
Abstract
Background:
Low health literacy, low levels of positive belief and privacy and security concerns have been identified as a significant barrier to personal electronic health record uptake and use. An important tool for overcoming these barriers is the consumer-facing information which accompanies the system. My Health Record (MyHR) is the Australian national e-health record system, for which a large suite of online resources exists to facilitate consumer registration and use. This study uses a number of different measures of health resource quality to assess the MyHR online consumer-facing information and identify any gaps or areas for improvement.
Objective:
To analyse the quality and content of the online consumer-facing resources which support the uptake and use of MyHR.
Method:
Australian information resources aimed at healthcare consumers about the MyHR were included in this study. A comprehensive search using Internet search engines was conducted to locate all online consumer-facing resources about MyHR from both government and non-government sources. Readability (measured by Flesch–Kincaid grade level), year of publication/review, publishing organisation type, presentation style, linked websites, target audience, and themes were identified as important measures of health information quality, and these were recorded and reported on for each resource.
Results:
Eighty resources met the inclusion criteria. The mean Flesch–Kincaid grade level was 11.8. Most resources were created by Australian government sources (n = 55), and the most common target audience was the general public (n = 65). Registration (n = 51), privacy/security (n = 49), and benefits of use (n = 46) were the most common resource themes.
Conclusion:
The authors identified a number of gaps and areas for improvement in the provision of consumer-facing information about MyHR. Readability is too high for the general Australian population, and there are few translated resources, which means that the information provided does not cater to people with low literacy levels, communication disability, and/or difficulties in understanding written English. The target audiences for resources do not reflect priority groups that were identified during the MyHR development processes. There are also gaps in information provision about how consumers can use MyHR as a tool to meaningfully engage with health professionals and services to support their own person-centred care.
Keywords
Introduction
On 1 July 2012, Australia introduced a national e-health record system (Department of Health, 2016c). All Australians enrolled in Medicare or the Department of Veterans Affairs, and anyone seeking healthcare in Australia, were eligible to register and begin using the Personally Controlled Electronic Health Record (PCEHR) to share personal health information across approved healthcare providers (Department of Human Services, 2016). A review in December 2013 recommended 38 separate changes (Department of Health, 2013) including renaming the PCEHR to “My Health Record” (MyHR) (Department of Health, 2013: 19) and changing the legislation governing MyHR to allow a trial of an opt-out system for consumers (Department of Health, 2013: 28–29). These changes, among others, were put into effect through legislation passed in September 2015.
MyHR is described in information to consumers as a “digital summary of your health record” (Department of Health, 2016a). The benefits of MyHR are purported to be “getting the right treatment faster, safer and easier” (Department of Health, 2016a) by allowing “information to be shared online quickly and easily by the health-care provider organisations looking after you” (Department of Health, 2016a). Information for healthcare providers from MyHR website describes MyHR as “an electronic summary of your patient’s key health information, drawn from their existing records” (Department of Health, 2016b) with “the potential to deliver better care for patients and make the health-care system more efficient” (Department of Health, 2016b). Information is uploaded to an individual user’s MyHR from a number of sources: (i) registered health providers can upload a range of clinical documents; (ii) the government agencies of Medicare and the Pharmaceutical Benefits Scheme add information about episodes of care or prescribed medications; and (iii) registered users can add contact and personal details, current medications, allergies, an advance care planning document, organ donation decisions, and create a personal health note which could be used as a journal (Australian Digital Health Agency, 2016a). Information on an individual’s MyHR is accessible by the registered user, registered health professionals and the user’s nominated or authorised representatives (Australian Digital Health Agency, 2016a). While uptake of MyHR by health consumers, health providers and health organisations was initially slow (National E-Health Transition Authority, 2016), according to figures released by MyHR, by 23 October 2016 (Australian Digital Health Agency, 2016b), 4.3 million people (approximately 17% of the Australian population) and 9299 health provider organisations had registered for MyHR. Usage has reportedly been low (National E-Health Transition Authority, 2016) but is increasing, with a total of 1.14 million clinical documents being uploaded since July 2012 (Australian Digital Health Agency, 2016b).
Studies of consumer attitudes to the use of personal e-health records from countries other than Australia show that uptake by consumers may be influenced by several factors. Income, education, technology use and access and personal innovativeness in information technology were all influencing factors on uptake of personal electronic health records (Emani et al., 2012). Positive perceptions of relative advantage, ease of use and privacy and security lead to higher uptake of personal electronic health records (Dontje et al., 2014; Emani et al., 2012). Identified barriers to consumer uptake of personal electronic health records include low health literacy and difficulty interpreting complex medical information (Dontje et al., 2014), a lack of compatibility with existing e-services (Andrews et al., 2014), concerns about privacy and security (Andrews et al., 2014; Lehnbom et al., 2016) and low levels of positive beliefs (Lehnbom et al., 2016).
An important tool for increasing uptake and encouraging use of MyHR is the consumer-facing information created to educate and support people interested in using, or already registered for, MyHR. Information is available to consumers through general practices (GPs), Medicare offices and the MyHR website from the Australian Department of Health (Australian Digital Health Agency, 2016d). The MyHR website houses consumer-facing information produced by the Department of Health related to MyHR and a link to the MyGov website which houses the MyHR consumer registration portal. In addition, a number of other government departments and non-government organisations have created MyHR consumer resources—including digital resources, hard copy resources (also available electronically) and promotional videos.
The aim of this study was to analyse the information quality of the consumer-facing resources which support the uptake and use of MyHR through analysis of information resources available from the MyHR website (www.myhealthrecord.gov.au) and any other government and non-government online sources for a health literacy appreciation of the information according to its (a) readability, (b) currency, (c) information source, (d) target audience, (e) theme categories, (f) presentation style and (g) links between resources. This was done to determine barriers to and facilitators for use of MyHR related to the available online information from the MyHR website and other sources.
This examination of the information quality of the online consumer-facing MyHR resources is the first analysis within of a larger piece of work by this team into the use of MyHR by people with disabilities.
Method
In January 2016, an online search was conducted by the first two authors (LW and SH) for consumer-facing information regarding MyHR using Google and Bing search engines; the YouTube search function; and the search function on each National, State and Territory Health and Human Services Department website. YouTube was included in the search as it is used to house audiovisual materials related to MyHR. Although YouTube could also be considered an example of an interactive forum about MyHR, commenting on videos created by the Australian Government is not made possible on the Department of Health channel where the MyHR videos are stored.
The following search terms were used: PCEHR, Personally Controlled e-Health Record, e-Health, e-Health Record and MyHR. These terms were also searched alongside the name of each Primary Health Network (PHN) to ensure any MyHR information on PHN websites was captured. The first 20 pages of results from each search were examined for eligible resources. This approach was deemed suitable to capture all publically available information because (a) no results which met the inclusion criteria were being returned by the 20th page of any search and (b) this approach goes well beyond the literature on consumer approaches to Internet searches for health information, which has demonstrated that consumers, especially low literacy consumers, only click on one or two search results and rarely move off the first page of search results (Birru et al., 2004; Zhang, 2014). In addition to the search, all hyperlinks on all retrieved consumer-facing information were followed and the linked webpages checked for relevance, and any consumer-facing information with reference to MyHR was included in the search results. Search results were recorded in a Microsoft Excel database.
The inclusion criteria were Australian information resources aimed at healthcare recipients (i.e. consumers and/or carers or support workers) about the Australian MyHR by whatever name, developed by any government department or any non-government organisations. Websites or online resources were excluded if they provided information about other e-Health programs or platforms (with no MyHR content) or information about MyHR that was aimed at healthcare providers or MyHR program implementers and not aimed at consumers or carers. Research reports, media releases, media resources, legislation, submissions, reviews, opinion pieces and videos of lectures or presentations were also excluded.
Our search in January 2016 returned 99 resources meeting the inclusion criteria. After review of consumer information, it was decided that eight webpages from individual medical practices would be excluded as (a) these webpages provided minimal information about the MyHR and (b) only linked back to the MyHR website homepage. Thus, a total of 91 resources (text-based and video-based) were included in this review.
Following the initial search and exclusion, in early March 2016, the MyHR website and the available consumer information underwent a substantial revision, which included changes in preparation for the implementation of opt-out trials. This revision changed the website layout and reduced the amount of consumer information provided. Therefore, the search was repeated on 16 March, using the same search terms and strategy. This search returned a final total of 80 resources for inclusion in the review.
Several measures of resource quality were recorded for each resource, including readability, year of publication and review, publishing organisation type, presentation style, and linked websites and electronic resources. An inductive content analysis method of open coding, grouping of data and category creation as described by Elo and Kyngäs (2008), was used to categorise the resource themes and target audiences for each resource. This method also followed the content analysis method outlined by Alaszewski (2007) where, rather than categories being fixed, coding categories emerge during the investigation and comparison process of the documents being analysed. In content analysis, because researchers develop codes, categories and themes based on their subjective perspective and interpretation of data (Elo and Kyngäs, 2008), there is disagreement over the value and appropriateness of multiple researchers seeking consensus on the coding of categories (Graneheim and Lundman, 2004; Sandelowski, 1998). For this research, resource theme and target audience coding were conducted by one investigator (LW).
Measures
Readability
Readability was chosen as a measure of resource quality because previous studies of online health information have demonstrated that readability is often too high for people with low or average literacy (Cheng and Dunn, 2015; Cochrane et al., 2012; McInnes and Haglund, 2011). To assess readability, the Flesch–Kincaid grade level (Flesch, 1979) was calculated for each text-based resource, by copying and pasting the resource text into a Microsoft Word 2013 document and analysing the Flesch–Kincaid grade level through the readability statistics. The Flesch–Kincaid grade level was chosen because of its ease in application, because the result (grade level) is easy to understand, and it has shown correlation with other readability measures (Friedman and Hoffman-Goetz, 2006). Flesch–Kincaid grade level when calculated electronically has been shown to be less accurate than manual calculation, but these inaccuracies tend to produce underestimation, rather than overestimation, of grade level (Friedman and Hoffman-Goetz, 2006).
Due to document formatting, two pieces of written information were unable to be tested. Video resources were not tested for readability, even if they contained some written elements. In total, 74 written resources from the January 2016 search and 64 resources from the March 2016 search were assessed using the Flesch–Kincaid grade level.
Currency
The year of publication or most recent review was recorded for each resource. The currency of information has been identified as an important determinant of information quality, both by healthcare consumers (Marton, 2010) and healthcare providers (Roberts, 2010). In the context of a rapidly evolving and changing project, we have also inferred that resource currency may also reflect the engagement and interest of organisations in MyHR. That is, an organisation that keeps its resources on MyHR up to date could be viewed as engaged and interested in the MyHR process and conveying accurate information about MyHR to consumers, while an organisation that has not even made simple updates to its information (such as changing the name from PCEHR to MyHR) could be viewed as disengaged from the MyHR process.
Information source
Diviani et al. (2015) reported that website authorship and website credentials were identified as important evaluation criteria for online health information in a number of studies. Additionally, there are potential opportunities for organisations other than the Department of Health to provide their specific target audiences or communities with tailored information about MyHR. We have included publishing organisation type in our content analysis to examine where the online information about MyHR is coming from, and whether organisations other than MyHR are engaging in, or connecting their audiences to, the MyHR process through the development of their own MyHR resources.
After gathering the resources, four main categories of publishing organisation type were evident in the resources reviewed: Australian Government—MyHR website; Australian Government—other; PHN; and other (State and Territory government; non-government organisations; Medicare locals, industry peak bodies, credentialing agencies, and health consortia).
PHNs are primary healthcare organisations which work to understand health needs of their local communities, support GP to increase efficiency and efficacy of services and work to coordinate care across primary health providers and local hospital networks (Primary Health Care Research & Information Service, 2016). There are 31 PHNs across Australia, and they play an important role in assisting GP to adopt e-health initiatives (Primary Health Care Research & Information Service, 2016). Medicare locals served the same function but were restructured and replaced by PHNs on 1 July 2015 (Department of Health, 2015). “Medicare local” was included in the “other” category because MyHR resources remain accessible online with Medicare local branding.
Target audience
Target audience was included in this analysis to enable identification of potential gaps in information provision, especially for groups who are at risk of communication difficulties or have limited understanding of written English. Additionally, including target audience in this content analysis enables examination of how well MyHR is meeting the online information needs of their own priority groups of consumers as identified in the Concept of Operations Relating to the Introduction of a Personally Controlled Electronic Health Record System (“Concept of Operations”) published by the Australian Department of Health and Ageing (2011). The Concept of Operations identified people with complex and chronic conditions, older Australians, Aboriginal and Torres Strait Islander people, mothers and their newborn children, people with mental health conditions, people with disabilities and people living in rural or remote communities as priority groups for registration (Australian Department of Health and Ageing, 2011).
Intended audience was coded by reviewing each document and recording mentions of, or information directed at, different audience types. Where no mention was made of a specific target audience, the audience type was recorded as “general public”. Resources which mentioned more than one audience type were recorded against each audience. The audience types identified were general public, carers, authorised/nominated representatives, parents of infants/toddlers; parents, adolescents, older people, veterans, people with chronic conditions, Aboriginal and Torres Strait Islanders, people with mental health conditions, people from culturally and linguistically diverse (CALD) communities, opt-out trial sites, health providers (if resources targeted both consumers and health providers) and other (MyHR implementers, health organisations, people with low vision (n = 1), people with hearing impairment/communication difficulties (n = 1) and people in aged care facilities (n = 1)).
Theme categories
Resource theme categories were assessed by reviewing each resource and using open coding to categorise the key information or topics within the resource. This process returned a large number of topics, which were then further coded into seven theme categories: benefits, registration, post-registration use, use of representatives, privacy/security, relationships with health providers, dispute resolution, and opt-out trial sites. All resources returned multiple topics and themes. Two resources were coded in two theme categories – “Access controls” (privacy/security and post-registration use) and “How to correct mistakes in the record” (post-registration use and relationships with health providers).
Presentation style
Presentation style was coded according to text-based and video-based categories. Presentation style can demonstrate adaptation to different audiences (e.g. video and audio resources may increase engagement, especially for low literacy audiences (US Department of Health and Human Services and Office of Disease Prevention and Health Promotion, 2015)).
Links between resources
Links between resources were recorded and followed. One advantage of presenting health information online is the chance to layer information and connect information and sources, which allows users to direct their own learning to a level of proficiency and interest that suits their needs and skills (Lawless and Brown, 1997). Linking resources online provides an opportunity for users to control their own learning and explore content in a nonlinear way, which may produce more effective learning outcomes than more traditional, creator-directed and linear presentations of information (Lawless and Brown, 1997).
It is important to note that the two searches were conducted before the closure of the National e-Health Transition Authority and the establishment of the current MyHR system operator, the Australian Digital Health Agency (www.digitalhealth.gov.au). Since the establishment of the Australian Digital Health Agency in July 2016, there have been further developments of the system and its supporting information. The results presented therefore reflect a snapshot in time of an evolving system, and the authors believe that having this historical snapshot and a method for analysis available in the literature could help inform deliberate design of more accessible consumer-facing information for both MyHR and other personal electronic health record platforms into the future.
Results
In this section, we report the results from the March 2016 search and note where the results differ from the January 2016 search.
Readability
The 64 resources tested from the March 2016 search returned a mean Flesch–Kincaid grade level score of 11.8 (SD = 2.6), with only 11 resources scoring between grades 7 and 9 and 1 resource scoring <6. Flesch–Kincaid grade levels between 7 and 9 are considered “plain English” writing and are readable by the majority of people, while documents which score <6 are considered to cater for people with low levels of English literacy (Flesch, 1979). The mean Flesch–Kincaid grade level score for resources tested from the January search (n = 73) was 11.7 (SD = 2.5), and the numbers of “plain English” and “low literacy” resources were unchanged between January and March. Thus, despite the changes to the consumer information and the MyHR website between January and March 2016, there were no improvements evident in the readability score of resources.
Currency
The results for year of publication/last review of the 80 resources from the March 2016 search were 2011 (n = 3), 2012 (n = 6), 2013 (n = 7), 2014 (n = 17), 2015 (n = 8), 2016 (n = 33) and unstated (n = 6).
Information source
Of the 80 resources retrieved from the March 2016 search, 23 were published on the MyHR website, 22 were published on other Australian government websites and 12 were published on PHN websites. Twenty-three resources were published in a variety of other locations including State and Territory government (n = 8), non-government organisation (n = 6), Medicare local (n = 3), credentialing agency (n = 2), health consortia (n = 2), industry peak body (n = 1) and private health provider (n = 1) websites.
Intended audience
The intended audience for resources included in this review is summarised in Table 1.
Intended audience of included resources from the March 2016 search.
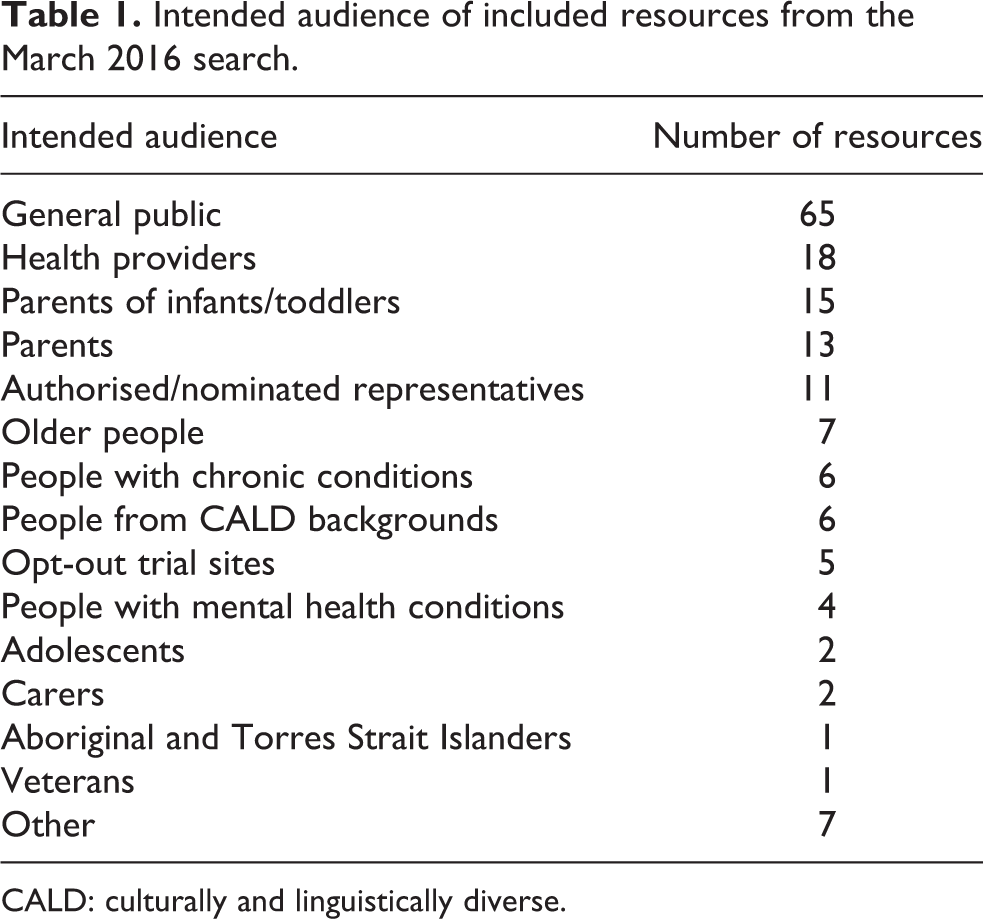
CALD: culturally and linguistically diverse.
Most resources (n = 52) had multiple target audiences (ranging from 2 to 6 target audience types). In the March 2016 search, few resources, with the exception of information relating to parents or to opt-out trial sites, explicitly identified a target audience. In comparison, in January 2016, MyHR housed consumer-facing information which explicitly directed resources at parents, older people, veterans, people with chronic conditions, people with mental health conditions and Aboriginal and Torres Strait Islanders (i.e. the names of the target audience were included in the resource title). By March 2016, these targeted consumer-facing information resources produced by MyHR were no longer publically available. Additionally, neither search uncovered any resources aimed at people with disabilities or people from rural and remote communities, two groups which were identified as priority populations in the Concept of Operations (Australian Department of Health and Ageing, 2011).
Other notable changes relating to target audience in the resources provided for consumers about MyHR between January 2016 and March 2016 were The target group “mothers and their newborn children,” as identified in the Concept of Operations, were now included in “parent” resources. “Carer” resources were reduced from 11 to 2. “Parents” resources were increased from 4 to 13. Five new opt-out trial site-specific resources were found.
There are very few translated resources available. In the January 2016 search, the only translated resources available regarding MyHR were produced by NPS MedicineWise and were inaccessible from the MyHR website. In the March search, basic registration information was available in seven languages (Italian, German, Arabic, Yumplatok, Tagalog, Spanish and Japanese) as part of a suite of resources produced for the opt-out trials.
Resource theme categories
All resources were categorised by resource theme and almost all resources incorporated more than one theme. The coding of research subjects into theme categories can be seen in Table 2. The themes of resources included in this review are summarised in Table 3.
Categorisation of consumer resource topics by theme.
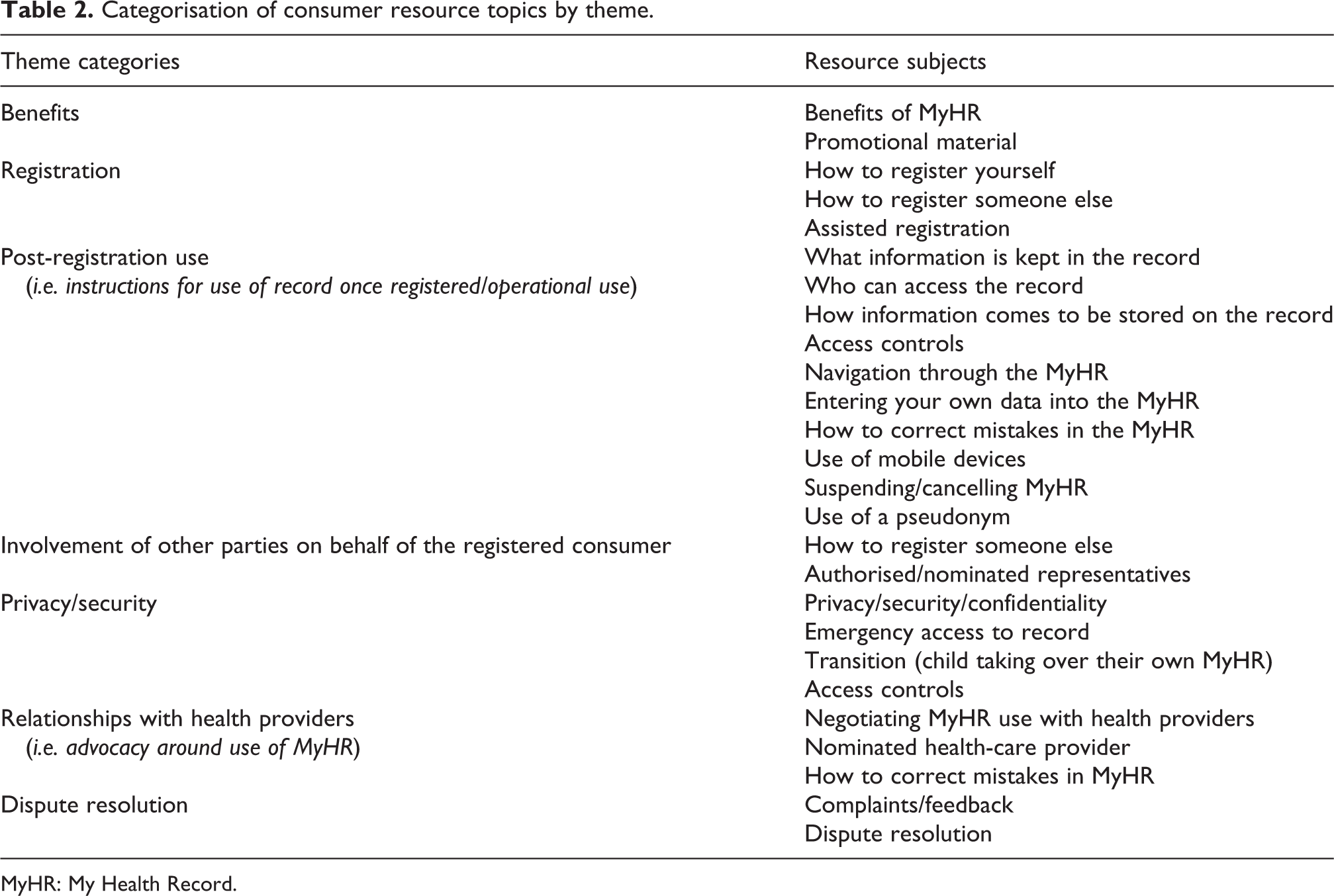
MyHR: My Health Record.
Themes of the included resources from the March 2016 search.
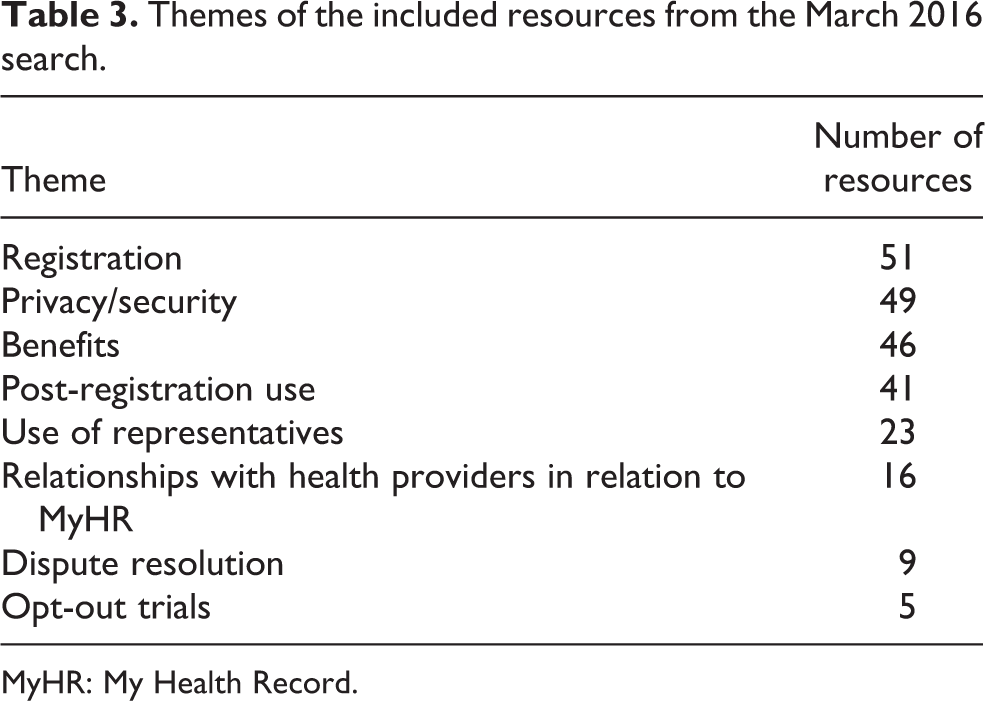
MyHR: My Health Record.
Presentation style
Presentation style was categorised into text-based or video-based resources. There were no purely audio resources or resources with high levels of interactivity (e.g. games and quizzes). Apart from videos on YouTube, there were no social media channels aimed at healthcare consumers. Of the 80 resources retrieved in the March 2016 search, 64 were text-based (46 web-only, 18 also available in Portable Document Format for hard copy printing) and 16 were videos.
The text-based resources rarely included visual content to help illustrate the text. Screenshots of MyHR beyond the registration page were only available in two resources, neither of which was accessible through the MyHR website. While MyHR has extensive “help” pages which include annotated screenshots to assist navigation and use of the record, these are accessible only after registration. There were no audio options for any of the text-based resources and no ability to easily change font size or contrast on any of the websites to assist people with low vision.
Of the 16 videos, most were focused only on registration and the benefits of MyHR with little practical information about how to use the record as a meaningful aspect of health care.
Finally, at the time of writing, there is currently no interactive content (e.g. games, “sandboxes” and quizzes) to allow users to experience using and navigating through the MyHR before committing to registration.
Links between resources
Links between resources were noted during the resource review. “Links” included hyperlinks and ways to seek information through non-electronic means (telephone helpline and visit Medicare office).
Health organisations were encouraged by the National E-Health Transition Authority (now Australian Digital Health Agency) to promote MyHR and link to the MyHR website (Australian Digital Health Agency, 2016c). However, we observed that MyHR rarely provides links to other information websites or resources, suggesting that the promotion is in one direction. In the January 2016 search, there were no external links from MyHR to other sites, including other government departments. In the March 2016 search, five MyHR resources provided links to non-MyHR government websites (e.g. Department of Human Services, Office of the Australian Information Commissioner and the National Relay Service). In comparison, all non-MyHR resources included in this study provided links back to the MyHR website and/or instructions for telephone or face-to-face registration.
Discussion
Considering the large volume of consumer-facing information available about MyHR, both through the MyHR website and from other sources, this analysis has identified several important aspects of the quality of MyHR information available to consumers. In the absence of previous research on the impact of the public-facing information online on MyHR upon uptake or use, it is not yet known if the consumer-facing information examined in this study has impacted on, or will further impact upon, the uptake, use and benefit of MyHR. However, it is important to consider the results of this study to identify where revisions could be made to improve the information on MyHR that is aimed at consumers and particularly to priority groups.
This analysis has revealed that, at a mean Flesch–Kincaid grade level of 11.8, readability levels of MyHR resources are generally higher than recommended levels for “low literacy” and “plain English” resources (Flesch, 1979). These readability problems remained unchanged despite a significant revision of the consumer information available on the MyHR website. Only “An Easier Way to Share Your Health Information” from NPS MedicineWise (National Prescribing Service, 2012) meets the readability criteria for a low literacy resource, and this resource is not accessible through the MyHR website. Given that the 2011–2012 Programme for the International Assessment of Adult Competencies showed that 13.7% of the Australia population scored at level 1 or below for English literacy and 44% of the population scored at level 2 or below (Australian Bureau of Statistics, 2013), the provision of low literacy and plain English resources is essential to improve the accessibility of the MyHR consumer-facing information, not just for people who have communication disability or difficulties in understanding written English but for a significant proportion of Australia’s general population.
As well as a lack of plain English and low literacy resources, there are very few translated resources available. If we consider both the translated information from MyHR produced as part of the opt-out trials and the translated information available from NPS MedicineWise, then there is currently basic MyHR registration information available in nine languages: Arabic, Chinese, Greek, Italian, German, Tagalog, Japanese, Spanish and Yumplatok. While seven of these nine languages are also in the top nine languages other than English spoken in Australia (Australian Bureau of Statistics, 2016), no translations for MyHR are available in either Vietnamese (fifth most common language other than English) or Hindi (eighth most common) (Australian Bureau of Statistics, 2016). It should be noted that there are no translated video resources available and there are no translated resources which provide information about MyHR beyond basic registration instructions. Given that nearly 4 million people in Australia (approximately 18% of the Australian population) speak a language other than, or in addition to, English (Australian Bureau of Statistics, 2016), providing a good range of written and audio/video translated resources, including resources that address MyHR information needs beyond basic registration instructions, is potentially one way to increase information access of MyHR.
In addition to low readability and lack of translated materials, this analysis has demonstrated the limited range of presentation styles of the resources which may also negatively impact information access for vulnerable groups who are more at risk of communication difficulties and who have difficulties in understanding written English. The majority of online resources are text-based and not supported by graphics, audio options or interactive content. The available video content is very basic and focuses on registration and benefits rather than meaningful use of MyHR as a tool to manage healthcare. Additionally, none of the video resources are provided in languages other than English. While it must be acknowledged that MyHR does provide consumer with both telephone and face-to-face support, the online content that users of MyHR can seek out independently should be presented in a variety of formats to increase resource accessibility to a wider range of audiences. This includes making MyHR resources accessible for people who are at risk of experiencing communication difficulties – including people with sensory, physical or intellectual disability; people from CALD backgrounds; Aboriginal and Torres Strait Islanders; older people; and people experiencing low socio-economic status. The provision of more video and audio content in a variety of languages, plus taking advantage of the interactive potential of the online space to create game-style resources or “sandbox” testing environments that allow experience of MyHR without the commitment of registration, might assist in translating the information beyond text and into formats which improve comprehension of the materials by a much wider audience.
Only 12 of the resources included in this study were created and published by nongovernment sources. While there has been some commentary about MyHR from consumer groups (Consumer Health Forum, 2014; Frommer, 2012), no disability or chronic illness advocacy or research organisations have produced consumer-facing information for their client groups about how to access and use MyHR, and our review shows that the availability of information for consumers is inconsistent across government agencies. We found no consumer-facing information about MyHR on state government websites from Tasmania, Victoria or Western Australia, and only 11 of the 31 PHNs include consumer-facing information about MyHR on their websites. There are opportunities for PHNs and State and Territory Governments to be more involved in promoting the MyHR to their local audiences and advocating for uptake of MyHR by the health services in their purview. Nongovernment organisations, especially condition-specific organisations and those with a focus on consumer participation in health, could have a large role to play in developing their own tailored information for their consumer audience or advocating for resource development by MyHR which meets their consumers’ needs. There are also opportunities for MyHR to capitalise on the work already done by some other agencies by providing more links to MyHR information available outside the MyHR website.
This review identified that several MyHR resources are aimed at multiple audiences but that there remain gaps in provision of information for some groups. More resources are needed for adolescents and young adults, especially considering the specific rules around ownership of the record and changes to available information from the time someone turns 14 (Office of the Australian Information Commissioner, 2016). Publishing or linking resources with good readability that are aimed at adolescents (Office of the Australian Information Commissioner, 2016), and linked to the MyHR website, might increase the accessibility of the information for adolescent audiences. Increasing the number of translated materials that are also linked to MyHR website could improve information access on MyHR for CALD groups. Materials aimed at priority groups nominated in the Concept of Operations (Australian Department of Health and Ageing, 2011) are urgently needed. The fact that people in opt-out trial areas have access to translated resources about MyHR is recognition that consumer-facing information for priority groups could impact on the outcomes of the trials. Further research is needed to evaluate the impact of these materials and future extension of these resources to more languages other than English, and more extensive information about MyHR is required.
In relation to MyHR resources for consumers, the information contained in the resources is detailed, particularly in relation to privacy and security, MyHR benefits and registration instructions. The amount of information on registration might reflect the current focus on getting users into the MyHR system, since benefits of the MyHR are expected only when used by the majority of the population. However, there is currently little information about use of MyHR post-registration in healthcare contexts – either in an operational sense (e.g. navigation, trouble shooting, complaints/dispute resolution) or in a strategic sense (e.g. convincing or persuading one’s health professionals to engage in using MyHR, user rights, knowing how MyHR fits in with other systems including the GP’s own medical record system). There is no information aimed at consumers to advise on ways to integrate the MyHR in their own self-advocacy or person-centred involvement in healthcare. Such information could be particularly helpful for consumers who wish to use the system but whose healthcare providers are not yet using the system. Increasing consumer-facing information about how the system works post-registration has the potential to positively impact consumer trust in MyHR and also support improvements in “person-centred healthcare” or “consumer-driven healthcare”. The practicalities and the benefits of post-registration use must be made clearer in the consumer-facing information about MyHR if consumers are to make an informed choice about registration and use.
Several opportunities exist to increase the consumer use of MyHR, if MyHR and other organisations produce accessible online consumer-facing information that addresses both facilitators and barriers to the use of the MyHR that are appearing in anecdotal reports and emerging in the literature. Recent studies (Andrews et al., 2014; Lehnbom et al., 2016) have shown that privacy and security concerns, ease of use, negative beliefs and lack of integration with existing systems are important barriers to MyHR use. While many of the current consumer-facing resources address privacy and security concerns and advertise the benefits of MyHR, our research has shown that the readability, format, and location of resources often render the information inaccessible to potential target audiences and priority groups. As identified by Hemsley et al. (2017), people at risk of communication difficulty and/or disability may be restricted in their ability to meaningfully use MyHR by making full use of the personal control features, accessing shared information and uploading their own information. Increasing the readability and range of formats available for the information that directly addresses concerns raised in the literature could increase the engagement of priority groups with MyHR and their ability to meaningfully use the record to manage their healthcare.
Limitations and directions for future research
This review of online consumer-facing information about MyHR did not include either paper-based or in-person (e.g. telephone helpline or Medicare offices) information materials. The authors acknowledge that paper-based or in-person information sources may include further or different resources and content, including low literacy materials or targeted materials for priority groups.
Additionally, the MyHR, in its operational and policy context, is a rapidly changing form of health information management. There have been recent changes to the information on, and layout of, the MyHR website, and our study represents only a “snapshot” in time of an evolving system. Furthermore, our study was conducted during a period of change, with changes in the legislation, the name change to MyHR and the implementation of opt-out trials. Therefore, we anticipate that consumer-facing information will continue to change with the rollout and evaluation of opt-out trials, and increased uptake of the MyHR, and we hope that this analysis helps to inform some of that future change.
This study examined the content of information resources against a number of measures of information quality. While information quality is one factor which may impact MyHR uptake, “ease of use” is also an important determinant of personal electronic health record use (Dontje et al., 2014; Emani et al., 2012). A future study will analyse the usability of MyHR and how usability may positively or negatively impact consumer uptake.
Further research about online MyHR information needs is needed to examine (i) the online information about MyHR following implementation of the opt-out trials in New South Wales and Queensland to determine any further improvements necessary to increase the accessibility of information (e.g. variety of formats, ease of reading and translations) for both the general population and priority groups; (ii) perceptions of healthcare consumers in priority groups about the accessibility of the information on the MyHR website and its usability; (iii) engagement of non-government organisations in creating materials to support information access about MyHR, particularly beyond the registration phase, to inform healthcare consumers in their services about using MyHR with healthcare providers; and (iv) ways that self-advocacy groups and self-advocates are engaging with information about MyHR, with any necessary supports from service provider or family members.
Conclusion
While the content available online about MyHR is relatively comprehensive, some key elements of the consumer-facing information must be improved to increase accessibility to priority groups and people who experience communication difficulties and difficulty in understanding written English. Improving the readability of MyHR materials online, providing more information in a greater number of languages, developing targeted resources for all identified priority groups and increasing links between resources are some practical strategies that the Australian Government should implement to improve the quality of the available consumer-facing information on the MyHR website. Providing information about “strategic,” rather than just “operational,” use of the record – for example, how consumers can integrate MyHR into person-centred care and self-advocacy approaches – may also facilitate uptake and use of MyHR by demonstrating the potential value of the record in improving healthcare interactions.
Consumer associations (e.g. representing people in diverse cultural groups, with disabilities, or specific health conditions) and non-government organisations (e.g. disability service providers) also have an important role to play in developing information about the MyHR that is specific to their consumer audiences. These organisations are in an ideal position to advocate for ways of using MyHR which best meets the needs of their communities; however, to date, few have produced MyHR information for consumers. The results of this study could be used to (a) improve the MyHR online information provided by government departments, (b) help non-government organisations identify important components to consider when creating online health information about MyHR and (c) inform future collaboration across sectors and service providers on ways to fill the existing gaps in information available online about MyHR for priority groups.
Footnotes
Acknowledgements
The authors would like to acknowledge Andrew Ingersoll and Dane Manning from the Australian Digital Health Agency for providing feedback regarding the terminology and timelines of the operation of My Health Record.
Authors’ contributions
LW conducted the search and content analysis and was a major contributor in writing the manuscript. SH assisted with the search and content analysis and was a major contributor in writing the manuscript. BH was a major contributor in writing the manuscript. AG, SB, BK, IH, MA, and SM all reviewed and commented on multiple drafts of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was funded in part by a project grant of the National Health and Medical Research Council of Australia.