personal limits to safeguard emotional well-being. Hennessy et al. (2022) likewise highlighted the value of ongoing communication, noting that routine check-ins between professional transcribers served as a protective factor against vicarious trauma.
Discussion
This research explored the available literature in relation to the potential BPSS impact upon HIMs and other non-clinical healthcare professionals due to their exposure to the content within medical and/or patient records. While the initial scoping revealed no data specific to HIMs, CCs and other non-clinical healthcare professionals, the eligible studies of similar occupational groups (e.g. transcriptionists, qualitative researchers) consistently illustrated that engagement with traumatic and/or sensitive data could result in biological, psychological, social and/or spiritual impacts.
BPSS framework
The biological domain revealed a number of acute and potentially chronic impacts that could affect HIMs, CCs and other non-clinical healthcare professionals. Among the breadth of studies, however, psychological impacts (ranging from deeply negative to more affirming and transformative experiences) were identified across all 13 articles, highlighting the prominence of psychological effects due to working with traumatic and/or sensitive data. Social impacts (both negative and positive) were also noted within the literature impacting interpersonal relationships with family and friends – though this domain had the lowest reported data across the literature.
Though fewer studies reported spiritual impacts compared with psychological or biological symptoms, the potential for moral or existential conflict emerged as a notable theme in over half of the included articles. Spiritual responses ranged from heightened gratitude and moral introspection to more distressing experiences, such as feelings of moral injury. Indeed, some accounts suggested that unresolved ethical dilemmas can lead to depression, social withdrawal, or more severe outcomes, such as a moral injury or self-harm (Hodgson and Carey, 2017). These findings reinforce the BPSS model’s holistic affirmation that spirituality, or broader existential reflection, can both exacerbate trauma and/or provide a pathway toward personal growth and meaning-making in professional contexts. Though fewer studies reported spiritual impacts compared with psychological or biological symptoms, the potential for moral or existential conflict emerged as a notable theme in over half of the included articles. These findings reinforce the BPSS model’s holistic affirmation that spirituality, or broader existential reflection, can both exacerbate trauma and/or provide a pathway toward personal growth and meaning-making in professional contexts.
Exposure duration
This review found insufficient empirical evidence regarding the length of exposure in relation to individuals experiencing BPSS impacts. Within this study, the majority of articles did not specifically address exposure, while the remaining studies only offered anecdotal or experiential accounts. Some research suggests that age and experience influence the susceptibility to secondary trauma, with younger, less experienced professionals at higher risk of developing secondary traumatic stress symptoms (Beck, 2011; Cieslak et al., 2014; Craig and Sprang, 2010; Hensel et al., 2015; Hinderer et al., 2014). Findings also indicate that extensive exposure to trauma can, in some cases, promote resilience and coping mechanisms among highly experienced practitioners (Cohen and Collens, 2013; Hernández et al., 2007; West et al., 2018). However, the literature cannot draw solid conclusions regarding the duration of exposure and development of secondary trauma, due to the number of confounders affecting an individual’s risk of workplace burnout (Ogińska-Bulik et al., 2021; Velasco et al., 2023). Nevertheless, it is clear there is a critical gap in the literature with regards to HIMs, CCs and non-clinical health professionals, which warrants the need for future studies to investigate whether prolonged exposure to traumatic and/or sensitive data impacts the development of vicarious trauma symptoms. Establishing the potential threshold at which exposure duration becomes problematic, could inform risk mitigation strategies and targeted interventions.
Education, training and support
This review did not identify any unified educational strategies or formal training aimed at protecting non-clinical staff from the BPSS impacts of exposure to distressing content, possibly due to the diversity of occupations included. However, debriefing was identified across the professions as the most utilised support mechanism. The included studies collectively highlighted several strategies that could serve as a framework for effective education and training interventions, as well as strategies that can be employed to support employee health and well-being. For example: content forewarnings, structured debriefing and self-care tactics. It should be noted that these recommendations remain largely anecdotal, lacking consistent evaluation or robust empirical support. As HIMs, CCs and other non-clinical healthcare professionals are often involved in processing large volumes of traumatic and/or sensitive patient data, opportunities for formal education and training programs should be researched, implemented and evaluated.
Additionally, established strategies from clinical healthcare contexts, where professionals routinely encounter patient trauma, offer valuable insights that could inform training and support initiatives for non-clinical staff. In clinical settings, structured interventions – such as resilience-building programs, formal debriefing sessions and peer support networks – have been shown to mitigate secondary traumatic stress, compassion fatigue and burnout among nurses, physicians and other frontline providers (Beck, 2011; Shapiro and Galowitz, 2016). Adapting these models for non-clinical health professionals – by incorporating education on recognising signs of emotional distress, providing regular debriefing opportunities and facilitating supervised or peer-led support – may similarly foster psychological well-being in those who interact with distressing patient data. While this scoping review identified limited instances of formalised training for non-clinical roles, the success of structured interventions in clinical domains underlines their potential applicability and efficacy in preventing and managing adverse outcomes in non-clinical healthcare settings. Future research should further explore how these established training frameworks might be tailored to the unique responsibilities of non-clinical staff, with particular attention to practical implementation and long-term sustainability.
Implications for health information management practice
Given that HIMs, CCs and other non-clinical workers routinely engage with large amounts of traumatic and/or sensitive data, the absence of health information management-specific research on BPSS impacts represents an important gap in the literature. The evidence from comparable occupations suggests that HIMs may be similarly vulnerable to BPSS impacts. Further research gathering evidence-based data specifically from practicing HIMs is required to bridge this gap and identify key themes related to this workforce group.
These preliminary findings also highlight the necessity for future research to identify education and training opportunities that should be provided to HIMs and other non-clinical health professionals based on specific findings captured from the health information management workforce. If necessary, comprehensive training programs that address the distinct needs of these non-clinical professionals who regularly are exposed to sensitive information should be developed and evaluated. Without these, there remains a risk that ongoing exposure to distressing material could result in negative outcomes for HIMs, CCs and other non-clinical healthcare professionals.
Limitations
This study was limited by a number of factors. While seven major databases were searched, these did not include these databases (e.g. Open Access Theses and Dissertations, ProQuest Dissertations and Theses Global). Also, an extensive search of the grey literature was not possible during the time of the literature search, due to subscription constraints. Nonetheless, after completing the scoping review, one piece of relevant grey literature (Best, 2017) became accessible via the HIM-Interchange professional practice journal. Best’s (2017) commentary highlights the current findings that it is “unrealistic to suggest that as individuals they [clinical coders] would be completely immune to the effects that [reading] this [traumatic and sensitive patient information] may have on their emotional wellbeing” (p. 31). This commentary, while outside the included literature, highlights a similar issue presented with this review. Another limitation is that the findings presented are categorised into distinct BPSS domains to assist with systematic analysis. It can, however, be challenging to categorise experiences into just one domain without recognising how each domain overlaps and interacts (Sulmasy, 2002). An individual who develops insomnia (a biological symptom) due to anxiety (a psychological symptom) may also withdraw from family and friends (a social response), as well as ritual activities (a spiritual response). Future research should therefore involve rigorous analysis utilising analytical measures that are inclusive of the multifaceted nature of BPSS impacts and the fluidity between these domains. A further limitation to consider concerns spiritual impacts. While fewer studies reported spiritual impacts compared with psychological or biological symptoms, nevertheless the potential for moral or existential conflict emerged as a theme in over half of the included articles. Indeed, some accounts suggested that unresolved ethical dilemmas can lead to depression, social withdrawal, or more severe moral, religious or spiritual problems – recently identified as “potential moral injurious experiences” (Hodgson and Carey, 2017; Koenig and Al Zaben, 2021). This an area that requires future exploration with regard to non-clinical health professionals.
Conclusion
While the literature on the direct examination of BPSS impact on HIMs remains scarce, findings from professions with similar occupational duties make a compelling case that exposure to traumatic and/or sensitive information carries the potential for multifaceted harm. This underscores the need for: (i) future studies that explicitly focus on HIMs and (ii) the development and evaluation of tailored interventions, such as training and both supervisory and organisational-level support, to protect the health and well-being of HIMs, CCs and other non-clinical healthcare professionals.
Footnotes
Acknowledgements
Appreciation is acknowledged to the Discipline of Digital Health and Information Management, Department of Public Health, La Trobe University for their support in producing this review. The authors would also like to acknowledge the support of Professor James Boyd (Chair of Digital Health) and Bernadette Gargan (Senior Librarian) at La Trobe University.
Accepted for publication April 12, 2025.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This review was partly supported by funding from the Health Information Management Association Australia (HIMAA) Research Grant (2024).
Ethics approval
As this scoping review did not require the involvement of animal or human participants, ethics approval was not required.