
Abstract
Background:
Fibrodysplasia ossificans progressiva (FOP) is an ultra-rare, disabling, genetic disorder characterized by progressive heterotopic ossification (HO). FOP care pathways are complex, and there are many underrepresented patients globally.
Objectives:
This scoping review aimed to identify global FOP case reports and investigate real-world management practices.
Evidence sources, eligibility criteria, and charting methods:
International/local databases and congress proceedings were searched. Publications reporting patient-level data for ⩾1 patient with an FOP primary diagnosis, published January 2000–January 2024, were eligible. Publication details, patient demographics, disease presentation, and care pathway were extracted. Data were charted through categorization of themes and frequency analyses.
Results:
Of 6064 publications screened, 369 were eligible, reporting on 541 patients with FOP. Most publications (82.4% (304/369)) reported an individual case; the remaining reported 2–25 cases. Cases were from 57 countries, most commonly in the Asia/Pacific region (47.0% (254/541)). Most patients had reportedly seen a single specialist (64.8% (59/91)), and care from multidisciplinary teams was reported for only 5.5% (5/91). HO (84.7% (458/541)) and great toe malformations (66.7% (361/541)) were the most commonly reported signs, though mobility limitations (46.2% (96/208)) and growths/lesions (38.5% (80/208)) were most common before diagnosis. The predominant drug classes reported for FOP treatment were corticosteroids (52.6% (102/194)) and nonsteroidal anti-inflammatory drugs (39.7% (77/194)). Surgeries were reported in 35.1% (190/541) of patients. Where specified, the most common surgery types were malformation correction/bone resection (43.6% (78/179)) and biopsies (34.1% (61/179)).
Conclusion:
This scoping review synthesized valuable real-world insights from case reports of FOP, potentially supporting outreach initiatives in underserved regions and facilitating shared learnings on diagnosis and treatment. Although the inherent selection bias of case studies toward atypical cases limits definitive conclusions, some global trends in the clinical management practices were revealed.
Plain language summary
Fibrodysplasia ossificans progressiva (FOP) is an ultra-rare genetic disease. As extra bone forms in places where it is not normally found, patients with FOP become physically disabled over time. While there are treatment guidelines, patients experience different symptoms and levels of disability. Doctors must therefore tailor treatment decisions for each patient and share their experiences to maximize quality of care. In this study, major literature databases were reviewed to find case studies of patients with FOP published worldwide between January 2000 and January 2024, and to explore how their care was managed. There were 369 case studies found, describing 541 patients from 57 countries. As FOP affects multiple body systems, the International Clinical Council on FOP’s Treatment Guidelines recommend that patients should be managed by a team of specialists. However, most case studies reported care by just one type of specialist. Regarding medications, many case studies reported those listed in the FOP Guidelines, including steroids and anti-inflammatory drugs. The FOP Guidelines recommend avoiding surgery to remove extra bone as it can worsen symptoms, yet 3.5 patients in 10 had a surgical procedure. Surgeries often resulted in abnormal bone growth. By collating global case reports, this review could connect patients and their doctors with the wider FOP community to help share experiences. However, case studies are not a complete history of a patient’s care and authors often focus on uncommon cases. Therefore, this review should only inform care practices in combination with accepted treatment guidelines, clinical trials, and physicians’ clinical experience.
Introduction
Fibrodysplasia ossificans progressiva (FOP; Online Mendelian Inheritance in Man [OMIM] #135100) is an ultra-rare, profoundly debilitating, genetic disorder with an estimated prevalence of 1.36 per million individuals (range: 0.036–1.428 per million individuals).1–3 Patients with FOP experience heterotopic ossification (HO), the irreversible transformation of soft and connective tissues into extra bone throughout the body and across joints.1,4 FOP is caused by spontaneous missense pathogenic variants in the Activin A Receptor Type 1 (ACVR1/Activin Receptor-Like Kinase 2 (ALK2)) gene, most commonly ACVR1R206H.5,6 The ACVR1R206H variant confers mild constitutive activity and enhanced ligand sensitivity to the ACVR1/ALK2 receptor, increases the activity of the ACVR1/ALK2 receptor after bone morphogenetic protein (BMP) binding, and alters the response to Activin A, leading to the activation of the BMP signaling pathway and dysregulated transcription of genes involved in bone formation.5–7 Patients with ACVR1R206H typically present with congenital skeletal malformations, including bilateral malformations of the great toes (hallux valgus) and progressive HO in childhood. Progression of HO can often occur in specific anatomic patterns, following trauma or spontaneously, with intermittent painful episodes of connective tissue swelling, known as flare-ups.8,9 The irreversible development of HO throughout the body progressively restricts movement, leading to cumulative disability, reduced quality of life (QoL), and shortened life expectancy for patients with FOP.10,11
The International Clinical Council (ICC) on FOP brought together expert clinicians to guide the optimal management of FOP. 12 While more targeted therapeutic options may become available in the near future, current care for most patients with FOP is mainly supportive and is limited to flare-up prevention and symptom management, including etiology-based pain relief.7,12 The ICC’s FOP Treatment Guidelines recommend the use of corticosteroids to prevent and treat flare-ups, while also recognizing the anecdotal benefits of alternative treatment classes such as nonsteroidal anti-inflammatory drugs (NSAIDs) and bisphosphonates to manage ongoing disease progression and disease-related symptoms.7,12 Potent medications that manage inflammation, such as selective tyrosine/Janus kinase inhibitors and anti-interleukin 1 (IL1) therapies, may reduce or ameliorate flare-ups; their off-label use is only recommended for patients with FOP who have refractory, severe flare-ups that have not responded to standard of care.12–15 Off-label treatments such as antimicrobials, immunosuppressants, and antiangiogenic agents have also been tried to help manage multi-systemic manifestations of FOP.16–18
Within the evolving FOP treatment landscape, palovarotene was the first treatment shown to reduce new HO.19,20 Palovarotene is an orally bioavailable retinoic acid receptor gamma (RARγ)-agonist that downregulates BMP pathway signaling to limit new bone formation. Palovarotene has been approved for the reduction of new HO in adult and pediatric patients with FOP aged ⩾8 years for females and ⩾10 years for males by the Australian Therapeutic Goods Administration (TGA), Health Canada, the Russian Federal Service for Surveillance in Healthcare (Roszdravnadzor), and the US Food and Drug Administration (FDA); however, the European Medicines Agency (EMA) did not approve the marketing authorization.21–25 Post hoc analyses of data from the phase III MOVE trial (NCT03312634) showed that mean annualized new HO volume was 54% lower in patients treated with palovarotene, compared with untreated participants in an FOP natural history study (NCT02322255). In addition to common retinoid-class side effects, the most notable adverse event reported in MOVE was an increased risk of premature physeal closure in skeletally immature palovarotene-treated patients. 20
Beyond pharmacological treatments, the ICC’s FOP Treatment Guidelines state that elective surgical and invasive procedures should be avoided in patients with FOP, due to a high risk of inciting flare-ups and rapidly progressing HO associated with soft-tissue trauma.12,26,27 There are some exceptions in which surgery should be considered, for example, in emergency care and minor surgeries that can improve QoL. When surgery is required, precautions should be taken to minimize adverse outcomes, such as pretreatment with corticosteroids and careful positioning of the patient during surgery.12,28
Despite the existence of guidelines for the management and treatment of FOP, the unpredictable nature of the disease and variation in patients’ symptoms mean that final individualized treatment decisions rest with the physicians and their patients. 12 Consequently, real-world management practices for FOP may vary between treating physicians. Certain interventions, such as those selected based on initial misdiagnoses given to many patients with FOP (e.g., cancer), can trigger flare-ups and/or irreversible disease progression. 26 Therefore, it is imperative that treating physicians are connected with the FOP community to share learnings and best practices.1,29 There is a multitude of undiagnosed, underserved, and underrepresented patients living with FOP, as evidenced by a mismatch in the number of patients affiliated with FOP organizations in many well-served and underserved countries, and the estimated global prevalence of FOP.1–3 Based on a global population of 8.2 billion, 30 the total number of cases globally could be up to around 11,000, though previously published estimates are between 2,600 and 4,000 patients.1,2 Despite this, to date, only 834 patients with clinically confirmed FOP are registered or associated with a regional, national, or international FOP organization. 1 This suggests there is a large population of patients with FOP, perhaps in underserved regions like Africa, South America, and Asia/Pacific, who lack access to the support and guidance available through the international FOP community. 1
To elucidate the areas of clinical practice where outreach from the international FOP community and sharing of learnings would be beneficial, an understanding of how FOP management and care pathways vary globally is needed. Case study publications identified through literature reviews can provide valuable insights into rare diseases.31–38 The synthesis and analysis of patient-level information can help identify trends and heterogeneity in treatments and patient pathways, temporally and geographically. This is particularly important for rare diseases, where identifying and studying large cohorts of patients is usually not possible. A scoping review was therefore conducted by identifying and synthesizing global case reports of FOP, providing a critically needed comprehensive analysis of FOP management and care pathways from across the world. It was envisioned that this study could aid in building the international FOP community by geographically locating individual patients and their treating physicians and revealing global trends in FOP management to elucidate areas of best practice where the mutual sharing of learnings would be valuable.
Methods
This scoping review is reported as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) Checklist. 39
Search strategy
Targeted searches of major electronic publication databases were undertaken to identify case reports or case series describing one or more patients with FOP for whom patient-level data were reported. Searches were conducted in accordance with a pre-specified protocol (see Supplemental Tables 1–5) and PRISMA guidelines. 40 A combination of international and local literature databases was searched, including MEDLINE, Embase, CNKI and CMAPH (Chinese), Ichushi-Web (Japanese), and RISS (Korean) (see Supplemental Table 1). Online information sources (see Supplemental Table 2) and relevant congress proceedings that took place between 2010 and 2020 (see Supplemental Table 3) were also searched. Each database was queried with search terms appropriate for its search functionality (e.g., Boolean operators were used where possible) and the specificity of the database.
Original searches were limited to studies published between January 2000 and May 2020. Subsequent updates were then conducted to capture case reports more recently published between May 2020 and January 2024 (Supplemental Figure 1). As searches of congress proceedings and online information sources yielded few results in the original searches, such searches were not conducted for the subsequent updates.
Eligibility criteria
PICOS criteria (P: population, I: intervention, C: comparator, O: outcomes, and S: study design) were used to determine article eligibility (see Supplemental Table 4 for full eligibility criteria). Briefly, articles in a pre-specified list of nine languages (Chinese Mandarin, English, French, German, Italian, Japanese, Korean, Portuguese, and Spanish) were eligible for inclusion if they reported patient-level data for one or more patients who had received a primary diagnosis of FOP, as reported by publication authors, irrespective of the methods used for diagnosis. Articles reporting on autopsy findings in patients with a primary diagnosis of FOP were included (Supplemental Methods). All articles were screened by a single reviewer against the pre-specified eligibility criteria. Reviewers had experience in literature reviews and were either fluent or had a high level of proficiency in the relevant language.
Data charting and analyses
Relevant data from case reports were extracted into a pre-determined Microsoft Excel® extraction grid. Details were extracted only as specified in the case report publications, with no inferences or assumptions made by reviewers; for example, HO was only extracted when specified as such in the publication, not inferred from reports of “growth,” “lesion,” “mass,” or “nodule.” Information extracted included the following: publication details, patient characteristics, disease characteristics, and the patient pathway of care (full list in Supplemental Table 5). Data extraction was performed in English by a single individual with experience in literature reviews who was fluent, or with a high level of proficiency, in the relevant publication language; any uncertainties were reviewed by a second individual.
A de-duplication step was conducted to identify articles that described the same patient. This step was carried out by looking for any direct reference made to a previous case report, or by matching the author lists; this was verified by confirming matching patient information. Information on the same patient was then combined.
Qualitative data were manually grouped into the most appropriate categories to facilitate descriptive analysis and identify trends (Supplemental Methods). Categorical data were summarized as frequencies and percentages. Descriptive analyses were performed to identify trends across case reports, for example, by geographical region, time period, or genetic variant. Variables were stratified by the following categories: medical departments and specialist referrals/consultations by country; signs related to the skeletal system by genetic variant; tests and assessments by pre- or post-diagnosis; treatment classes by country and publication year; surgical procedures by pre- or post-diagnosis, country, and publication year (Supplemental Methods).
Results
Search results
Overall, a total of 6064 publications were screened, of which 369 (6.1%) publications were eligible for extraction (Supplemental Figure 1). The majority of articles excluded were duplicates or did not report on a patient with a primary diagnosis of FOP or were not case reports. Most eligible publications (82.4% (304/369)) reported on an individual case of FOP, with the rest reporting between 2 and 25 cases.
Patient characteristics
In total, case reports on 541 patients with FOP were identified in this scoping review; 7 of these cases were autopsies.41–43 A similar proportion of patients were male (47.9% (259/541)) and female (49.7% (269/541)); no patients were reported as non-binary, and sex was not reported for 2.4% of patients (13/541). Age was reported for 506 patients at varying clinical and non-clinical milestones (Table 1), ranging from 0 months (birth) to 72 years of age. A summary of patient characteristics is presented in Table 1, provided at the individual patient level in Supplemental Table 6.
Characteristics of patients with FOP included within case reports.

Mean age/age groups reported here include patients for whom age at the time of the following key clinical and non-clinical milestones was reported: age at presentation, diagnosis, symptom onset, publication, referral, and pharmacological or surgical management. Patients for whom milestones deemed least relevant to the care pathway were reported (age at the time of pregnancy, age at the time of death, and age at the time of autopsy) were not included.
FOP, fibrodysplasia ossificans progressiva; NR, not reported.
Cases were spread across 57 countries, with patients most commonly cared for in China (13.3% (72/540)), the United States (12.4% (67/540)), India (9.8% (53/540)), and Japan (9.1% (49/540)) (Figure 1); country of management could not be identified in one case report. 44 The region with the highest number of published cases was Asia/Pacific, followed by Western Europe, North America, Latin America, Africa, Eastern Europe, and Oceania.

Number of case reports by country (N = 541).
An ACVR1 pathogenic variant was reported for 39.7% (215/541) of patients. Of cases where the specific point-mutation of the variant in the ACVR1 gene was reported (189/215), 81.5% (154/189) specified the most common ACVR1R206H variant. Other non-canonical ACVR1 variants reported in multiple cases included R375P (n = 8), R258S (n = 3), G356D (n = 3), G328E (n = 2), G328R (n = 2), and Q207E (n = 2). For variants reported in one case each (n = 5), see Supplemental Table 7; the amino acid substitution was not specified in 10 cases.
Disease presentation
Signs prior to diagnosis
Signs that presented prior to a diagnosis of FOP were reported for 38.4% (208/541) of patients. The most commonly reported signs prior to diagnosis included mobility limitations (46.2% (96/208)) and growths/lesions (38.5% (80/208)). The classic signs of great toe malformations and HO were reported in 29.3% (61/208) and 23.1% (48/208) of cases, respectively, prior to diagnosis (Table 2).
Signs of FOP pre-diagnosis.

Pre-diagnosis signs reported in <5.0% patients included: tumor (3.8%, n = 8); calcifications, dental-related (each 2.9%, n = 6); respiratory-related (2.4%, n = 5); special senses-related (including signs related to sight, hearing, smell, taste, and touch), digit malformations (each 1.9%, n = 4); fracture, gastric symptoms, integumentary-related (each 1.4%, n = 3); biochemical changes, congenital abnormality (each 1.0%, n = 2); altered voice, arthritis, choroid plexus proliferation, contused back, cyst, fatigue, fibroblastic proliferation, hernia, hormone-related disease, mucoid change, premature delivery, seizure (each 0.5%, n = 1). Pre-diagnosis signs were not reported for 333 (61.6%) patients.
FOP, fibrodysplasia ossificans progressiva; HO, heterotopic ossification.
Signs related to the skeletal system
Of all signs reported in the absence of pharmacological or surgical management (pre- or post-diagnosis), the classic clinical features of FOP were most common. Specifically, HO was reported in 84.7% (458/541) of patients, and great toe malformations in 66.7% (361/541) of patients. Other reported signs included impaired mobility (53.6% (290/541)), stiff neck (41.4% (224/541)), jaw ankylosis (23.1% (125/541)), pain (22.0% (119/541)), and flare-ups (22.0% (119/541)). The most common events that preceded HO progression or a flare-up were surgery, trauma, falls, and biopsies (Table 3). Signs reported during pregnancy, in fetuses, in newborns, and at autopsy are detailed in the Supplemental Results.
Events preceding HO or flare-ups.

Events preceding HO or flare-ups were reported in only one case (1.5%), each of which was as follows: anesthetic procedure, massage therapy, invasive procedure, physiotherapy, injection, pregnancy, back strain, blunt injury, excision, incision, and knee sprain. Events preceding HO or flare-ups were not reported for 473 (87.4%) patients.
HO, heterotopic ossification.
Prevalence of skeletal signs appeared to vary with certain non-canonical ACVR1 variants (Supplemental Table 7). Of the variants reported in more than one case, patients with the R375P variant were reported to have a mild FOP phenotype, with HO specified in 62.5% (5/8), great toe malformation in 25.0% (2/8), and impaired mobility in 37.5% (3/8) of cases. 45 HO was reported in all patients with the G356D and R258S variants, with varying reports of other signs related to the skeletal system (Supplemental Table 7).
Patient care setting
Most patients referred to or consulted by a specialist (16.8% (91/541)) were reported to have seen a single specialist (64.8% (59/91)), with 18.7% (17/91) of patients seeing two specialists. Very few patients were reported to have seen more than two specialists (three: 6.6% (6/91); five: 1.1% (1/91); six or more: 3.3% (3/91)). Care from multidisciplinary teams was specifically reported for just 5.5% of patients (5/91).
The specialists referred to or consulted with throughout a patient’s care pathway were described for 16.8% (91/541) of cases, most commonly orthopedists (15.4% (14/91)) and maxillofacial/oral surgeons (11.0% (10/91)) (Figure 2). Across geographical regions, the reported specialist referrals varied widely (Figure 2).

Specialist referrals/consultations, stratified by region (N = 91).
The hospital departments most commonly involved in patients’ care, based on the affiliations of corresponding authors of the case reports (Supplemental Methods), were Orthopedics (28.1% (135/481)), Pediatrics (10.2% (49/481)), and Radiology (8.1% (39/481)) (Supplemental Figure 2). When stratified by geographical region, Orthopedics was the most commonly reported department in North America (45.0% (27/60)), Western Europe (36.6% (37/101)), and Asia/Pacific (28.9% (68/235)). In Latin America, the highest proportion of corresponding authors were affiliated with Genetics departments (42.2% (19/45)) (Supplemental Figure 2).
Patient care pathway
Clinical tests or assessments
Clinical tests or assessments were reported to have been performed prior to a diagnosis of FOP in 34.0% (184/541) and post-diagnosis in 12.8% (69/541) of patient cases. Imaging techniques reported included radiographs (pre-diagnosis: 25.0% (46/184); post-diagnosis: 18.8% (13/69)), computerized tomography (CT) scans (pre-diagnosis: 21.7% (40/184); post-diagnosis: 36.2% (25/69)), magnetic resonance imaging (MRI; pre-diagnosis: 16.8% (31/184); post-diagnosis: 17.4% (12/69)), and ultrasound (pre-diagnosis: 6.0% (11/184); post-diagnosis: 10.1% (7/69)) (Table 4). Expectedly, genetic tests (24.9% (74/297), regardless of whether an ACVR1 pathogenic variant was reported), when performed, were nearly always conducted prior to diagnosis (Table 4). A post-diagnosis genetic test was reported in one case (1.4% (1/69)), to identify the genetic variant for a patient previously diagnosed with FOP. 46 The proportion of patients reported to have received a clinical/physical examination was 30.4% (56/184) prior to diagnosis and 8.7% (6/69) after diagnosis (Table 4).
Clinical tests and assessments.

Clinical tests/assessments reported to have been undertaken for fewer than 10 patients with FOP were as follows: histopathology (3.0%, n = 9); bone scintigraphy scan, imaging (not specified; 2.7%, n = 8); pathological examination (2.4%, n = 7); autopsy, neurological evaluation (each 2.0%, n = 6); biochemical evaluations, ECG (each 1.3%, n = 4); audiological evaluation, DNA sequencing analysis, endoscopy, neuropsychological testing (each 1.0%, n = 3); bone marrow aspiration, lumbar puncture, measure of oxygen saturation, NaF PET/CT, PET/CT (each 0.7%, n = 2); 24-h Holter test, abdominal examination, angiography, arterial blood gas study, blood pressure, cardiotocograph, cytology study, dental screening, EEG, electromyography, fetal ECG, Glasgow coma scale, hormone test, hysteroscopy, intracompartmental pressure measure, investigatory surgery, lung function test, Mantoux test, mass puncture, phosphocalcic samples, pregnancy evaluation, prenatal ultrasound, pulmonary examination, respiratory function test, SPECT/CT imaging, tilt-table test, venous Doppler USG (each 0.3%, n = 1). A test/assessment was not reported for 244 patients. It was unclear whether the reported test/assessment was performed pre- or post-diagnosis for 19.2% (57/297) of cases.
24-h, 24-hour; CT, computed tomography; DNA, deoxyribonucleic acid; ECG, electrocardiogram; EEG, electroencephalogram; FOP, fibrodysplasia ossificans progressiva; MRI, magnetic resonance imaging; NaF, natrium sodium fluoride; PET, positron emission tomography; SPECT, single-photon emission computed tomography; USG, ultrasonography.
Pharmacological management
Of the 35.9% (194/541) of cases where a prescribed pharmacological treatment class could be categorized, the most common treatment classes prescribed were corticosteroids (52.6% (102/194)) and NSAIDs (39.7% (77/194)) (Supplemental Figure 3). There were no apparent trends in the frequency of articles reporting use of corticosteroids and NSAIDs between 2000 and 2024 (Supplemental Figure 4). Among cases where the specific drug was reported (Figure 3), prednisone (16.0% (23/144)) and prednisolone (12.5% (18/144)) were the most commonly reported corticosteroids used. The route of corticosteroid administration was specified in 36 instances, with multiple routes reported in 7 cases. Oral (66.7% (24/36)) and intravenous (41.7% (15/36)) modes of administration were most common (topical and inhalation both 5.6% (2/36)). Among NSAIDs, the most commonly reported included indomethacin (10.4% (15/144)), ibuprofen (5.6% (8/144)), celecoxib (4.2% (6/144)), and naproxen (2.8% (4/144)) (Figure 3). Corticosteroids and NSAIDs were the predominant drug classes reported across all global regions (Supplemental Figure 3), with the exception of Latin America.

Pharmacological treatments received (N = 144).
Compared with corticosteroids and NSAIDs, fewer global case reports described bisphosphonate use (30.9% (60/194)), although bisphosphonates were the most frequently reported treatment class in Latin America (57.9% (11/19)) (Supplemental Figure 3). Etidronate (16.0% (23/144)) and alendronate (7.6% (11/144)) were the most frequently reported bisphosphonates, while pamidronate (4.2% (6/144)) and zoledronate (2.1% (3/144)) were reported less frequently (Figure 3).
Among other treatment classes, antimicrobials were reported in 11.9% (22/194) of cases for suspected infections or post-surgical care (Supplemental Figure 3). Specific antimicrobials reported in more than one case were cefazolin (2.1% (3/144)), amoxicillin (1.4% (2/144)), and vancomycin (1.4% (2/144)) (Figure 3). The regions with the highest proportion of antimicrobial use were Africa (22.2% (2/9)) and Eastern Europe (22.2% (2/9)) (Supplemental Figure 3). Immunosuppressant use was reported for 7.2% (14/194) of patients, most commonly in Latin America (26.3% (5/19)). Methotrexate was the most commonly reported immunosuppressant (6.9% (10/144)) (Figure 3), followed by sulfasalazine (1.4% (2/144)), sirolimus, and cyclosporine (each 0.7% (1/144)). There were eight case reports describing the off-label use of the tyrosine kinase inhibitor, imatinib, to manage severe flare-ups in North America, and one report of the off-label use of the tyrosine kinase inhibitor, sunitinib, in Eastern Europe (Figure 3); no case reports described the use of Janus kinase inhibitors.13,14,47 Use of the IL1-inhibitors, canakinumab and anakinra, was only reported in one case each. Beyond NSAIDs and corticosteroids, use of the pain management options mentioned by the ICC’s FOP Treatment Guidelines included calcium channel alpha 2-delta ligands, which were reported in four cases (gabapentin and pregabalin, n = 2 each), serotonin–norepinephrine reuptake inhibitors used by one patient (venlafaxine), and opioids, which were prescribed to nine patients (morphine, n = 3; fentanyl and oxycodone, n = 2 each; remifentanil, n = 1; type of opioid not specified in two cases). Paracetamol use was reported in six patients (Figure 3). Finally, four case reports described the use of palovarotene during participation in phase II (NCT02190747; n = 1) and phase III (NCT03312634; n = 3) clinical trials.14,48
Surgical management
Surgical procedures were reported in 35.1% (190/541) of patient cases, taking place both before (40.5% (77/190)) and after a diagnosis of FOP (40.5% (77/190)). The proportion of articles reporting surgery stayed consistent between 2000 and 2024 (Supplemental Figure 6). For those cases where the surgery type was described, the most frequent type was malformation correction/bone resection (43.6% (78/179)), followed by biopsy (34.1% (61/179)) (Figure 4). Where it was possible to discern the timing, biopsies were always reported to have taken place prior to FOP diagnosis (25.1% (45/179)), though the purpose of the biopsy was not always clear. Surgeries for malformation correction/bone resection took place at a similar frequency before (16.8% (30/179)) and after diagnosis of FOP (19.0% (34/179)). Dental procedures (16.2% (29/179)), most commonly tooth extractions (67.9% (19/29)), occurred more frequently after diagnosis than before (Figure 4). Seven cases of emergency surgery were reported, including tracheostomy (n = 3), caesarean sections (n = 2), hysterectomy (n = 1), and thrombectomy (n = 1), all reported post-diagnosis.49–54
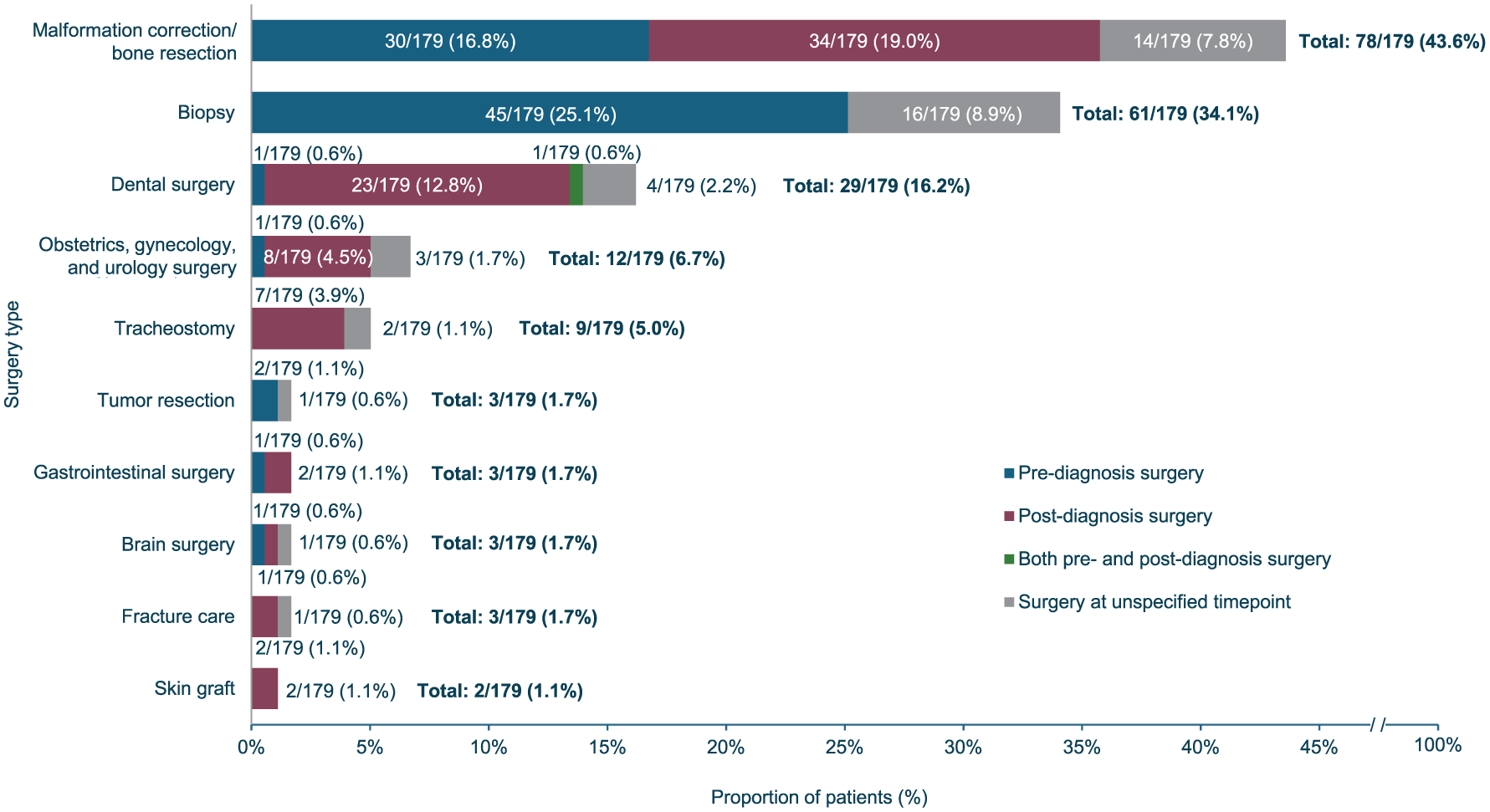
Types of surgery performed (N = 179).
The geographical region where the highest proportion of patients were reported to have undergone a surgical procedure was North America (53.6% (37/69)), followed by Africa (34.6% (9/26)), Asia/Pacific (33.5% (85/254)), Western Europe (28.8% (34/118)), Oceania (25.0% (1/4)), and Latin America (22.4% (13/58)). The proportion of surgeries for malformation correction/bone resection was higher in Asia/Pacific (50.6% (43/85)) and North America (48.6% (18/37)) than other surgery types (Supplemental Figure 5). Biopsies were the most common surgery type reported in Latin America (53.8% (7/13)), Africa (44.4% (4/9)), and Western Europe (35.3% (12/34)). In Africa, dental procedures were the second most common type of surgery (33.5% (3/9)).
The outcome of surgery was reported in 103 cases. The most commonly reported events were accumulation of new HO (45.6% (47/103)), as well as worsened mobility (10.7% (11/103)) and general symptom progression (9.7% (10/103)) (Table 5).
Surgical outcomes or complications.
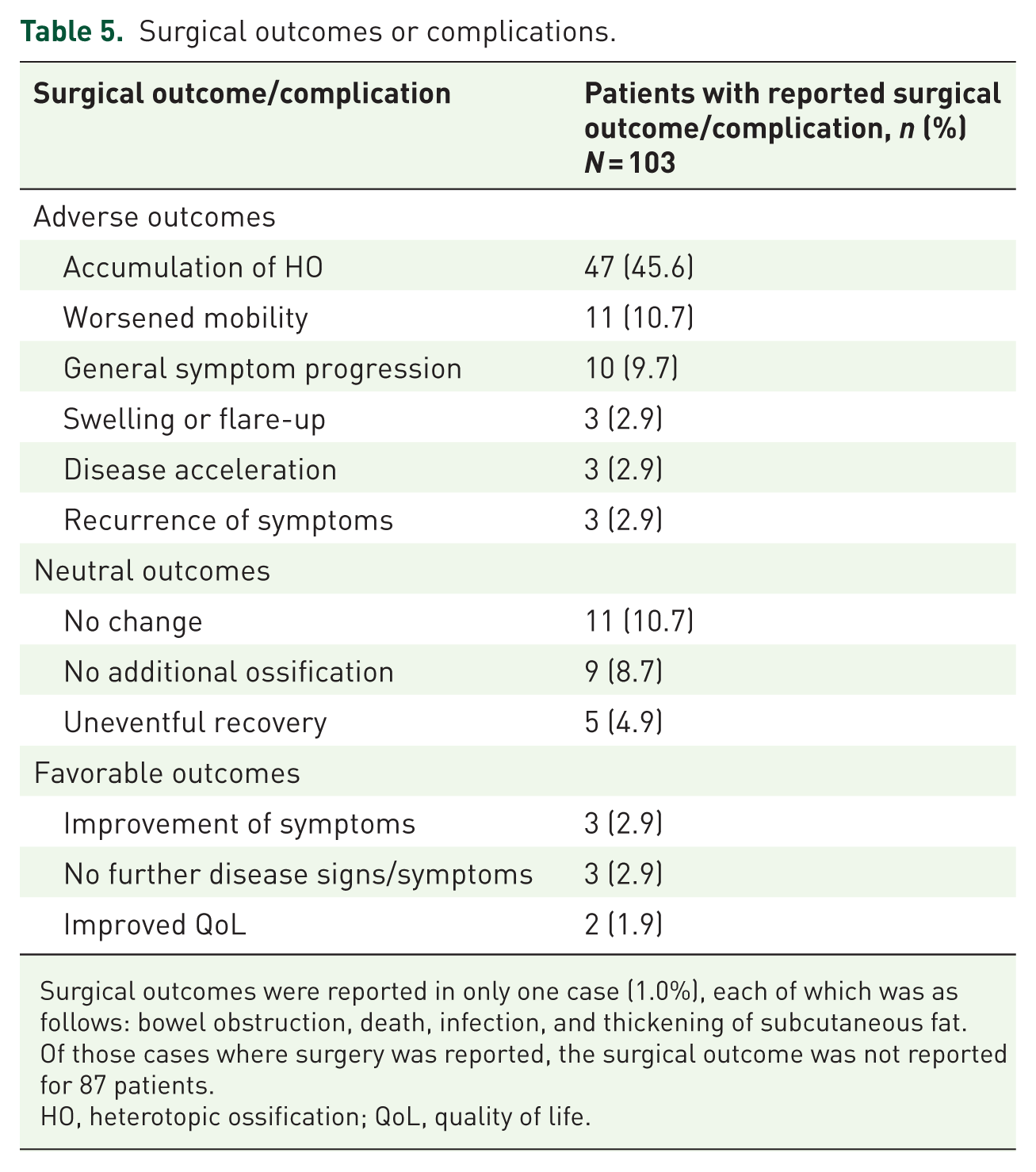
Surgical outcomes were reported in only one case (1.0%), each of which was as follows: bowel obstruction, death, infection, and thickening of subcutaneous fat. Of those cases where surgery was reported, the surgical outcome was not reported for 87 patients.
HO, heterotopic ossification; QoL, quality of life.
Improvements in symptoms or QoL immediately following surgery were reported in only 5.8% (6/103) of cases; however, long-term outcomes were not detailed for these patients.54–58
Discussion
To identify opportunities for international collaboration within the FOP community and characterize global variation in management practices, we conducted a scoping review of published case reports. This study is the first to use global case report data to examine care pathways and management patterns for FOP across diverse health systems. Analysis of case reports from 57 countries revealed substantial heterogeneity in clinical assessments, access to multidisciplinary care, and pharmacological and surgical approaches. These findings highlight the need for international outreach to share best practices, connect patients with experienced clinicians, and harmonize care through collaborative networks, ultimately supporting the adoption of evidence-based standards worldwide.
Identification of patients with FOP
Liljesthröm et al. 1 reported a prevalence of 834 patients with FOP based on a review of international, national, and regional organizational databases conducted in 2016. The current scoping review applied a different methodology and timeframe, focusing on case reports published between 2000 and 2024. Using this approach, 541 global cases were identified, with notable representation from the Asia/Pacific region and Africa (Figure 1). The current scoping review also identified case reports from countries such as Thailand, which, to the best of our knowledge, have not been represented in FOP prevalence studies or patient registry publications to date.1–3 Isolated cases of FOP from countries with underserved communities may have been published in case reports rather than being included in large database studies, due to limited access to healthcare, a lack of existing FOP organizations, and potential language barriers among medical professionals in these regions. 1 The case report review methodology, therefore, has value in finding patients beyond the demographic typically represented in larger observational studies, as well as those who may not have connections to FOP organizations. The findings of this study indicate where outreach efforts to connect patients with local FOP patient organizations may be beneficial, for example, in regions such as Asia/Pacific and Africa. In addition, through the collation of information related to individual patients and their managing physicians, this scoping review may serve as an opportunity to connect underserved groups with the international FOP community, though there remains a need to address barriers such as lack of access to online resources, difficulty in traveling to community events, and language differences.
Insights on FOP management practices
By synthesizing patient-level insights from global case reports, this scoping review has revealed trends and heterogeneity in FOP real-world management practices as well as variable degrees of alignment to the ICC recommendations for the management of FOP. However, these findings should be interpreted with caution due to the inherent selection bias of case studies routinely reporting atypical clinical cases, such as unusual or severe case presentations or patients with non-canonical ACVR1 variants. Indeed, the R206H variant accounted for 81.5% of patients in this scoping review, but published literature estimates that 95%–97% of FOP cases are caused by the classic R206H variant.59–61 This discrepancy could indicate inclusion of populations with non-canonical ACVR1 variants in this scoping review that have been underrepresented or underestimated in previously published data, perhaps due to the growing availability of genetic testing. Alternatively, the discrepancy may simply reflect a tendency to publish novel or rare variants as case reports; therefore, reports may not always be representative of disease progression or clinical management associated with classic FOP.
The ICC’s FOP Treatment Guidelines stipulate that clinical observation of skeletal malformations, including malformed great toes, soft tissue swelling, and progressive HO, is required for the diagnosis of FOP. 12 The classic signs of HO and great toe malformations were reported prior to diagnosis in 23.1% and 29.3% of patients, respectively, where they may have contributed to the diagnosis of FOP. However, despite being pathognomonic signs of FOP, HO and great toe malformations were observed with a lower prevalence than expected.9,62 Infrequent reporting of great toe malformation and HO before diagnosis in the identified case reports may indicate a lack of awareness of classic clinical features of FOP among clinicians. Indeed, non-specific mobility limitations and growths/lesions were the most commonly reported signs before diagnosis; examining such signs in isolation heightens the risk of diagnostic delay and misdiagnosis that are often seen in FOP. 29 Imaging techniques such as MRI and CT scans are generally considered superfluous to the diagnosis of FOP and are not normally used in routine follow-up for serial assessments of disease burden, yet they were often used prior to, and after, a FOP diagnosis in identified case reports. 12 As these tests would typically be included in the assessment of a non-specific lump/swelling, 63 this finding may again reflect a lack of recognition or incomplete assessment of pre-diagnostic signs of FOP. Initiatives to raise awareness of the unique characteristics of FOP could support better recognition and reduce diagnostic delays. For example, early identification of classic signs might be aided by newborn screening programs, such as a current initiative in Brazil looking for great toe malformations at birth. 64 Such initiatives would need to be targeted widely, given the variety of hospital departments and specialists involved in the care of patients with FOP, as identified in this scoping review.
Globally, the most commonly used treatments for FOP were corticosteroids and NSAIDs, aligning with recommendations by the ICC. 12 Bisphosphonates were also used globally, with the predominant bisphosphonate reported being etidronate (16.0% of cases). Etidronate was previously approved for the management of HO, but its marketing status has been discontinued in the United States, with evidence that high dosage for long durations can lead to osteomalacia and impaired ossification of the skeletal system.12,65,66 Use of newer aminobisphosphonates described in the ICC’s FOP Treatment Guidelines, such as pamidronate and zoledronate (reported in 4.2% and 2.1% of cases, respectively), does not appear to have overtaken etidronate use over the duration of cases reported during the timeframe covered by this scoping review. Despite the ICC’s FOP Treatment Guidelines recognizing potential benefits of off-label tyrosine kinase inhibitors for uncontrolled flare-ups, 12 their use was reported infrequently in North America and Eastern Europe only. Limited access to new aminobisphosphonates and tyrosine kinase inhibitors in certain geographical regions, or lack of awareness of the anecdotal benefits recognized in the ICC’s FOP Treatment Guidelines, may explain the infrequent use of these treatments. The high proportion of patients receiving antimicrobials in Africa and Eastern Europe, relative to other treatment classes, may be a reflection of increased risk or community-acquired infections, rather than being an FOP management strategy.
For the management of pain in FOP, the ICC’s FOP Treatment Guidelines indicate a variety of first, second, and third-line agents that could be considered, depending on whether the pain is chronic (neuropathic or nociceptive) or acute. 12 NSAIDs or corticosteroids are recommended for acute pain, and for chronic nociceptive pain, NSAIDs are the mainstay of treatment. Corticosteroid or NSAID use was reported in 102 and 77 cases in this scoping review, respectively; however, it was not always specified whether this was for pain management purposes. For neuropathic pain, recommended first-line treatments are calcium channel alpha 2-delta ligands, tricyclic antidepressants, and serotonin–norepinephrine reuptake inhibitors, yet use of these treatment classes was reported for just five patients. Second-line treatments (antiepileptics and tramadol) and third-line opioids 12 were also rarely reported. The low number of cases in which neuropathic pain medication was reported may suggest its underutilization in FOP.
The ICC’s FOP Treatment Guidelines also suggest that, in most circumstances, elective invasive procedures other than dental surgery should be avoided for patients with FOP due to the high risk of inciting flare-ups and progression of HO. 12 Dental procedures may be considered necessary and appropriate in patients with FOP when appropriate care is taken to avoid flare-ups and disease progression. Yet, other surgeries such as malformation correction/bone resection and biopsies were more common, and for many non-dental invasive surgery types, the frequency of patients undergoing a procedure was similar or higher after a diagnosis of FOP than before. These findings indicate that some clinicians might not be aware of the adverse impacts of surgery in FOP, though it could not be determined whether any surgeries were performed in the knowledge of the ICC’s FOP Treatment Guidelines and could have been avoided. Indeed, accumulation of HO and general symptom progression after surgery were noted in many cases, as well as impaired mobility. These results highlight the importance of widespread accessibility to, and education on, the ICC’s FOP Treatment Guidelines, to facilitate timely diagnosis and to reduce the likelihood of unnecessary or potentially harmful invasive procedures.
Due to the multisystemic manifestations of FOP, in addition to the risks that certain interventions pose in triggering flare-ups or irreversible disease progression, patients require specialist, multidisciplinary care to optimize disease management.12,29,67 The low reported rates of specialist referrals and patients seen by multidisciplinary care teams reflect discussions in a 2021 multi-stakeholder meeting, which noted the need to standardize access to specialist, multidisciplinary care, and expertise across all regions, to reflect the complexity and heterogeneity of FOP. 29
Overall, the scoping review revealed variation in real-world FOP management practices globally and some variability in the application of ICC expert recommendations. Treating physicians may have selected alternative management approaches to those recommended in the ICC’s FOP Treatment Guidelines due to factors such as a patient’s unique symptom presentation or disease progression, to address urgent manifestations appropriately, or due to healthcare and medication access restrictions. Low awareness of the ICC’s FOP Treatment Guidelines may also have been a contributing factor; however, peer-reviewed guidance regarding the management of FOP is available via GeneReviews, accessible to clinicians internationally. 68 To enhance patient care, connections must be forged among the international FOP community to facilitate the sharing of learnings and to help establish FOP care pathways in underserved regions. Further studies synthesizing the real-world impacts of specific pharmacological and surgical approaches on manifestations and health-related QoL would continue to guide best practices in clinical management.
Strengths and limitations of the review
In this study, the case report review methodology was an effective tool that was able to identify global cases of FOP and gather insights into real-world management practices, particularly from previously underrepresented geographical regions. In addition, the disease presentation described in identified case reports reflected well-characterized clinical features of FOP (such as HO and great toe malformation). This suggests that in understudied rare diseases with a less advanced network structure than FOP, the methodology may have value to better understand disease natural history, especially where large cohort studies are challenging due to small population sizes. Indeed, the case review methodology has previously been used to gain insights into ultra-rare conditions such as mucopolysaccharidosis type II, Krabbe disease, and Farber disease.33,35,37
Any conclusions on the generalizability of real-world FOP management practices are limited by the aforementioned reporting selection bias, as well as variability in reporting of outcomes, for instance, the timepoint at which age was reported (e.g., age at the time of presentation vs age at diagnosis). This variability resulted in small sample sizes for analyses, meaning potential confounding factors could not be controlled for; therefore, results from the analyses should be interpreted with considerable caution. In addition, the variability in reported data meant that analyses were descriptive; while this allowed for the observation of patterns, causality could not be determined, and statistical testing between groups could not be performed. Furthermore, according to the current scoping review’s methodology, eligible case reports had to describe a patient with a primary diagnosis of FOP as reported by the authors; however, genetic confirmation was not always specified in the case reports. This limitation, which may be due to challenges in access to genetic testing in certain geographies or inconsistency in reporting whether a genetic test was conducted, meant that it could not be verified whether all included patients had FOP. It was not possible to determine whether the lack of a reported test or outcome reflected its absence in clinical practice for the patient, since it could have been that it was simply not reported by the authors. Future consistent and comprehensive case reporting, in line with case reporting guidelines, for example, CARE (CAse REport), would ensure that the case review methodology is standardized and allow for more precise insights into disease characteristics and management. 69 A more standardized approach to case reporting would help to reduce the knowledge gap in many rare or recently described diseases, where published literature is sparse.
Due to the pragmatic nature of our scoping review, other limitations were also inherent. Although a de-duplication step was performed, it was not possible to verify that all patient records in the scoping review represented unique patients. The searches and data extraction for this scoping review were conducted by a single reviewer, and involving multiple reviewers could strengthen reliability, improve accuracy, and reduce bias. Furthermore, analyses of variables over time were based on the date of individual case report publications, which may not directly relate to the date that a variable occurred (e.g., when a patient received a treatment), limiting the robustness of the conclusions drawn. Finally, manual classifications of qualitative data provided insights into trends, such as types of surgery performed. However, this required simplification of the patient care pathway, which limited the ability to capture nuances of FOP management practices in individual cases. For example, by classifying surgeries under “malformation correction/bone resection,” the variation in types of malformations was obscured. These limitations highlight the need for future research, such as registry and natural history studies, to complement the insights that can be gained through reviews of case reports for rare and ultra-rare diseases.
Conclusion
This study identified and synthesized patient-level data from case reports, supporting patient-finding efforts and providing insights into real-world management practices. The global identification of patients with FOP may aid in connecting patients and treating physicians in underserved regions with the international FOP community. This review highlights real-world patterns in the management of FOP globally, although the inherent selection bias of case studies toward atypical cases should be considered when interpreting the findings. Limited reporting of the hallmark features of FOP (HO and great toe malformation) before diagnosis, as well as regional differences in access to multidisciplinary teams and pharmacological treatments, underscores the need for mutual sharing of learnings on best practices for diagnosing and managing FOP, to optimize patient care.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X251407060 – Supplemental material for Identifying global trends from case reports of fibrodysplasia ossificans progressiva: a scoping review
Supplemental material, sj-docx-1-tab-10.1177_1759720X251407060 for Identifying global trends from case reports of fibrodysplasia ossificans progressiva: a scoping review by Christiaan Scott, Mona Al Mukaddam, Michelle Davis, Carmen L. De Cunto, Edward C. Hsiao, Robert J. Pignolo, Odette Schwegler, Alexander Artyomenko, Kim Croskery, Kate Hanman, Boris Sanchot, Emma Warnants and Frederick S. Kaplan in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-pdf-2-tab-10.1177_1759720X251407060 – Supplemental material for Identifying global trends from case reports of fibrodysplasia ossificans progressiva: a scoping review
Supplemental material, sj-pdf-2-tab-10.1177_1759720X251407060 for Identifying global trends from case reports of fibrodysplasia ossificans progressiva: a scoping review by Christiaan Scott, Mona Al Mukaddam, Michelle Davis, Carmen L. De Cunto, Edward C. Hsiao, Robert J. Pignolo, Odette Schwegler, Alexander Artyomenko, Kim Croskery, Kate Hanman, Boris Sanchot, Emma Warnants and Frederick S. Kaplan in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
The authors acknowledge Amicie De Pierrefeu, PhD (Employee and shareholder—Ipsen) for her contributions to the analyses. The authors also acknowledge Sunandan Dhar, PhD, and Megan Allfrey, BSc, of Costello Medical for medical writing and submission assistance based on the authors’ input and authorization, which was sponsored by Ipsen in accordance with Good Publication Practice guidelines.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.