
Abstract
Background:
Systemic sclerosis (SSc) alterations of the face and of the mouth cause aesthetic modifications and disability, impairing self-esteem and quality of life (QoL). The aim of this study was to verify the effects of two rehabilitation protocols on facial mimic and mouth opening.
Methods:
A total of 47 SSc patients (40 females and 7 males, mean age ± SD 59.08 ± 10.31 years), were consecutively selected: 22 were randomly assigned to protocol 1 [home exercises for temporomandibular joint (TMJ), mimic, masticatory and cervical spine muscles] and 25 to protocol 2 (home exercises and combined physiotherapeutic procedures performed by a physiotherapist). Each treatment had a duration of 12 weeks with a follow up of 8 weeks. TMJ dysfunction, orofacial involvement, disability, QoL, and safety were assessed at enrollment (T0), at the end of the treatment (T1), and at follow up (T2).
Results:
Both Protocol 1 and Protocol 2 induced significant improvements of some clinical and clinimetric parameters, but better results were obtained with Protocol 2. In the comparison between the effects of Protocol 1 and Protocol 2 at T1 and T2, a significant difference was observed only for Mouth Handicap in SSc [MHISS; Total (p = 0.00178] and for MHISS Mouth opening (p = 0.0098) at T1. No significant difference of indices of short-form 36 was observed.
Conclusion:
The present data suggest that TMJ involvement in SSc may be managed by rehabilitation treatments. The action of a physiotherapist prescribing and personalizing exercises may induce better therapeutic effects.
Background
Systemic sclerosis (SSc) is a connective autoimmune disease that affects the immune system and the microcirculation, leading to fibrosis of the skin and internal organs (heart, lungs, kidneys, gastrointestinal system) and affecting the musculoskeletal system. 1
In SSc, the involvement of hands and face causes global disability: the modifications of the face modify aesthetic appearance and cause disability, impairing self-esteem and reducing quality of life (QoL).2,3
Skin and subcutaneous tissues fibrosis and atrophy lead to the disappearance of wrinkles and hypo- or amimia. In this process, the sclerosis and thinning of mimic muscles provoke a sharp nose, thin lips (microcheilia) with a reduction in mouth opening (microstomia).4–6
Among other SSc facial alterations, patients may present with teleangectasia, especially in the perioral and oral mucosa,4–7 trigeminal neuropathy, 8 xerophthalmia, and xerostomia.4–7,9 In 70% of SSc patients, microstomia may be due to fibrosis of the face and oral mucosa and to alterations of the temporomandibular joint (TMJ). On X-ray, this joint may show bone resorption of the condyles and of the jaw angle (“whale tail”). Rarely, as a consequence of bone resorption, pathological fractures of the jaw may develop.4–7 Moreover, it makes chewing and speaking, as well as maintaining adequate oral hygiene and dental care, problematic.
In SSc, studies assessing TMJ involvement report a higher prevalence of symptoms and clinical signs.10–12 Despite the evidence, only a few studies have addressed and proposed treatments for these problems.5–7,9,11–13 For severe microstomia, sometimes surgery is required (bilateral commissurotomy),4,6 but preventative rehabilitation is preferable, although not widely used. Protocols including stretching exercises of mimic muscles and exercises aimed to prevent and reduce microstomia have improved mouth opening in a small number of SSc patients.13,14
In SSc, our previous data have shown the efficacy of a combined program of face rehabilitation (based on connective tissue massage, Kabat technique, physiokinesitherapy performed by and under the guidance of a physiotherapist) in improving face skin score, mouth opening, and mouth disability with respect to home exercises only.15,16 Moreover, we have also shown that the efficacy of a rehabilitation program, including district rehabilitation of face and hands and global rehabilitation (land-based kinesitherapy and hydrokinesitherapy); at the end of the treatment, SSc patients exhibited improved QoL, global disability and disability and mobility of hands and mouth, with the hands’ improvement maintained also at follow up. 17
The aim of the present study was to evaluate the effects on TMJ of two specifically designed rehabilitation protocols in SSc.
TMJ, mouth and neck involvement were assessed by validated questionnaires and scales, to evaluate the clinical features of those patients with TMJ involvement and dysfunction and to verify the effects on TMJ of two specifically designed rehabilitation protocols.
Patients and methods
Patients
A total of 47 SSc patients [40 females and 7 males with mean age ± standard deviation (SD) 59.08 ± 10.31 years and disease duration ± SD 13.65 ± 5.71 years] were enrolled from the outpatient clinic of the Rheumatology Unit, Department of Experimental and Clinical Medicine of the University of Florence.
Inclusion criteria were classification of SSc according to American College of Rheumatology/ European Alliance of Associations for Rheumatology (ACR/EULAR) criteria and at least one of the following characteristics 18 :
(a) Measurement of mouth opening ⩽40 mm;
(b) Score ⩾8 of Mouth Handicap in SSc (MHISS) subscale assessing the disability related to reduced mouth opening (items 1, 3, 4, 5, and 6); 19
(c) Helkimo clinical index >1. 20
At enrollment, patients were evaluated for clinical and demographic data [sex, years from diagnosis and disease subset [limited or diffuse cutaneous subset SSc (lSSc or dSSc)], 21 organ (skin, lung, heart, gastrointestinal, renal) involvement and autoantibody pattern, according to international guidelines]. 22
All SSc patients continued their pharmacological treatment and did not begin any other physiotherapy treatment.
Following enrollment, participants were randomly assigned to protocol 1 or protocol 2. The study was approved by the local ethics committee (711/12) and written informed consent form was signed by all patients.
Study design
A total of 22 patients (18 females and 4 males; mean age ± SD 63.68 ± 9.45 years; disease duration: mean ± SD 13.59 ± 6.18 years) were assigned randomly to protocol 1 and 25 (22 females and 3 males; mean age ± SD 58.92 ± 10.20 years; disease duration: mean ± SD 11.60 ± 6.38 years) to protocol 2. Protocol 1 included home exercises (20 min/day, 3 times/week) for TMJ, mimic, masticatory and cervical spine muscles, while Protocol 2 included home exercises (20 min/day, 3 times/week) and a combined procedure (once a week; 45 min/session) comprising connective tissue massage of face and neck, Kabat technique applied to mimic muscles, and manual techniques (intra- and extra-oral TMJ manipulation, stretching and mobilization of the cranio-cervical district).
Each protocol had a total duration of 20 weeks (5 months), i.e., 12 weeks (3 months) of treatment and 8 weeks (2 months) of follow up. Both rehabilitation protocols were discontinued or suspended if they caused adverse effects such as increased pain and fatigue in the treated areas.
Techniques
Home exercises, to be performed at home, were taught by an expert physiotherapist at enrollment to all SSc patients (organized in small groups). Such exercises included self-maneuvers of joint release of TMJ, stretching of the cheeks and mouth, movement in order to exercise mimic and cervical spine muscles and coordinate masticatory muscles.
Connective tissue massage treats the altered connective tissue by stretching techniques, based on a deep tissue massage by skin sliding on its support (e.g., bones, tendons and muscles) in order to improve blood flow and to relax the connective tissue. 7 Face, neck, and sopraclavear areas were treated. 23
The Kabat technique is a neurorehabilitation technique that uses diagonal and spiral movements, stretching, and resistance movements, and other facilitation techniques to reinforce the proprioceptive neuromuscular recruitment. In the face, the orbicularis muscle of the mouth, the zygomatic muscle, upper lip elevator, nasal, buccinator, front, and corrugator muscles are stimulated. 24 Proprioceptive neuromuscular facilitation (Kabat technique) is based on a succession of contraction-relaxation-stretching of the muscle.
Manuals techniques, performed by the therapist, included intra- and extra-oral manipulations of TMJ, exercises of neuromuscular coordination for the TMJ, stretching, and mobilization of the cervical region, including tongue muscles, hyoid, and tracheal muscles.14–17,19
Assessment
Patients were assessed at enrollment (T0), after 12 weeks of treatment (T1) and after 8 weeks of follow up (T2) for:
(a) Patient history;
(b) Face skin score: the modified Rodnan skin score (mRSS) (from 0 to 3) was used 25 ; mRSS was assessed in the following regions: forehead, right check, left check, and neck. The four values were added to obtain a total mRSS for every patient;
(c) Mouth opening: the maximum mouth opening was evaluated as a mean (in millimeters) of the two measurements of the distance between central incisors (from the lower edge of the upper incisors to the upper edge of the lower incisors) adding the amount of vertical incisor overbite.14,15 A Thera Bite device was used;
(d) Clinical evaluation of TMJ: evaluation of joint play, joint sounds (clicks or crackling) and TMJ pain induced by palpation or TMJ movement (opening, closing, laterality, protrusion);
(e) Evaluation of cervical spine movements [flexion-extension, lateral flexion, rotation of the head on the spine (cm)];
(f) Helkimo index – a score ranging from 0 to 25 (0 = absence of clinical symptoms; 1–4 = minor dysfunction; 5–9 = moderate dysfunction; 10–25 = severe dysfunction) 20 ;
(g) MHISS: evaluated by 12 items (ranging score of each item = 0–4); the total score (range 0–48) is divided into three partial scores concerning: (1) the disability related to the reduced mouth opening (five items; score ranging 0–20), (2) the handicap correlated to Sicca syndrome (five items; score ranging 0–20), (3) aesthetic problems (two items; score ranging 0–8) 17,19,26;
(h) Medical Outcomes Survey Short Form 36 (SF36): this questionnaire, including 10 subscales, was used to assess QoL.8,27
(i) Safety was evaluated by recording the occurrence of adverse effects due to the treatment.
The characteristics of patients assigned to Protocol 1 and Protocol 2 are reported in Tables 1 and 2. They were evaluated to verify the homogeneity of the study population at T0.
Anamnestic and clinical characteristics of patients of Protocol 1 and Protocol 2.
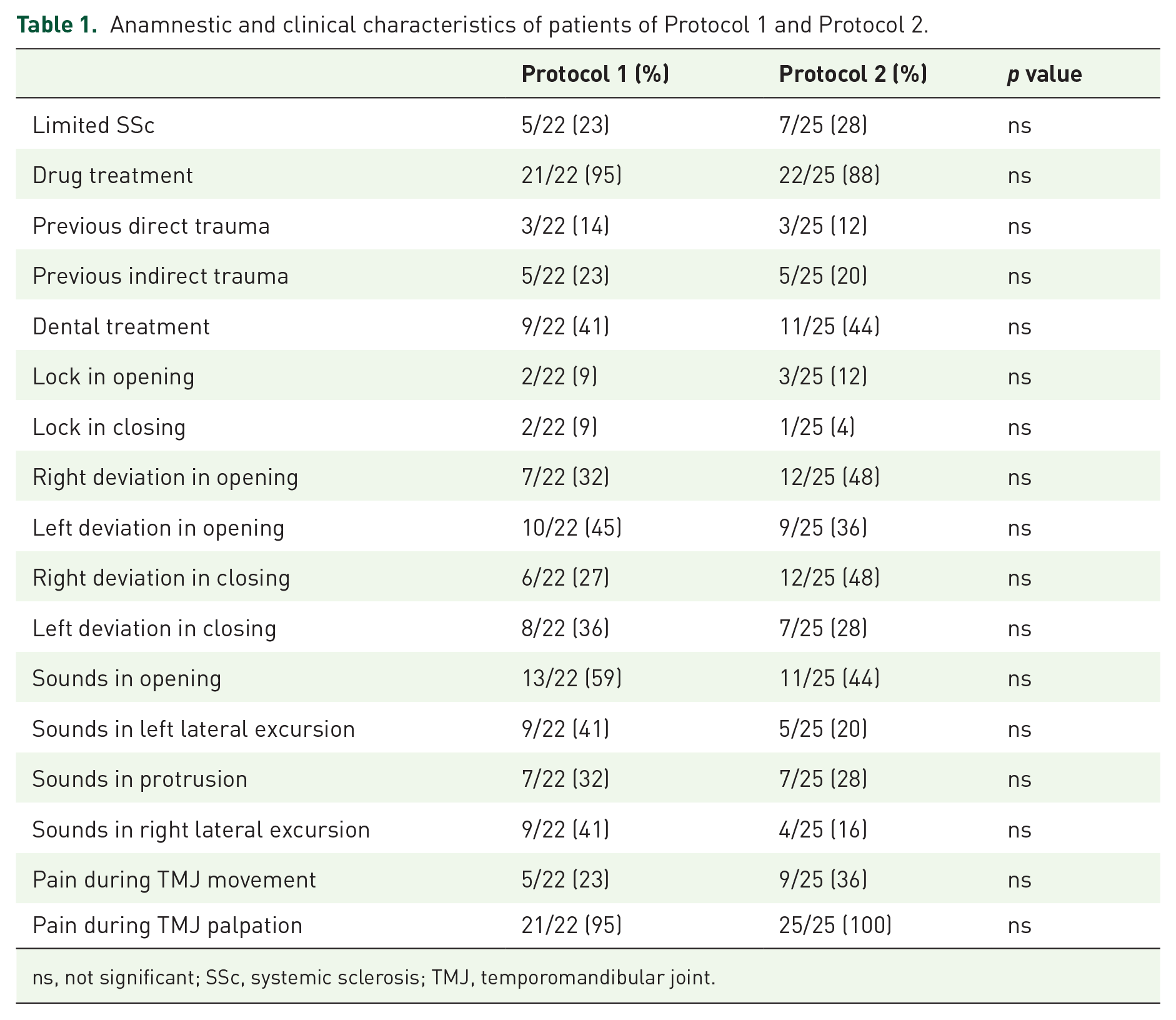
ns, not significant; SSc, systemic sclerosis; TMJ, temporomandibular joint.
Clinical characteristics of patients of Protocol 1 and Protocol 2.

mRSS was assessed in the following regions: forehead, right check, left check and neck: the four values were added to obtain a total mRSS for every patient.
MHISS, mouth handicap in systemic sclerosis scale; mRSS, modified Rodnan skin score; ns, not significant.
Statistical analysis
Demographic, clinical and clinimetric characteristics of the two groups were presented as mean ± SD for continuous variables and as numbers and percentages for binomial variables.
To evaluate the difference in continuous variables at T0 and groups unpaired t test, Satterthwait t test or Mann–Whitney test, according to Shapiro–Wilk test for normality and Bartlett test for homoschedasticity, were used.
To assess the association between categorical variables at T0 and groups, the Fisher exact test was used.
In order to evaluate the change in each item between T2, T1, and T0 paired t test or Signed rank test, according to Shapiro–Wilk test for normality, were used.
To assess the difference in change in each item at T1 and T2 between groups unpaired t test, Satterthwait t test or Mann–Whitney test, according to Shapiro–Wilk test for normality and Bartlett test for homosedasticity, were used.
All analyses were performed using SPSS version 20.0 for Windows (SPSS, Chicago, IL, USA).
Results
Results are shown in Tables 3–9.
Protocol 1 patients: effect of treatment (skin score, mouth opening and neck movement).

mRSS was assessed in the following regions: forehead, right check, left check and neck: the four values were added to obtain a total mRSS for every patient.
mRSS, modified Rodnan skin score.
Protocol 1 patients: effect of treatment (Helkimo and MHISS indices).

MHISS, mouth handicap in systemic sclerosis scale; ns, not significant; T0, before treatment; T1, end of treatment; T2, follow up after 8 weeks.
Protocol 2 patients: effect of treatment (skin score, mouth opening and neck movement).
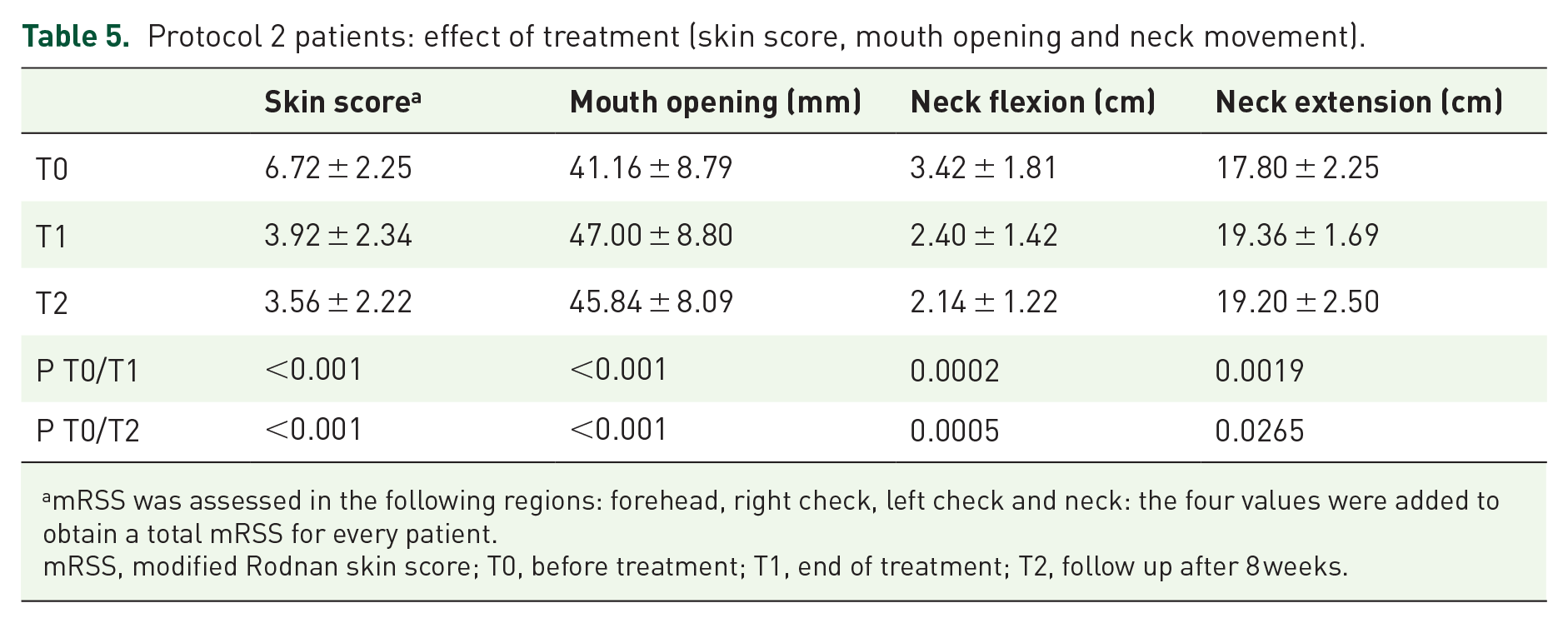
mRSS was assessed in the following regions: forehead, right check, left check and neck: the four values were added to obtain a total mRSS for every patient.
mRSS, modified Rodnan skin score; T0, before treatment; T1, end of treatment; T2, follow up after 8 weeks.
Protocol 2 patients: effect of treatment (mouth opening and neck movement).

MHISS, mouth handicap in systemic sclerosis scale; ns, not significant; T0, before treatment; T1, end of treatment; T2, follow up after 8 weeks.
Induced pain and joint sounds in Protocol 1 and Protocol 2 patients.

ns, not significant; T0, before treatment; T1, end of treatment; T2, follow up after 8 weeks; TMJ, temporomandibular joint.
Comparison of differences of effects between Protocol 1 and Protocol 2 at T1.

MHISS, mouth handicap in systemic sclerosis scale; ns, not significant; T1, end of treatment.
Comparison of differences of effects between Protocol 1 and Protocol 2 at T2.

MHISS, mouth handicap in systemic sclerosis scale; ns, not significant; T2, follow up after 8 weeks.
Protocol 1 induced a significant improvement of skin score at T1 (p = 0.0021) and T2 (p < 0.0001), of mouth opening at T1 (p = 0.0006) and at T2 (p = 0.0004) of neck flexion at T1 (p = 0.0175) and at T2 (p = 0.0223), of neck extension at T1 (p = 0.0005) and at T2 (p = 0.0025), of Helkimo disfunction index at T1 (p = 0.0045) but not at T2, of MHISS total at T2 (p = 0.0413) and of MHISS Sicca Syndrome at T2 (p = 0.0216).
Protocol 2 obtained a significant improvement of the following parameters: Skin Score at T1 (p < 0.001) and T2 (p < 0.01); mouth opening at T1 (p < 0.001) and T2 (p < 0.001); neck flexion at T1 (p = 0.0002) and T2 (p = 0.0005); neck extension at T1 (p = 0.0019) and T2 (p = 0.0265); Helkimo anamnestic index at T1 (p = 0.0005) and T2 (p = 0.0501); Helkimo disfunction index at T1 (p < 0.0001) but not at T2; MHISS total at T1 (p = 0.0002) and T2 (p = 0.0008); MHISS opening of the mouth at T1 (p = 0.0001) and T2 (p = 0.0007); MHISS Sicca Syndrome at T1 (p = 0.0111) and at T2 (p = 0.0499); MHISS aesthetic problems at T1 (p = 0.0201). (Tables 3–6). In Protocol 2, pain induced by movements of the mandible (7) was reduced only at T2 (p < 0.05). In the comparison between the effects of Protocol 1 and Protocol 2 at T1 and at T2 (8 and 9), a significant difference was observed only for MHISS Total (p = 0.00178) and for MHISS Mouth opening (p = 0.0098).
No significant difference of indices of SF36 was observed.
Discussion
Our study shows that facial and TMJ rehabilitation is useful for improving mouth movements and reducing pain in patients with SSc.
In SSc, dysfunction and X-ray changes seen in TMJ are described in some case reports and in a few observational studies.4–6,10–12 In the study of Haers et al., systematic X-ray screening of different SSc groups showed a resorption of the mandible in 20–33% of cases. 28 Matarese et al. assessed TMJ involvement by magnetic resonance imaging (MRI) and found degenerative bone changes in 66.6% of patients. 11 Mandibular resorption was usually detected 5–7 years after SSc diagnosis.11,29,30 Other pathologic conditions, such as local infection, necrotic bone damage, and trigeminal neuropathy were described.29,30 In SSc, TMJ dysfunction may be related to progressive reduction and loss of skin elasticity due to local skin ischemia and to increased skin thickness, and may be associated with reduced mandibular movements and to alteration of the position of the condyle. 11 A high prevalence of these symptoms in SSc was reported in previous investigations and the most frequently reported symptoms were TMJ sounds followed by deviation during mouth opening.9–11
As already highlighted, despite the high prevalence of TMJ dysfunction, only a few studies have assessed the effects of rehabilitation protocols in SSc.13–15 In the present study, the combined involvement of TMJ, mouth, and neck in SSc patients was investigated, and the effects of two specifically designed physiotherapy protocols were tested on a large spectrum of clinical and clinimetric characteristics. The effects of two rehabilitation protocols were compared in patients with SSc and TMJ involvement: Protocol 1 included only home exercises; Protocol 2 included home exercises and connective tissue massage, Kabat technique, and manual techniques performed by a physiotherapist.
In our study, both rehabilitation protocols induced an improvement of some clinical and clinimetric variables (face skin score, mouth opening, neck mobility, pain), with a long lasting effect. It is interesting to note that the results of the present investigation demonstrated that SSc with TMJ involvement may be managed not only by pharmacological therapy but also by rehabilitation treatments. Moreover, the action of a physiotherapist prescribing and personalizing exercises may induce better results. 16
In SSc patients, TMJ involvement is one of the most important causes of pain and reduced mouth opening, leading to severe disability12,14,15: the improvement of these clinical aspects should be the goal of rehabilitation. Furthermore, our study stressed the relationship between neck involvement and TMJ dysfunction with skin fibrosis. In fact, neck-related symptoms are associated frequently with TMJ involvement in SSc patients and contribute significantly to TMJ-related disability.14,15,31,32 On the other hand, SSc patients may suffer also from neck limitation due to fibrosis. 31 Therefore, in these patients it is important to evaluate neck disability and to include specific exercises in rehabilitation protocols.
It is interesting to observe that, in the present study, better results were obtained by the rehabilitation protocol including stretching, connective tissues massage, and neuro-rehabilitation techniques performed by a physiotherapist, improving neuromuscular recruitment.
Early integration of drug treatment with individual rehabilitation programs could also be useful in preventing severe complications such as condylar resorption or fractures.
The limitations of the present study are the small sample size, the short follow up, which does not allow the assessment of a change of QoL and the possible effect of the pharmacological therapy. In the future, it may be useful to observe and compare the effects of home-based or combined rehabilitation programs over a longer period and to compare the effects of adding rehabilitation to drugs with only drugs (e.g., rituximab), which may have an action on the skin. 33
In conclusion, selection of appropriate and comprehensive rehabilitative programs, in particular in the early phase of the disease, might improve TMJ dysfunction, mouth and neck function, pain, and finally health-related Qol. Further studies are needed to evaluate the long-term effects of these different rehabilitation programs in order to create standard protocols.