
Abstract
Background:
The Manchester University National Health Service (NHS) Foundation Trust (MFT) is one of the largest NHS Trusts in England. Historically, the Trust has had very mixed clinical record keeping, including over 1000 individual information systems. None of these health information technology systems had the full functionality of an integrated electronic patient record (EPR). MFT evolved to its current size and complexity with a vision to improve patient care in Greater Manchester by adopting a Trust-wide EPR. The EPR “Go Live” occurred in September 2022.
Aim:
To describe the process of EPR integration as it reflected and impacted upon MFT’s health information management (HIM) teams.
Method:
MFT worked through a 2-year readiness program of work. This included technical readiness, software development and migration planning. Migration of data from the approximately 1000 systems was a major undertaking, during which access to the clinical history and ongoing operational reporting needed to be maintained. Pre-implementation requirements were outlined, a change management program was implemented, and the overall implementation was managed to tight timelines.
Discussion:
“Go Live” was achieved for the EPIC EPR product (HIVE) within MFT. Legacy systems are still in the process of being decommissioned and staff are transacting within HIVE. Significant changes in processes and reporting continue to be made, despite some challenges.
Conclusion:
The Trust delivered the single largest EPIC European “Go live.” Lessons learnt continue to be identified. The impact of what the EPR means for the HIM function is described.
Keywords
Introduction
Combining information technology (IT) by integrating and synthesising health information systems (HIS) and electronic health records (EHR) can streamline processes, increase efficiency, improve quality and safety and reduce costs (Campbell and Giadresco, 2020). However, excellent and reliable data quality is fundamental to any successful integration of datasets and systems. A recent study by Woods et al. (2021) focused on the quality of data in a national dataset relevant to palliative care for Indigenous Australians, specifically in relation to upgrades to data-checking systems. These authors suggested that secondary use of large, curated datasets could contribute towards improving data processes via feedback to data managers. Another study in Ireland (McGrath et al., 2022) described a multi-method approach towards improving the quality of health and social care data. This program provided information about the quality of health data and included guidance and support for users to implement standards and review and assess compliance, which led to improvements in health information management (HIM) practices. Reynolds (2022) described results of a 5-year learning-agenda program (learn-by-doing) designed to increase effectiveness of HIS interventions in low- and middle-income countries. Tools developed strengthened the HIS and country HIS profiles, as well as improving indicators, measures and documentation, creating a searchable database of HIS assessment tools and enabling the synthesising of results.
Similar amalgamation projects designed to integrate electronic medical records (EMR) and other electronic systems have focused on several different priorities. For example, Mensah et al. (2023) highlighted managerial performance, increased coordination of care, practice efficiency, improving health outcomes and patient safety. Nguyen et al. (2014) provided a review of EHR implementations around the world and reported on findings including benefits and issues associated with EHR implementation. Other perspectives have also been offered. For example, Kyozira et al.’s (2021) study in Uganda described an integrated data management system designed to harmonise United Nations High Commission for Refugees and Refugee Health Information System data with the Ugandan National Health Management Information System data to improve services for refugees, to reduce gaps in information, improve accuracy and facilitate planning, resource allocation and decision making. Challenges to achieving better health data quality were data collection, analysis and reporting. Seif et al. (2023: 1) leveraged electronic health systems with the aim to consolidate selected variables into one single “data universe” to create an “accessible and intuitive query tool for rapid data retrieval.” Their enhanced recovery program universe increased efficiency across several analytical tasks without adding to costs or interrupting workflows. Recent examples of newly created and innovative systems include a digital clinical information system designed for a forensic unit in Greece to manage the life cycle of forensic data, including new records, assignment to forensic pathologists, reports, multimedia requirements, issuing certificates and legal documents and statistics (Kalochristianakis et al., 2022). Sheikhtaheri et al. (2022) described the implementation of a near real-time EHR-based surveillance system for COVID-19 in Iran, to integrate data from multiple hospital information and EHR systems. Their system allowed researchers to coordinate a variety of tasks, including funding arrangements, allocating hospital resources, assigning hospital beds, acquiring and distributing equipment and setting up isolation centres. Such surveillance infrastructure created by integrating EHR and hospital HIS can also assist decision making, inform policy and lead to improved research data analysis.
Successful integration of systems also depends on collaboration and a willingness to share data among users. Lloyd et al. (2023: 1) explored perspectives of medical and nursing clinicians on the usability of an EMR. Perceived benefits related to “system design, human factors, safety and risk, system response time, and stability, alerts, and supporting the collaboration between healthcare sectors.” Krahe et al. (2023) examined the data sharing practices of 77 researchers from one institute in relation to barriers and facilitators of target behaviours that encourage data sharing. Perceived negative consequences and lack of competency were barriers; while trust in other users and the perceived social benefits of sharing data facilitated effective target behaviours.
There are many challenges and barriers to integration, as well as facilitators of success. Hoxha et al. (2022) reviewed technical, behavioural, organisational and environmental challenges to the use of data across four electronic databases. While organisational and environmental challenges were the most frequently reported, most strategies adopted tended to focus on technical barriers. In a study in Ghana (Mensah et al., 2023), the authors reported on a range of challenges to implementing EHR in low- and middle-income countries, including insufficient training, inadequate equipment and Internet access and lack of funding. Managerial support, together with relevant technical and logistical support, were seen to be fundamental to overcoming these challenges.
Much also depends on governance and management of health information. Kwan et al. (2022) examined the maturity of health information governance systems in Australian hospitals, specifically in relation to data privacy and security. While most hospitals surveyed had well-developed information governance schedules, policies and practices, only half had a formal information governance program in place. The authors reported that HIS were strengthened through the application of a “learn by doing” agenda, supported by team activities guided by an advisory group. Krahe et al. (2020) examined research data management skills, capacity and practices in medical researchers and academic institutes. While they found considerable variation across their sample (81 members of a research institute), these authors suggested that institutional strategies that focused on tasks related to creation, processing and analysis of data were most likely to improve the capabilities of researchers and promote sound practice. This would, in turn, improve health informatics and research data quality.
England’s lengthy, ambitious and sometimes fraught pathway to the electronic patient record (EPR) has been well documented (Greenhalgh et al., 2010, 2013; Houses of Parliament, Parliamentary Office of Science and Technology, 2016). The “Spine” (the National Health Service (NHS) centralised demographic system) is a now well-established, core component of the national EHR strategy. It supports the IT infrastructure for health and social care in England, joining together over 44,000 healthcare IT systems in 26,000 organisations (NHS Digital, 2023). The Spine allows information to be shared securely through national services such as the electronic prescription service, the personal demographics service, the summary care record and the e-referral service. None of these systems possess the full functionality of an integrated EPR.
Current study
Manchester University NHS Foundation Trust (MFT) is the largest provider of specialist services in England, covering a population of 2.8 million. It is the sole provider for several tertiary services across Greater Manchester. MFT is the Leading Trust in the North-West of England for research and teaching. It has a unique clustering of clinical services with life sciences and academia, and the largest critical care facilities in England. The organisation consists of 10 hospitals, two community care organisations, 3000 beds and employs 28,000 +staff and 8000+ associates (Manchester University NHS Foundation Trust, 2023).
The Trust had four non-integrated patient administration systems (PAS) and an EPR; multiple and duplicate third-party systems; multiple laboratory information management systems; and the stand-alone Manchester and Trafford local care organisation services, which had not been integrated into the acute services. Due to the number of mergers and acquisitions since 2012, the Trust had many IT systems, with some having similar functionality but supporting different services. In addition, one of the hospital sites (North Manchester) had only joined MFT in April 2021.
The Trust has evolved over many years to its current size and complexity. Consequently, MFT had very mixed clinical record-keeping and information systems. There was a hybrid medical records system, which included traditional paper health records, “paper-light” or scanned (digitised) records, or both, and a partial EPR. This combination was problematic for providing complete clinical histories for patient interactions, for ensuring necessary data were present and for accurate reporting through multiple systems for one Trust submission. Some of the systems were old and limited in functionality whereas others met required national standards. The Trust’s vision of a single hospital service was intended to create clinical services that could provide local accessibility using new models of care to deliver consistent, high quality and safe patient care. The introduction of a single EPR was an essential requirement to support this vision. Following an extensive and in-depth procurement process, the EPR solution put forward by EPIC (an American EPR product) was selected as the best option to meet the complex and specialist needs of the Trust. The HIVE was the agreed local title for the new EPR because it reflected the “Worker Bee” symbol for Manchester. 1 The Trust agreed to a whole-system Go Live across its 10 hospitals on 8 September 2022.
The aim of the current article is to describe the program in brief and outline the particular challenges, barriers and success that this implementation had upon the HIM teams that were part of MFT’s Informatics–Patient Services: Health Records, Clinical Coding and Data Quality.
Program
Following the decision to adopt the EPIC solution, MFT worked through a 2-year readiness program of work. This included technical readiness as well as software development and migration planning. Issues associated with the merger of multiple systems, such as the “pulling together” of all the different patient master indices (PMIs) into one, were identified. The NHS has a medical record unique numbering system for patients called the “NHS Number,” which is managed via The Spine. Some of the legacy systems within MFT were not fully “spine-compliant,” and while steps had been taken to ensure safety, the merger into one EPR would eliminate this inconsistency.
The single patient identifier (SPID) program involved work across the original three PAS to ensure each patient had a unique identifier and that all health records reflected this. Over a September weekend in 2020, all patients on the Wythenshawe Trafford Withington Altringham (WTWA) PAS were given a new number, which correlated to the Oxford Road Campus (ORC) PAS; their case notes were relabelled. Each required cross-checking and the Data Quality Team validated over 19,600 patients against The Spine and ORC PAS to ensure the numbering was correct. The decision was made not to integrate the physical records at this time, as the Trust planned to scan these records into HIVE and it was felt that this work would not add value because the scanning program was planned to start ahead of the HIVE Go Live. Therefore, if a patient had activity on the WTWA and ORC sites, the staff continued to use the WTWA physical case notes and ORC case notes, respectively. The SPID did not cover North Manchester patients or systems as they joined after this work had been completed. Simultaneously, the Data Quality Team was undertaking other significant work, including the collation of referral-to-treatment reporting. This involved drawing information from all main PASs to produce a single data submission to complete an NHS-required data return, and to produce the many reports for COVID-19 pandemic reporting requirements (from March 2020 and ongoing).
Many practices across MFT required reviewing to ensure alignment of staffing levels and procedures. To this end, the Data Quality, Health Records, and Clinical Coding Teams were centralised under Informatics–Patient Services, and lead staff in each area and site were brought together under one structure. Adjustments in each team were required and engagement with staff was key to ensuring they were well informed of what was happening, provided an opportunity for questions, clarification and to undertake additional upskilling ahead of HIVE training. Multiple meetings were held within each of the teams to brief them on planned changes.
To support the move to digital records, an electronic document management system (EDMS) was purchased. Hyland OnBase was deemed the most appropriate fit for MFT and the HIVE program. Any previous scanned images on the various legacy systems would be migrated via EDMS into HIVE. It was also envisaged that all active physical health records would be scanned and migrated through the EDMS into HIVE. This led to the closure of four on-site health records libraries and the reduction of off-site medical record storage, estimated to save £60 million (gross) over the 15-year life cycle of HIVE, and provided a major financial offset from the program. Clinical benefits were also envisaged via easier access to clinical records, as all records were now accessible in one location and one format (HIVE).
Migration of data from the nearly 1000 systems required planning to ensure access to the clinical history and the maintenance of ongoing operational reporting before, during, and after Go Live. Pre-implementation requirements included identifying: additional resources, key tasks to be undertaken, training and current skillsets of staff and staff requirements for the move to the EPR. Change management for such a fundamental shift in working practices had to be factored in and managed to tight timelines.
Preparatory work
As part of the preparatory work ahead of Go Live, several components of work were identified for HIM areas. These included:
Clinical coding
Establish required work-queues for the Clinical Coding Team across all sites (i.e., moving from hospital/site speciality teams to a single chronological order work-queue)
Support for chronological setup and evaluating skill and experience (i.e., qualified versus unqualified).
Define presentation and format for clinical coding in the EPR versus the case note (electronic document presentation differs from paper documents and key components are located in different areas of the electronic record).
Establish a process to manage missing data items.
Define support and training for staff who had not previously used encoder software.
Health records
Identify current physical case notes, their locations and who used them.
Identify and refine case note tracking location and borrower codes across all systems.
Investigate services using physical case notes (e.g., recording information or clinical histories), and whether this requirement would continue to exist post-EPR.
Identify remaining physical documents post-Go Live and establish how to manage these.
Define how scanning/EDMS would impact on the service.
Develop document types to support legacy data migration, and identify new document types for uploading documents from external and internal sources.
Establish an easily recognisable naming convention for document types that supported rapid document location.
Review digital competency of staff (e.g., some staff were dedicated to “transit,” did not use computers and moved physical records in trolleys or were drivers for health records).
Data quality
Define and describe required validations and priorities to support Go Live (i.e., merging PMIs, single patient index/master files, open registrations, pathways datasets).
Review and define required clinical pathway data flows for setup within the EPR.
Establish stabilisation and optimisation plans for the team following implementation.
These were some of the original objectives, which continued to evolve during the preparatory work. The establishment of rapid decision groups (RDGs) for each of the services was a key requirement to progress these objectives. Each RDG had a mix of staff including EPIC specialists, MFT HIVE leads, operational and clinical leads from each of the Trust hospitals and services, and leads from within the patient service areas. This approach ensured that the process was reviewed from end-to-end and met all requirements. It became apparent that the scale of work required was significant and although the Clinical Coding and Health Records Teams were able to realign tasks to facilitate input and support for HIVE without additional resources, the Data Quality Team was allocated resources to undertake the actual transactions, due to the volume of that work.
Deliverables
Health records
Following an individual training needs analysis of all staff, additional skills development training was offered. Staff were allowed to repeat HIVE training multiple times and were given dedicated weekly practice time ahead of Go Live.
The number of borrower codes for case note tracking across all Department systems was reduced from >3000 to approximately 600 by reviewing, refining and ensuring consistency. The Health Records Team undertook several schemes of repatriation of loose documents (for filing into case notes) to assure the Trust that all records were complete and up-to-date. The Health Records Team also undertook several “amnesty” days, which involved case notes being collected and filed back into the libraries. This also served to limit the availability of paper within clinical settings and ensured physical case notes could not be used to record clinical information. The Team achieved a reduction in the routine provision of case notes from 192 services pre-Go Live to 130 at Go Live. With the cessation of case notes, the cost of folders and pre-printed paper has reduced by over £150K recurring per annum from Health Records alone. The Trust anticipates saving over £1 million in 12 months on paper, and a further £1 million on printing consumables.
Data quality
Over the 2-years implementation period, the Data Quality program undertook validation across a range of areas:
Wythenshawe SPID, updated in the system and physical records.
Auto-discharge (system-initiated discharges) reviewed and validated.
Consultant master file validated and updated, and patient episodes refreshed.
Open registrations, reviewed and confirmed as valid.
MPI potential duplicates (due to the merger of PAS systems) were reviewed, checked on The Spine and details confirmed or merged.
Pathways created and validated to fit the new way of working.
The pre-Go Live phase was a major undertaking for the Data Quality Team. Additional staff were onboarded and trained to support the different validation schemes. The Trust had been advised before Go Live by EPIC that a duplicate rate of less than 3% must be achieved. As the existing duplicate rate was higher than this, the Data Quality Team diverted staff to this program and successfully reduced the rate to less than 3% prior to Go Live. The Trust undertook the updating of a total of 4,000,000+ records, migrated from 80 different systems, and 800+ testing scripts, including: future appointments, pathways, referrals, waiting lists (day case and surgical), waiting list (outpatients) and waiting list (invasive cardiology). The Data Quality Team has continued to update patient demographic information against the National Spine as part of stabilisation work, and has also shifted focus to data quality assurance and audits.
Clinical coding
Clinical coding successfully went live on HIVE for discharges at Go Live. A dedicated team supported “crossover” patients (admitted on the legacy system and remaining an inpatient at Go Live), whose records required clinical coding on both systems. There was a plan to support long-term patients and how and where their activity was to be coded so that the inpatient episode was not compromised (i.e., to avoid discharge from the old system and admission to HIVE EPR, thereby maintaining integrity of the episode of care data). Clinical coders were trained on the system prior to Go Live and knew where to find key information. They were also provided with coder booklets designed by the Clinical Coding Training Team.
Staff adjusted from work tasks that had been driven by physical case note availability to a digital work queue that identified discharged patients. Clinical coding was successfully completed on first attempt as all necessary information was in one location, thus negating the need for partial coding or pauses while awaiting further information (e.g., paper-based test results). The Clinical Coding Team has continued to work on developing clinical coding flags within the system. For clinical coders, the shift from reading and interpreting handwritten to typed notes marked significant improvements in efficiency and accuracy.
Additional functionality within HIVE has enabled the routine monitoring of clinical coder productivity and of the activities of individual consultants who support clinical coding improvement schemes. The functionality within HIVE has also allowed our clinical coding audit processes to be standardised across all sites, as one system enables comparisons to be made easily. This has facilitated knowledge sharing across all staff and facilitated support for staff to gain experience in all areas without having to physically move sites.
Implementation
The upload of legacy scanned records at Go Live was delayed because migrated images, an essential element of document structure, were unavailable due to supplier issues and direct access within HIVE to view these records was not possible. A second system was temporarily used to view images. This issue has since been resolved and this component of the system is now fully operational.
A week after Go Live, one hospital site encountered an unplanned event, where access to HIVE was lost for approximately 24 hours. This had an impact on health records because staff reverted to paper records that required scanning into HIVE. This was not the agreed downtime procedure, but rather a reversion to a familiar process. Health Records staff were able to support this process by printing cover sheets and scanning several thousand documents into HIVE within a few days; however, a review was undertaken of how the downtime procedure had been cascaded and a new communication plan was initiated.
Data reporting
Initially, there were challenges related to the level of reporting available from within HIVE to support clinical coding. With assistance from business intelligence colleagues, a suite of reports was developed that exceeded the initial requirements and supported wider reporting functionality. Clinical coding of crossover patients required attention, as the legacy systems were “off” for several days and the “cut off” dates provided were challenging. These were successfully addressed.
To date, there has been no change in productivity within clinical coding since moving to an electronic system (see Figures 1 and 2). It is estimated that within the next few months, as staff become more familiar with HIVE, productivity is likely to improve. The focus on depth of clinical coding (number of secondary diagnosis codes for each record) has shown an improvement against pre-live statistics. Greater depth of clinical coding supports additional income into the Trust, increased research opportunities, and improved reporting overall. Depth is currently averaging 7.2 comorbidities per patient.
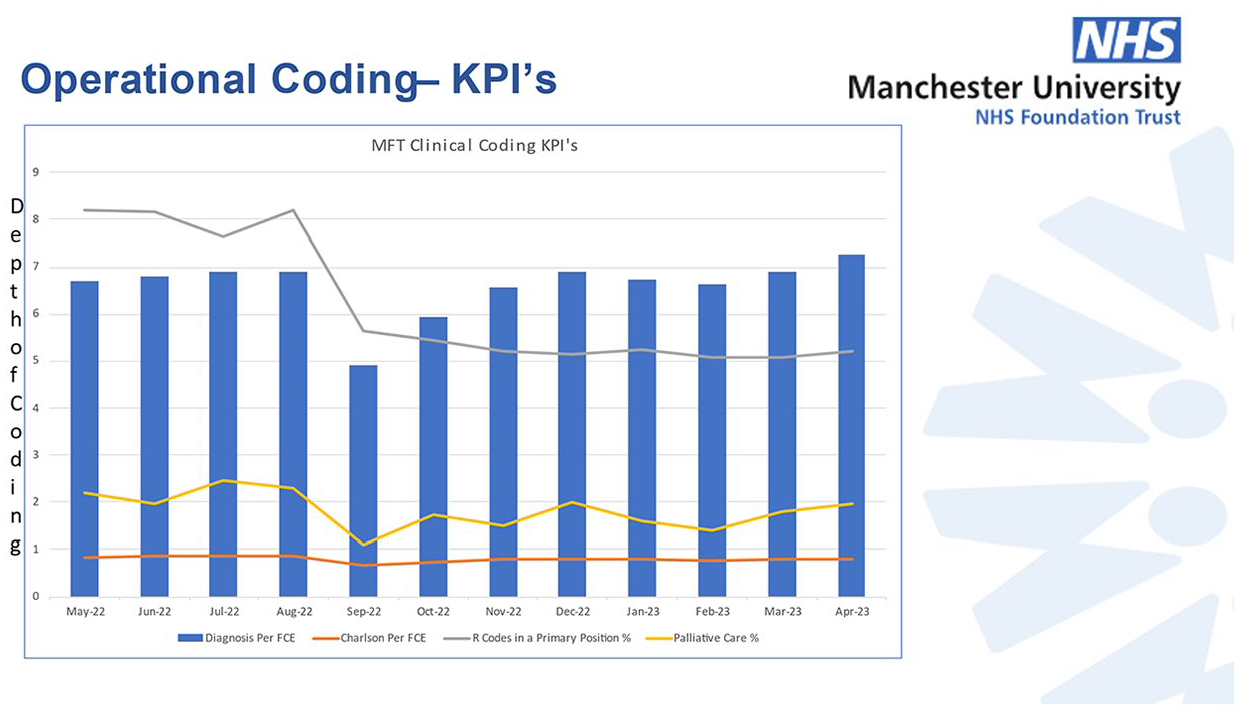
Operational clinical coding from May 2022 to April 2023.
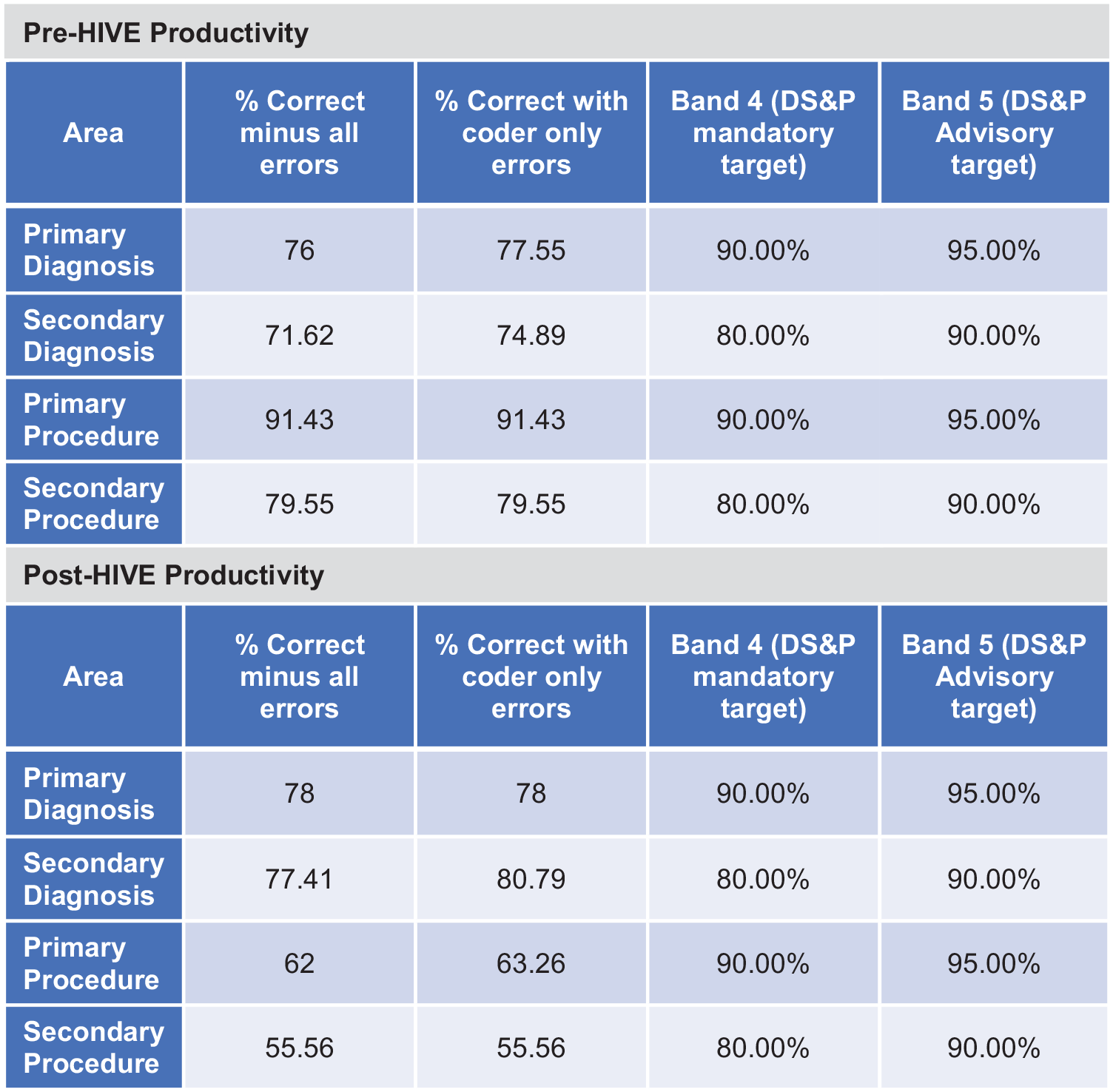
Productivity in clinical coding before and after HIVE Go Live.
Effects of soft Go Live
MFT undertook a soft Go Live, meaning some information was dual entered: some on HIVE only and some remaining on legacy systems. The messaging ahead of the soft Go Live was unclear and resulted in data and information either being recorded in Legacy only, some inappropriately on either Legacy or HIVE, or some being missed completely due to administration staff assuming information would flow automatically through the two systems. These issues were identified post Go Live and impacted on the pathway management of patients. The Data Quality Team was required to unpick this information across all systems, identify the relevant activity and ensure it was correctly recorded (i.e., appointments to be attended after going live were on HIVE, and only activity that had occurred prior to Go Live was recorded on Legacy).
Since Go Live, the Data Quality Team has continued to support key schemes within HIVE as part of the stabilisation process, including ongoing validation and testing of new functionality as it was released. We also experienced some issues with data quality that impacted on clinical coding, which could not be undertaken until the issues were resolved. As staff knowledge of the system has increased through daily use and continuing to make functional amendments, data quality issues have decreased. The Data Quality Team has also ensured that MFT’s Referral To Treatment (Government standard for treatment from decision to refer until definitive treatment is provided) position is accurate and meets national standards.
Outcomes and experience
The project went live during a turbulent period in the United Kingdom (UK), which included the COVID-19 pandemic and subsequent elective recovery program, the UK leaving the European Union, the Platinum Jubilee for Queen Elizabeth II and her subsequent death, the accession of King Charles III and changes in political leadership with three prime ministers in 3 months. Despite these distractions, the planned Go Live date of 8 September 2022 was achieved and HIVE is now operational within MFT. Legacy systems are still being decommissioned. Staff are fully transacting within HIVE. Optimisation of processes and reporting have been, and continue to be, made. Statutory (national) data reporting is live, and there is confidence in its accuracy in light of the uniform data location and a strong validation process. A new suite of standard operating procedures has been developed and implemented across the organisation, assisted by the Data Quality Team.
The project was not without challenges, but no adverse events were experienced due to the Go Live. Patients have continued to be treated and have been provided with enhanced access to their data. Box 1 shows the MFT’s considerable activity undertaken between September 2022 and February 2023.
MFT activity between September 2022 and February 2023.
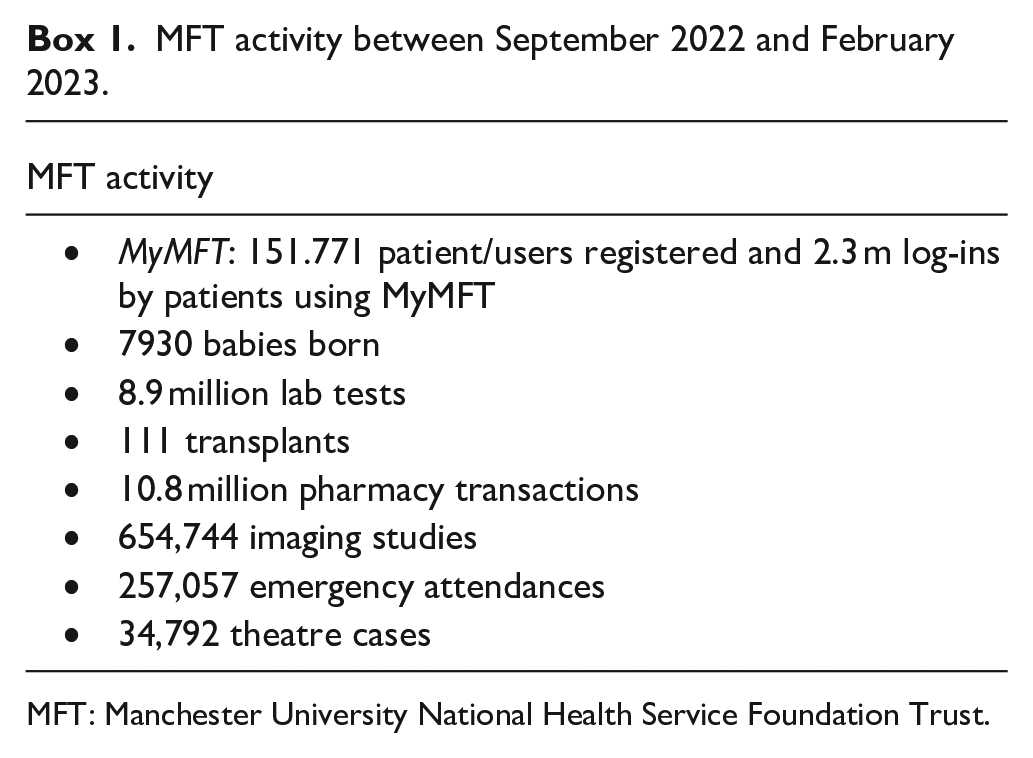
MFT: Manchester University National Health Service Foundation Trust.
A full EDMS that contains a scanned copy of physical case notes is not yet available; therefore, from a HIM perspective, one important operational function that remains to be delivered is fully digitised health records. Currently, HIVE only contains data from the legacy electronic systems and data entered from Go Live onwards. The business case for fully digitised health records is being evaluated.
Benefits
A single Go Live at the largest NHS Trust in England was delivered. It was EPIC’s largest single Go Live within Europe. Benefits have already accrued from the implementation of HIVE, including:
Improvement in operating theatre utilisation.
MyMFT (a new online web portal and mobile app that connects patients to their MFT information) is live and patients have improved access to their data, including information recorded after 8 September 2022 and clinical correspondence.
Secure chat in use for communication between teams.
Outpatient letter turnaround is under 7 days.
Bespoke urgent care workflows are improving patient transfer between Urgent and Emergency Care services.
Single speciality patient tracking lists are in place.
Patient records shared with other EPIC sites (where there is shared care agreement).
Standardised discharge letters, with reduced duplication and improvement of accuracy.
Improved results management.
The preparation and preliminary work undertaken were key enablers to the success of the system at Go Live. Some essential dependencies (e.g., the maximum number of duplicates allowed) could have been covered earlier, would have allowed for a more staggered approach and would have supported other validations and process checking ahead of Go Live.
Staff training and education were important to ensure that HIVE processes were appropriately supported by administration. A review of operational reporting to maintain patient care and patient flow was undertaken ahead of Go Live; this work was developed further during the stabilisation and optimisation periods to maximise the benefits of all data being available from one system. The next step will be digitisation of legacy case notes and a paperless health record.
Patient access
New functionality within HIVE, called MyMFT, has allowed patients to access certain parts of their digital record and to request a copy of their full health record within “two clicks.” As a result, subject-patient access requests for release of information doubled in the first month of MyMFT becoming active, and continued to rise. Additional staff were allocated to support this function, and all timeframes are now being met.
Lessons learnt
From the Trust perspective, the main lessons learnt were:
Staff are resilient and tolerant if the right ethos is created. Do not be afraid to talk to staff and advise them of future plans.
Recognise and be realistic about funding requirements and timescales to deliver effective implementation.
Maintain the clinically led, operationally delivered and digitally enabled vision. A system designed by clinicians to ensure appropriate usability to support patient care, and operationally delivered so local services are invested in recording and transacting all possible digital opportunities.
Prioritise staff training; ensure accessible training is available across different venues and days/times, including e-learning and face-to-face options. Encourage staff to attend as many sessions as possible. Training cannot be overdone.
Use incumbent staff, where possible, for training because they understand the full process. The Trust appointed an external provider to deliver training based on EPIC’s train-the-trainer modules and Trust-developed scripts; however, they were not employed within the Trust and could not answer procedural or process questions.
Maintain executive oversight and organisational ownership.
Do not be afraid to de-scope. Consider what is essential and deliver that safely before adding additional functionality.
Performance-manage the change process.
Identify all stakeholders involved in the program, internal and external, and maintain regular communication.
Start data migration preparedness early. It is easy to underestimate timeframes.
Start early and focus on benefit realisation. With sufficient preparation, benefits should be immediately apparent. Insufficient preparation can lead to loss of potential financial benefits (e.g., cancellation of legacy systems, reducing consumable contracts).
Be prepared for the stabilisation and optimisation phases of the program and ensure they are defined and factored in to the overall plan.
This was a huge program of work that was delivered on time due to organisation-wide commitment and drive, from the Executive Team down. It was clinically led and continues to be driven by our clinical staff who have appointed champions to shape and develop the system. All staff within the organisation recognise and appreciate that this is a 15-year program of work and that while significant changes and benefits have already been achieved, the system will continue to be developed during its lifespan.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.