
Abstract
Background:
Psoriatic arthritis (PsA) is a chronic inflammatory disease that causes pain and fatigue, reduces physical function, and negatively impacts health-related quality of life (HRQoL). In the phase III BE OPTIMAL and BE COMPLETE studies, bimekizumab demonstrated clinical efficacy and meaningful improvements in patient-reported outcome (PRO) measures in biologic disease-modifying antirheumatic drug (bDMARD)-naïve patients, and those who had prior inadequate response/intolerance to tumor necrosis factor inhibitors (TNFi-IR).
Objectives:
To examine the association between achieving increasingly stringent clinical disease control criteria and improvements in PRO measures in patients with active PsA receiving bimekizumab.
Design:
Post hoc analysis of two phase III studies.
Methods:
BE OPTIMAL and BE COMPLETE assessed subcutaneous bimekizumab 160 mg every 4 weeks in bDMARD-naïve and TNFi-IR patients with active PsA. Disease control was assessed using American College of Rheumatology (ACR) response criteria, Minimal Disease Activity, Disease Activity Index for Psoriatic Arthritis, and the composite outcome of ACR50 and 100% improvement in Psoriasis Area and Severity Index. Associations between clinical disease control criteria and PRO measures of pain, fatigue, physical function, and HRQoL were assessed at week 16 and week 52/40 (BE OPTIMAL/BE COMPLETE).
Results:
Achievement of increasingly stringent clinical disease control criteria was generally associated with sequentially greater improvements in all PRO measures, including pain. At week 52/40, 94.7% of bDMARD-naïve and 97.6% of TNFi-IR patients achieving ACR70 reported ⩾50% improvements in pain from baseline, and the greatest numerical improvements (−48.5 bDMARD-naïve; −54.7 TNFi-IR). This pattern was evident as early as week 16 and sustained when assessed at week 52/40 across the majority of clinical disease control criteria and PRO measures reported.
Conclusion:
The achievement of increasingly stringent thresholds of disease control was associated with corresponding greater improvements in PROs, for patients receiving bimekizumab treatment, irrespective of prior TNFi use.
Trial registration ClinicalTrials.gov:
NCT03895203, NCT03896581, and NCT04009499.
Keywords
Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory disease that is characterized by symptoms in multiple domains, including peripheral and axial joints, psoriatic skin and nail lesions, dactylitis, and enthesitis.1,2 The diverse range of clinical manifestations contributes to a substantial patient burden, profoundly impacting both patient function and quality of life.3,4 The most problematic patient-reported symptoms of PsA include pain, fatigue, and reduced physical activity. 5
A key goal, common to all international treatment recommendations for PsA, is to maximize patients’ health-related quality of life (HRQoL) through symptom control, prevention of structural damage, and normalization of physical and social function.6–9 As such, treatments should aim to reduce the impact of PsA on patients’ lives by achieving and maintaining the lowest possible level of disease activity in all domains.
Treatment efficacy is assessed using clinical outcomes such as the American College of Rheumatology (ACR) response criteria, Psoriasis Area and Severity Index (PASI) for skin, and composite outcomes that evaluate multiple domains, such as the Minimal Disease Activity (MDA) criteria and the Disease Activity Index for Psoriatic Arthritis (DAPSA). While these measures determine the clinical efficacy of a treatment, current evidence associating improvements or achievement of higher thresholds across these outcomes with meaningful impact for patient-reported symptoms following treatment is limited, with few post hoc analyses of interventional studies in PsA.10–12 Therefore, it is of clinical interest to determine the extent to which the achievement of increasingly stringent clinical disease control (i.e., achieving sequentially lower levels of disease activity) following clinical intervention is associated with greater improvements in patient-reported outcome (PRO) measures, specifically those evaluating pain, fatigue, physical functioning, and HRQoL.
Bimekizumab is a humanized monoclonal IgG1 antibody that selectively inhibits IL-17F in addition to IL-17A. 13 The phase III BE OPTIMAL and BE COMPLETE studies demonstrated the tolerability and sustained efficacy of bimekizumab in biologic disease-modifying antirheumatic drug (bDMARD)-naïve patients, and those who had prior inadequate response or intolerance to tumor necrosis factor inhibitors (TNFi-IR).14–17 Up to 1 year, similar clinically meaningful improvements in joint and skin efficacy outcomes, as well as PRO measures, were observed irrespective of patients’ prior biologic use.16,17
Here, we present a post hoc analysis of bimekizumab-treated patients with active PsA in BE OPTIMAL and BE COMPLETE that examines the association between achieving increasingly stringent clinical disease control criteria and improvements in PRO measures of pain, fatigue, physical function, and HRQoL at week 16 and with longer-term treatment up to week 52.
Methods
Study design and participants
Full methodological details of the phase III, multicenter, randomized BE OPTIMAL (NCT03895203) and BE COMPLETE (NCT03896581) studies, and their open-label extension (OLE) BE VITAL (NCT04009499), have been reported previously.14–17
In brief, BE OPTIMAL and BE COMPLETE were placebo-controlled to week 16 and assessed the efficacy and safety of subcutaneous bimekizumab in bDMARD-naïve (BE OPTIMAL) and TNFi-IR patients (BE COMPLETE) with a documented diagnosis of adult-onset, active PsA that met the Classification Criteria for Psoriatic Arthritis for at least 6 months prior to study screening. 18 Eligible patients had no active comorbidities that could potentially interfere with efficacy outcomes and PRO measures. Results reported here are for patients receiving bimekizumab 160 mg every 4 weeks (Q4W) from baseline in both studies.
Patients initially randomized to bimekizumab in BE OPTIMAL received 52 weeks of blinded treatment with bimekizumab. Those patients initially randomized to bimekizumab in BE COMPLETE received 16 weeks of blinded treatment with bimekizumab and then open-label bimekizumab 160 mg Q4W (as part of the BE VITAL OLE).
Assessments
Associations between clinical disease control criteria and PRO measures are reported to week 52 of BE OPTIMAL for bimekizumab-randomized patients. For patients completing BE COMPLETE and entering the BE VITAL OLE, all PRO measures are reported to week 40 (24 weeks of open-label treatment in BE VITAL; Supplemental Figure 1). The next assessment of all PROs in the study was not until week 68; thus, week 40 results are presented in this analysis.
The clinical disease control criteria, assessing disease activity, used in this analysis, included the following outcomes: ACR response criteria, reported using mutually exclusive improvement from baseline thresholds of <20% (<ACR20), ≥20% to <50% (ACR20 to <ACR50), ≥50% to <70% (ACR50 to <ACR70), and ≥70% (ACR70); DAPSA, reported using disease states of high disease activity (HDA), moderate disease activity (MoDA), and low disease activity/remission (LDA/REM); MDA, reported as non-MDA and MDA; the composite outcome of ACR50 and 100% improvement in PASI (ACR50+PASI100, in patients with psoriasis involving ≥3% body surface area [BSA] at baseline), reported as non-responder and responder.
Week 16 and week 52/40 (BE OPTIMAL/BE COMPLETE) data are reported for the association between achievement of the abovementioned clinical disease control criteria and change from baseline in the following PRO scores: arthritis pain visual analog scale (pain VAS) score, which ranges from 0 (“no pain”) to 100 (“most severe pain”), 19 Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue subscale score, Health Assessment Questionnaire-Disability index (HAQ-DI), 12-item PsA Impact of Disease (PsAID-12) total and single-item domain scores, Short-Form 36-item Health Survey (SF-36) Physical Component Summary (PCS) score, and EQ-5D-3L VAS and EQ-5D-3L utility scores.
Associations were also assessed between the achievement of clinical disease control criteria and ⩾30/50/70% improvements from baseline in pain VAS (⩾50% improvement hereafter referred to as “substantial” improvement),20,21 pain VAS score ⩽15, FACIT-Fatigue minimal clinically important difference (MCID; increase of ⩾4 from baseline in patients with a score ⩽48 at baseline), 22 HAQ-DI MCID (decrease of ⩾0.35 from baseline in patients with a score ⩾0.35 at baseline), 23 and HAQ-DI normative value response (normative state was defined as HAQ-DI ⩽0.5). 24
Additional analyses were conducted to assess the association between the achievement of PASI100 and disease impact, captured with the PsAID-12 total score, as well as PASI100 and skin problems, captured with the related PsAID-12 single-item domain, in patients with psoriasis affecting ≥3% BSA at baseline.
Statistical analysis
All analyses reported here are post hoc. Data are reported as observed cases (no imputation of missing data) and describe the mean change from baseline with 95% confidence intervals (CI), for subgroups of patients defined by the achievement of mutually exclusive clinical disease control criteria (as described above) at week 16 and week 52/40. These post hoc data are descriptive and thus no formal statistical testing was performed.
Results
Patient disposition and baseline characteristics
In BE OPTIMAL, 431 of 852 bDMARD-naïve patients were randomized to bimekizumab, and 388/431 (90.0%) completed week 52. In BE COMPLETE, 267 of the 400 TNFi-IR patients were randomized to bimekizumab; 246/267 (92.1%) of these remained in the study at week 40. Bimekizumab was well tolerated across both studies and full safety results up to week 52 have previously been reported; the overall safety profile of bimekizumab was consistent with previous reports.14–17,25,26
The previously reported baseline demographics and disease characteristics of bimekizumab-randomized patients were representative of bDMARD-naïve and TNFi-IR patients with moderate-to-severe PsA (Supplemental Table 1).14,15 The TNFi-IR population was numerically slightly older than the bDMARD-naïve population (mean age: 50.1 [SD 12.4] years vs 48.5 [SD 12.6] years) and reported more prominent disease symptoms, such as swollen and tender joints, pain, and reduced physical functional. In addition, the TNFi-IR population had a numerically greater duration of time since PsA diagnosis (mean: 9.6 [SD 9.9] years), as compared with the bDMARD-naïve population (6.0 [SD 7.3] years). A numerically higher proportion of bDMARD-naïve patients were receiving concomitant methotrexate at baseline (58.5%), than were TNFi-IR patients (44.6%).
Pain
Patients with PsA who reached increasingly stringent disease control criteria reported greater improvements in pain (Figure 1). In both bDMARD-naïve and TNFi-IR patients randomized to bimekizumab, achievement of increasingly stringent ACR response levels, DAPSA disease states, MDA response criteria, and ACR50+PASI100 response criteria was associated with sequentially numerically larger mean reductions from baseline in the pain VAS score. These associations were evident at week 16 (Table 1) and sustained when assessed at week 52/40 (Figure 1(a)).
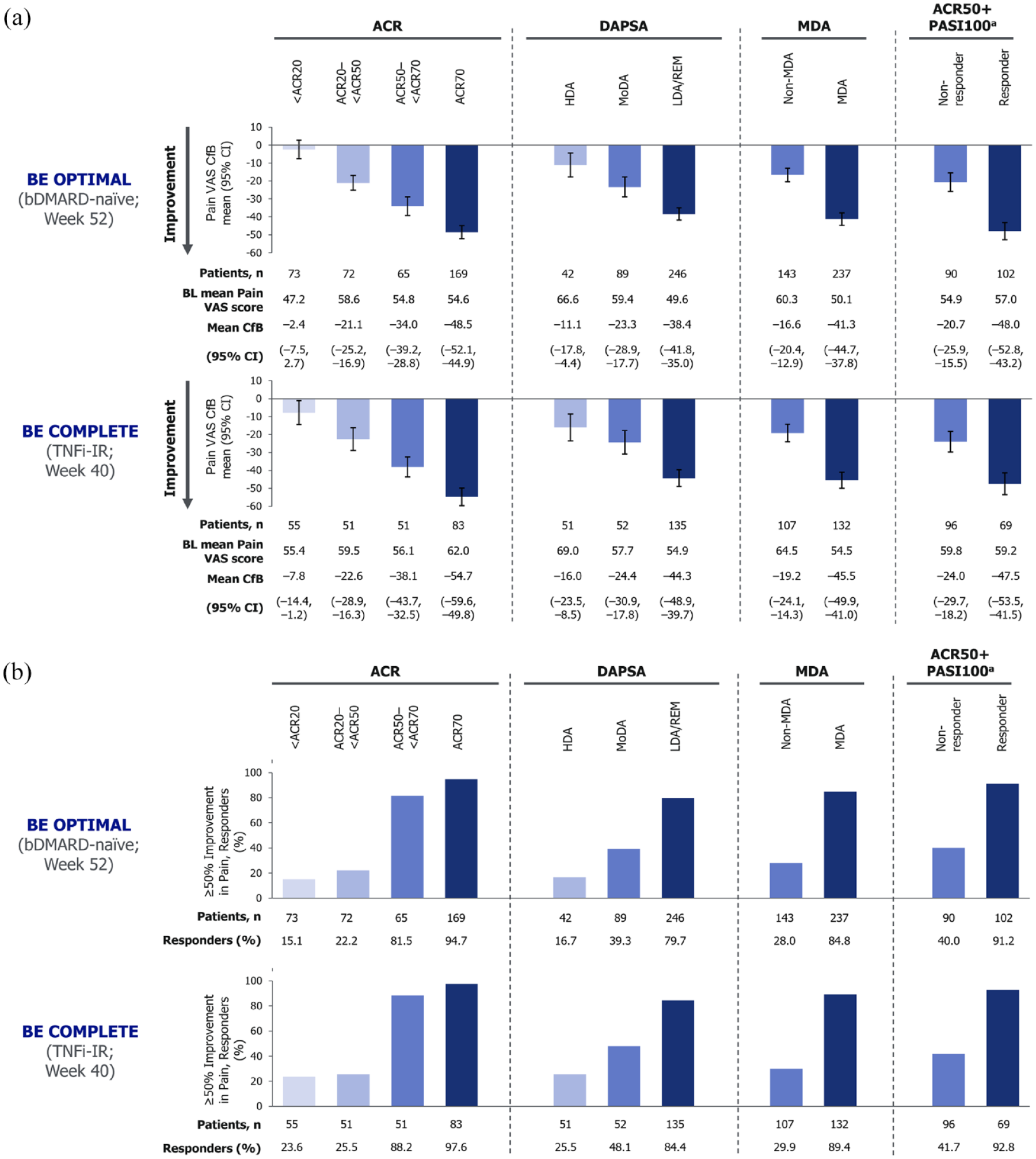
Association of disease activity with patient-reported pain at week 52 for bDMARD-naïve patients and week 40 for TNFi-IR patients (OC). (a) Pain VAS CfB and (b) substantial improvement (⩾50% improvement from baseline in pain VAS).
Association of disease activity with patient-reported outcome measures at week 16 (OC).

Randomized set. PsAID-12 scores range from 0 to 10; higher scores indicate worse status. 27
⩾50% improvement from baseline in pain VAS.
FACIT-Fatigue score increase of ⩾4 from baseline in patients with a FACIT-Fatigue score ⩽48 at baseline.
HAQ-DI decrease of ⩾0.35 from baseline in patients with a HAQ-DI score ⩾0.35 at baseline.
In patients with psoriasis affecting ≥3% BSA at baseline.
ACR, American College of Rheumatology; bDMARD, biologic disease-modifying antirheumatic drug; BKZ, bimekizumab; BSA, body surface area; CfB, change from baseline; CI, confidence interval; DAPSA, Disease Activity Index for Psoriatic Arthritis; FACIT‑Fatigue, Functional Assessment of Chronic Illness Therapy‑Fatigue; HAQ‑DI, Health Assessment Questionnaire‑Disability Index; HDA, high disease activity; LDA, low disease activity; MCID, minimal clinically important difference; MDA, minimal disease activity; MoDA, moderate disease activity; OC, observed case; PASI, Psoriasis Area and Severity Index; PsAID-12, Psoriatic Arthritis Impact of Disease-12; REM, remission; TNFi-IR, inadequate response or intolerance to tumor necrosis factor inhibitors; VAS, visual analog scale.
Achievement of stringent clinical response criteria, such as ACR50 to <ACR70 and ACR70, DAPSA LDA/REM, MDA, and ACR50+PASI100, was associated with greater proportions of bDMARD-naïve and TNFi-IR patients achieving substantial (≥50%) reductions in pain VAS from baseline by Week 52 and 40 (Figure 1B). This trend in associations was also evident for both ≥30% and ≥70% improvements in pain VAS (Supplementary Figure 2), and the achievement of pain VAS score ≤15 (Supplementary Figure 3).
Fatigue
In bDMARD-naïve patients at week 52, achievement of the most stringent disease control criteria, ACR70, DAPSA LDA/REM, MDA, and ACR50 + PASI100 was associated with the greatest improvements in FACIT-Fatigue and a higher proportion of patients achieving FACIT-Fatigue MCID (Figure 2). For TNFi-IR patients at week 40, the achievement of the most stringent ACR response, ACR70, or ACR50+PASI100 response was associated with the greatest improvements in FACIT-Fatigue score and higher proportions reaching MCID (Figure 2). These associations observed at week 52/40 were sustained from those observed at week 16 (Table 1).

Association of disease activity with fatigue at week 52 for bDMARD-naïve patients and week 40 for TNFi-IR patients (OC). (a) FACIT-fatigue CfB and (b) FACIT-fatigue MCID (score increase ⩾4 in patients with baseline score ⩽48).
In bDMARD-naïve patients, lower DAPSA disease activity was associated with greater improvements in FACIT-Fatigue score (Figure 2(a)). Achievement of DAPSA LDA/REM resulted in the highest proportion of patients (69.5%) reaching the MCID threshold, while proportions for MoDA (44.9%) and HDA (45.2%) were similar (Figure 2(b)). Despite improvements in FACIT-Fatigue score for TNFi-IR patients being similar for MoDA and LDA/REM, a distinct association between disease activity and the proportion of patients achieving FACIT-Fatigue MCID was observed (Figure 2(a) and (b)).
Furthermore, in bDMARD-naïve and TNFi-IR patients at week 52/40, achievement of MDA was associated with improvements in both FACIT-Fatigue score and achievement of MCID (Figure 2(a) and (b)). For both bDMARD-naïve and TNFi-IR patients, the achievement of ACR50 + PASI100 response, at week 52/40, resulted in greater improvements in fatigue (Figure 2).
Physical function
Increasingly stringent disease control criteria were associated with sequentially larger mean reductions from baseline in physical function (i.e., improvements), assessed with HAQ-DI, and with increased proportions of patients achieving HAQ-DI MCID and HAQ-DI normative value response. Associations were evident at week 16 (Table 1 and Supplemental Table 2) and sustained when assessed at week 52/40 (Figure 3 and Supplemental Figure 4).

Association of disease activity with physical function captured with HAQ-DI at week 52 for bDMARD-naïve patients and week 40 for TNFi-IR patients (OC). (a) HAQ-DI CfB and (b) HAQ-DI MCID (score decrease ⩾0.35 in patients with baseline score ⩾0.35).
At Week 52, mean reductions from baseline in physical function were greatest for bDMARD-naïve patients at the most stringent ACR response threshold, ACR70 (−0.59), while the ACR20 to <ACR50 and ACR50 to <ACR70 thresholds had similar values (−0.26 and −0.29, respectively; Figure 3A); this trend in associations was mirrored in the proportion of patients achieving HAQ-DI MCID (Figure 3B) and HAQ-DI normative value response (Supplementary Figure 4). At Week 40, sequential improvements in physical function by increasing ACR response thresholds were observed in TNFi-IR patients (Figure 3A). Greater proportions of TNFi-IR patients also achieved HAQ-DI MCID and normative value response at more stringent ACR response thresholds (Figure 3B, Supplementary Figure 4).
Achievement of lower disease activity, assessed by DAPSA disease states, in both bDMARD-naïve and TNFi-IR patients at week 52/40 was also associated with greater mean reductions from baseline in physical function, a trend also observed for the proportion achieving HAQ-DI MCID and normative value response. Patients achieving MDA or ACR50 + PASI100 at week 52/40 had greater improvements in physical function, and higher proportions reached HAQ-DI MCID and normative value response (Figure 3 and Supplemental Figure 4).
Similar results were observed when exploring the associations between stringent disease control and improvement in physical function assessed with the SF-36 PCS for both bDMARD-naïve and TNFi-IR patients at week 16 and week 52/40 (Supplemental Table 2 and Supplemental Figure 5).
Disease impact and HRQoL
At week 52/40, mean reductions from baseline (i.e., improvements) in disease impact, assessed using PsAID-12 total score, were sequentially greater for bDMARD-naïve and TNFi-IR patients that achieved increasingly stringent disease control criteria (Figure 4). The observed trend was sustained from week 16 (Table 1).

Association of disease activity with disease impact on HRQoL at week 52 for bDMARD-naïve patients and week 40 for TNFi-IR patients (OC).
Achievement of MDA, or increasingly stringent ACR response thresholds, was associated with greater improvements in all of the PsAID-12 single-item domain scores, with the greatest improvements observed for pain, fatigue, and functional capacity domains, in both bDMARD-naïve and TNFi-IR patients at week 52/40 (Figure 5).

Association of ACR and MDA response criteria with PsAID-12 single-item domain mean scores at week 52 for bDMARD-naïve patients and week 40 for TNFi-IR patients (OC). (a) ACR response and (b) MDA response.
In bDMARD-naïve and TNFi-IR patients, associations between the most stringent disease control criteria and improvements in HRQoL, assessed using EQ-5D, were observed at week 16 (Supplemental Table 2), and trends further sustained at week 52 and 40, respectively (Supplemental Figure 6). At week 52/40, improvements in EQ-5D-3L VAS and EQ-5D-3L utility values were sequentially greater for bDMARD-naïve and TNFi-IR patients who achieved increasingly stringent disease control criteria, with the exception of DAPSA disease activity in TNFi-IR patients (Supplemental Figure 6A/B). In TNFi-IR patients, achievement of DAPSA LDA/REM resulted in the greatest improvements from baseline in EQ-5D-3L VAS (22.4), while improvements for MoDA (12.3) and HDA (13.2) were similar; clear associations between DAPSA disease activity and EQ-5D-3L utility values were not observed (Supplemental Figure 6A/B).
Skin symptom impact
Although associations between impact and musculoskeletal disease were more marked in this cohort, control of skin disease was also relevant. Achievement of complete skin clearance (PASI100; non-responder, responder), as expected, resulted in reduced impact of skin problems on patients, as assessed with the PsAID-12 skin problem single-item domain score (bDMARD-naïve: non-responder –3.5, responder –4.8; TNFi-IR: non-responder –4.0, responder –4.6, where non-response is defined as PASI < 100%) at week 52/40. The association of complete skin clearance with other PRO measures within this analysis was less defined.
Discussion
In this post hoc analysis, we report that patients with active PsA who achieved increasingly stringent thresholds of disease control with bimekizumab treatment, in general, experienced reduced pain, fatigue, and disease impact, as well as reporting increased physical function and improved HRQoL, irrespective of prior TNFi treatment. Given the negative impact of PsA on patients’ lives, the analysis presented here demonstrates the importance of providing treatment strategies with the intention of achieving the greatest possible disease control and, thus, meeting more stringent disease control criteria.3,4 This approach is in agreement with international treatment guidelines that aim to maximize improvements in patient’s symptoms, physical function, and HRQoL.6–9
The data presented here demonstrate that meeting greater clinical disease control criteria thresholds ACR70, DAPSA LDA/REM, MDA, and ACR50 + PASI100, generally, translates into larger improvements in PsA that can reduce symptoms and positively impact patients’ lives. In particular, pronounced associations were observed between more stringent disease control and reduced pain, as well as increased physical function, both of which are commonly reported by patients as among the most problematic symptoms of PsA and the most important domains for improvement.5,28 Interestingly, while there was an overall association between stringent disease control and improvements in FACIT-Fatigue, the results were less pronounced than for other PRO measures. This may reflect the multifaceted nature of fatigue in PsA, 29 and difficulties associated with quantifying fatigue improvements, and aligns with previous studies that have acknowledged this, particularly for patients who are TNFi-experienced. 30
A key strength of this study is the use of multiple composite clinical efficacy endpoints and a variety of PROs, resulting in a comprehensive analysis of associations. The selected endpoints enabled the assessment of outcomes that are most relevant to patients, including pain, fatigue, physical function, and overall HRQoL. This analysis included both bDMARD-naïve and TNFi-IR patients from two independent trials, showing the relevance to patients across the two PsA populations. Another key strength of this study is the consistency of results at both short and longer timepoints, with results observed at week 16 sustained at the longer-term, week 52/40 assessments across both populations. In addition, patient retention rates were high over the duration of the study, with 90.0% of bDMARD-naïve patients completing week 52 and 92.1% of TNFi-IR patients completing week 40. Taken together, these provide support for the robustness of observed associations presented here.
A limitation of this post hoc analysis is that there is the possibility of internal bias within some of the measures reported here; for example, HAQ-DI is a component of the MDA measure, while pain is a component of the ACR measure. Despite this, similar trends were demonstrated for the PsAID-12, EQ-5D, and SF-36 measures, where no such circularity with PRO measures is present. In addition, the data used in this study were generated in clinical trials, thus limiting the generalizability of these findings to a wider PsA patient population who may not be eligible to enroll in clinical trials. Furthermore, patients with multiple active comorbidities, which could impact their self-evaluation of PRO measures, were not included in the clinical trial populations and therefore may be less applicable to patients in real-world clinical practice. Real-world evidence could potentially provide further support for the findings presented here and strengthen their applicability to clinical practice.
A further limitation is that BE OPTIMAL and BE COMPLETE did not assess the impact of skin disease on HRQoL using a validated tool such as the Dermatology Life Quality Index (DLQI). In addition, the pain VAS measure was specific to arthritis pain and may not have captured general pain, or pain associated with skin symptoms. Furthermore, the outcome used to assess skin disease in this analysis, PASI100, is a very stringent threshold, in which a patient achieving ⩾90% improvement in PASI (PASI90) would be classified as non‑responder which may weaken observed associations with PRO measures. As such, it may have been optimal to explore other PASI thresholds to assess associations with PRO measures. However, the results reported for ACR50 + PASI100 and PsAID-12 skin problem single-item domain scores provide some indication that addressing skin symptoms has a positive impact on patients’ outcomes.
Conclusion
The data presented here demonstrate that the achievement of increasingly stringent thresholds of disease activity with bimekizumab treatment is associated with corresponding greater improvements in PROs, irrespective of prior biologic use.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X241288071 – Supplemental material for Association of achieving clinical disease control criteria and patient-reported outcomes in bimekizumab-treated patients with active psoriatic arthritis: results from two phase III studies
Supplemental material, sj-docx-1-tab-10.1177_1759720X241288071 for Association of achieving clinical disease control criteria and patient-reported outcomes in bimekizumab-treated patients with active psoriatic arthritis: results from two phase III studies by Lars Erik Kristensen, William Tillett, Peter Nash, Laura C. Coates, Philip J. Mease, Alexis Ogdie, Paolo Gisondi, Barbara Ink, Adam R. Prickett, Rajan Bajracharya, Vanessa Taieb, Nikos Lyris, Jérémy Lambert and Jessica A. Walsh in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
The authors thank the patients, the investigators, and their teams who took part in this study. The authors also acknowledge Heather Edens, PhD, UCB, Smyrna, GA, USA, for publication coordination and editorial assistance, Nadine Goldammer for their work as clinical program delivery lead for the bimekizumab PsA program, and David Morgan, PhD, Costello Medical, Manchester, UK, for medical writing and editorial assistance based on the authors’ input and direction. This study was funded by UCB.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.