
Abstract
Background:
Giant cell arteritis (GCA) is the most common systemic vasculitis. Relapses are frequent. The aim of this study was to identify relapse risk factors in patients with GCA with complete large-vessel imaging at diagnosis.
Methods:
Patients with GCA followed in our institution between April 1998 and April 2018 were included retrospectively. We included only patients who had undergone large vascular imaging investigations at diagnosis by computed tomography (CT)-scan and/or positron emission tomography (PET)-scan and/or angio-magnetic resonance imaging (MRI). Clinical, biological, and radiological data were collected. Relapse was defined as the reappearance of GCA symptoms, with concomitant increase in inflammatory markers, requiring treatment adjustment. Relapsing patients (R) and non-relapsing patients (NR) were compared. Relapse and multiple relapses (>2) risk factors were identified in multivariable Cox analyses.
Results:
This study included 254 patients (73.2% women), with a median age of 72 years at diagnosis and a median follow up of 32.5 months. At diagnosis, 160 patients (63%) had an inflammatory large-vessel involvement on imaging, 46.1% (117 patients) relapsed at least once, and 21.3% (54 patients) had multiple relapses. The median delay of first relapse after diagnosis was 9 months. The second relapse delay was 21.5 months. NR patients had more stroke at diagnosis than R (p = 0.03) and the brachiocephalic trunk was involved more frequently on CT-scan (p = 0.046), as carotids (p = 0.02) in R patients. Multivariate Cox model identified male gender [hazard ratio (HR): 0.51, confidence interval (CI) (0.27–0.96), p = 0.04] as a relapse protective factor, and peripheral musculoskeletal manifestations [HR: 1.74 (1.03–2.94), p = 0.004] as a relapse risk factor. Peripheral musculoskeletal manifestations [HR: 2.78 (1.23–6.28), p = 0.014], negative temporal artery biopsy [HR: 2.29 (1.18–4.45), p = 0.015], large-vessel involvement like upper limb ischemia [HR: 8.84 (2.48–31.56), p = 0.001] and inflammation of arm arteries on CT-scan [HR: 2.39 (1.02–5.58), p = 0.04] at diagnosis were risk factors of multiple relapses.
Conclusion:
Male gender was a protective factor for GCA relapse and peripheral musculoskeletal manifestations appeared as a relapsing risk factor. Moreover, this study identified a particular clinical phenotype of multi-relapsing patients with GCA, characterized by peripheral musculoskeletal manifestations, negative temporal artery biopsy, and large-vessel involvement with upper limb ischemia or inflammation of arm arteries.
Plain language Summary
46.1% of patients with GCA relapse, and 21.3% undergo multiple relapses;
Male gender appears as a protective factor for relapsing in GCA;
Peripheral musculoskeletal manifestations are a relapse and multiple relapses risk factor;
A negative temporal artery biopsy is predictive of multiple relapses;
Large-vessel involvement is predictive of multiple relapses.
Keywords
Introduction
Giant cell arteritis (GCA) is the most common vasculitis in people over 50 years of age, 1 typically affecting temporal arteries and other branches of external carotids, but also the aorta and its branches, 2 mainly brachiocephalic trunk, subclavian, axillary arteries, carotids, and vertebral arteries. Symptoms usually include headache, vision disturbances, jaw claudication, tender or swollen superficial temporal arteries, scalp tenderness, polymyalgia rheumatica (PMR), or nonspecific symptoms such as fever, weight loss, and asthenia.3,4 In around 50% of cases in some series, and sometimes even higher, patients develop extracranial large vessel involvement (LV-GCA), leading to limb claudication, stroke, aortic aneurysm, dissection/rupture, or aortic insufficiency.5–9 In GCA, relapses are frequent, occurring in at least 40% of cases, mostly during progressive steroids tapering, and at low doses (prednisone 5–15 mg/day). Thus, this leads to increased duration and cumulative doses of steroids, and to discuss steroid sparing treatments like tocilizumab and methotrexate.10–13 Corticosteroid treatment is often associated with side effects, occurring in 36–86% of cases, such as diabetes, hypertension, gastrointestinal bleeding, posterior subcapsular cataracts, psychiatric complications, myopathy, infections, and osteoporotic fractures.14–16
Factors associated with GCA relapses remain poorly known. Female gender has been described as a predictor of relapse, as well as anemia (Hb < 12 g/dl).12,17 Serum interleukin-6 (IL-6) levels may help predict relapse under tocilizumab treatment. 18 On the other hand, C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) levels at diagnosis have not been associated with relapse.11,19 Recent data in the literature suggest that LV-GCA patients (patients with large-vessel vasculitis) are more prone to relapse and to die than patients with isolated cranial involvement. Moreover, patients with stroke at diagnosis seem to have a less relapsing course.20,21 In accordance with this, our group has previously suggested that inflammatory aortic involvement at diagnosis of GCA could predict a more chronic/relapsing course. 22
Patients with GCA are increasingly benefiting from imaging of large arteries at diagnosis. However, prognosis of LV-GCA at diagnosis remains unclear. To our knowledge, there is no study of GCA relapse risk factors in a large cohort of patients with detailed arterial evaluation at diagnosis. The aim of this study was to identify risk factors for relapse in GCA patients who had a systematic large-vessel imaging at diagnosis.
Methods
This retrospective study included GCA patients diagnosed between April 1998 and April 2018 in Nantes University Hospital, France. They fulfilled the GCA American College of Rheumatology (ACR) 1990 criteria or were aged over 50 years old, CRP > 10 mg/l, and one or more GCA clinical signs and involvement of large vessels with wall inflammation on imaging.23,24 Each patient had an imaging assessment of large vessels at diagnosis of GCA, by computed tomography (CT)-scan and/or positron emission tomography (PET)-scan and/or angio-magnetic resonance imaging (MRI), and had a follow up of at least 6 months (unless they died before then). We excluded patients who only had a Doppler ultrasound vascular exploration and patients with insufficient data on their records.
Each previously defined GCA patient had a PET-scan, an injected CT-scan and/or an angio-MRI to evaluate the large vessels at GCA diagnosis. Patients were included whether or not the imaging revealed vascular inflammatory involvement due to GCA.
All medical files of the patients were reviewed. Many of them have been the subject of a standardized collection of disease characteristics since the initiation of our center’s research studies in 1998.2,22,25–27 We collected 247 parameters, including demographic features, comorbid conditions, systemic and associated GCA symptoms like PMR meeting the European League Against Rheumatism (EULAR) criteria, 28 or any other peripheral musculoskeletal manifestations not meeting PMR criteria (peripheral arthritis/synovitis, polyarthritis/polyarthralgia, myalgia, or rheumatoid arthritis meeting the ACR criteria, 29 extremity swelling with or without pitting edema, distal tenosynovitis) but improving under corticosteroids. A GCA cranial involvement was defined by the presence of headaches, and/or temporal artery tenderness or swelling, and/or jaw claudication, and/or scalp tenderness and/or ophthalmological signs of GCA.
We also collected laboratory assessments, histological parameters and imaging data at diagnosis. Therapeutic and follow-up data, including relapses, vascular events (occurrence of any aortic event like aortic dissection or symptomatic aortic aneurysm, myocardial infarction, stroke, limb or mesenteric ischemia and de novo stage 3 or 4 lower limbs arteritis), and death-associated data, were also collected in a standardized anonymized electronic form.
An aortic involvement at diagnosis was defined by aortitis (circumferential aortic parietal thickening >2.2 mm on CT-scan/MRI, and/or a grade 2 or 3 parietal aortic hypermetabolism on PET-scan), aneurysm (a thoracic aortic diameter >4 cm or abdominal aorta diameter >3 cm) or by aortic dissection.
Inflammatory involvement of the peripheral arteries was defined by long circumferential hypoechoic thickening >1 mm without atherosclerotic lesion (calcification or irregular soft atheroma) on CT and/or Doppler ultrasound. Arm arteries included axillary and brachial arteries. The brachiocephalic trunk is the first artery coming from the aorta with a cephalic destiny, which will divide into the right subclavian and the right common carotid artery.
LV-GCA patients were patients with large-vessel vasculitis on imaging, including patients with aortitis and/or patients with inflammatory involvement of the peripheral arteries.
Relapse was defined as the reappearance of GCA symptoms (or appearance of new GCA symptoms), with a concomitant increase in inflammatory markers, requiring treatment adjustment. 30 Multiple relapses were defined as the occurrence of at least two relapses during follow up. This study has been conducted in compliance with the Declaration of Helsinki principles and has received ethics board approval by GNEDS (Groupe Nantais d’Ethique et de Soin), the local ethics committee of the University Hospital of Nantes (20200108). Each patient included in this study received written information and no patient objected to this study. The need for written informed consent was waived by the Ethics Committee because of the retrospective study design (French public health code article: L 1121-1).
Quantitative variables were described as median (Quartile 1–Quartile 3) and mean [± standard deviation (SD)]. Qualitative variables were described as number (%). The two patients groups with Relapsing (R) and non-relapsing (NR) patients were compared using the Fisher exact test for categorical variables and Student tests (Mann–Whitney test when n < 30) for quantitative variables. In all cases, statistical significance was assumed for p < 0.05. A univariable Cox model was used to identify factors associated with relapse. All baseline variables with a p value <0.20 in univariable analysis and variables already known to be confounding factors were included in multivariable Cox model. The hazard ratio (HR) and the confidence intervals (CI) are presented in the Tables. The relationship between recorded variables and the occurrence of multiple relapses has been assessed too. Statistical analysis was performed with SPSS v26 (IBM Corp. Armonk, NY, USA). The multivariate analysis was performed only on our 229 patients who had a CT-scan, for quality and statistical consistency.
Results
This study included 254 patients; among 804 patients identified by our Department of Medical Information, we excluded 171 patients miscoded, 349 patients without a vascular imaging evaluation at diagnosis, and 30 patients with less than 6 months of follow up or insufficient data. Main clinical characteristics and laboratory assessments at diagnosis are summarized in Table 1. The median follow-up was 32.5 months.17"/>-53
Main characteristics of the cohort at diagnosis of GCA.

Data are expressed as median (IQR) and number/available data (percentage), n (%).
Peripheral musculoskeletal manifestations included peripheral arthritis/synovitis, polyarthritis/polyarthralgia, willingly with myalgia, rheumatoid arthritis meeting the ACR criteria in two cases (with positive temporal artery biopsy), extremity swelling with or without pitting edema, distal tenosynovitis.
ACR, American College of Rheumatology; BMI, body mass index; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; GCA, giant cell arteritis; IQR, interquartile range.
A total of 56 patients (22.3%) had PMR at diagnosis. Peripheral musculoskeletal manifestations at diagnosis (n = 64, 26.4%), not meeting PMR criteria but improving under corticosteroids, related to peripheral joints or periarticular pain, were associated with PMR in 37 patients.
At diagnosis, 160 of our 254 patients (63%) had an inflammatory large-vessel involvement on imaging; 56 of the 79 patients (70.9%) who had a PET-scan, 9 of the 13 patients (69.2%) who had angio-MRI, and 122 of the 229 (53.3%) patients with CT-scan. The mean thickness on CT-scan was 4.2 ± 1.9 mm (±SD) and 40 aortic aneurysm or ectasia (15.7%) were identified at GCA diagnosis. Descriptions of the patterns of vascular involvement at diagnosis of GCA are summarized in Table 2.
Description of the patterns of vascular involvement at diagnosis of GCA.

GCA, giant cell arteritis; LV-GCA, large vessel giant cell arteritis.
A total of 46 of the 94 patients (48.9%) with isolated cranial GCA, 49 (45.8%) of the 107 GCA patients with both cranial and large vessel involvement, and 22 (41.5%) of the 53 patients with isolated LV-GCA had at least one relapse. Relapsing rates were not significantly different between these groups (p = 0.68).
Among the 53 patients with isolated LV-GCA at imaging (no cranial symptoms), 10 had PMR at diagnosis and 13 had peripheral musculoskeletal manifestations. Among the 10 patients who had PMR, 6 had a positive TAB, 3 had isolated aortitis, and 7 had aortitis plus peripheral arteries inflammatory involvement.
Table 3 presents the characteristics of therapeutics. A total of 40 patients (15.9%) received methylprednisolone infusion therapy at diagnosis: 19 patients with ocular involvement, 3 with upper limb ischemia, 2 with lower limb ischemia, 3 with stroke, 2 with aortic dissection, 1 with carotid dissection, 4 with extensive arterial involvements at CT-scan, and 6 received infusions without ophthalmological or vascular complications; 54 patients (24.7%) received immunosuppressive treatments, in relapsing patients or as glucocorticoid-sparing agents to reduce comorbidity related to prolonged glucocorticoid therapy: 39 (72.2%) received methotrexate, 7 (13%) received hydroxychloroquine, 6 (11.1%) azathioprine, 5 (9.3%) tocilizumab, 2 (3.7%) cyclophosphamide, and 1 leflunomide. Sometimes, several immunosuppressive treatments were required. There were 8 patients who received immunosuppressive treatments at diagnosis, and 46 received these treatments subsequently, in the context of a first relapse in 26 patients, a second relapse in 13 patients, a third relapse in 3 patients, early corticoresistance in 1 patient.
Therapeutic management.
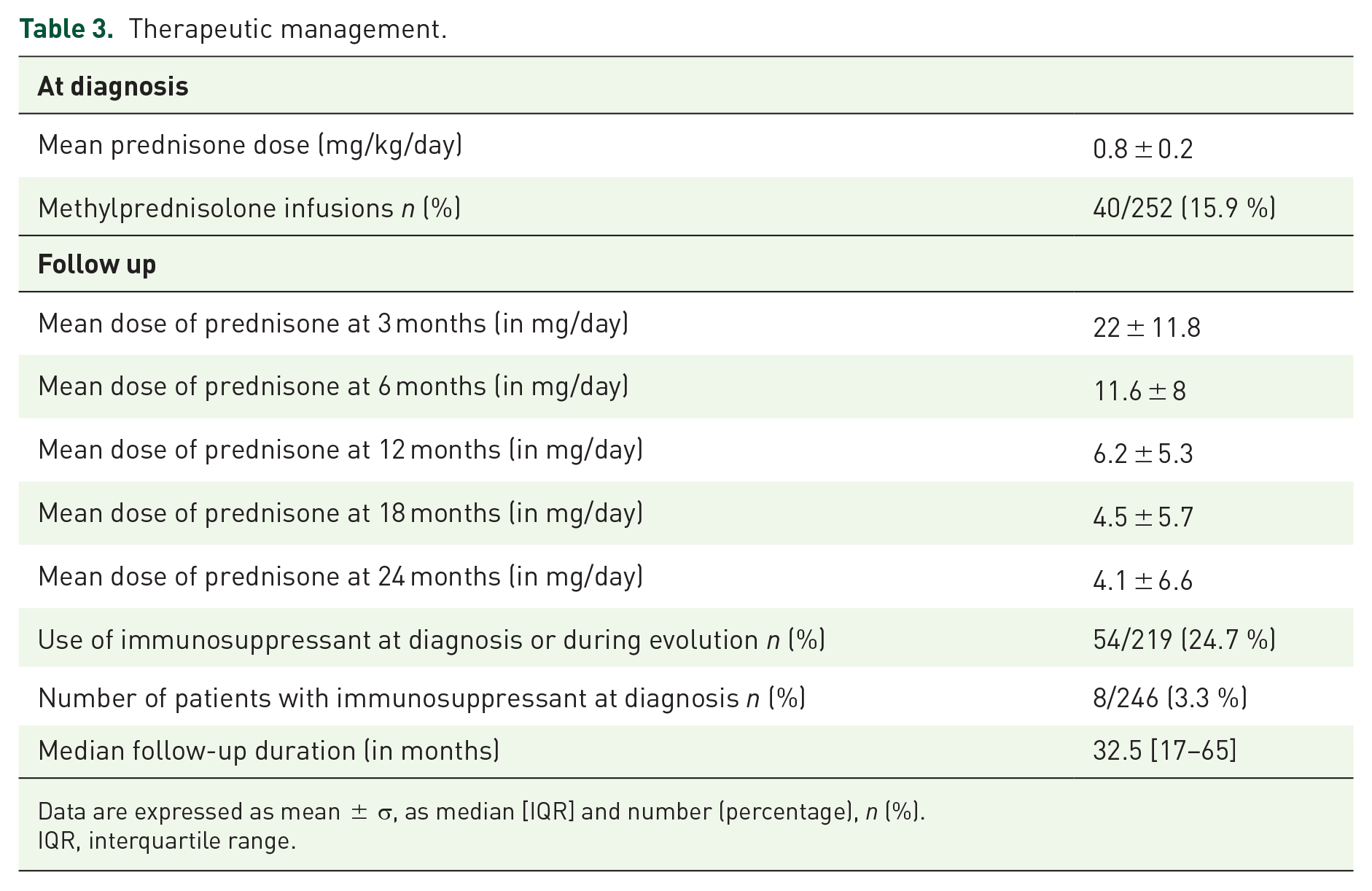
Data are expressed as mean ± σ, as median [IQR] and number (percentage), n (%).
IQR, interquartile range.
In this cohort of 254 patients, 117 relapsed (46.1%). Among relapsing patients, 53.8% experienced only one relapse (63/117), 27.4% two relapses (32/117), and 19% more than two relapses (22/117); 54 patients (21.3% of the cohort) experienced multiple (at least two) relapses.
Median time to first relapse after diagnosis was 9 months,4–17 with a mean dose of prednisone at first relapse of 10.9 (±11.7) mg/day. Median time to second relapse after diagnosis was 21.5 months [10–32.3] with a mean prednisone dose at second relapse of 5.8 (±5.6) mg/day.
A total of 39 patients (15.4%) experienced at least one vascular event during follow up, with a median time to onset of 21.5 months: aortic event in 7.1%, limb ischemia in 5.5%, myocardial infarction in 5.1% and stroke in 4.7%. Death occurred in 11% (n = 28) of our patients.
Clinical characteristics and laboratory assessments at diagnosis of both groups, R (n = 117; 46.1%) and NR (n = 137; 53.9%), were compared; 32.8% (45/137) of NR patients were male versus 19.7% (23/117) of R patients (p = 0.02), and 33% (38/115) of R patients had peripheral musculoskeletal manifestations versus 20.5% (26/127) of NR (p = 0.03). We found no differences between the two groups in terms of biological and histological data. NR patients had significantly more strokes at diagnosis than R patients (4.4% versus none, p = 0.03). Table 4 presents a comparison of CT-scan data at diagnosis. The brachiocephalic trunk was affected more frequently on CT-scan (p = 0.046), as carotids (p = 0.02), in R patients.
Comparison of CT-scan data at diagnosis.

Significant at p < 0.05.
CT, computed tomography.
Data from PET-scan and angio-MRI imaging did not show any significant differences between the two groups. Table 5 presents a comparison of the therapeutic management between the two groups.
Comparison of the therapeutic management of the two groups.

Significant at p < 0.05.
Mean ± σ (median).
Tables 6 and 7 show the multivariable analysis conducted to identify predictive factors associated with relapse and multiple relapses during the follow-up period. All the variables assessed in the two models are shown in Supplemental Tables S1 and S2.
Multivariable analysis of factors associated with relapse in GCA patients.
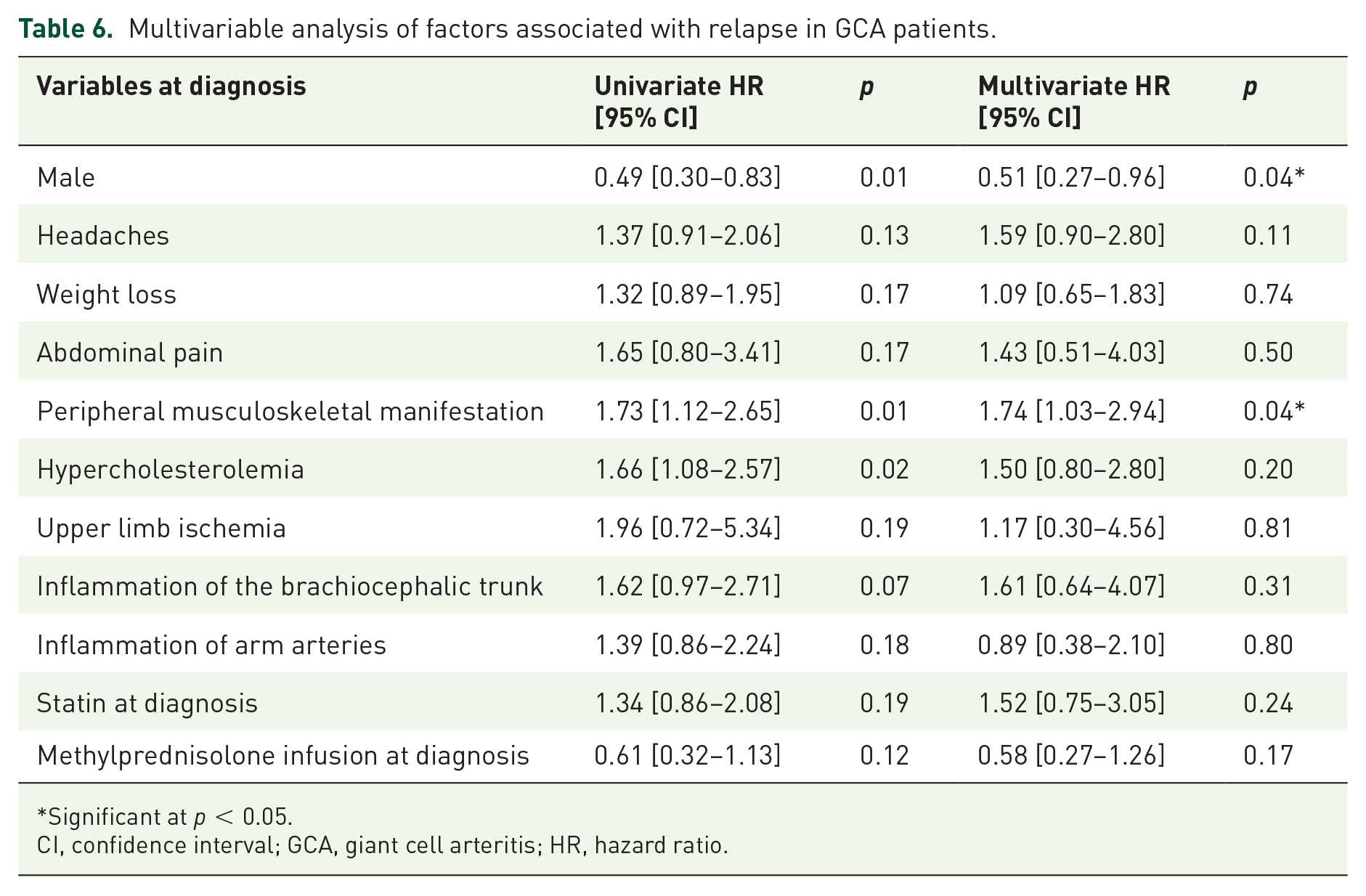
Significant at p < 0.05.
CI, confidence interval; GCA, giant cell arteritis; HR, hazard ratio.
Multivariable analysis of factors associated with multiple relapses in GCA patients.

Significant at p < 0.05.
CI, confidence interval; GCA, giant cell arteritis; HR, hazard ratio; TAB, temporal artery biopsy.
Relapsing patients experienced a vascular event (aortic, limb or mesenteric ischemia, stroke, myocardial infarction or de novo distal arteritis) in 19.7% of cases during follow-up versus 11.7% of the non-relapsing (p = 0.08). Thus, we did not note more deaths among R patients (9.4%) than among NR patients (12.4%, p = 0.55).
Discussion
A descriptive analysis of our patients found clinical, biological, and therapeutic characteristics somewhat similar to those of the main cohorts in the international literature.11–13,17,19–21,30–41 The initial corticosteroid therapy was fully consistent with current treatment recommendations.42–44 To our knowledge, our study is the first to assess GCA relapse risk factors in a large cohort of patients who all had a detailed arterial evaluation with appropriate vascular imaging at diagnosis.
Relapse occurred in 46.1% of cases; nearly half of relapsing patients were multi-relapsers. In the literature, similar results were observed with 36.5–40.8% of relapsing patients, 12 and 18.4% with at least two relapses. 13 In this study, the median follow-up time of 32.5 months is quite long, with a median time to first relapse after diagnosis of 9 months and time to second relapse of 21.5 months. In the study published by Restuccia et al., 27.3% of relapses occurred during the first year of follow up and 19.1% in the second year, 13 with a median of 12 months for the first relapse, whereas 50% of relapses occurred in the first year in the study published by Labarca et al. 17
Risk factors for GCA relapse are poorly identified. Biological inflammatory syndrome at diagnosis was not a risk factor for relapse in our study, as in the literature.12,13,17,30 Male gender was a protective factor for relapse, which was also the case in the cohort of Labarca et al. 17 It has been suggested that women have a GCA with more general symptoms, more often fever, and more frequently a biological inflammatory syndrome, 45 which are more frequent manifestations in LV-GCA. There could be a hormonal influence, as one study suggested a protective role of pregnancy on the onset of GCA, probably due to the protection of the vascular wall through hyperestrogenia. 46 Postmenopausal hypoestrogenesis may have a deleterious effect on the smooth muscle cells in the walls of large vessels. Indeed, early menopause could be a risk factor for developing GCA. 47 Cytoplasmic expression of estrogen receptor-alpha (ER-alpha) has been demonstrated in the smooth muscle cells of temporal arteries of GCA patients, as well as in the activated mononuclear cells and giant cells of these patients, compared with age- and sex-matched controls. 48
The presence of peripheral musculoskeletal manifestations was identified in this study as a risk factor for relapse and multiple relapses (HR: 1.74 and 2.78, respectively). These peripheral musculoskeletal manifestations, whether or not associated with PMR, 49 tend to be underestimated, and remain poorly described in the literature. Therefore, our results encourage us to look for these symptoms in the case of any suspicion or diagnosis of GCA, which seems to reflect an extensive disease, not limited to rhizomelic or cranial involvement. Large vessel vasculitis is not uncommon to be disclosed by imaging techniques, such as PET-scan, in patients initially diagnosed as having an isolated PMR. 50 Moreover, inflammatory low back pain, pelvic girdle pain and bilateral diffuse lower limb pain have been found to be predictors of a positive PET-scan for LV-GCA in patients initially diagnosed with isolated PMR. 51
PMR associated with GCA, 22.3% in this study, is also lower than the 40% usually estimated in the literature. 3 This difference can be explained by a clear distinction between PMR defined on EULAR criteria, 28 and peripheral musculoskeletal manifestations which did not meet PMR criteria. This level of precision is not always present in GCA studies, but is in accordance with previous data already reported by Salvarani. 49
Upper limb ischemia and inflammation of arm arteries (axillary and brachial arteries) on CT-scan at diagnosis, which reflect large-vessel extracranial involvement, were, in this study, found as multiple relapse risk factors (HR: 8.84 and 2.39, respectively). Thus, carotids and brachiocephalic trunk inflammatory involvement on CT-scan were more frequent in relapsing patients. According to the literature, LV-GCA patients, particularly involving the subclavian artery or with aortitis, would relapse more than isolated cranial forms.20,22,33 Recently, Sugihara et al. 52 found the presence of large-vessel lesions at baseline as associated significantly with poor treatment outcomes (HR: 3.54). Thus, large-vessel involvement could be predictive of multiple relapses in GCA.
Moreover, stroke was more frequent among non-relapsing patients: it can evoke a different GCA phenotype with cranial manifestations. Muratore et al. reported that cranial forms relapse less than extracranial forms, which would be more associated with vascular complications, particularly of the aorta.33,40 In the work of Dumont et al., relapsing patients had less history of stroke (p = 0.01) and presented large-vessel vasculitis more frequently on imaging (p = 0.01) than non-relapsing patients. 20 Therefore, LV-GCA was an independent predictive factor of relapse (HR: 1.49), as in our work, and stroke a protective factor against relapse (HR: 0.21).
Furthermore, Assie et al. 53 has suggested that upper limbs arteries involvement, in particular axillary arteries, remain under-diagnosed, as well as the need to look for vascular damage to the upper and lower limbs from the time of diagnosis and during follow up.
At last, a negative temporal artery biopsy was here a multiple relapse risk factor. Among patients with GCA-related aortitis, our group already showed that diffuse arterial involvement from the aortic arch was more frequent in temporal artery biopsy (TAB)-patients (29.1 versus 8.9%, p = 0.03), compared with those with positive TAB. 27 In this study, a positive TAB was associated with a lower relapse rate.
This retrospective study has limitations, with some missing data. Moreover, there was no systematic evaluation by imaging test of the cranial arteries. In this study, which extends over a period of 20 years, few patients had duplex ultrasonography of the temporal arteries because this technique has only been available in our center for a few years. Thus, the proportion of patients with an evaluation of the temporal arteries is not representative and cannot be taken into account as a predictive factor. There was no systematic evaluation by imaging test of the cranial arteries, but 248 of our 254 patients (97.6%) had a TAB, and it was positive for 67.3% (167 patients).
For the 254 patients included, the imaging techniques (PET, MRI, CT) for vascular assessment could be different at GCA diagnosis, but the multivariate analysis was performed only on the 229 patients who had a CT-scan for quality and statistical consistency.
The choice of treatment (methylprednisolone infusions, immunosuppressive drugs) was at the discretion of the physician, but the median corticosteroid doses at 3, 6, 12, 18, and 24 months are fully in line with current recommendations. Few patients received immunosuppressive treatments at GCA diagnosis due to the age of this cohort.
Conclusion
This study, on a large series of 254 patients with an initial vascular imaging screening at diagnosis, shows a relapse rate of 46.1% and highlights male gender as a relapse protective factor. To our knowledge, this is the first study to identify risk factors of GCA multiple relapses: peripheral musculoskeletal manifestations, a negative temporal artery biopsy and large-vessel involvement with upper limb ischemia and/or inflammation of arm arteries at CT-scan at diagnosis, hence the necessity to evaluate LV involvement, especially axillary and brachial arteries at GCA diagnosis. Factors associated with potential relapse remain to be validated in a multicenter prospective cohort. If they are confirmed, an early adjunction of an immunosuppressive drug could be evaluated in order to limit relapses and spare corticosteroids.
Footnotes
Author contributions
Donatienne de Mornac: study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript. Olivier Espitia: study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript. Antoine Néel: critical review, commentary and revision. Jérôme Connault: critical review, commentary and revision. Agathe Masseau: critical review, commentary and revision. Alexandra Espitia-Thibault: critical review, commentary and revision. Mathieu Artifoni: critical review, commentary and revision. Aurélie Achille: critical review, commentary and revision. Anaïs Wahbi: critical review, commentary and revision. Mathieu Lacou: critical review, commentary and revision. Cécile Durant: critical review, commentary and revision. Pierre Pottier: critical review, commentary and revision. François Perrin: critical review, commentary and revision. Julie Graveleau: critical review, commentary and revision. Mohamed Hamidou: critical review, commentary and revision. Jean-Benoit Hardouin: methodology, formal analysis. Christian Agard: study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; supervision.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.