
Abstract
Background:
The independent association between hepatic steatosis and rheumatoid arthritis is poorly defined.
Methods:
The presence of moderate to severe steatosis was assessed, using liver ultrasonography, in 364 consecutive non-diabetic subjects (223 patients with rheumatoid arthritis and 141 age- and sex-matched healthy controls). Adjusted multiple regression analysis was performed to explore the association between rheumatoid arthritis and moderate to severe steatosis in the overall sample and identify independent risk factors in the rheumatoid arthritis subgroup.
Results:
The prevalence of moderate to severe steatosis in the overall sample was 31.3%, with a significantly higher prevalence in patients with rheumatoid arthritis than healthy controls (38.7% versus 19.7%, p < 0.0001). After adjustment for sex, age, cholesterol, triglycerides, body mass index, waist, hypertension and smoke, rheumatoid arthritis remained significantly associated with moderate to severe steatosis [odds ratio (95% confidence interval) = 2.24 (1.31, 3.84); p = 0.003]. In the rheumatoid arthritis group, male sex, higher body mass index, higher triglycerides concentrations and higher cumulative dosage of methotrexate [odds ratio (95% confidence interval) = 1.11 (1.01, 1.23); p = 0.026] were significantly associated with moderate to severe steatosis, while systemic inflammation, disease activity, use of steroids and biologics were not.
Conclusion:
Rheumatoid arthritis is independently associated with moderate to severe steatosis, with male sex, higher body mass index and cumulative dose of methotrexate being predisposing factors. Further prospective studies are warranted to confirm our findings and to investigate the effect of steatosis on liver outcomes in the rheumatoid arthritis population.
Introduction
Liver steatosis belongs to the spectrum of liver diseases caused by an increase in fat liver content, collectively known as non-alcoholic fatty liver disease (NAFLD). 1 Besides liver steatosis, NAFLD encompasses conditions such as non-alcoholic steatohepatitis, liver fibrosis, cirrhosis and ultimately hepatocellular carcinoma. 1
Patients with rheumatoid arthritis (RA) appear to be at increased risk of developing fatty liver disease/NAFLD given their adverse cardiovascular profile, unfavourable metabolic status, persistent systemic inflammatory burden and chronic exposure to steatogenic drugs such as glucocorticoids and methotrexate.2–7 Fatty liver disease was reported in 22% of 117 liver biopsies performed in patients with RA. 8 More recently, a high prevalence of NAFLD-like lesions was documented in a histological liver study of patients with RA presenting with elevated liver enzymes. 9 In a cross-sectional study by Ursini and colleagues, liver steatosis was demonstrated by ultrasonography in 41 out of 164 (25%) consecutive patients with RA. It appeared to be independently associated with the male gender, increasing body mass index (BMI) and complement C3 concentrations. 10 Similarly, in another study, significant steatosis was demonstrated by abdominal computed tomography in 20 out of 114 patients with RA (18%). It was significantly associated with increased serum triglyceride concentrations, lower high-density lipoprotein (HDL) levels, adiposity measures and systemic inflammation. 11
Despite this preliminary evidence, the independent association between RA and liver steatosis remains poorly defined as no study has also investigated the presence of steatosis in a non-RA control group. We sought to address this issue by examining the overall prevalence of moderate to severe steatosis using liver ultrasound and the variables that are independently associated with this condition in a large consecutive series of patients with RA and healthy controls.
Materials and methods
Patients with RA and healthy controls
Consecutive unselected patients with RA attending the outpatient clinic of the Rheumatology Unit of the Azienda Ospedaliero-Universitaria of Sassari (Italy), and fulfilling the 2010 ACR/European League Against Rheumatism (EULAR) classification criteria for RA, 12 were enrolled in the study. As a control group, we enrolled age- and sex-matched healthy blood donors (controls) attending the local blood transfusion service and authors’ friends and relatives.
Exclusion criteria were the following, as previously published: 13 history of hepatitis B and C virus infection; treatment with hepatotoxic drugs other than RA-specific drugs; alcohol abuse (i30 g/day in men and ⩾20 g/day in women); history or clinical suspicion of Wilson’s disease, α1-antitrypsin deficiency or genetic hemochromatosis; history or clinical suspicion of autoimmune liver disease; recent infection; cancer; and pregnancy. Patients with impaired fasting glucose (fasting glycaemia >106 mg/dl) or diabetes (diagnosed according to the patient’s history and treatment with insulin or oral hypoglycaemic agents) were also excluded from the study.
The following clinical and laboratory data were routinely collected: age, weight, BMI, waist circumference, total cholesterol, triglycerides, aspartate aminotransferase (AST), alanine aminotransferase (ALT) and smoking habit (yes or no). Arterial hypertension was defined as a blood pressure ⩾140/90 mmHg or treatment with antihypertensive medications.
To evaluate the presence of correlations between steatosis and RA-specific features, the following disease-specific scores, disease descriptors and treatment data were collected: current steroid treatment; cumulative dosage of steroids (last 12 months); current treatment with biological or targeted-synthetic disease-modifying anti-rheumatic drugs (b/tsDMARDs); current use of methotrexate; cumulative dosage of methotrexate (from the initial prescription); C-reactive protein (CRP) concentrations, mg/dl; erythrocyte sedimentation rate (ESR), mm/h; clinical disease activity index (CDAI). Cumulative dosages of methotrexate and steroids were ascertained by patients’ interview and medical records review.
Ultrasound
The ultrasound examinations were performed, after overnight fasting, by two experienced investigators (P.M. and G.V.), respectively, with 5 and 20 years of experience in liver ultrasound. Both investigators were blinded to the patient’s condition (patients with RA or healthy controls) and the ultrasound examinations were performed with the same ultrasound scanner, Aixplorer (SuperSonic Imaging, S.A., Aix en Provence, France) and convex broadband probe (SC6-1).
Hepatic steatosis was scored by assessing the severity of hepatic fat infiltration, which takes into account increased liver echogenicity (which makes the liver brighter than the renal cortex), tightly packed echo pattern, portal and hepatic vein blurring, posterior beam attenuation and poor diaphragm visualization.14,15
In particular, steatosis was graded as follows:
(a) Absent, when the echotexture of the liver was normal and there was no difference in terms of echogenicity with renal cortex, combined with absence of deep attenuation and vessel blurring.
(b) Mild, when there was a slight and diffuse increase of liver echogenicity with respect to renal cortex, associated with no ultrasound beam attenuation and regular visualization of the diaphragm and the portal and hepatic veins wall.
(c) Moderate, in case of a moderate increase of liver echogenicity with slightly impaired appearance of the portal or hepatic veins wall and the diaphragm.
(d) Severe, in case of marked increase of liver echogenicity with poor or no visualization of portal vein wall, diaphragm and posterior part of the right liver lobe.
All liver images were saved and then anonymized for the inter-rater agreement assessment by another investigator (A.S.). To avoid recall bias, all images were collected in a folder for each single patient and identified by a number corresponding to the ID of each single patient.
There was almost perfect agreement between the two investigators (P.M. and G.V.) who performed the ultrasounds and did the review of the liver images in classifying the severity of liver steatosis on 171 randomly selected liver ultrasounds: Cohen’s κ = 0.945, 95% confidence interval (CI) = [0.88, 0.95], p < 0.0001 (Supplementary file, Table 1S; p. 1).
Statistical analysis
Normality of data was assessed testing the skewness and kurtosis jointly. Non-normally distributed variables were then reported as median with the interquartile range. Categorical variables were reported as frequencies (n) and percentages (%). RA and control groups were compared with the median and chi-square test, as appropriate. Multiple logistic regression analysis (ENTER method) was performed to assess the association between moderate to severe steatosis and RA in the overall sample and identify variables independently associated with moderate to severe steatosis in the RA population. All biologically plausible variables were included in the multiple regression models; results were expressed as the odds ratio (OR) and 95% CI.
Given the relatively high number of missing data (Supplementary file, Table 2S and 3S; pp 2.3), regression analyses were performed after multiple imputation. Multiple imputation was performed using the multivariate imputation by chained equations (MICE). Forty sets of data were imputed, the analysis was performed on the imputed datasets and model estimates for each regression were then combined using standard methods.
Given the lack of available reliable information about the prevalence and the determinants of moderate to severe steatosis in the RA population, a formal calculation of sample size adjusted for potential confounders was not done: however, considering the prevalence of age-adjusted moderate to severe steatosis in the general population of Western countries being 21% (as reported in the National Health and Nutrition Examination Survey, NHANES III) 16 and assuming a prevalence of moderate to severe steatosis of 34.5% (as estimated in a preliminary evaluation in 50 RA from a previous study) 13 we calculated that a sample size of 363 subjects (case: control = 1.5:1) would be needed to find a statistically significant difference (p < 0.05) with a power of 80%.
The reporting of this study conforms to the STROBE statement. 17 Analyses were performed using Stata 16.1 in Stata 16.1 (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC). A p-value <0.05 was considered statistically significant.
Ethical considerations
All subjects gave their written informed consent before starting the study. The study followed the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the ASL1-Sassari institutional review board (2351/CE_2017).
Results
Patients with RA and controls
We assessed the presence and severity of liver steatosis in 364 subjects (223 patients with RA and 141 controls) (see Table 1), of whom 273 (173 RA and 100 controls) were previously enrolled in a study aimed to evaluate liver fibrosis. 13
Demographic, laboratory and clinical characteristics of patients with RA and controls.

ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; RA, rheumatoid arthritis.
Values are median (interquartile range, IQR).
Mean age, gender distribution and lipid profile were similar across the groups, as per protocol (Table 1). In contrast, hypertension was significantly more prevalent in the RA population than in controls (Table 1). Patients with RA had a long disease duration and moderate disease activity.
The vast majority of patients with RA were under treatment with sDMARDs at the moment of enrolment, with methotrexate being the most frequently used sDMARD (81.5% of patients) (Table 2).
Characteristics of patients with RA.

ACPA, anti-citrullinated peptide antibodies; CDAI, clinical disease activity index; CRP, C-reactive protein concentrations, mg/dl; ESR, erythrocyte sedimentation rate, mm/h; IQR, interquartile range; RA, rheumatoid arthritis; RF, rheumatoid factor; sDMARDs, synthetic disease-modifying anti-rheumatic drugs; TNFi, tumour necrosis factor inhibitors.
Values are median (IQR).
Moderate to severe steatosis
The distribution of steatosis severity classes was significantly different between patients with RA and controls, with a higher prevalence of advanced severity classes of steatosis in the RA population (Table 3). Moderate to severe steatosis was diagnosed in about a third of the overall sample, with significantly higher prevalence in patients with RA than in controls (38.5% versus 19.8% respectively, p < 0.005).
Ultrasonographic parameters in patients with RA and control.

RA, rheumatoid arthritis.
In multivariate logistic regression in the overall sample, performed after multiple imputation analysis, having RA was independently and significantly associated with the presence of moderate to severe liver steatosis at ultrasound examination [OR (95% CI) = 2.24 (1.31, 3.84); p = 0.003] (Table 4). Increasing age, male gender, BMI and triglycerides were also significantly associated with the presence of moderate to severe steatosis in the overall sample (Table 4).
Variables associated with moderate to severe steatosis in the overall sample.
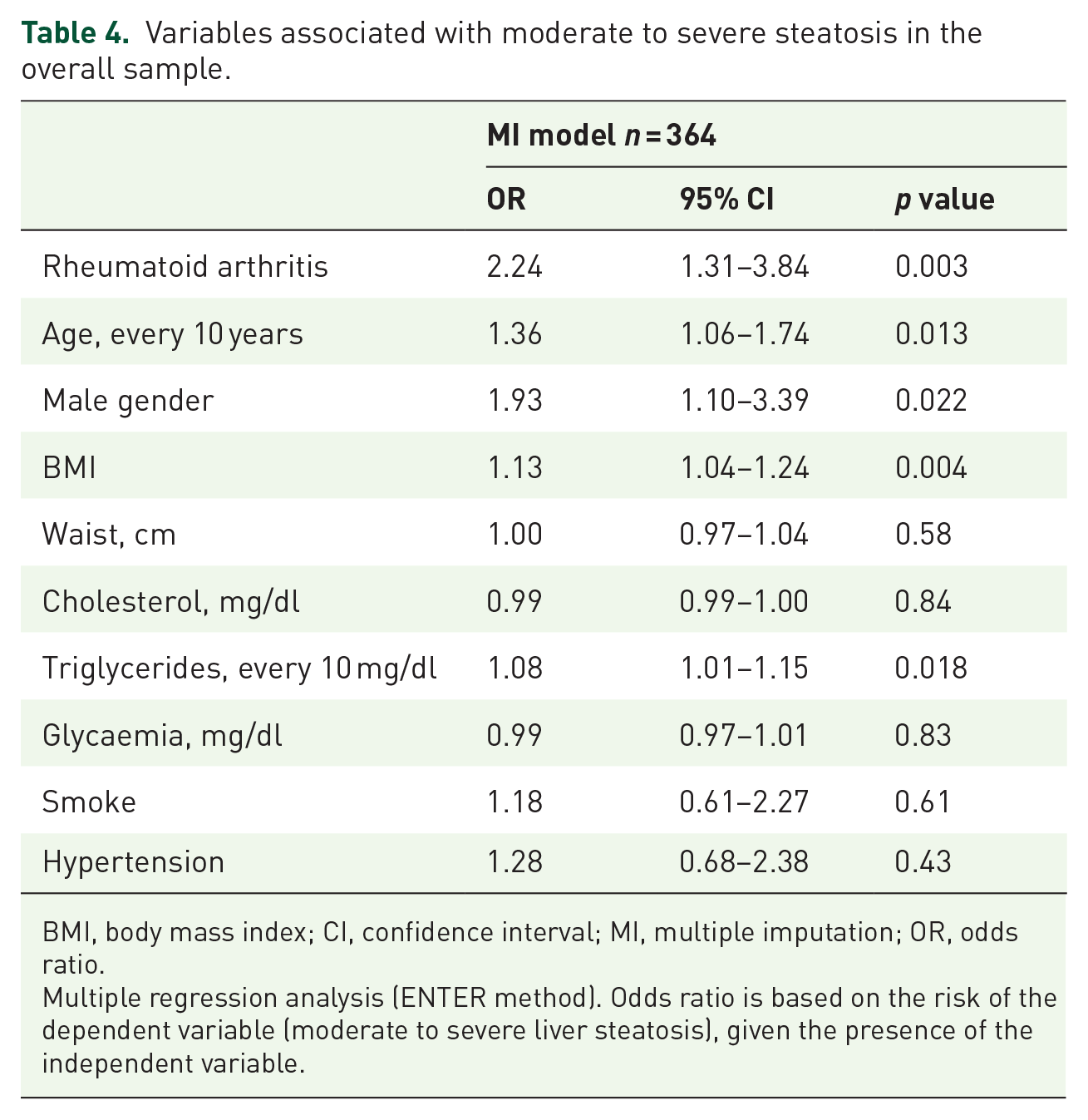
BMI, body mass index; CI, confidence interval; MI, multiple imputation; OR, odds ratio.
Multiple regression analysis (ENTER method). Odds ratio is based on the risk of the dependent variable (moderate to severe liver steatosis), given the presence of the independent variable.
In the multivariate logistic analysis performed in the RA sample, male gender, higher BMI and elevated triglycerides concentrations were significantly associated with moderate to severe steatosis in the RA population. Of interest, increasing cumulative dosage of methotrexate was also significantly associated, [OR (95% CI) = 1.11 (1.01, 1.23); p = 0.026], with the presence of moderate to severe steatosis (Table 5).
Variables associated with moderate to severe steatosis in the rheumatoid arthritis sample.

b/tsDMARDS, biological or targeted-synthetic disease-modifying anti-rheumatic drugs; BMI, body mass index; CDAI, clinical disease activity index; CI, confidence interval; CRP, C-reactive protein; MI, multiple imputation; MTX, methotrexate.
Multiple regression analysis (ENTER method). Odds ratio is based on the risk of the dependent variable (moderate to severe liver steatosis), given the presence of the independent variable.
On the contrary, the use of leflunomide did not significantly associate with moderate to severe steatosis (Supplementary file, Table 4S; p. 4).
Results of logistic regressions performed both in the full and imputed datasets were presented in the Supplementary file (Tables 5S and 6S; pp. 5–6).
Discussion
In this study, we found for the first time a significantly higher prevalence of moderate to severe steatosis in the non-diabetic RA population compared with healthy controls sharing a similar metabolic profile. Our results suggest that at least one every three patients with RA has significant liver steatosis on ultrasound. This figure is significantly higher than that previously reported by other authors documenting a prevalence of steatosis ranging from 18% to 25%.10,11,18 Differences in diagnostic methodologies and steatosis definition are likely to have significantly influenced study results.
Similar to the general population and according to previous studies in patients with RA,10,19 we observed that higher BMI values and male gender are risk factors of fatty liver disease in RA; however, we also demonstrated that having a diagnosis of RA is per se independently associated with an increased risk of moderate to severe liver steatosis. This suggests that factors specifically related to RA may be involved in the development of liver steatosis in this patient group.
In patients with RA, typical body composition changes, including visceral adiposity and intramuscular fat accumulation, have been linked to the development of insulin resistance and metabolic syndrome and therefore are likely to be associated with liver steatogenesis.7,20–22 Moreover, increasing BMI has been linked to high disease activity, refractoriness to treatment and ultimately persistent high-grade systemic inflammation, a condition associated with increased risk of fatty liver disease and NAFLD.7,23 Therefore, it is plausible that a complex interplay between visceral adiposity and systemic inflammation may be involved in liver steatogenesis and that lifestyle modifications leading to weight loss and attainment of a remission/low disease activity may be useful in reducing liver steatosis and the risk of NAFLD progression in patients with RA.
It is also plausible that the autoimmune process involved in RA’s pathogenesis might also substantially contribute to liver damage and fatty liver disease. In fact, despite a clinically overt liver disease is rarely seen in patients with RA, 24 a significant prevalence of ‘mild autoimmune hepatitis’ has been demonstrated in liver biopsies.8,9
The chronic use of drugs linked to the steatogenic liver process may also account for the increased prevalence of significant steatosis in the RA population. Despite its proven benefits in RA,25,26 the use of methotrexate has been linked with liver toxicity.5,6,27,28 Of note, we found a statistically significant association between the cumulative dose of methotrexate and the presence of moderate to severe steatosis in RA. This is of uncertain clinical significance and requires further studies.
The use of glucocorticoids has been linked to accelerated liver steatogenesis and NAFLD, primarily through hyperphagia, gluconeogenesis, insulin resistance, hyperglycaemia, hyperinsulinemia and increased lipogenesis. 29 However, in our series of patients with RA, we found no significant association between the cumulative dosage of steroids and the presence of moderate to severe steatosis.
Increased levels of pro-inflammatory cytokines tumour necrosis factor (TNF)-alpha and interleukin (IL)-6, often observed in RA, have been linked to excessive fatty acids liver deposition, non-alcoholic steatohepatitis and liver fibrosis. 30 Therefore, blunting the TNF signal with TNF inhibitors might theoretically reduce the risk of liver steatogenesis and NAFLD in patients with chronic inflammatory diseases.31,32 Conversely, liver steatosis and steatohepatitis have been documented histologically in patients with RA receiving TNF inhibitors with increased transaminase concentrations. 33 Therefore, the effect of treatment with TNF inhibitors on liver steatogenesis is currently unclear. In our series of patients with RA, we found no significant relationship between the use of TNF inhibitor and other biological and targeted-synthetic drugs and the presence of moderate to severe steatosis.
Our study has some potential limitations. First, the severity of steatosis was indirectly diagnosed using ultrasonography. However, while inferior to liver biopsy for diagnosing steatosis, liver ultrasonography has high specificity for moderate to severe liver steatosis. 34 Furthermore, performing a liver biopsy in patients with relative mild liver diseases is questionable from an ethical perspective. 35 Second, our patients with RA were under immunosuppressive and anti-inflammatory therapy, which may have influenced the study results. Third, the presence of a relationship between insulin resistance and liver steatosis in RA was not formally assessed. Moreover, unmeasured potential confounders (e.g. level of physical activity and alcohol use) may have influenced the distribution of moderate to severe steatosis between groups. Finally, due to this study’s cross-sectional nature, a cause–effect relationship between factors associated with liver steatosis and steatosis itself cannot be firmly established. Therefore, larger prospective studies are required to establish the role of specific risk factors and assess the development and progression of liver steatosis in RA.
Conclusion
Non-diabetic patients with RA have a higher prevalence of moderate to severe steatosis than the general population, with male gender and higher BMI, and cumulative dose of methotrexate being independent risk factors. Further studies are needed to investigate the cause–effect relationship between specific risk factors and liver steatosis and the impact of the latter on clinical outcomes in RA.
Supplemental Material
sj-doc-1-tab-10.1177_1759720X211042739 – Supplemental material for Prevalence and risk factors of moderate to severe hepatic steatosis in patients with rheumatoid arthritis: an ultrasonography cross-sectional case–control study
Supplemental material, sj-doc-1-tab-10.1177_1759720X211042739 for Prevalence and risk factors of moderate to severe hepatic steatosis in patients with rheumatoid arthritis: an ultrasonography cross-sectional case–control study by Gian Luca Erre, Floriana Castagna, Assunta Sauchella, Pierluigi Meloni, Arduino Aleksander Mangoni, Giuseppina Farina, Richard Woodman, Maria Pina Dore and Gianpaolo Vidili in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Author contributions
GLE is the submission’s guarantor. GLE, GV, MPD and AAM designed the research study and wrote the paper; FC, AS, PM, GF and RW collected and analysed the data; all authors approved the final version of the manuscript.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded with a grant from ‘Fondazione Banco di Sardegna’.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.