
Abstract
Background:
The Minimum Data Set (MDS) plays a vital role in data exchange, collection and quality improvement. In the context of the COVID-19 pandemic, there is a need for a tailored MDS that aligns with the specific information needs of the Iranian community and integrates seamlessly into the country’s Hospital Information Systems (HIS).
Objective:
The study aimed to develop a comprehensive MDS for COVID-19 patients in Iran, with objectives to identify essential data elements and integrate the MDS into HIS, enhancing data exchange and supporting decision-making.
Method:
This study employed a comparative-descriptive approach to design COVID-19 patient data elements based on World Health Organisation and Centers for Disease Control and Prevention guidelines. The Delphi technique involved 35 experts in two rounds for checklist refinement. The finalised MDS consisted of 9 main terms and 80 sub-terms, analysed using descriptive statistics and IBM SPSS software.
Results:
Of 35 experts involved with the study, 69% were male and 31% female, and Health Information Management experts were the majority (34%). The refined MDS for COVID-19 in Iran comprises 50 data elements, while 30 elements were excluded. The MDS includes 8 main terms and 80 sub-terms, with unanimous approval for identity, underlying disease, and treatment sections.
Conclusion:
The customised MDS for COVID-19 patients in Iran addresses data collection challenges and supports effective disease prevention and management. By providing comprehensive and reliable information, the MDS enhances healthcare quality, facilitates timely access to medical records, and fosters integrated health services.
Keywords
Introduction
For the past 3 years, the COVID-19 pandemic has been a pressing global issue, affecting countries worldwide, including Iran. Ensuring the provision of timely and effective care, preventive measures and treatment services to the community has consistently remained a top priority for the Iranian healthcare system. This commitment has continued unwaveringly throughout the pandemic, underscoring its significance and urgency (Mohammadpour et al., 2023). Access to accurate and comprehensive information is essential for various stakeholders, including healthcare providers, policymakers and decision-makers. This access enables them to make informed decisions and develop effective strategies, both at the individual patient care level and on a broader scale when formulating macro decisions and policies. Therefore, Iran’s electronic health record (EHR) system (called SEPAS) and hospital information systems (HIS) play a crucial role in providing high-quality care by facilitating the seamless sharing of health information among healthcare providers (Abbasi et al., 2019; Ahmadi et al., 2014).
The quality of the information shared from the HIS to the SEPAS, in terms of studies, analysis and scientific and statistical information, is dependent on the completeness and accuracy of the medical notes recorded by the treating clinicians (Farhan et al., 2005). Quality encompasses aspects such as availability, timeliness and readability. Therefore, proper documentation of patient health records is a significant legal obligation in healthcare. Adequate reporting facilitates the exchange of patient information among all members of the treatment team, ensuring that necessary care is provided to the patient (Safdari et al., 2014). The Health Information Management (HIM) Committee, operating at the national level, plays a pivotal role in making decisions based on Minimum Data Set (MDS) for data collection and reporting. These decisions are crucial for ensuring standardised and accurate information exchange within the healthcare system. Additionally, the sharing of health data and the global implementation of EHRs are essential components for effective healthcare management and information exchange (AIHW, 2003). One of the national challenges identified in a study conducted in Finland was the documentation and standardisation of data, for which the MDS was proposed as a recommended solution (Tanttu et al., 2008). Similarly, another study in Canada emphasised the significance of an MDS in health information systems as an essential standard for EHRs (Spigolon et al., 2012).
Previous studies have made significant contributions to the successful development of a new MDS. Ghazisaeidi et al. (2018) conducted a study to determine the information elements and MDS required for web-based electronic records of patients with glaucoma. Their questionnaire-based data collection approach involved 22 glaucoma specialists Additionally, Sadoughi et al. (2013) established an MDS for the country’s national cancer registry system, drawing insights from comparative studies and recognising differences in cancer data collection systems. The suggested MDS encompassed demographic data, tumour information, treatment details and end-of-life status.
Given the significant prevalence of COVID-19 cases in Iran over the past 3 years, a wealth of information has been diligently gathered and documented regarding these patients (Mohammadpour et al., 2023). However, there is still a deep gap between gathering, understanding and interpreting these data. On the other hand, health data are inherently voluminous and, in some cases, confusing for those who are unfamiliar with their collection and management. Additionally, the MDS provides a standardised approach to collecting key data elements, facilitating data comprehension and comparison, meeting government requirements, internal institutional needs and serving the medical community (AIHW, 2003). The MDS Forms for patients with COVID-19 are designed by the World Health Organisation (WHO) and the Centers for Disease Control and Prevention (CDC) to capture patient information, clinical details, occupational and virus exposure information, hospital data and laboratory information (CDC, 2020; WHO, 2020). While the Ministry of Health and Medical Education mandates the use of data element forms in hospitals across the country, the current forms may not be entirely applicable to Iran, as they do not consider the local conditions and Iranian HIS. The volume of data generated by using these forms may overwhelm healthcare providers during the current critical situation in Iranian hospitals. As a result, there was a need to customise the MDS to fit the Iranian context, ensuring efficient data collection, and enabling effective decision-making and healthcare management during the COVID-19 pandemic.
Aim and objectives
This study aimed to develop a comprehensive national MDS for COVID-19 patients in Iran. The objectives were:
To identify the essential data elements needed for the COVID-19 MDS.
To provide a standardised approach for integrating the MDS into Iran’s HIS, enabling efficient data exchange and utilisation.
Method
This study utilised a comparative-descriptive approach based on variables collected by the World Health Organisation (WHO, 2020) and the Centers for Disease Control and Prevention (CDC, 2020). Neither the WHO nor the CDC appear to have yet named a definitive MDS for COVID-19; however, Allan et al. (2022) describe the WHO, supported by an international working group, proposing a list of essential variables and standards. These were included into the T0 questionnaire (WHO, 2019), which was used to develop the initial case reporting form for COVID-19. The process is described in Perrocheau et al. (2021). On the basis that the Case Reporting Form was developed from this process for defining a minimal dataset, the authors adopted the Case Reporting Form as a proxy for an MDS. Similarity of data variables collected in the CDC “COVID-19 person under investigation and case report” form supported similar adoption of the form as a proxy for the MDS. Henceforth, these are referred to as the “WHO MDS” and “CDC MDS” throughout this study.
Data collection
The data collection process involved three phases:
Phase 1: A comparative-descriptive study was conducted, and data elements were designed for COVID-19 patients in Iran based on the MDS.
Phase 2: in 2020, a Delphi technique was employed, consisting of two rounds of interviews with 35 experts who were selected based on their expertise and qualifications in relevant fields. Our approach aimed to include representation from diverse domains, encompassing clinicians, HIM specialists and medical informatics professionals. The experts’ selection process considered key factors, such as their professional background, experience and involvement in HIM and COVID-19 patient care, to ensure a comprehensive and well-rounded perspective during the Delphi technique rounds.
During the first round, a checklist was designed by the researchers conducting the study to gather essential data elements that were relevant for COVID-19 patients in Iran. The checklist was then carefully revised and edited by the researchers in collaboration with the experts, both in-person and electronically, ensuring that their valuable input was incorporated. In the second round, the refined checklist was distributed to the experts, who were asked to evaluate and rate their agreement with each data element using a five-point Likert scale. This iterative process allowed for the incorporation of expert feedback and refinement of the checklist. In addition, an open-ended question was included in the second round to gather further suggestions and opinions from the experts. This approach aimed to capture a comprehensive understanding of the subject matter, ensuring that valuable insights and potential improvements could be considered in the development of the final MDS for COVID-19 patients in Iran.
Phase 3: The MDS was categorised into 9 main terms and 80 sub-terms, which were recommended for implementation in all health information systems. The main terms included: (1) patient identity information (4 questions); (2) patient symptoms (15 questions); (3) underlying disease information (11 questions); (4) history related to COVID-19 (11 questions); (5) patient diagnostic results (15 questions); (6) disease progression (11 questions); (7) occupation (5 questions); (8) discharge status (4 questions); and (9) diagnostic laboratory information (4 questions).
Data analysis
During the data analysis process, the significance of each data element was determined based on experts’ ratings. If 75% or more of the participants chose “high and very high” options for a specific element, it was considered a main term. If 50–74% of the respondents selected “very high and high” options, the element was considered a recommended element. Any element for which less than 50% of the experts chose “very high and high” options was removed from the final recommendations. The data analysis considered the perspectives of clinical experts, information management specialists and medical informatics professionals. Descriptive statistics were employed in the analysis, and the data processing was carried out using SPSS software version 26. These MDS forms served as the basis for our initial dataset development. By examining and comparing these different MDS, we aimed to identify relevant data elements and adapt them to the specific needs and context of the Iranian healthcare system. The implementation of the MDS also provided a standardised approach for collecting essential data elements related to COVID-19 patients.
Results
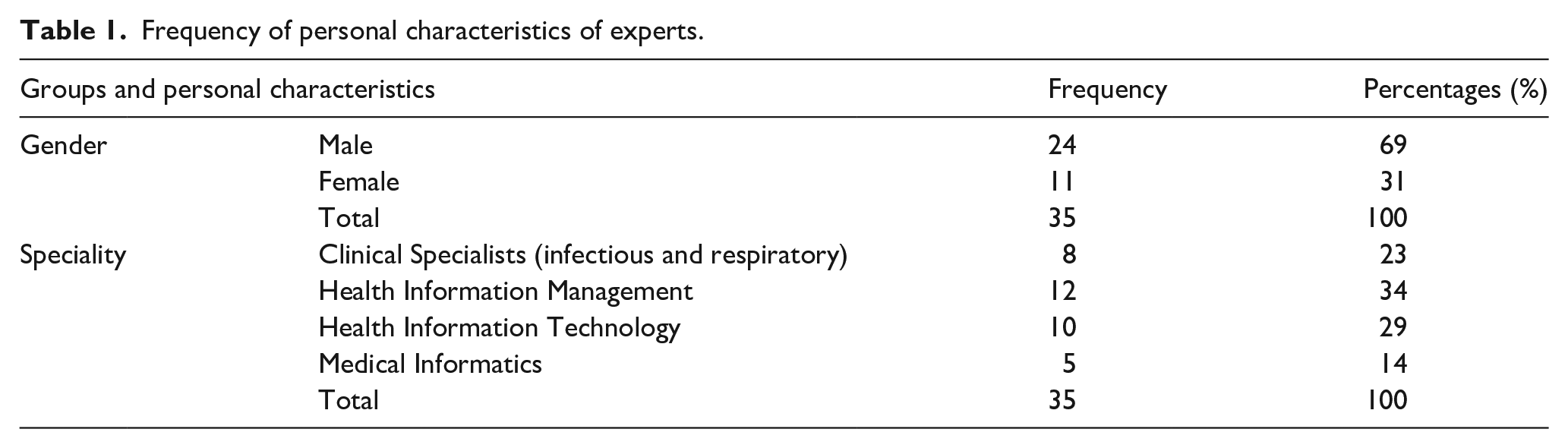
Personal characteristics of the 35 experts participating in our study are shown in Table 1. The frequency of males was higher than that of females, with the highest frequency being among the HIM experts (34%). Table 2 shows the recommended MDS for COVID-19 in Iran, categorised based on main terms and sub-terms. Among the 80 surveyed data elements, 50 achieved an agreement of 75% or higher. Conversely, 30 elements, comprising two main terms and 21 sub-terms, had less than 50% agreement and were consequently excluded from the draft MDS. The Delphi rounds also introduced 10 new data elements, including first and last name, national code, number of family members, address and contact number, job, HIV and addiction status, antiviral drugs, antibacterial drugs and other treatments. The final version of the MDS encompassed eight main terms, covering patient identity information, patient symptoms, underlying disease information, COVID-19-related history, patient diagnostic results, treatment measures, disease progression and discharge status, which were recommended for incorporation into Iranian HIS.
Frequency of personal characteristics of experts.
The recommended COVID-19 MDS for Iran.
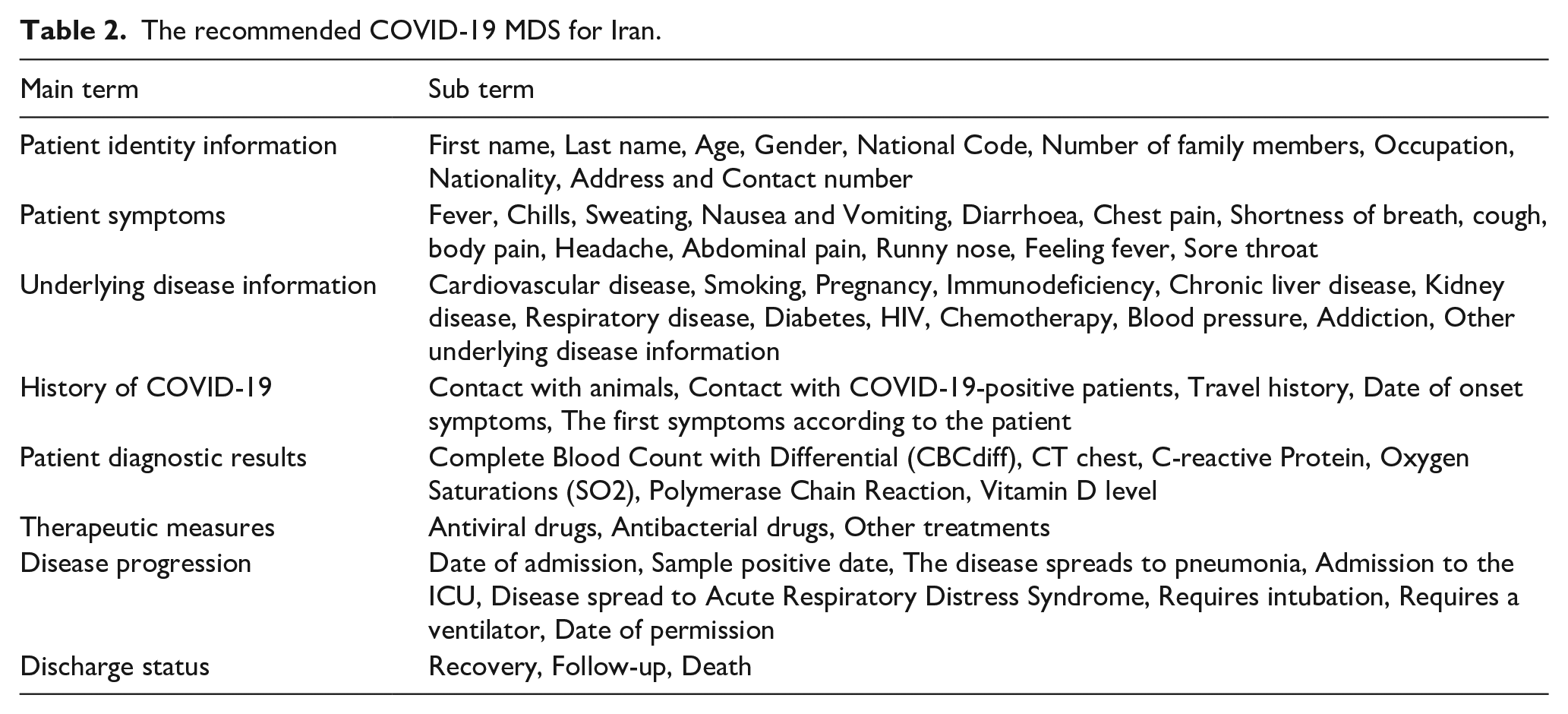
The data elements were unanimously agreed upon, and for the discharge status index, three out of the four data elements were selected. Moreover, all of the recommended data elements in the sections of identity information, underlying disease information and treatment measures (8, 13, and 3 data elements, respectively) were approved by the experts.
Finally, the MDS was categorised into 9 main terms and 80 sub-terms, which were recommended for all health information systems. The main terms included: patient identity information (4 questions); patient symptoms (15 questions); underlying disease information (11 questions); history related to COVID-19 (11 questions); patient diagnostic results (15 questions); disease progression (11 questions); occupation (5 questions); discharge status (4 questions); and diagnostic laboratory information (4 questions).
Discussion
This study focused on designing an MDS tailored to the Iranian community, facilitating data exchange, collection and quality improvement in COVID-19 patient care. Timely and accurate information is vital for effective treatment processes, making the quality of available information essential for healthcare decision-making (Patak et al., 2009). By adopting a standardised MDS, data collection becomes more efficient, enabling better comprehension and comparison of information (Safdari et al., 2014). To enhance healthcare quality, it is crucial to establish suitable methods for data collection, focusing on measuring healthcare system effectiveness and efficiency. By adhering to a standardised MDS, data collected can be efficiently utilised for decision-making, quality improvement and research, while promoting data exchange and interoperability among healthcare facilities, fostering a comprehensive and integrated approach to managing the pandemic in Iran (European Commission, 2004). In comparison to other relevant studies, several registries and surveillance systems have been established in Iran to bridge the knowledge gap surrounding COVID-19. The Sina Hospital COVID-19 Registry (SHCo-19R) comprehensively assessed patient characteristics, imaging features, laboratory findings, management strategies and adverse outcomes of Iranian COVID-19 patients (Roshandel et al., 2020). In line with this registry, our study holds its distinct value by customising the MDS to suit the unique Iranian context. By incorporating local factors, cultural considerations, and specific healthcare practices, our approach ensures that data collection remains relevant, comprehensive, and meaningful to the challenges faced in Iran throughout this health crisis. This customised approach enhances the accuracy of the information gathered, empowering healthcare management and decision-making.
Various studies have highlighted the importance of registries and EHRs in managing COVID-19 data (Kazemi-Arpanahi et al., 2020; Khorrami et al., 2020; Sheikhtaheri et al., 2022; Zarei et al., 2021). For instance, a web-based registry specifically designed for COVID-19 aimed to provide a reliable data source for reporting and benchmarking the disease (Kazemi-Arpanahi et al., 2020). The implementation protocol of the regional COVID-19 registry in Hormozgan province emphasised the potential for collaborative studies and data coordination, enabling comprehensive insights into COVID-19 data (Khorrami et al., 2020), and a real-time EHR-based COVID-19 surveillance system demonstrated its effectiveness in monitoring and managing the pandemic (Sheikhtaheri et al., 2022). Our study’s customised MDS approach enhances the accuracy and relevance of COVID-19 data in Iran, supporting evidence-based strategies for pandemic control. Integration of the MDS with other registries contributes to a more comprehensive understanding of the virus’s impact, guiding informed decision-making and policy formulation. The tailored approach complements standardised tools from the WHO and CDC, bridging global standards with local needs and fostering efficient healthcare management in Iran. This collective effort strengthens the nation’s response, creating a resilient healthcare system for future challenges.
The WHO and CDC have played a crucial role in providing standardised data collection tools for COVID-19 through their MDS. The WHO MDS encompasses vital patient information, clinical details, travel history, exposure to the virus and laboratory data, aiming to facilitate a uniform approach to gathering essential data elements for new COVID-19 cases. Similarly, the CDC MDS captures interviewer information, basic patient details, symptoms, clinical timeline, prior medical history and individual social records, offering a comprehensive means of gathering critical insights into COVID-19 patients for improved understanding, management and response to the pandemic (CDC, 2020; WHO, 2020). While the WHO and CDC MDS forms provide essential foundations, our study has added additional value by customising the MDS to the unique Iranian context. We considered local factors, cultural considerations and specific healthcare practices that are relevant to Iran. By customising the MDS to meet the specific information needs of the Iranian population, we aimed to enhance data exchange, collection and quality improvement in COVID-19 patient care, ensuring that the data collected aligned seamlessly with the country’s healthcare system. This customisation makes the MDS a more efficient and relevant tool for healthcare decision-making, quality enhancement and research purposes in Iran’s dynamic and evolving healthcare landscape.
In addition to the WHO and CDC MDS, the United Kingdom Government has provided guidance for the Middle East MDS (Public Health England, 2023), focusing on patient-related information, disease descriptions, side effects, signs and symptoms and diagnostic tests (Romanow, 2006). Our study’s expert informants collectively agreed on the proposed demographic and clinical data elements for the new MDS, ensuring comprehensive data coverage. By incorporating both demographic and clinical data, our MDS facilitates direct patient care, reimbursement, planning and research, offering a holistic approach to COVID-19 patient management. By integrating our study with the collective efforts of other registries and surveillance systems, we have contributed to a more comprehensive understanding of COVID-19 in Iran and supported the development of evidence-based strategies for controlling the pandemic (Roshandel et al., 2020). The customised MDS approach in our study adds value by considering local factors and ensuring efficient healthcare management, thereby complementing the standardised data collection tools provided by the WHO and CDC for COVID-19. Through our collaborative efforts, we have envisioned a strengthened healthcare system, better equipped to face future health challenges.
Limitations
This study has several limitations. First, its focus on the Iranian community may limit the generalisability of the developed MDS to other regions. Second, the expert panel’s composition mainly included experts in HIM, health information technology and medical informatics, with relatively limited representation from clinical specialists, which could have potentially overlooked crucial clinical aspects in the MDS development. Additionally, the reliance on expert consensus may have introduced bias, with the MDS primarily capturing demographic and clinical data and potentially missing other important factors. As well, the guidelines used for MDS design were developed early in the pandemic and would not have included the latest advancements and knowledge, such as vaccination status. Despite these limitations, the study has contributed valuable insights into data standardisation and decision-making in COVID-19 management, highlighting the need for future research to refine and update the MDS based on evolving scientific understanding and healthcare requirements.
Conclusion
In conclusion, the COVID-19 pandemic has highlighted the importance of reliable and comprehensive data to effectively prevent, monitor and manage the disease. Various challenges have been identified in data collection and information systems, including tracking and recording infor-mation, lack of timely access to medical records and inconsistencies in data elements. To address these issues and improve the quality and accessibility of health services, we developed an MDS specifically tailored to the needs of COVID-19 patients in Iran. The MDS aims to support integrated health services and offer comprehensive, valid and accessible information for better decision-making and future planning. By standardising data collection and incorporating essential demographic and clinical data, the MDS will contribute to enhancing healthcare quality and efficiency, ultimately supporting the healthcare system’s preparedness for potential outbreaks or similar public health emergencies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from the project with the ethics code IR.ABADANUMS.REC.1398.117 approved by Abadan faculty of medical sciences.