
Abstract
Introduction
Telemedicine is the provision of remote health services by health professionals using information and communication technology, including the exchange of information on diagnosis, treatment, prevention of disease and injury, research and evaluation, and continuing education of health service providers for the benefit of improving individual and community health (American Telemedicine Association [ATA], 2018, 2022; Anderson et al., 2017; Kalaivanan et al., 2021; Sasangohar et al., 2020). “Telehealth” is sometimes referred to interchangeably with “telemedicine” in the literature, but for the purpose of the current article, the focus is on “telemedicine.”
Types of telemedicine services include telepsychiatry, which provides medical services related to psychiatry such as psychiatric evaluation, therapy (individual therapy, group therapy, family therapy), patient education and therapy management using interactive telecommunications equipment, including audio and video. During the COVID-19 pandemic, the use of telemedicine was a solution for people who needed health services. The physical distancing and self-quarantine policies implemented to break the chain of transmission of the COVID-19 disease complicated the interaction between doctors and patients. The use of telemedicine is particularly beneficial for patients diagnosed with mental disorders (such as agoraphobia and anxiety disorders) who might otherwise not seek treatment due to difficulty leaving their homes or because they experience anxiety when participating in face-to-face treatment modalities (American Psychiatric Association, 2013). It can facilitate medical care at home without the patient needing to go to the hospital (Kaufman et al., 2020; Kruszyńska-Fischbach et al., 2022; Severe et al., 2020).
During the COVID-19 pandemic, the Indonesian Psychiatric Association (PDSKJI) urged psychiatrists to continue providing health services to patients through telepsychiatry, thereby bringing services to patients’ homes, assisting with integrated behavioural health and primary services care that have an impact on better outcomes (Ministry of Health Republic Indonesia, 2020; Kalaivanan et al., 2021; Sasangohar et al., 2020).
Montoya et al. (2022) reported that most clinicians (90.5%) surveyed in their international study had commenced or increased the provision of telehealth services since the onset of the COVID-19 pandemic; most clinicians indicated that they had positive perceptions of both service effectiveness and of patient satisfaction with telehealth. In the United States, analysis of trends in telemedicine used during the pandemic showed an increase of 154% in the period January–March 2020, compared to the same period in 2019, when most of the consultations had involved patients seeking treatment for conditions other than COVID-19 (American Psychiatric Association, 2021; Koonin et al., 2020). Li et al. (2022) reported in their review of the international literature that the majority of patients and healthcare providers were satisfied with telepsychiatry services and suggested that they constituted a feasible modality for service delivery that was appropriate for supporting patients and providers during the pandemic.
Some of the needs telepsychiatry can address include overcoming patient barriers to receiving care (e.g. distance, availability or transportation difficulties) and improving provider and staff access to training, resources or other critical elements. Service provision should ideally be planned to accommodate the goals and expectations of both patients and treating clinicians. Potential benefits to the service provider could include a reduced no-show rate, increased reporting of quality outcome measures, provider satisfaction, reduced provider travel time and increased efficiency. Benefits to patients could include improved outcomes, access to care and follow-up, and reduced travel time. Plans to introduce telepsychiatry and to assess its benefits should include the development of measurable goals based on the expected use of the service; the Maryland Health Care Commission [MHCC] (2020) and Mishkin et al. (2022) have suggested that these might include the number of encounters or outcome measures for a sub-population.
The Dr. Soeharto Heerdjan Hospital in Jakarta, Indonesia, provides in-person patient care via its 300 beds and 495 employees. The hospital’s Department of Psychiatry began to provide telepsychiatry services, which are part of telemedicine, in May 2020. The objective was to provide continuing care, for patients previously diagnosed with mental disorders, in the processes of treatment, continuity of medication and maintenance of clinical stability. The telepsychiatry services were implemented per the documentary guidance of the Ministry of Health Republic of Indonesia (Ministry of Health Republic Indonesia, 2019, 2020).
Community demand has continued for telepsychiatry services at the Dr. Soeharto Heerdjan Hospital. Telepsychiatry service visits increased by 704% in 2021, with a shift from 26 patients in 2020 to 183 patients in 2021. These services have not run optimally due to several obstacles, including the absence of a designated consultation room; no registration officer; a sub-optimal appointment system, and the fact that the majority of patients or their representatives have been unable to use the telepsychiatry applications (e.g. lack of user-friendly telepsychiatry applications and electronic media for information on telepsychiatry). The aim of our study was to assess telepsychiatry readiness at Dr. Soeharto Heerdjan Hospital.
Method
Research design
An observational survey was conducted at the Department of Psychiatry, Dr. Soeharto Heerdjan Hospital, in April–May 2022. Ethics approval was received from the Hospital’s Ethics Committee (approval number 0923-02.045/DPKE-KEP/FINAL-EA/UEU/III/2022).
Sample and recruitment
The sample was the entire staff who were directly responsible for telepsychiatry services. The 40 persons consisted of 16 administrative staff, 8 clinical staff (psychiatrists and nurses), 8 technology information staff and 8 management staff members. Data were collected using online questionnaires designed in Google Forms for 7 days.
Data collection
The Telehealth Readiness Assessment (TRA) tool (MHCC, 2020) was used for the data collection. The TRA tool was not designed specifically for psychiatry but for general telehealth interactions. However, it has been validated for small physician practices (MHCC, 2020; Nayar et al. 2017), and (to our knowledge) a bespoke tool for telepsychiatry readiness assessment does not yet exist, and as this is a small case report of one health facility department, we chose to employ it for this study. There are other toolkits available for introducing and delivering telepsychiatry (e.g. the American Psychiatry Association has a “Telepsychiatry Toolkit” for “members who want to learn about the various aspects of telepsychiatry, including clinical, training, and policy considerations”) but not whether a facility is prepared or has the resources to deliver it. For this reason, the TRA seemed more suited to the aims of this study.
The TRA tool includes five key domains associated with the successful implementation of telehealth: core readiness; financial considerations; operations; staff engagement and patient readiness:
(1) Core readiness in considering the need for, benefits of and challenges of implementing telepsychiatry. There are two aspects to “core readiness”: acceptance that telepsychiatry services are needed in the organisation; and organisational leadership and positive support for introducing the service.
(2) Financial considerations refer to having considered realistically the financial implications of implementing telepsychiatry including initial costs, sustainability, liability insurance and reimbursement procedures.
(3) Operations refer to considering how telepsychiatry will impact on current operations, and if the practice is able and willing to make appropriate changes to accommodate these. The six main operational areas to consider under this domain are as follows: telepsychiatry roles, scheduling and workflows, operational requirements, assessment approaches, technologies and physical space.
(4) Staff engagement refers to the practice team’s interest and engagement in implementing telepsychiatry. Two concepts relevant to this domain are as follows: education and awareness, and innovators and champions.
(5) Patient readiness refers to patients prepared for and motivated to participate in telepsychiatry. Relevant concepts for patient readiness are patient engagement and health literacy.
The TRA toolkit includes the components a service provider would require to apply it to their facility. These consist of a questionnaire, a scoring sheet, supporting guidance for each section of the assessment and other additional resources for engagement with staff and patients. The questionnaire is made up of 54 questions covering the five domains associated with the successful implementation of telehealth. Response options range from 0 = not applicable; 1 = no/unsure; 2 = somewhat [true] and 3 = definitely [true]. Responses of no or unsure are allocated 1 point; somewhat or partially [true] are allocated 2 points and definitely or fully [true] are assigned 3 points. Responses of not applicable are not assigned points and are not used to calculate the concept score. Items that were skipped (missing responses) were excluded from the calculation:
Composite scores on the TRA indicate the readiness level of a practice to introduce telehealth services. A low readiness score (⩽50%) indicates that the practice is either in the early stages of offering telehealth services or has not yet considered key aspects relating to the introduction of such services. Moderate readiness (a score of >50% and ⩽75%) suggests the practice has considered some aspects of introducing telehealth services but shows a need for some improvement. A high readiness score (>75%) shows that the practice has already taken into account many aspects of telehealth services and is in the more advanced stages of readiness. The overall TRA readiness score is a weighted average of the concept scores included within each of the five domains. Weights are assigned based on the relative importance of each item to the readiness score for each concept, and statistical ranking is determined through field testing of the TRA tool with small physician practices. If a concept is scored as not applicable, then that value is removed from the denominator when calculating the weighted average (MHCC, 2020).
Results
Demographic characteristics
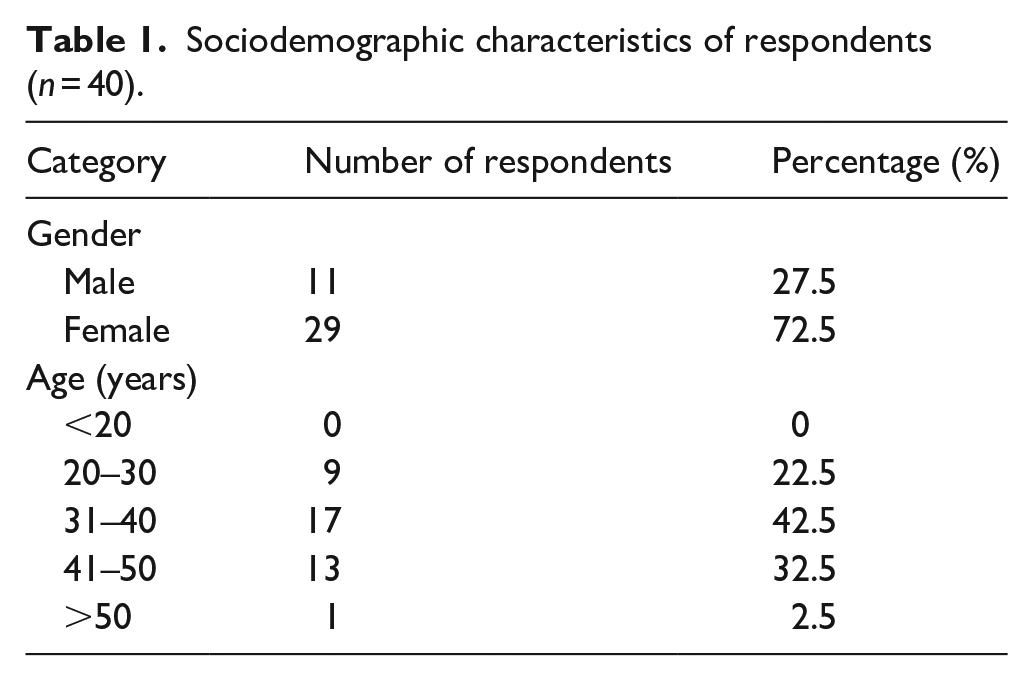
The sociodemographic characteristics of respondents are outlined in Table 1. Of the 40 respondents, the majority (72.5%) were females; 42.5% were aged between 31 and 40 years and 32.5% between 41 and 50 years.
Sociodemographic characteristics of respondents (n = 40).
Telepsychiatry readiness assessment
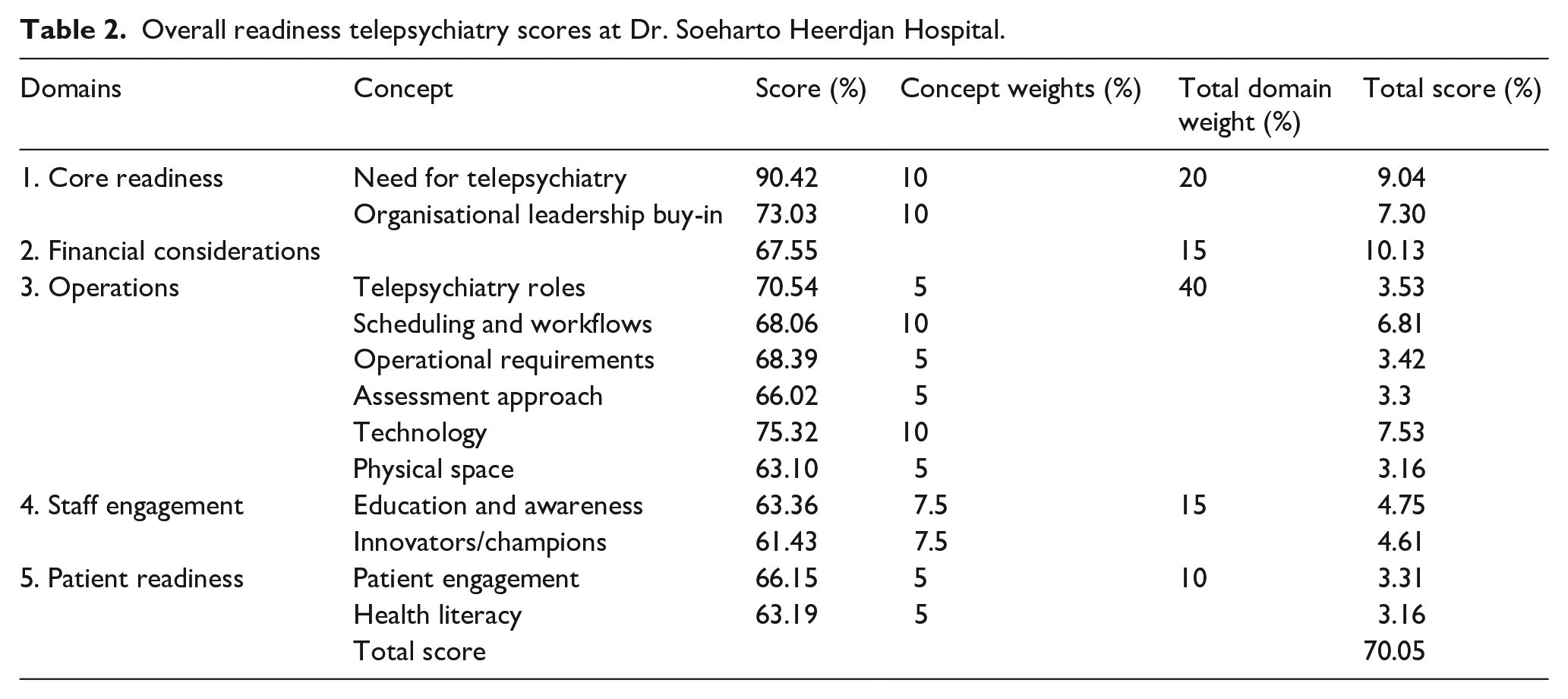
Full results for each Domain and Concept are shown in Table 2. In the case of Dr. Soeharto Heerdjan Hospital, the concept scores for the five domains of the TRA tool were as follows:
(1) Core readiness: The score for the need to introduce telepsychiatry was 90.42%, indicating high readiness; and for organisational leadership support it was 73.03%, which indicated moderate readiness.
(2) Financial considerations: The score for financial considerations was 67.55%, indicating moderate readiness.
(3) Operations: The score for telepsychiatry roles was 70.54% (moderate readiness); the score for scheduling and workflows was 68.06% (moderate readiness); the score for operational requirements was 68.39% (moderate readiness); the score for assessment approach was 66.02% (moderate readiness); the score for technology was 75.32% (high readiness) and the score for physical space was 63.10% (moderate readiness).
(4) Staff engagement: The score for education and awareness was 63.36% (moderate readiness), and for innovators/champions the score was 61.43% (moderate readiness).
(5) Patient readiness: The score for patient engagement was 66.15% (moderate readiness), and the score for health literacy was 63.19% (moderate readiness).
A total score for five domains of telepsychiatry readiness at Dr. Soeharto Heerdjan Hospital was 70.05% so the level of readiness for the implementation of telepsychiatry was “moderate” level.
Overall readiness telepsychiatry scores at Dr. Soeharto Heerdjan Hospital.
Discussion
Our research aimed to assess the status of telepsychiatry readiness at the Dr. Soeharto Heerdjan Hospital. It revealed a very high (90.42%) need for the telepsychiatry service, and scope for improvement in a range of non-clinical components of service and patient support and engagement. Telepsychiatry was needed due to some of the benefits of telepsychiatry which have been felt during the COVID-19 pandemic. Telepsychiatry has been also promoted during the first stages of the pandemic and can be sustainable over time, beyond the current healthcare emergency (Kaufman et al., 2020; Torales et al., 2022). “The psychiatrists continue to rely on telehealth for treating psychiatric and substance use disorders, and the regulatory changes made at the beginning of the Public Health Emergency to increase access to these services continue to be essential for doctors and patients alike”(American Psychiatric Association, 2021). Telehealth or telepsychiatry can improve access to healthcare, increase delivery options and improve patient outcomes (Bieber et al., 2022; MHCC, 2020; Torales et al., 2022). Patients and providers are generally satisfied with telepsychiatry services. Telepsychiatry is not more expensive than face-to-face delivery of mental health services and can actually be more cost-effective (Hubley et al., 2016). Torales et al. (2022) reported patients’ general satisfaction with the quality of care in telepsychiatry, mainly regarding the perception of healthcare, but had lower satisfaction with the doctor–patient relationship. Nine out of 10 psychiatrists felt satisfied with the telepsychiatry service and considered that the degree of patient satisfaction was acceptable during the Telepsychiatry consultation (Torales et al., 2022).
The total score over the five domains of telepsychiatry readiness at Dr. Soeharto Heerdjan Hospital was 70.05%, that is, the level of readiness for the implementation of telepsychiatry was “moderate” (>50% and ⩽75%). “Moderate” is explained as the facility that has considered some aspects related to the concept or domain and should review the associated supporting guidance document(s) to identify areas for improvement. There are several types of actions to consider prior to telehealth implementation including the determination of what telehealth services to offer, and documenting the benefits of telehealth services (MHCC, 2020). The results indicated that the Dr. Soeharto Heerdjan Hospital could usefully effect improvements in the domains of operations, staff engagement and patient readiness. This includes determining the staff responsibilities required to manage the administrative aspects of telepsychiatry such as appointment scheduling, coordinating information across providers and patient documentation. The staff responsibilities required to support telepsychiatry patients also include having a dedicated telepsychiatry contact person to explain telehealth, answer patient questions and provide assistance during telepsychiatry appointments. The additional telepsychiatry staffing support is needed to implement and maintain a telepsychiatry programme.
One advantage of telepsychiatry is that patients can access consultations from the security of their home; however, if the patient does not have the necessary privacy, they may not be able to respond candidly during the consultation. This potential barrier is beyond the capacity of the hospital to resolve, no matter how ready it may be to deliver this service.
Limitations
The TRA tool used in the current study has previously been validated only for the delivery of telehealth by small physician practices in a general health setting, whereas our application was to assess telepsychiatry readiness. Notwithstanding this limitation, the domains investigated included elements common to any facility or practice wanting to introduce service delivery via telehealth – the need for the service, the financial and operation considerations and the potential impact on staff and patients. COVID-19 propelled many areas of the health sector to urgently develop methods of service delivery that substituted for face-to-face interactions. In the absence of a bespoke assessment tool for telepsychiatry, we believe that, on balance, the TRA has enabled an acceptable assessment of this hospital’s telepsychiatry readiness.
Conclusion
The level of telepsychiatry readiness at Dr. Soeharto Heerdjan Hospital was a “moderate” level.
While many of the results are encouraging, our research has also identified several opportunities for enhancing the capacity of the supporting functions and facilities that underpin the hospital’s telepsychiatry services and, therefore, contribute to high-quality patient care. There is room for improvement in almost all of the domains of readiness, including providing workforces for patient registration of telepsychiatry, drug delivery, scheduling, designated consultation rooms for telepsychiatry, user-friendly telepsychiatry applications and electronic media for information on telepsychiatry.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.